Comparison of Skin Lesions Caused by Ixodes ricinus Ticks and Lipoptena cervi Deer Keds Infesting Humans in the Natural Environment


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Area
2.2. Clinical Cases
3. Results and Discussion
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Haarløv, N. Life cycle and distribution pattern of Lipoptena cervi (L.) (Dipt., Hippobosc.) on Danish deer. Oikos 1964, 15, 93–129. [Google Scholar] [CrossRef]
- Medlock, J.M.; Hansford, K.M.; Bormane, A.; Derdakova, M.; Estrada-Peña, A.; George, J.C.; Kazimirova, M. Driving forces for changes in geographical distribution of Ixodes ricinus ticks in Europe. Parasit. Vectors 2013, 6, 1. [Google Scholar] [CrossRef] [Green Version]
- Härkönen, L.; Härkönen, S.; Kaitala, A.; Kaunisto, S.; Kortet, R.; Laaksonen, S.; Ylönen, H. Predicting range expansion of an ectoparasite—The effect of spring and summer temperatures on deer ked Lipoptena cervi (Diptera: Hippoboscidae) performance along a latitudinal gradient. Ecography 2010, 33, 906–912. [Google Scholar] [CrossRef]
- Dehio, C.; Sauder, U.; Hiestand, R. Isolation of Bartonella schoenbuchensis from Lipoptena cervi, a blood-sucking arthropod causing deer ked dermatitis. J. Clin. Microbiol. 2004, 42, 5320–5323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Regier, Y.; Komma, K.; Weigel, M.; Pulliainen, A.T.; Göttig, S.; Hain, T.; Kempf, V.A.J. Microbiome Analysis Reveals the Presence of Bartonella spp. and Acinetobacter spp. in Deer Keds (Lipoptena cervi). Front. Microbiol. 2018, 9, 3100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buss, M.; Case, L.; Kearney, B.; Coleman, C.; Henning, J.D. Detection of Lyme disease and anaplasmosis pathogens via PCR in Pennsylvania deer ked. J. Vector Ecol. 2016, 41, 292–294. [Google Scholar] [CrossRef]
- Halos, L.; Jamal, T.; Maillard, R.; Girard, B.; Guillot, J.; Chomel, B.; Vayssier-Taussat, M.; Boulouris, H.-J. Role of Hippoboscidae flies as potential vectors of Bartonella spp. infecting wild and do-mestic ruminants. Appl. Environ. Microbiol. 2004, 70, 6302–6305. [Google Scholar] [CrossRef] [Green Version]
- Adamska, M. Wild ruminants in the area of the North-Western Poland as potential reservoir hosts of Bartonella schoenbuchensis and B. bovis. Acta Parasitol. 2008, 53, 407. [Google Scholar] [CrossRef]
- Matsumoto, K.; Berrada, Z.L.; Klinger, E.; Goethert, H.K.; Telford, S.R., III. Molecular detection of Bartonella schoenbuchensis from ectoparasites of deer in Massachusetts. Vector Borne Zoonot. Dis. 2008, 8, 549–554. [Google Scholar] [CrossRef]
- Korhonen, E.M.; Perez, V.C.; Pulliainen, A.T.; Sironen, T.; Aaltonen, K.; Kortet, R.; Mustonen, A.M. Molecular detection of Bartonella spp. in deer ked pupae, adult keds and moose blood in Finland. Epidemiol. Infect. 2015, 143, 578–585. [Google Scholar] [CrossRef] [Green Version]
- Duodu, S.; Madslien, K.; Hjelm, E.; Molin, Y.; Paziewska-Harris, A.; Harris, P.D.; Colquhoun, D.J.; Ytrehus, B. Bartonella infections in deer keds (Lipoptena cervi) and moose (Alces alces) in Norway. Appl. Environ. Microbiol. 2013, 79, 322–327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Razanske, I.; Rosef, O.; Radzijevskaja, J.; Klepeckiene, K.; Lipatova, I.; Paulauskas, A. Infections with Bartonella spp. in free-ranging cervids and deer keds (Lipoptena cervi) in Norway. Comp. Immunol. Microbiol. Infect. Dis. 2018, 58, 26–30. [Google Scholar] [CrossRef] [PubMed]
