Physician-Delivered Pain Neuroscience Education for Opioid Tapering: A Case Report



Abstract
:1. Introduction
2. Case Report
3. Visit 1
4. Visits 2–7
5. Discussion
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- National Institute on Drug Abuse. Pain. Available online: https://www.drugabuse.gov/related-topics/pain (accessed on 5 March 2020).
- Dahlhamer, J.; Lucas, J.; Zelaya, C.; Nahin, R.; Mackey, S.; DeBar, L.; Kerns, R.; Von Korff, M.; Porter, L.; Helmick, C. Prevalence of Chronic Pain and High-Impact Chronic Pain Among Adults—United States, 2016. Morb. Mortal. Wkly. Rep. 2018, 67, 1001–1006. [Google Scholar] [CrossRef]
- Van Hecke, O.; Torrance, N.; Smith, B.H. Chronic pain epidemiology and its clinical relevance. Br. J. Anaesth. 2013, 111, 13–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dorner, T.E. Pain and chronic pain epidemiology. Wien. Klin. Wochenschr. 2018, 130, 1–3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palinkas, L.A. Opioid Use Epidemic in Mexico: Global Solutions to a Global Problem. Am. J. Public Health 2019, 109, 26–27. [Google Scholar] [CrossRef]
- Hoots, B.E.; Xu, L.; Kariisa, M.; Wilson, N.O.; Rudd, R.A.; Scholl, L.; Schieber, L.; Seth, P. 2018 Annual Surveillance Report of Drug-Related Risks and Outcomes—United States. CDC Natl. Cent. Inj. Prev. Control 2018. Available online: https://www.cdc.gov/drugoverdose/pdf/pubs/2018-cdc-drug-surveillance-report.pdf (accessed on 6 March 2020).
- Lee, M.; Silverman, S.M.; Hansen, H.; Patel, V.B.; Manchikanti, L. A comprehensive review of opioid-induced hyperalgesia. Pain Phys. 2011, 14, 145–161. [Google Scholar]
- Shah, A.; Hayes, C.J.; Martin, B.C. Characteristics of Initial Prescription Episodes and Likelihood of Long-Term Opioid Use—United States, 2006–2015. Morb. Mortal. Wkly. Rep. 2017, 66, 265–269. [Google Scholar] [CrossRef] [Green Version]
- Ballantyne, J.C.; LaForge, K.S. Opioid dependence and addiction during opioid treatment of chronic pain. Pain 2007, 129, 235–255. [Google Scholar] [CrossRef]
- American Society of Anesthesiologists Task Force on Chronic Pain Management; American Society of Regional Anesthesia; Pain, M. Practice guidelines for chronic pain management: An updated report by the American Society of Anesthesiologists Task Force on Chronic Pain Management and the American Society of Regional Anesthesia and Pain Medicine. Anesthesiology 2010, 112, 810–833. [Google Scholar]
- Malfliet, A.; Kregel, J.; Coppieters, I.; De Pauw, R.; Meeus, M.; Roussel, N.; Cagnie, B.; Danneels, L.; Nijs, J. Effect of Pain Neuroscience Education Combined With Cognition-Targeted Motor Control Training on Chronic Spinal Pain: A Randomized Clinical Trial. JAMA Neurol. 2018, 75, 808–817. [Google Scholar] [CrossRef]
- Vowles, K.E.; McEntee, M.L.; Julnes, P.S.; Frohe, T.; Ney, J.P.; van der Goes, D.N. Rates of opioid misuse, abuse, and addiction in chronic pain: A systematic review and data synthesis. Pain 2015, 156, 569–576. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mark, T.L.; Parish, W. Opioid medication discontinuation and risk of adverse opioid-related health care events. J. Subst. Abus. Treat. 2019, 103, 58–63. [Google Scholar] [CrossRef] [PubMed]
- Tennant, F. A Plea for Proper Opioid Tapering. Practical Pain. Available online: https://www.practicalpainmanagement.com/treatments/pharmacological/tapering/plea-proper-opioid-tapering (accessed on 28 December 2018).
