What is the Role of the Horizontal Transmission of Hepatitis B Virus Infection in Young Adult and Middle-Aged Roma Population Living in the Settlements in East Slovakia?

 , , ,
, , ,  ,
,
Abstract
:1. Introduction
- Vertical: mother to child—perinatal
- Horizontal: by blood or sexual intercourse [2]
- Countries with low prevalence of hepatitis B (up to 2%)
- Countries with moderate prevalence of hepatitis B (2%–8%)
- Countries with a high prevalence of hepatitis B (over 8%)
2. Methods
Statistical Analysis
3. Results
Description of Study Population
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| Anti HBc | Antibodies to Hepatitis B core antigen |
| Anti HBe | Antibodies to Hepatitis B e antigen |
| Anti HBs | Antibodies to Hepatitis B surface antigen |
| HBV | Hepatitis B virus |
| HBeAg | Hepatitis B e antigen |
| HBsAg | Hepatitis B surface antigen |
| HCC | Hepatocellular cancer |
| IgG | Immunoglobulin G |
| IVDU | Intravenous drug user |
| PEG | IFN Pegylated interferon |
Appendix A
References
- Fattovich, G. Natural history of hepatitis B. J. Hepatol. 2003, 39 (Suppl. S1), S50–S58. [Google Scholar] [CrossRef]
- Alter, M.J. Epidemiology of hepatitis b in europe and worldwide. J. Hepatol. 2003, 39 (Suppl. S1), S64–S69. [Google Scholar] [CrossRef]
- Nelson, N.P.; Easterbrook, P.J.; McMahon, B.J. Epidemiology of hepatitis B virus infection and impact of vaccination on disease. Clin. Liver Dis. 2016, 20, 607–628. [Google Scholar] [CrossRef] [Green Version]
- Alter, M.J.; Margolis, H.S. The emergence of hepatitis B as a sexually transmitted disease. Med. Clin. North Am. 1990, 74, 1529–1541. [Google Scholar] [CrossRef]
- Lok, A.S.; McMahon, B.J. Chronic hepatitis B. Hepatology 2007, 45, 507–539. [Google Scholar] [CrossRef] [Green Version]
- Drazilova, S.; Janicko, M.; Kristian, P.; Schreter, I.; Halanova, M.; Urbancikova, I.; Madarasova-Geckova, A.; Marekova, M.; Pella, D.; Jarcuska, P.; et al. Prevalence and risk factors for hepatitis B virus infection in Roma and non-Roma people in Slovakia. Int. J. Environ. Res. Public Health 2018, 15, 1047. [Google Scholar] [CrossRef] [Green Version]
- Stevens, C.E.; Neurath, R.A.; Beasley, R.P.; Szmuness, W. Hbeag and anti-HBe detection by radioimmunoassay: Correlation with vertical transmission of hepatitis B virus in Taiwan. J. Med. Virol. 1979, 3, 237–241. [Google Scholar] [CrossRef]
