Examining Regional Differences of Dietary Inflammatory Index and Its Association with Depression and Depressive Symptoms in Korean Adults


Abstract
:1. Introduction
2. Methods
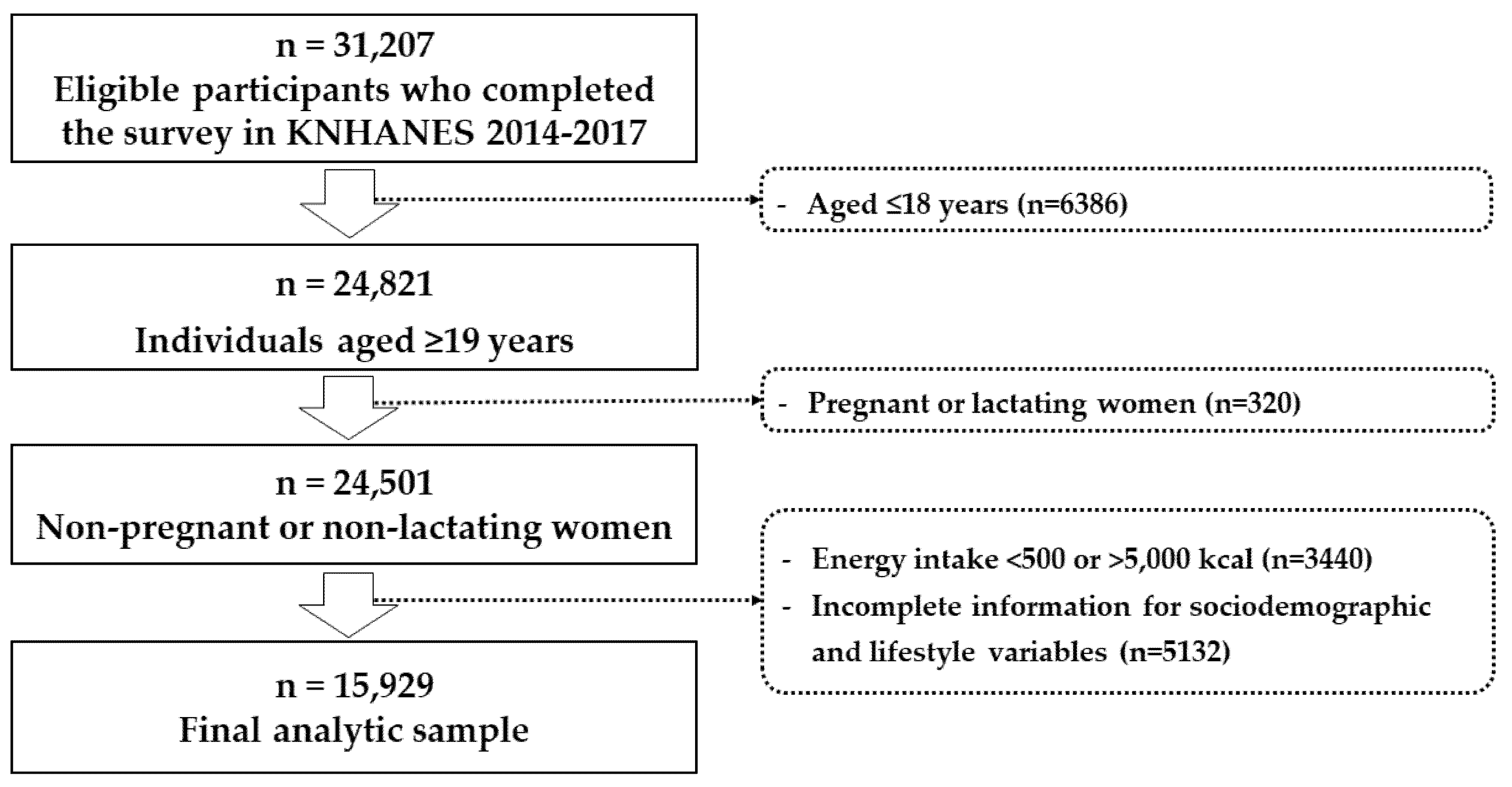
2.1. Study Population
2.2. Dietary Inflammatory Index (DII®)
2.3. Assessment of Depression and Depressive Symptoms
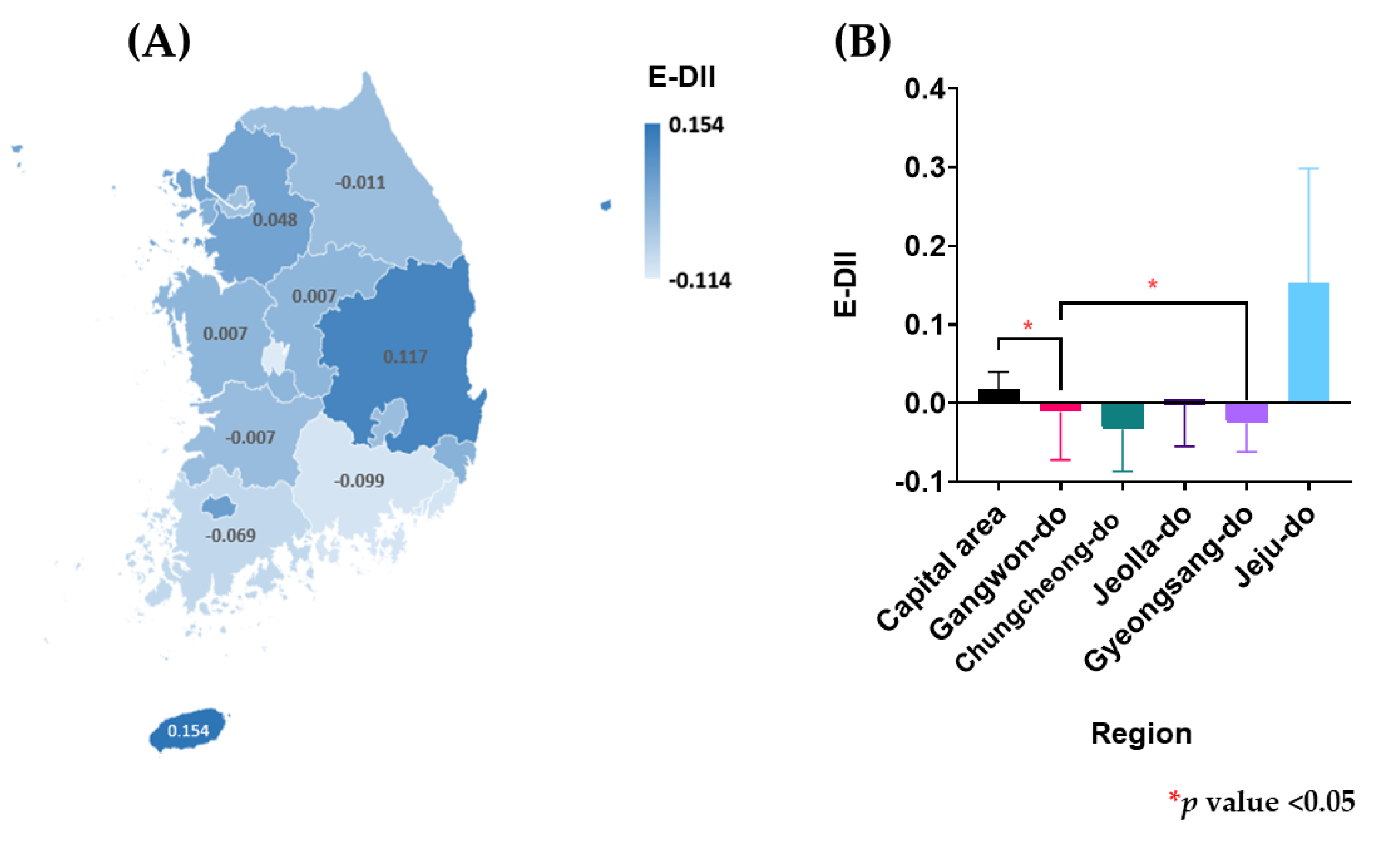
2.4. Definition of Regions
2.5. Statistical Analyses
3. Results
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization. Depression and Other Common Mental Disorders: Global Health Estimates; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Kim, W.K.; Shin, D.; Song, W.O. Are dietary patterns associated with depression in US adults? J. Med. Food 2016, 19, 1074–1084. [Google Scholar] [CrossRef] [PubMed]
- Parletta, N.; Zarnowiecki, D.; Cho, J.; Wilson, A.; Bogomolova, S.; Villani, A.; Itsiopoulos, C.; Niyonsenga, T.; Blunden, S.; Meyer, B.; et al. A Mediterranean-style dietary intervention supplemented with fish oil improves diet quality and mental health in people with depression: A randomized controlled trial (HELFIMED). Nutr. Neurosci. 2019, 22, 474–487. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cabello, M.; Miret, M.; Caballero, F.F.; Chatterji, S.; Naidoo, N.; Kowal, P.; D’Este, C.; Ayuso-Mateos, J.L. The role of unhealthy lifestyles in the incidence and persistence of depression: A longitudinal general population study in four emerging countries. Glob. Health 2017, 13, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skapinakis, P.; Lewis, G.; Araya, R.; Jones, K.; Williams, G. Mental health inequalities in Wales, UK: Multi-level investigation of the effect of area deprivation. Br. J. Psychiatry 2005, 186, 417–422. [Google Scholar] [CrossRef] [Green Version]
- Hodes, G.E.; Menard, C.; Russo, S.J. Integrating Interleukin-6 into depression diagnosis and treatment. Neurobiol. Stress 2016, 4, 15–22. [Google Scholar] [CrossRef] [Green Version]
- Anderson, G.; Kubera, M.; Duda, W.; Lason, W.; Berk, M.; Maes, M. Increased IL-6 trans-signaling in depression: Focus on the tryptophan catabolite pathway, melatonin and neuroprogression. Pharmacol. Rep. 2013, 65, 1647–1654. [Google Scholar] [CrossRef]
- Vogelzangs, N.; Duivis, H.E.; Beekman, A.T.; Kluft, C.; Neuteboom, J.; Hoogendijk, W.; Smit, J.H.; de Jonge, P.; Penninx, B.W. Association of depressive disorders, depression characteristics and antidepressant medication with inflammation. Transl. Psychiatry 2012, 2, e79. [Google Scholar] [CrossRef] [Green Version]