- Kominek, C. What’s the safest, effective way to taper a patient off of opioid therapy? Pract. Pain Manag. 2018, 18, 5. [Google Scholar]
- Dowell, D.; Haegerich, T.M.; Chou, R. CDC Guideline for Prescribing Opioids for Chronic Pain—United States, 2016. MMWR Recomm. Rep. 2016, 65, 1–49. [Google Scholar] [CrossRef]
- Berna, C.; Kulich, R.J.; Rathmell, J.P. Tapering Long-term Opioid Therapy in Chronic Noncancer Pain: Evidence and Recommendations for Everyday Practice. Mayo Clin. Proc. 2015, 90, 828–842. [Google Scholar] [CrossRef] [Green Version]
- Atayde, E.R.; Britcher, R.; Chaffman, M.O.; Devlin, C.K.B.; Drexler, K.; Grief, W.; Hardin, J.; Kurihara, C.; Macedo, F.; Mardian, A.; et al. VA/DoD Clinical Practice Guideline for Opioid Therapy for Chronic Pain. Available online: https://www.healthquality.va.gov/guidelines/Pain/cot/VADoDOTCPG022717.pdf (accessed on 6 March 2020).
- Holden, J.E.; Jeong, Y.; Forrest, J.M. The endogenous opioid system and clinical pain management. AACN Clin. Issues 2005, 16, 291–301. [Google Scholar] [CrossRef]
- Ballantyne, J.C.; Sullivan, M.D. Discovery of endogenous opioid systems: What it has meant for the clinician’s understanding of pain and its treatment. Pain 2017, 158, 2290–2300. [Google Scholar] [CrossRef]
- Wertli, M.M.; Eugster, R.; Held, U.; Steurer, J.; Kofmehl, R.; Weiser, S. Catastrophizing-a prognostic factor for outcome in patients with low back pain: A systematic review. Spine J. 2014, 14, 2639–2657. [Google Scholar] [CrossRef]
- Benedetti, F.; Piedimonte, A. The neurobiological underpinnings of placebo and nocebo effects. Semin. Arthritis Rheum. 2019, 49, S18–S21. [Google Scholar] [CrossRef]
- Benedetti, F.; Thoen, W.; Blanchard, C.; Vighetti, S.; Arduino, C. Pain as a reward: Changing the meaning of pain from negative to positive co-activates opioid and cannabinoid systems. Pain 2013, 154, 361–367. [Google Scholar] [CrossRef]
- Louw, A.; Puentedura, E.J.; Diener, I.; Peoples, R.R. Preoperative therapeutic neuroscience education for lumbar radiculopathy: A single-case fMRI report. Physiother. Theory Pract. 2015, 31, 496–508. [Google Scholar] [CrossRef] [PubMed]
- Moseley, G.L. Widespread brain activity during an abdominal task markedly reduced after pain physiology education: fMRI evaluation of a single patient with chronic low back pain. Aust. J. Physiother. 2005, 51, 49–52. [Google Scholar] [CrossRef] [Green Version]
- Naugle, K.M.; Fillingim, R.B.; Riley, J.L., 3rd. A meta-analytic review of the hypoalgesic effects of exercise. J. Pain 2012, 13, 1139–1150. [Google Scholar] [CrossRef] [Green Version]