- Xu, Z.Y.; Liu, C.B.; Francis, D.P.; Purcell, R.H.; Gun, Z.L.; Duan, S.C.; Chen, R.J.; Margolis, H.S.; Huang, C.H.; Maynard, J.E. Prevention of perinatal acquisition of hepatitis B virus carriage using vaccine: Preliminary report of a randomized, double-blind placebo-controlled and comparative trial. Pediatrics 1985, 76, 713–718. [Google Scholar]
- Polaris Observatory, C. Global prevalence, treatment, and prevention of hepatitis b virus infection in 2016: A modelling study. Lancet Gastroenterol. Hepatol. 2018, 3, 383–403. [Google Scholar]
- Tanaka, J.; Akita, T.; Ko, K.; Miura, Y.; Satake, M. Epidemiological Research Group on Viral Hepatitis and its Long -term Course, Ministry of Health, Labour and Welfare of Japan. Countermeasures against viral hepatitis B and C in Japan: An epidemiological point of view. Hepatol. Res. 2019, 49, 990–1002. [Google Scholar] [CrossRef] [Green Version]
- Hou, J.; Liu, Z.; Gu, F. Epidemiology and prevention of hepatitis B virus infection. Int. J. Med. Sci. 2005, 2, 50–57. [Google Scholar] [CrossRef] [Green Version]
- Shepard, C.W.; Simard, E.P.; Finelli, L.; Fiore, A.E.; Bell, B.P. Hepatitis B virus infection: Epidemiology and vaccination. Epidemiol. Rev. 2006, 28, 112–125. [Google Scholar] [CrossRef]
- Andre, F. Hepatitis B epidemiology in Asia, the Middle East and Africa. Vaccine 2000, 18 (Suppl. S1), S20–S22. [Google Scholar] [CrossRef]
- Tanaka, J. Hepatitis B epidemiology in Latin America. Vaccine 2000, 18 (Suppl. S1), S17–S19. [Google Scholar] [CrossRef]
- Maynard, J.E. Hepatitis B: Global importance and need for control. Vaccine 1990, 8, S18–S20. [Google Scholar] [CrossRef]
- Gecková, A.M.; Jarcuska, P.; Mareková, M.; Pella, D.; Siegfried, L.; Jarcuska, P.; Halánová, M. Hepameta—Prevalence of hepatitis B/C and metabolic syndrome in population living in separated and segregated Roma settlements: A methodology for a cross-sectional population-based study using community-based approach. Cent. Eur. J. Public Health 2014, 22, S6–S11. [Google Scholar] [CrossRef]
- Do, S. The natural history of hepatitis B in Asian Americans. Asian Am. Pac. Isl. J. Health 2001, 9, 141–153. [Google Scholar]
- Minuk, G.Y.; Bohme, C.E.; Bowen, T.J.; Hoar, D.I.; Cassol, S.; Gill, M.J.; Clarke, H.C. Efficacy of commercial condoms in the prevention of hepatitis B virus infection. Gastroenterology 1987, 93, 710–714. [Google Scholar] [CrossRef]