- Levine, J.; Barak, Y.; Chengappa, K.N.; Rapoport, A.; Rebey, M.; Barak, V. Cerebrospinal cytokine levels in patients with acute depression. Neuropsychobiology 1999, 40, 171–176. [Google Scholar] [CrossRef]
- Rethorst, C.D.; Bernstein, I.; Trivedi, M.H. Inflammation, obesity, and metabolic syndrome in depression: Analysis of the 2009-2010 National Health and Nutrition Examination Survey (NHANES). J. Clin. Psychiatry 2014, 75, e1428–e1432. [Google Scholar] [CrossRef] [Green Version]
- Kim, W.K.; Shin, D.; Song, W.O. Depression and its comorbid conditions more serious in women than in men in the United States. J. Womens Health 2015, 24, 978–985. [Google Scholar] [CrossRef]
- Khandaker, G.M.; Pearson, R.M.; Zammit, S.; Lewis, G.; Jones, P.B. Association of serum interleukin 6 and C-reactive protein in childhood with depression and psychosis in young adult life: A population-based longitudinal study. JAMA Psychiatry 2014, 71, 1121–1128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Felger, J.C. Role of Inflammation in Depression and Treatment Implications. Handb. Exp. Pharmacol. 2019, 250, 255–286. [Google Scholar] [PubMed]
- Felger, J.C.; Lotrich, F.E. Inflammatory cytokines in depression: Neurobiological mechanisms and therapeutic implications. Neuroscience 2013, 246, 199–229. [Google Scholar] [CrossRef] [Green Version]
- Shivappa, N.; Steck, S.E.; Hurley, T.G.; Hussey, J.R.; Hebert, J.R. Designing and developing a literature-derived, population-based dietary inflammatory index. Public Health Nutr. 2014, 17, 1689–1696. [Google Scholar] [CrossRef] [Green Version]
- Ramallal, R.; Toledo, E.; Martinez-Gonzalez, M.A.; Hernandez-Hernandez, A.; Garcia-Arellano, A.; Shivappa, N.; Hebert, J.R.; Ruiz-Canela, M. Dietary Inflammatory Index and Incidence of Cardiovascular Disease in the SUN Cohort. PLoS ONE 2015, 10, e0135221. [Google Scholar] [CrossRef] [PubMed]
- Shivappa, N.; Steck, S.E.; Hurley, T.G.; Hussey, J.R.; Ma, Y.; Ockene, I.S.; Tabung, F.; Hebert, J.R. A population-based dietary inflammatory index predicts levels of C-reactive protein in the Seasonal Variation of Blood Cholesterol Study (SEASONS). Public Health Nutr. 2014, 17, 1825–1833. [Google Scholar] [CrossRef]