- Louw, A.; Vogsland, R.; Marth, L.; Marshall, P.; Cox, T.; Landers, M. Interdisciplinary Pain Neuroscience Continuing Education in the Veteran’s Affairs: Live Training and Live-Stream with 1-year Follow-up. Clin. J. Pain 2019, 35, 901–907. [Google Scholar] [CrossRef] [PubMed]
- Moseley, G.L. Evidence for a direct relationship between cognitive and physical change during an education intervention in people with chronic low back pain. Eur. J. Pain 2004, 8, 39–45. [Google Scholar] [CrossRef]
- Marris, D.; Theophanous, K.; Cabezon, P.; Dunlap, Z.; Donaldson, M. The impact of combining pain education strategies with physical therapy interventions for patients with chronic pain: A systematic review and meta-analysis of randomized controlled trials. Phys. Theory Pract. 2019, 28, 1–12. [Google Scholar] [CrossRef]
- Louw, A.; Zimney, K.; Puentedura, E.J.; Diener, I. The Efficacy of Therapeutic Neuroscience Education on Musculoskeletal Pain—A Systematic Review of the Literature. Physiother. Theory Pract. 2016, 32, 332–355. [Google Scholar] [CrossRef]
- Tegner, H.; Frederiksen, P.; Esbensen, B.A.; Juhl, C. Neurophysiological Pain Education for Patients with Chronic Low Back Pain: A Systematic Review and Meta-Analysis. Clin. J. Pain 2018, 34, 778–786. [Google Scholar] [CrossRef] [Green Version]
- Zimney, K.; Louw, A.; Johnson, J.; Peppers, S.; Farrell, K. Effects of Pain Science Education on Physician Assistant Students Understanding of Pain and Attitudes and Beliefs about Pain. S. D. Med. J. 2018, 71, 506–511. [Google Scholar]
- Liebenson, C.; Yeomans, S. Assessment of psychosocial risk factors for chronicity—“Yellow flags”. In Rehabilitation of the Spine: A Practitioners Manual, 2nd ed.; Liebenson, C., Ed.; Lippincott Williams & Wilkins: Baltimore, MD, USA, 2007; pp. 183–202. [Google Scholar]
- Smart, K.M.; Blake, C.; Staines, A.; Thacker, M.; Doody, C. Mechanisms-based classifications of musculoskeletal pain: Part 1 of 3: Symptoms and signs of central sensitisation in patients with low back (+/−leg) pain. Man. Ther. 2012, 17, 336–344. [Google Scholar] [CrossRef] [Green Version]
- Louw, A. Why Do I Hurt? A Neuroscience Approach to Pain; OPTP: Minneapolis, MN, USA, 2013. [Google Scholar]
- Butler, D.S.; Moseley, G.L. Explain Pain Supercharged; NOI Group: Adelaide, Australia, 2017. [Google Scholar]
- Louw, A. Why You Hurt: Therapeutic Neuroscience Education System; OPTP: Minneapolis, MN, USA, 2014. [Google Scholar]
- Nichols, V.P.; Toye, F.; Eldabe, S.; Sandhu, H.K.; Underwood, M.; Seers, K. Experiences of people taking opioid medication for chronic non-malignant pain: A qualitative evidence synthesis using meta-ethnography. BMJ Open 2020, 10, e032988. [Google Scholar] [CrossRef]