- Bernabe-Ortiz, A.; Carcamo, C.P.; Scott, J.D.; Hughes, J.P.; Garcia, P.J.; Holmes, K.K. HBV infection in relation to consistent condom use: A population-based study in Peru. PLoS ONE 2011, 6, e24721. [Google Scholar] [CrossRef]
- Kirwan, P.; Evans, B.; Sentinel Surveillance of Hepatitis Testing Study, G.; Brant, L. Hepatitis C and B testing in English prisons is low but increasing. J. Public Health 2011, 33, 197–204. [Google Scholar] [CrossRef] [Green Version]
- Jafari, S.; Buxton, J.A.; Afshar, K.; Copes, R.; Baharlou, S. Tattooing and risk of hepatitis B: A systematic review and meta-analysis. Can. J. Public Health 2012, 103, 207–212. [Google Scholar] [CrossRef] [PubMed]
- Zampino, R.; Boemio, A.; Sagnelli, C.; Alessio, L.; Adinolfi, L.E.; Sagnelli, E.; Coppola, N. Hepatitis B virus burden in developing countries. World J. Gastroenterol. 2015, 21, 11941–11953. [Google Scholar] [CrossRef] [PubMed]
- Geckova, A.M.; Babinska, I.; Bobakova, D.; Veselska, Z.D.; Bosakova, L.; Kolarcik, P.; Jarcuska, P.; Pella, D.; Halanova, M.; HepaMeta Team. Socioeconomic characteristics of the population living in Roma settlements and their association with health and health-related behaviour. Cent. Eur. J. Public Health 2014, 22, S57–S64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Babinska, I.; Geckova, A.M.; Jarcuska, P.; Pella, D.; Marekova, M.; Stefkova, G.; Veselska, Z.D.; HepaMeta, Team. Does the population living in Roma settlements differ in physical activity, smoking and alcohol consumption from the majority population in Slovakia? Cent. Eur. J. Public Health 2014, 22, S22–S27. [Google Scholar] [CrossRef] [Green Version]
- Jarcuska, P.; Bobakova, D.; Uhrin, J.; Bobak, L.; Babinska, I.; Kolarcik, P.; Veselska, Z.; Madarasova Geckova, A.; HEPA-META Team. Are barriers in accessing health services in the Roma population associated with worse health status among roma? Int. J. Public Health 2013, 58, 427–434. [Google Scholar] [CrossRef] [Green Version]
- Dolak, F.; Sedova, L.; Novakova, D.; Olisarova, V. Approach to prevention of obesity of Roma population in the region of south bohemia with focus on selected eating behaviors. Neuro Endocrinol. Lett. 2016, 37, 46–51. [Google Scholar]