- Tabung, F.K.; Steck, S.E.; Zhang, J.; Ma, Y.; Liese, A.D.; Agalliu, I.; Hingle, M.; Hou, L.; Hurley, T.G.; Jiao, L. Construct validation of the dietary inflammatory index among postmenopausal women. Ann. Epidemiol. 2015, 25, 398–405. [Google Scholar] [CrossRef] [Green Version]
- Wirth, M.D.; Shivappa, N.; Davis, L.; Hurley, T.G.; Ortaglia, A.; Drayton, R.; Blair, S.N.; Hebert, J.R. Construct Validation of the Dietary Inflammatory Index among African Americans. J. Nutr. Health Aging 2017, 21, 487–491. [Google Scholar]
- Shin, D.; Lee, K.W.; Brann, L.; Shivappa, N.; Hebert, J.R. Dietary inflammatory index is positively associated with serum high-sensitivity C-reactive protein in a Korean adult population. Nutrition 2019, 63–64, 155–161. [Google Scholar]
- Burrows, K.; Stewart, J.L.; Antonacci, C.; Kuplicki, R.; Thompson, K.; Taylor, A.; Teague, T.K.; Paulus, M.P. Association of poorer dietary quality and higher dietary inflammation with greater symptom severity in depressed individuals with appetite loss. J. Affect. Disord. 2020, 263, 99–106. [Google Scholar] [CrossRef]
- Bergmans, R.S.; Malecki, K.M. The association of dietary inflammatory potential with depression and mental well-being among U.S. adults. Prev. Med. 2017, 99, 313–319. [Google Scholar] [CrossRef] [PubMed]
- Jorgensen, D.; White, G.E.; Sekikawa, A.; Gianaros, P. Higher dietary inflammation is associated with increased odds of depression independent of Framingham Risk Score in the National Health and Nutrition Examination Survey. Nutr. Res. 2018, 54, 23–32. [Google Scholar] [CrossRef] [PubMed]
- Adjibade, M.; Lemogne, C.; Touvier, M.; Hercberg, S.; Galan, P.; Assmann, K.E.; Julia, C.; Kesse-Guyot, E. The Inflammatory Potential of the Diet is Directly Associated with Incident Depressive Symptoms Among French Adults. J. Nutr. 2019, 149, 1198–1207. [Google Scholar] [CrossRef] [PubMed]
- Shivappa, N.; Hebert, J.R.; Veronese, N.; Caruso, M.G.; Notarnicola, M.; Maggi, S.; Stubbs, B.; Firth, J.; Fornaro, M.; Solmi, M. The relationship between the dietary inflammatory index (DII®) and incident depressive symptoms: A longitudinal cohort study. J. Affect. Disord. 2018, 235, 39–44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akbaraly, T.; Kerlau, C.; Wyart, M.; Chevallier, N.; Ndiaye, L.; Shivappa, N.; Hebert, J.R.; Kivimaki, M. Dietary inflammatory index and recurrence of depressive symptoms: Results from the Whitehall II Study. Clin. Psychol. Sci. 2016, 4, 1125–1134. [Google Scholar] [CrossRef] [Green Version]