- Davis, M.P.; Digwood, G.; Mehta, Z.; McPherson, M.L. Tapering opioids: A comprehensive qualitative review. Ann. Palliat Med. 2020, 9, 586–610. [Google Scholar] [CrossRef] [PubMed]
- Davis, B.; Archambault, C.; Davis, K.; Oagley, C.; Schneider, J.; Kennedy, A.; Wilensky, D. A patient-centered approach to tapering opioids. J. Fam. Pract. 2019, 68, 548–556. [Google Scholar] [PubMed]
- Lembke, A. Tapering Long-Term Opioid Therapy. Am. Fam. Phys. 2020, 101, 49–52. [Google Scholar]
- Rubin, R. HHS Guide for Tapering or Stopping Long-term Opioid Use. JAMA 2019, 322, 1947. [Google Scholar] [CrossRef]
- Rubin, R. Limits on Opioid Prescribing Leave Patients With Chronic Pain Vulnerable. JAMA 2019, 321, 2059–2062. [Google Scholar] [CrossRef]
- Darnall, B.D.; Juurlink, D.; Kerns, R.D.; Mackey, S.; Van Dorsten, B.; Humphreys, K.; Gonzalez-Sotomayor, J.A.; Furlan, A.; Gordon, A.J.; Gordon, D.B.; et al. International Stakeholder Community of Pain Experts and Leaders Call for an Urgent Action on Forced Opioid Tapering. Pain Med. 2019, 20, 429–433. [Google Scholar] [CrossRef]
- Darnall, B.D.; Mackey, S.C.; Lorig, K.; Kao, M.C.; Mardian, A.; Stieg, R.; Porter, J.; DeBruyne, K.; Murphy, J.; Perez, L.; et al. Comparative Effectiveness of Cognitive Behavioral Therapy for Chronic Pain and Chronic Pain Self-Management within the Context of Voluntary Patient-Centered Prescription Opioid Tapering: The EMPOWER Study Protocol. Pain Med. 2019. [Google Scholar] [CrossRef] [Green Version]
- Pack, R.; Mpt, O.C.S.; Gilliland, R.P.; Mecham, A.D. The treatment of central sensitization in an adolescent using pain neuroscience education and graded exposure to activity: A case report. Physiother. Theory Pract. 2018. Available online: https://0-doi-org.brum.beds.ac.uk/10.1080/09593985.2018.1551454 (accessed on 6 March 2020). [CrossRef]
- Shepherd, M.P.T.; Louw, A.P.T.; Podolak, J.P.T. The clinical application of pain neuroscience, graded motor imagery, and graded activity with com plex regional pain syndrome—A case report. Physiother. Theory Pract. 2018, 1–13. Available online: https://0-doi-org.brum.beds.ac.uk/10.1080/09593985.2018.1548047 (accessed on 6 March 2020). [CrossRef]
- Sawyer, E.E.; McDevitt, A.W.; Louw, A.; Puentedura, E.J.; Mintken, P.E. Use of Pain Neuroscience Education, Tactile Discrimination, and Graded Motor Imagery in an Individual With Frozen Shoulder. J. Orthop. Sports Phys. Ther. 2018, 48, 174–184. [Google Scholar] [CrossRef] [PubMed]