- Veseliny, E.; Janicko, M.; Drazilova, S.; Siegfried, L.; Pastvova, L.; Schreter, I.; Kristian, P.; Viag, L.; Jarcuska, P.; Valkova, I.; et al. High hepatitis B and low hepatitis C prevalence in Roma population in Eastern Slovakia. Cent. Eur. J. Public Health 2014, 22, S51–S56. [Google Scholar] [CrossRef] [Green Version]
- European Association for the Study of the Liver. EASL 2017 clinical practice guidelines on the management of hepatitis B virus infection. J. Hepatol. 2017, 67, 370–398. [Google Scholar] [CrossRef] [Green Version]
- Drazilova, S.; Janicko, M.; Kristian, P.; Schreter, I.; Kucinsky, B.; Kozlej, M.; Hockickova, I.; Jarcuska, P. Lower viral response to pegylated interferon alpha 2a treatment of chronic hepatitis b in Roma people in Eastern Slovakia. Gastroenterol. Res. Pract. 2016, 2016, 8682494. [Google Scholar] [CrossRef] [Green Version]
- Spearman, C.W.; Afihene, M.; Ally, R.; Apica, B.; Awuku, Y.; Cunha, L.; Dusheiko, G.; Gogela, N.; Kassianides, C.; Kew, M.; et al. Hepatitis B in Sub-saharan Africa: Strategies to achieve the 2030 elimination targets. Lancet Gastroenterol. Hepatol. 2017, 2, 900–909. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| High Prevalence of Hepatitis B | Moderate Prevalence of Hepatitis B | Low Prevalence of Hepatitis B | |
|---|---|---|---|
| Prevalence of chronic infection | 8%–15% | 2%–7% | 0.1%–1% |
| Prevalence of past infection | 40%–90% | 16%–55% | 4%–15% |
| Perinatal infection | Frequent (more than 20%) * | Infrequent (10%–60%) * | Rare (less than 10%) * |
| Early young age at the time of infection | Very frequent (more than 60%) H | Frequent (10%–60%) H | Rare (less than 10%) H |
| Adolescent and adult age at the time of infection | Infrequent (10%–20%) | Frequent (20%–50%) | Very frequent (70%–90%) |
| Geographic distribution | Southeast Asia, China, Pacific islands, Sub-Saharan Africa, Alaska (Eskimo) | Mediterranean sea, Eastern Europe, Central Asia, Japan, South and Latin America, Middle East | USA, Canada, Western Europe, Australia, New Zealand |
| Absolute(Relative) Count or Median ± IQR (Where Noted) | 95% CI | |
|---|---|---|
| Imprisonment | 46 (10.3%) | 7.8–12.5 |
| IVDU | 2 (0.5%) | 0.08–1.8 |
| Sex for money | 13 (3%) | 1.7–5 |
| Condom use always/almost always | 41 (9.3%) | 0.7–12.4 |
| >4 sexual partners | 52 (11.9) | 9.2–15.3 |
| Tattoo total | 173 (39.1%) | 34.7–43.8 |