- Phillips, C.M.; Shivappa, N.; Hebert, J.R.; Perry, I.J. Dietary inflammatory index and mental health: A cross-sectional analysis of the relationship with depressive symptoms, anxiety and well-being in adults. Clin. Nutr. 2018, 37, 1485–1491. [Google Scholar] [CrossRef]
- Han, A.L.; Shin, S.R. Relationship between dietary intake and depression in metabolic syndrome among Korean adults: Korea National Health and Nutrition Examination Survey 2014. J. Agric. Med. Community Health 2017, 42, 79. [Google Scholar]
- Wirth, M.D.; Shivappa, N.; Burch, J.B.; Hurley, T.G.; Hébert, J.R. The Dietary Inflammatory Index, shift work, and depression: Results from NHANES. Health Psychol. 2017, 36, 760. [Google Scholar] [CrossRef]
- Shivappa, N.; Schoenaker, D.A.; Hebert, J.R.; Mishra, G.D. Association between inflammatory potential of diet and risk of depression in middle-aged women: The Australian Longitudinal Study on Women’s Health. Br. J. Nutr. 2016, 116, 1077–1086. [Google Scholar] [CrossRef] [Green Version]
- Kendler, K.S.; Gardner, C.; Neale, M.; Prescott, C. Genetic risk factors for major depression in men and women: Similar or different heritabilities and same or partly distinct genes? Psychol. Med. 2001, 31, 605–616. [Google Scholar] [CrossRef]
- Demirkan, A.; Penninx, B.W.; Hek, K.; Wray, N.R.; Amin, N.; Aulchenko, Y.S.; Van Dyck, R.; de Geus, E.J.; Hofman, A.; Uitterlinden, A.G. Genetic risk profiles for depression and anxiety in adult and elderly cohorts. Mol. Psychiatry 2011, 16, 773–783. [Google Scholar] [CrossRef] [PubMed]
- Cole, S.W.; Arevalo, J.M.G.; Takahashi, R.; Sloan, E.K.; Lutgendorf, S.K.; Sood, A.K.; Sheridan, J.F.; Seeman, T.E. Computational identification of gene–social environment interaction at the human IL6 locus. Proc. Natl. Acad. Sci. USA 2010, 107, 5681–5686. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wirth, M.D.; Hebert, J.R.; Shivappa, N.; Hand, G.A.; Hurley, T.G.; Drenowatz, C.; McMahon, D.; Shook, R.P.; Blair, S.N. Anti-inflammatory Dietary Inflammatory Index scores are associated with healthier scores on other dietary indices. Nutr. Res. 2016, 36, 214–219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Drewnowski, A.; Aggarwal, A.; Hurvitz, P.M.; Monsivais, P.; Moudon, A.V. Obesity and supermarket access: Proximity or price? Am. J. Public Health 2012, 102, e74–e80. [Google Scholar] [CrossRef] [PubMed]