- Louw, A.; Puentedura, E.L.; Mintken, P. Use of an abbreviated neuroscience education approach in the treatment of chronic low back pain: A case report. Physiother. Theory Pract. 2012, 28, 50–62. [Google Scholar] [CrossRef] [PubMed]
- Weller, J.; Boyd, M.; Cumin, D. Teams, tribes and patient safety: Overcoming barriers to effective teamwork in healthcare. Postgrad. Med. J. 2014, 90, 149–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Humphrey, K.; Brichko, L.; Cobbett, J. Breaking down the silos of medical error. Emerg. Med. Australas. 2019, 31, 659–661. [Google Scholar] [CrossRef] [PubMed]
- Nimmon, L.; Stenfors-Hayes, T. The “Handling” of power in the physician-patient encounter: Perceptions from experienced physicians. BMC Med. Educ. 2016, 16, 114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCullough, L.B. Physicians’ Professionally Responsible Power: A Core Concept of Clinical Ethics. J. Med. Philos. 2016, 41, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Louw, A.; Puentedura, E.J.; Zimney, K.; Cox, T.; Rico, D. The clinical implementation of pain neuroscience education: A survey study. Physiother. Theory Pract. 2017, 33, 869–879. [Google Scholar] [CrossRef]
- Hashmi, J.A.; Baliki, M.N.; Huang, L.; Baria, A.T.; Torbey, S.; Hermann, K.M.; Schnitzer, T.J.; Apkarian, A.V. Shape shifting pain: Chronification of back pain shifts brain representation from nociceptive to emotional circuits. Brain A J. Neurol. 2013, 136, 2751–2768. [Google Scholar] [CrossRef] [Green Version]
- Benedetti, F. Placebo and the new physiology of the doctor-patient relationship. Physiol. Rev. 2013, 93, 1207–1246. [Google Scholar] [CrossRef]
- White, R.; Hayes, C.; White, S.; Hodson, F.J. Using social media to challenge unwarranted clinical variation in the treatment of chronic noncancer pain: The “Brainman” story. J. Pain Res. 2016, 9, 701–709. [Google Scholar]
- Louw, A.; Zimney, K.; Johnson, E.A.; Kraemer, C.; Fesler, J.; Burcham, T. De-educate to re-educate: Aging and low back pain. Aging Clin. Exp. Res. 2017, 29, 1261–1269. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Pain (Q 1) | Health Confidence (Qs 3, 4, 6 and 8) | Fear-Avoidance (Qs 9, 11, 12 and 13) | Emotional (Qs 5, 7 and 10) | Total Score (All 13 Qs) * | |
|---|---|---|---|---|---|
| (0–10) | (0–40) | (0–40) | (0–30) | (0–130) | |
| Initial Visit— | 7 | 21 | 18 | 15 | 65 |
| Final Visit—9 months | 3 | 8 | 10 | 5 | 26 |
| Visit | Information | Treatment |
|---|---|---|
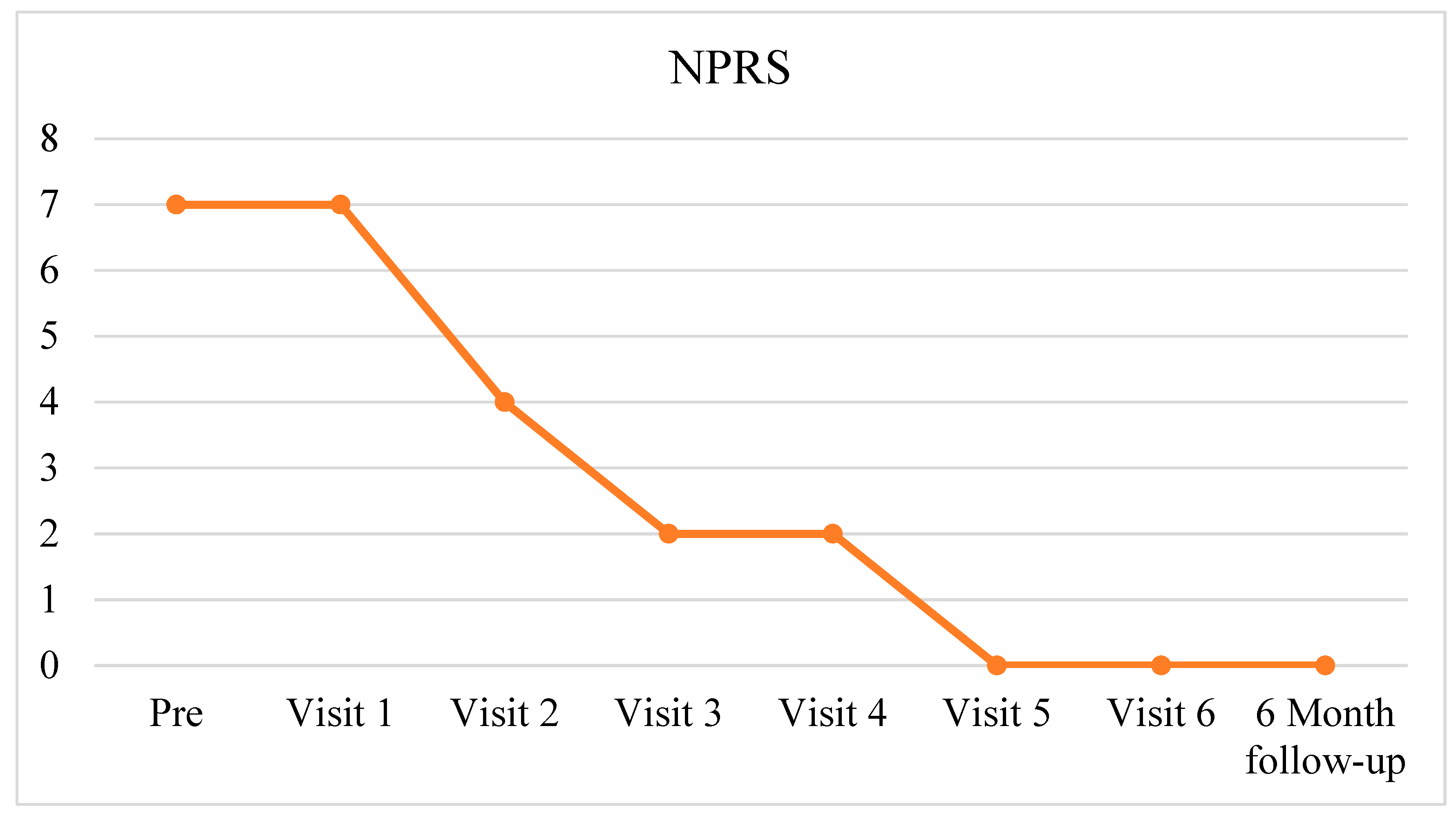
| 1 | Follow-up visit 5 days after discharge from hospital Nausea improved Willing to talk about her CLBP and opioid use “What do you think is going on with your back?”