- Hornok, S.; de la Fuente, J.; Biró, N.; Fernández de Mera, I.G.; Meli, M.L.; Elek, V.; Gönczi, E.; Meili, T.; Tánczos, B.; Farkas, R.; et al. First molecular evidence of Anaplasma ovis and Rickettsia spp. in keds (Diptera: Hippoboscidae) of sheep and wild ruminants. Vector Borne Zoonotic. Dis. 2011, 11, 1319–1321. [Google Scholar] [CrossRef] [Green Version]
- De Bruin, A.; van Leeuwen, A.D.; Jahfari, S.; Takken, W.; Földvári, M.; Dremmel, L.; Sprong, H.; Földváriet, G. Vertical transmission of Bartonella schoenbuchensis in Lipoptena cervi. Parasit. Vectors 2015, 8, 176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Foley, J.E.; Hasty, J.M.; Lane, R.S. Diversity of rickettsial pathogens in Columbian black-tailed deer and their associated keds (Diptera: Hippoboscidae) and ticks (Acari: Ixodidae) J. Vector Ecol. 2016, 41, 41–47. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.-H.; Kim, K.-T.; Kwon, O.-D.; Ock, Y.; Kim, T.; Choi, D.; Kwak, D. Novel Detection of Coxiella spp., Theileria luwenshuni, and T. ovis Endosymbionts in Deer Keds (Lipoptena fortisetosa). PLoS ONE 2016, 11, e0156727. [Google Scholar] [CrossRef] [Green Version]
- Szewczyk, T.; Werszko, J.; Steiner-Bogdaszewska, Ż.; Jeżewski, W.; Laskowski, Z.; Karbowiak, G. Molecular detection of Bartonella spp. in deer ked (Lipoptena cervi) in Poland. Parasit. Vectors 2017, 10, 487. [Google Scholar] [CrossRef] [Green Version]
- Izenour, K.; Zikeli, S.; Kalalah, A.; Ditchkoff, S.D.; Starkey, L.A.; Wang, C.; Zohdy, S. Diverse Bartonella spp. detected in white-tailed deer (Odocoileus virginanus) and associaced keds (Lipoptena mazamae) in the southeastern United States. J. Wildl. Dis. 2020. [Google Scholar] [CrossRef]
- Bartosik, K.; Buczek, A. Determination of the parameters of the parasitic stage in Ixodes ricinus females. Ann. Agric. Environ. Med. 2013, 20, 441–446. [Google Scholar]
- Bartosik, K.; Sitarz, M.; Szymańska, J.; Buczek, A. Tick bites on humans in the agricultural and recreational areas in south-eastern Poland. Ann. Agric. Environ. Med. 2011, 18, 151–157. [Google Scholar]
- Reunala, T.; Brummer-Korvenkontio, H.; Palosuo, K.; Miyanij, M.; Ruiz-Maldonado, R.; Löve, A.; François, G.; Palosuo, T. Frequent occurrence of IgE and IgG4 antibodies against saliva of Aedes communis and Aedes aegypi mosquitoes in children. Int. Arch. Allergy Immunol. 1994, 104, 366–371. [Google Scholar] [CrossRef] [PubMed]
- Rantanen, T.; Reunala, T.; Vuojolahti, P.; Hackman, W. Persistent pruritic papules from deer ked bites. Acta Derm. Venereol. 1982, 62, 307–311. [Google Scholar] [PubMed]
- Härkönen, S.; Laine, M.; Vornanen, M.; Reunala, T. Deer ked (Lipoptena cervi) dermatitis in humans—An increasing nuisance in Finland. Alces 2009, 45, 73–79. [Google Scholar]
- Laukkanen, A.; Ruoppi, P.; Mäkkinen-Kiljunen, S. Deer ked-induced occupational allergic rhinoconjunctivitis. Ann. Allergy Asthma Immunol. 2005, 94, 604–608. [Google Scholar] [CrossRef]
- Bartosik, K.; Buczek, A. The impact of intensity of invasion of Ixodes ricinus and Dermacentor reticulatus on the course of the parasitic phase. Ann. Agric. Environ. Med. 2012, 19, 651–655. [Google Scholar]
- Parola, P.; Raoult, D. Ticks and Tickborne Bacterial Diseases in Humans: An Emerging Infectious Threat. Clin. Infect. Dis. 2001, 32, 897–928. [Google Scholar] [CrossRef]
- Kannangara, D.W.; Patel, P. Report of Non-Lyme, Erythema Migrans Rashes from New Jersey with a Review of Possible Role of Tick Salivary Toxins. Vector Borne Zoonotic Dis. 2018, 18, 641–652. [Google Scholar] [CrossRef]
- Tibbles, C.D.; Edlow, J.A. Does This Patient Have Erythema Migrans? JAMA 2007, 297, 2617–2627. [Google Scholar] [CrossRef]
- CDC 2018. Available online: https://www.cdc.gov/lyme/signs_symptoms/rashes.html (accessed on 3 April 2020).