- Darmon, N.; Drewnowski, A. Does social class predict diet quality? Am. J. Clin. Nutr. 2008, 87, 1107–1117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, E.; Jeong, Y.H. Decomposition of regional income inequality in Korea. Rev. Reg. Stud. 2003, 33, 313–327. [Google Scholar]



{kind=link}
{kind=link}
| E-DII | ||||||||
|---|---|---|---|---|---|---|---|---|
| Tertile 1 (n = 5309) | Tertile 2 (n = 5310) | Tertile 3 (n = 5310) | Total | |||||
| n | Wt’d % | n | Wt’d % | n | Wt’d % | n | p Value 1 | |
| Gender | ||||||||
| Men | 1998 | 43.5 | 2405 | 52.6 | 2798 | 60.3 | 7201 | <0.0001 |
| Women | 3311 | 56.5 | 2905 | 47.4 | 2512 | 39.7 | 8728 | |
| Age (year) | ||||||||
| 19–29 | 315 | 10.0 | 559 | 16.4 | 1075 | 29.4 | 1949 | <0.0001 |
| 30–49 | 1766 | 39.3 | 1928 | 41.3 | 2033 | 41.9 | 5727 | |
| 50–64 | 1899 | 34.0 | 1582 | 27.7 | 1113 | 17.7 | 4594 | |
| ≥65 | 1329 | 16.7 | 1241 | 14.5 | 1089 | 10.9 | 3659 | |
| Household income | ||||||||
| Low | 819 | 12.3 | 891 | 12.7 | 1026 | 14.7 | 2736 | <0.0001 |
| Middle low | 1247 | 21.4 | 1318 | 22.9 | 1348 | 25.2 | 3913 | |
| Middle high | 1511 | 30.1 | 1508 | 31.3 | 1490 | 29.3 | 4509 | |
| High | 1732 | 36.2 | 1593 | 33.1 | 1446 | 30.8 | 4771 | |
| Education | ||||||||
| ≤Elementary school | 849 | 11.2 | 920 | 11.3 | 891 | 9.9 | 2660 | <0.0001 |
| Middle/high school | 2253 | 40.4 | 2078 | 36.7 | 1834 | 31.7 | 6165 | |
| ≥College | 2207 | 48.4 | 2312 | 52.1 | 2585 | 58.4 | 7104 | |
| Employment status (n = 15,906) | ||||||||
| Blue-collar Worker 2 | 1940 | 40.8 | 1989 | 42.8 | 2057 | 44.2 | 5986 | <0.0001 |
| White-collar Worker 3 | 1157 | 21.2 | 1298 | 23.9 | 1299 | 22.9 | 3754 | |
| Unemployed | 2208 | 37.9 | 2015 | 33.3 | 1943 | 32.8 | 6166 | |
| Drinking status | ||||||||
| Nondrinker | 2379 | 40.6 | 2165 | 37.0 | 1782 | 29.0 | 6326 | <0.0001 |
| 1–4 times/month | 1924 | 39.3 | 1915 | 38.4 | 1959 | 40.9 | 5798 | |
| ≥2 times/week | 1006 | 20.1 | 1230 | 24.7 | 1569 | 30.0 | 3805 | |
| Smoking status | ||||||||
| Nonsmoker | 4669 | 84.8 | 4387 | 78.6 | 3961 | 70.7 | 13,017 | <0.0001 |
| Current smoker | 640 | 15.2 | 923 | 21.4 | 1349 | 29.3 | 2912 | |
| Physical activity 4 | ||||||||
| No | 2662 | 46.5 | 2847 | 48.8 | 2807 | 47.9 | 8316 | 0.16 |
| Yes | 2647 | 53.5 | 2463 | 51.2 | 2503 | 52.1 | 7613 | |