| Tattoo privately | 164 (37.1%) | 32.7–41.7 |
| Blood transfusion | 71 (16.7%) | 13.4–20.5 |
| Hepatitis B vaccination | 15 (3.5%) | 2.1–4.5 |
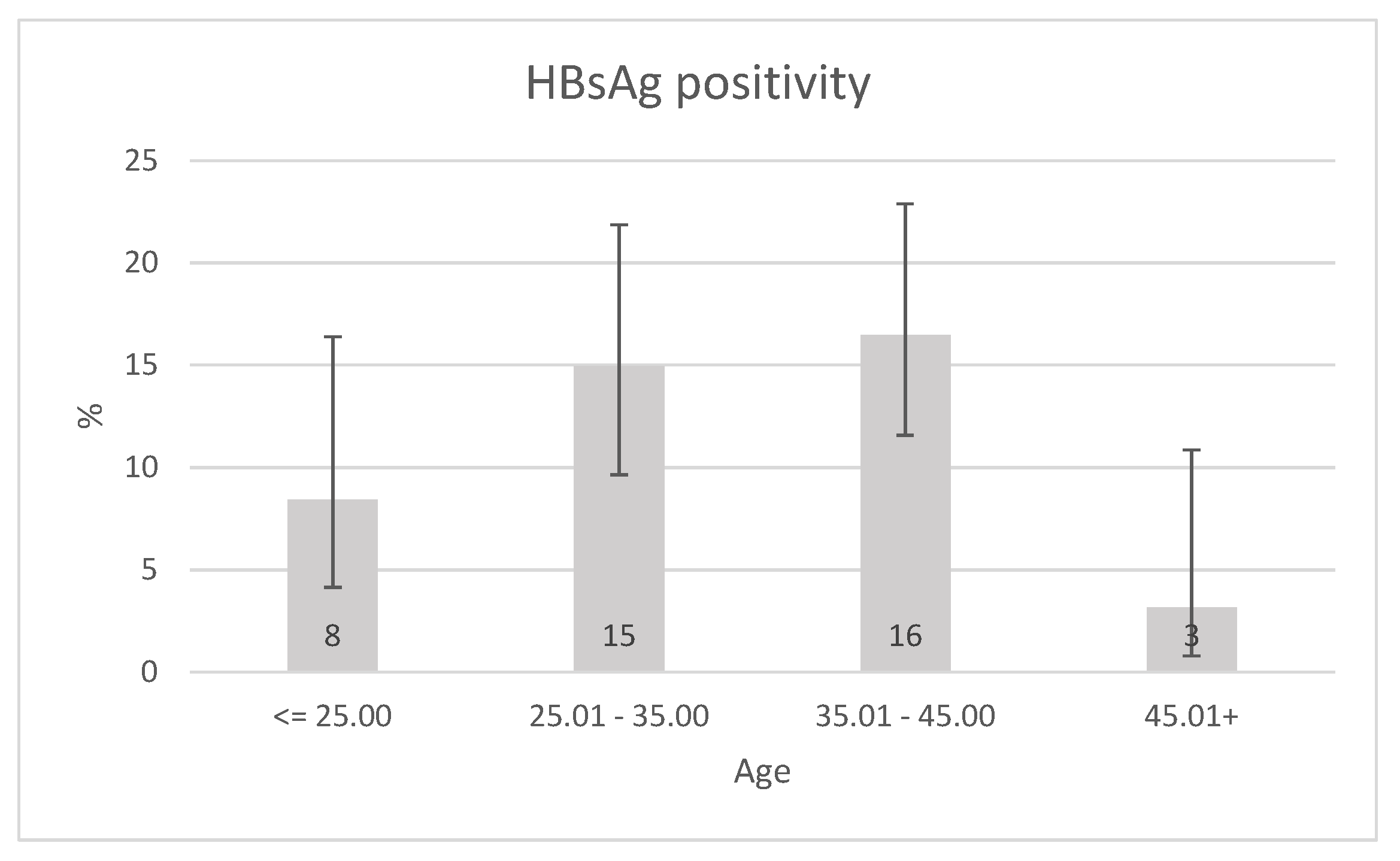
| HBsAg positivity | 55 (12.4%) | 9.7–15.8 |
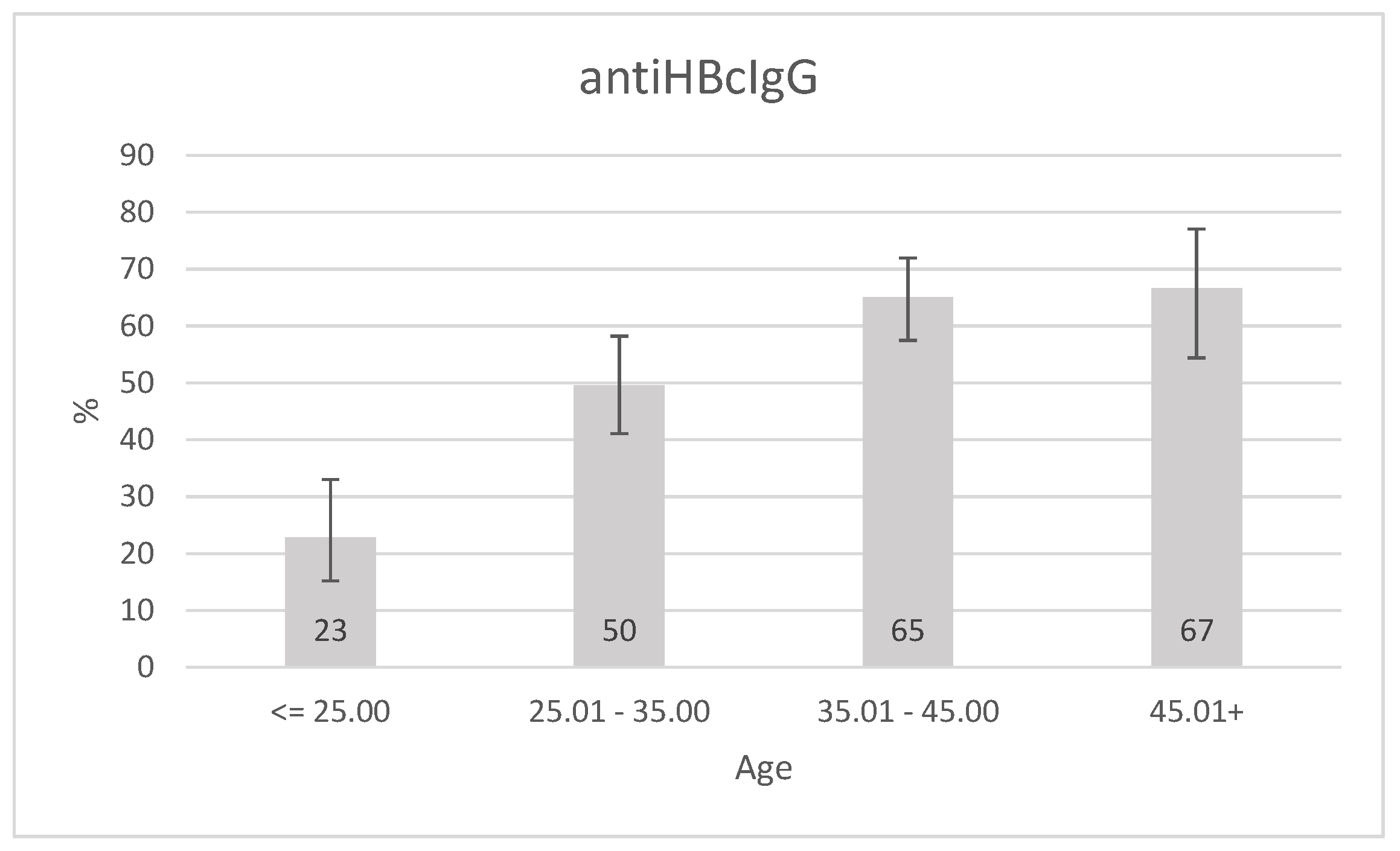
| Anti HBc IgG positivity | 233 (52.8%) | 48.2–57.4 |
| Persons in living unit (median ± IQR) | 7 ± 4 |
| Age Group | ≤25 Years | 25.01–35 Years | 35.01–45 Years | >45 Years | Sig |
|---|---|---|---|---|---|
| Male sex | 36 (42.4%) | 45 (34.4%) | 56 (34.1%) | 22 (32.8%) | 0.541 |
| Age (Mean ± Std. deviation) | 21.8 ± 1.9 | 29.8 ± 3.1 | 39.6 ± 2.2 | 48.3 (2.2%) | <0.0001 |
| Imprisonment | 6 (7.1%) | 10 (7.7%) | 20 (12.3%) | 10 (14.9%) | 0.242 |
| IVDU | 1 (1.2%) | 0 | 1 (0.6%) | 0 | 0.994 |
| Sex for money | 1 (1.2%) | 7 (5.4%) | 3 (1.9%) | 2 (3.0%) | 0.432 |
| Condom use always/almost always | 11 (13.4%) | 15 (11.8%) | 12 (7.4%) | 3 (4.5%) | 0.165 |
| >4 sexual partners | 14 (17.1%) | 18 (14.3%) | 10 (6.3%) | 10 (14.9%) | 0.04 |
| Tattoo total | 30 (35.7%) | 35 (26.9%) | 69 (43.1%) | 38 (56.7%) | 0.0003 |
| Tattoo privately | 29 (34.5%) | 31 (23.8%) | 66 (41.3%) | 37 (55.2%) | 0.0001 |
| Blood transfusion | 6 (7.7%) | 23 (18.5%) | 30 (18.8%) | 12 (20.0%) | 0.123 |
| Hepatitis B vaccination | 2 (2.4%) | 5 (3.8%) | 5 (3.0%) | 3 (4.5%) | 0.657 |
| Persons in living unit (median ± IQR%) | 6 ± 5 | 6 ± 4 | 7 ± 4 | 6 ± 4 | 0.286 |
| n | HBsAg Positive | HBsAg Negative | p | Multivariate Analysis OR and Significance | |||
|---|---|---|---|---|---|---|---|
| Male sex | 442 | 28 | 50.9% | 127 | 32.8% | 0.01 | 2.083 (95% CI 1.176−3.690); p = 0.012 ** |
| Imprisonment | 435 | 7 | 12.7% | 37 | 9.7% | 0.475 | |
| Drugs total | 439 | 1 | 1.9% | 9 | 2.3% | 1 | |
| Drugs iv | 432 | 0 | 0.0% | 2 | 0.5% | 1 | |
| >4 sexual partners | 427 | 8 | 14.5% | 43 | 11.6% | 0.507 | |
| Sex for money | 429 | 2 | 3.6% | 11 | 2.9% | 0.677 | |
| Tattoo total | 432 | 23 | 44.2% | 147 | 38.7% | 0.453 | |
| Tattoo private | 432 | 20 | 38.5% | 141 | 37.1% | 0.879 | |
| Tattoo parlor | 432 | 3 | 5.8% | 6 | 16.8% | 0.082 | |
| Blood transfusion | 418 | 8 | 14.8% | 61 | 16.8% | 0.845 | |
| Age(years) * | 442 | 35.24 (12.17) | 35.5 (15.5) | 0.864 | |||
| n | Anti HBcIgG Positive | Anti HBcIgG Negative | p | Multivariate ORs and Significance | |||
|---|---|---|---|---|---|---|---|