- Cardenas-de la Garza, J.A.; De la Cruz-Valadez, E.; Ocampo-Candiani, J.; Welsh, O. Clinical spectrum of Lyme disease. Eur. J. Clin. Microbiol. Infect. Dis. 2019, 38, 201–208. [Google Scholar] [CrossRef]
- Wilhelmsson, P.; Lindblom, P.; Fryland, L.; Nyman, D.; Jaenson, T.G.; Forsberg, P.; Lindgren, P.E. Ixodes ricinus ticks removed from humans in Northern Europe: Seasonal pattern of infestation, attachment sites and duration of feeding. Parasit. Vectors 2013, 6, 362. [Google Scholar] [CrossRef]
- Kortet, R.; Härkönen, L.; Hokkanen, P.; Härkönen, S.; Kaitala, A.; Kaunisto, S.; Ylönen, H. Experiments on the ectoparasitic deer ked that often attacks humans; preferences for body parts, colour and temperature. Bull. Entomol. Res. 2010, 100, 279–285. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Ixodes ricinus | Lipoptena cervi | |
|---|---|---|
| Most frequent localization on the human body | Lower extremities, chest, abdomen, and upper extremities in adult patients. In children, it’s the same as adults and additionally the head and neck as well as the genital area. | Upper body parts (most frequently the back of the head and neck). |
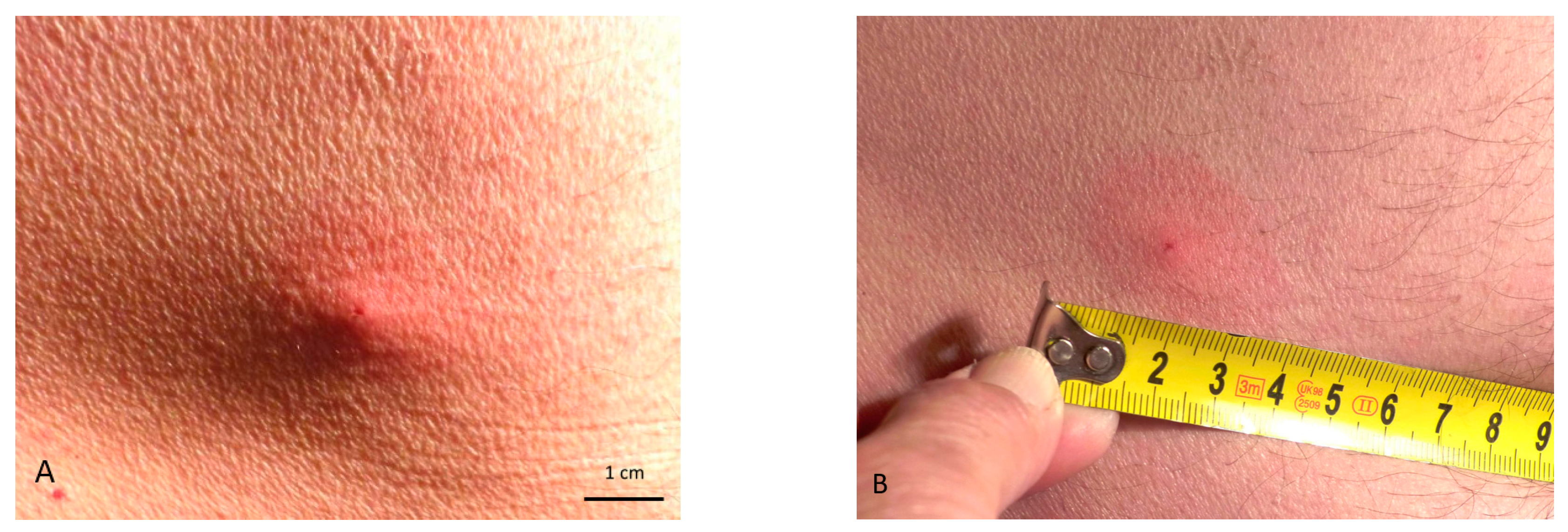
| Type of skin lesions | Clearly visible puncture; erythematous infiltrated non-demarcated lesions. | Invisible or poorly visible puncture; irregularly shaped scattered erythematous papules. |
| Symptoms of a bite and development of skin lesions | The bite is painless and non-itchy; after detachment of an engorged tick or mechanical removal, an itching, burning, or red spot may sometimes develop; inflammation usually resolves after a few days, but may last longer in sensitive individuals. | Pain and itching may appear immediately after the bite; skin lesions persist for a long time, from several weeks to a year. |
| Time of exposure to bites | Throughout the seasonal activity of nymphs and adult stages, mainly at its peaks (i.e., in May and September). | Period of activity of adult stages from September to December. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Buczek, W.; Buczek, A.M.; Bartosik, K.; Buczek, A. Comparison of Skin Lesions Caused by Ixodes ricinus Ticks and Lipoptena cervi Deer Keds Infesting Humans in the Natural Environment. Int. J. Environ. Res. Public Health 2020, 17, 3316. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17093316
Buczek W, Buczek AM, Bartosik K, Buczek A. Comparison of Skin Lesions Caused by Ixodes ricinus Ticks and Lipoptena cervi Deer Keds Infesting Humans in the Natural Environment. International Journal of Environmental Research and Public Health. 2020; 17(9):3316. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17093316
Chicago/Turabian StyleBuczek, Weronika, Alicja M. Buczek, Katarzyna Bartosik, and Alicja Buczek. 2020. "Comparison of Skin Lesions Caused by Ixodes ricinus Ticks and Lipoptena cervi Deer Keds Infesting Humans in the Natural Environment" International Journal of Environmental Research and Public Health 17, no. 9: 3316. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17093316