| BMI (kg/m2) | ||||||||
| <18.5 | 166 | 3.4 | 218 | 4.3 | 260 | 5.1 | 644 | 0.0002 |
| 18.5–22.9 | 2153 | 40.3 | 2017 | 38.3 | 2094 | 39.7 | 6264 | |
| 23–24.9 | 1315 | 24.5 | 1244 | 22.9 | 1158 | 21.5 | 3717 | |
| ≥25 | 1675 | 31.7 | 1831 | 34.5 | 1798 | 33.7 | 5304 | |
| Region | ||||||||
| Capital area | 2728 | 54.1 | 2754 | 56.0 | 2741 | 56.1 | 8223 | 0.36 |
| Gangwon-do | 185 | 2.7 | 219 | 3.1 | 179 | 2.6 | 583 | |
| Chungcheong-do | 584 | 9.3 | 592 | 9.5 | 561 | 8.5 | 1737 | |
| Jella-do | 485 | 8.5 | 448 | 8.0 | 495 | 8.5 | 1428 | |
| Gyeongsang-do | 1237 | 24.7 | 1192 | 22.5 | 1229 | 23.3 | 3658 | |
| Jeju-do | 90 | 0.8 | 105 | 0.9 | 105 | 1.0 | 300 | |
| No Depression (n = 15,177; 95.8%) | Depression (n = 752; 4.2%) | ||||
|---|---|---|---|---|---|
| n | Wt’d % | n | Wt’d % | p Value 1 | |
| Gender | |||||
| Men | 7024 | 53.6 | 177 | 30.4 | <0.0001 |
| Women | 8153 | 46.4 | 575 | 69.6 | |
| Age (year) | |||||
| 19–29 | 1891 | 19.5 | 58 | 13.7 | <0.0001 |
| 30–49 | 5544 | 41.4 | 183 | 31.1 | |
| 50–64 | 4319 | 25.6 | 275 | 34.4 | |
| ≥65 | 3423 | 13.6 | 236 | 20.9 | |
| Household income | |||||
| Low | 2501 | 12.7 | 235 | 27.1 | <0.0001 |
| Middle low | 3714 | 23.1 | 199 | 26.8 | |
| Middle high | 4361 | 30.6 | 148 | 21.0 | |
| High | 4601 | 33.6 | 170 | 25.1 | |
| Education | |||||
| ≤Elementary school | 2443 | 10.3 | 217 | 19.7 | <0.0001 |
| Middle/high school | 5832 | 35.5 | 333 | 46.7 | |
| ≥College | 6902 | 54.1 | 202 | 33.6 | |
| Employment status | |||||
| Blue-collar worker 2 | 5838 | 43.5 | 148 | 25.2 | <0.0001 |
| White-collar worker 3 | 3610 | 22.9 | 144 | 18.3 | |
| Unemployed | 5706 | 33.6 | 460 | 56.5 | |
| Drinking status | |||||
| Nondrinker | 5903 | 34.5 | 423 | 50.2 | <0.0001 |
| 1–4 times/month | 5590 | 40.0 | 208 | 30.5 | |
| ≥2 times/week | 3684 | 25.5 | 121 | 19.3 | |
| Smoking status | |||||
| Nonsmoker | 12,390 | 77.5 | 627 | 78.9 | 0.46 |
| Current smoker | 2787 | 22.5 | 125 | 21.1 | |
| Physical activity 4 | |||||
| No | 7899 | 47.7 | 417 | 49.1 | 0.53 |
| Yes | 7278 | 52.3 | 335 | 50.9 | |
| BMI (kg/m2) | |||||
| <18.5 | 611 | 4.3 | 33 | 5.7 | 0.11 |
| 18.5–22.9 | 5988 | 39.5 | 276 | 36.8 | |
| 23–24.9 | 3553 | 23.0 | 164 | 20.8 | |
| ≥25 | 5025 | 33.2 | 279 | 36.8 | |
| Region | |||||
| Capital area | 7850 | 55.5 | 373 | 55.2 | 0.62 |
| Gangwon-do | 551 | 2.8 | 32 | 3.3 | |
| Chungcheong-do | 1644 | 9.1 | 93 | 8.6 | |