| Male sex | 441 | 91 | 39.10% | 64 | 60.8% | 0.069 | |
| Imprisonment | 434 | 31 | 13.50% | 13 | 6.4% | 0.014 | 1.600; (95% CI 0.702–3.646); p = 0.263 ** |
| Drugs total | 438 | 3 | 1.30% | 6 | 2.9% | 0.317 | |
| Drugs iv | 431 | 1 | 0.40% | 1 | 0.5% | 1 | |
| >4 sexual partners | 426 | 23 | 10.20% | 28 | 14.0% | 0.225 | |
| Sex for money | 428 | 8 | 3.50% | 5 | 2.5% | 0.533 | |
| Tattoo total | 431 | 100 | 44.20% | 69 | 33.7% | 0.025 | 1.070; (95% CI 0.663–1.727); p = 0.781 ** |
| Tattoo private | 431 | 95 | 42.00% | 65 | 31.7% | 0.027 | 1.163; (95% CI 0.704–1.833); p = 0.601 ** |
| Tattoo parlor | 431 | 5 | 2.20% | 4 | 2.0% | 1 | |
| Blood transfusion | 417 | 35 | 15.80% | 33 | 16.8% | 0.783 | |
| Age(years) * | 436 | 37.7 (11.98%) | 30.75 (16.12) | <0.0001 | OR for 1-year increment was 1.080; (95% CI 1.054–1.107); p < 0.0001 *** | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Drazilova, S.; Kristian, P.; Janicko, M.; Halanova, M.; Safcak, D.; Dorcakova, P.D.; Marekova, M.; Pella, D.; Madarasova-Geckova, A.; Jarcuska, P.; et al. What is the Role of the Horizontal Transmission of Hepatitis B Virus Infection in Young Adult and Middle-Aged Roma Population Living in the Settlements in East Slovakia? Int. J. Environ. Res. Public Health 2020, 17, 3293. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17093293
Drazilova S, Kristian P, Janicko M, Halanova M, Safcak D, Dorcakova PD, Marekova M, Pella D, Madarasova-Geckova A, Jarcuska P, et al. What is the Role of the Horizontal Transmission of Hepatitis B Virus Infection in Young Adult and Middle-Aged Roma Population Living in the Settlements in East Slovakia? International Journal of Environmental Research and Public Health. 2020; 17(9):3293. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17093293
Chicago/Turabian StyleDrazilova, Sylvia, Pavol Kristian, Martin Janicko, Monika Halanova, Dominik Safcak, Patricia Denisa Dorcakova, Maria Marekova, Daniel Pella, Andrea Madarasova-Geckova, Peter Jarcuska, and et al. 2020. "What is the Role of the Horizontal Transmission of Hepatitis B Virus Infection in Young Adult and Middle-Aged Roma Population Living in the Settlements in East Slovakia?" International Journal of Environmental Research and Public Health 17, no. 9: 3293. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17093293