| Education about the normal anatomical changes and aging of her low back
|
| 2 (5 days later) | Follow-up visit LBP 4/10 Completed her sensitive nerves and yellow flags homework Her questions at follow-up:
| Review content from session 1 and HEP Discussion of list of opioid side effects and identified those she was suffering from PNE for weather changes and pain:
Cognitive homework:
|
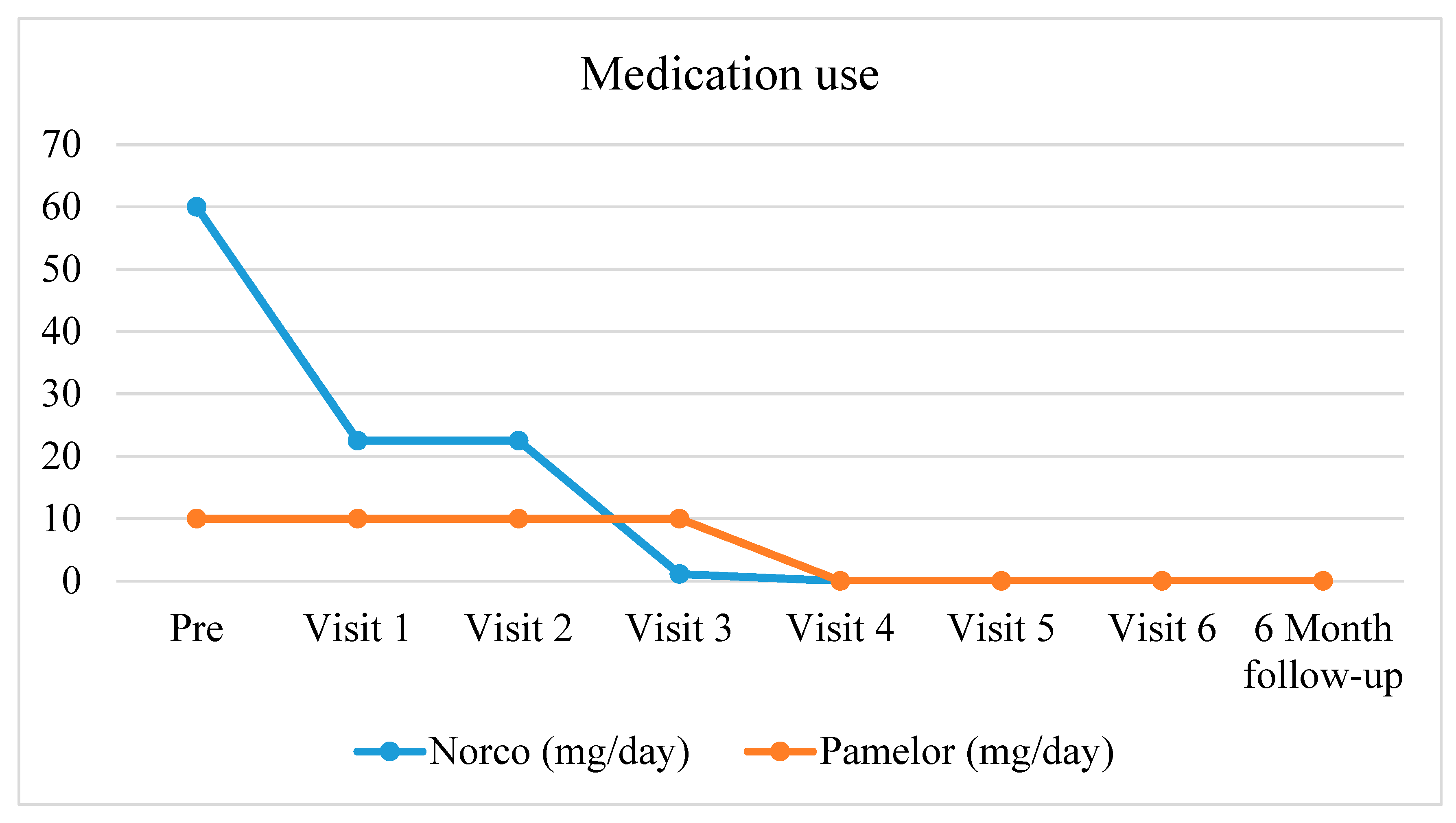
| 3 (9 days later) | Review side-effects of opioids reflection Over the last 3 weeks she has only taken 3 Norco and has done fairly well
| Review content from session 2 and HEP PNE: Explain Pain Supercharged nuggets
Cognitive Homework:
|
| 4 (7 days later) | Follow-up Done her homework States she is “better than before”—pain and outlook towards life is improved Not been taking any Norco Food tastes better Dry mouth continues to improve Does not feel as “groggy” as before—“more in tune with people” around her Realizing she was staying more at home—deliberately trying to go out more LBP 2/10 Discontinued Colace since she was no longer constipated Pamelor (nortriptyline) 10mg (anti-depressant) nightly discontinued See her again in 2 weeks | Review content from session 3 and HEP Additional education—myths about LBP:
|
| 5 (14 days later) | Follow-up Reports no pain “Frustration and stress make me uncomfortable in my back”—does not use the “P” word anymore Reports no problem with discharging her Pamelor No constipation anymore She discontinued her Prilosec since she’s not having any heartburn anymore | Review content from sessions 1-4 Reflect on PNE and application to her specific presentation of CLBP Questions/answers |