| Jella-do | 1371 | 8.4 | 57 | 6.8 | |
| Gyeongsang-do | 3477 | 23.4 | 181 | 25.0 | |
| Jeju-do | 284 | 0.9 | 16 | 1.2 | |
| E-DII | |||||
| Tertile 1 | 5058 | 30.2 | 251 | 31.5 | 0.80 |
| Tertile 2 | 5054 | 33.1 | 256 | 32.8 | |
| Tertile 3 | 5065 | 36.7 | 245 | 35.7 | |
| Region | No Depression (n = 15,177; 95.8%) | Depression (n = 752; 4.2%) | p Value 1 |
|---|---|---|---|
| Capital area 2 (n = 8223) | 0.021 ± 0.0211 | −0.051 ± 0.083 | 0.38 |
| Gangwon-do (n = 583) | 0.005 ± 0.060 | −0.325 ± 0.272 | 0.26 |
| Chungcheong-do (n = 1737) | −0.041 ± 0.053 | 0.147 ± 0.158 | 0.22 |
| Jeolla-do (n = 1428) | 0.001 ± 0.054 | −0.085 ± 0.235 | 0.73 |
| Gyeongsang-do (n = 3658) | −0.028 ± 0.037 | 0.027 ± 0.153 | 0.72 |
| Jeju-do (n = 300) | 0.144 ± 0.151 | 0.328 + 0.344 | 0.66 |
| Region | E-DII | ||
|---|---|---|---|
| Tertile 1 | Tertile 2 | Tertile 3 | |
| Capital area (n = 8223) | 1.00 (Ref.) | 1.22 (0.89–1.68) | 1.44 (1.04–1.99) * |
| Gangwon-do (n = 583) | 1.00 (Ref.) | 3.64 (1.40–9.48) * | 1.57 (0.57–4.33) |
| Chungcheong-do (n = 1737) | 1.00 (Ref.) | 1.92 (0.97–3.80) | 2.97 (1.36–6.52) * |
| Jeolla-do (n = 1428) | 1.00 (Ref.) | 0.87 (0.52–1.47) | 1.60 (0.88–2.90) |
| Gyeongsang-do (n = 3658) | 1.00 (Ref.) | 1.05 (0.73–1.51) | 0.96 (0.63–1.47) |
| Jeju-do (n = 300) | 1.00 (Ref.) | 3.61 (0.93–13.99) | 4.06 (1.56–10.53) * |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shin, D.; Shivappa, N.; Hébert, J.R.; Lee, K.W. Examining Regional Differences of Dietary Inflammatory Index and Its Association with Depression and Depressive Symptoms in Korean Adults. Int. J. Environ. Res. Public Health 2020, 17, 3205. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17093205
Shin D, Shivappa N, Hébert JR, Lee KW. Examining Regional Differences of Dietary Inflammatory Index and Its Association with Depression and Depressive Symptoms in Korean Adults. International Journal of Environmental Research and Public Health. 2020; 17(9):3205. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17093205
Chicago/Turabian StyleShin, Dayeon, Nitin Shivappa, James R. Hébert, and Kyung Won Lee. 2020. "Examining Regional Differences of Dietary Inflammatory Index and Its Association with Depression and Depressive Symptoms in Korean Adults" International Journal of Environmental Research and Public Health 17, no. 9: 3205. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17093205