| 6 (7 weeks later) | Follow-up Off Norco for a few months No pain—feels much better Much more active More energy Had a slight flare recently but did not freak out and no medicine, including over the counter medicine No heartburn; no abdominal pain Improved mood; not anxious or depressed; no sleep disturbance LBP 0/10 Patient brought all her prescription and OTC medicines to the clinic—review all medicines and update her current medication list in the medical records to reflect the changes Follow-up in 6 months | Review content from sessions 1-5 Reflect on PNE and application to her specific presentation of CLBP Questions/answers |
| 7 (6 months later) | Follow-up Continued all opioid medications Little to no pain experienced Still active and feeling energetic Patient Reported Outcome measures:
|
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Agarwal, V.; Louw, A.; Puentedura, E.J. Physician-Delivered Pain Neuroscience Education for Opioid Tapering: A Case Report. Int. J. Environ. Res. Public Health 2020, 17, 3324. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17093324
Agarwal V, Louw A, Puentedura EJ. Physician-Delivered Pain Neuroscience Education for Opioid Tapering: A Case Report. International Journal of Environmental Research and Public Health. 2020; 17(9):3324. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17093324
Chicago/Turabian StyleAgarwal, Vikas, Adriaan Louw, and Emilio J. Puentedura. 2020. "Physician-Delivered Pain Neuroscience Education for Opioid Tapering: A Case Report" International Journal of Environmental Research and Public Health 17, no. 9: 3324. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17093324