Hand-Washing Practices among Adolescents Aged 12–15 Years from 80 Countries

 ,
,  , , ,
, , ,  ,
,  , ,
, ,  and
and
Abstract
:1. Introduction
2. Methods
2.1. Hand-Washing Practices
2.2. Food Insecurity (Proxy of Socioeconomic Status)
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A



References
- Rabie, T.; Curtis, V. Handwashing and risk of respiratory infections: A quantitative systematic review. Trop. Med. Int. Health 2006, 11, 258–267. [Google Scholar] [CrossRef] [PubMed]
- Aiello, A.E.; Coulborn, R.M.; Perez, V.; Larson, E.L. Effect of hand hygiene on infectious disease risk in the community setting: A meta-analysis. Am. J. Public Health 2008, 98, 1372–1381. [Google Scholar] [CrossRef] [PubMed]
- Freeman, M.C.; Stocks, M.E.; Cumming, O.; Jeandron, A.; Higgins, J.P.; Wolf, J.; Prüss-Ustün, A.; Bonjour, S.; Hunter, P.R.; Fewtrell, L.; et al. Systematic review: Hygiene and health: Systematic review of handwashing practices worldwide and update of health effects. Trop. Med. Int. Health 2014, 19, 906–916. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cairncross, S.; Hunt, C.; Boisson, S.; Bostoen, K.; Curtis, V.; Fung, I.C.; Schmidt, W.P. Water, sanitation and hygiene for the prevention of diarrhoea. Int. J. Epidemiol. 2010, 39, i193–i205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolf, J.; Hunter, P.R.; Freeman, M.C.; Cumming, O.; Clasen, T.; Bartram, J.; Higgins, J.P.; Johnston, R.; Medlicott, K.; Boisson, S.; et al. Impact of drinking water, sanitation and handwashing with soap on childhood diarrhoeal disease: Updated meta-analysis and meta-regression. Trop. Med. Int. Health 2018, 23, 508–525. [Google Scholar] [CrossRef] [PubMed]
- Johns Hopkins University & Medicine. Coronavirus Resource Centre. Available online: https://0-coronavirus-jhu-edu.brum.beds.ac.uk/map.html (accessed on 28 November 2020).
- World Health Organization. Coronavirus Disease Advice for the Public. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/advice-for-public (accessed on 28 November 2020).
- Wolf, J.; Johnston, R.; Freeman, M.C.; Ram, P.K.; Slaymaker, T.; Laurenz, E.; Prüss-Ustün, A. Handwashing with soap after potential faecal contact: Global, regional and country estimates. Int. J. Epidemiol. 2019, 48, 1204–1218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luby, S.P.; Halder, A.K. Associations among handwashing indicators, wealth, and symptoms of childhood respiratory illness in urban Bangladesh: Handwashing indicators, wealth, and symptoms of childhood respiratory illness. Trop. Med. Int. Health 2008, 13, 835–844. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, W.P.; Aunger, R.; Coombes, Y.; Maina, P.M.; Matiko, C.N.; Biran, A.; Curtis, V. Determinants of handwashing practices in Kenya: The role of media exposure, poverty and infrastructure. Trop. Med. Int. Health 2009, 14, 1534–1541. [Google Scholar] [CrossRef] [PubMed]
- Dobe, M.; Mandal, R.N.; Ayan, J.H.A. Social Determinants of Good Hand-Washing Practice (GHP) Among Adolescents in a Rural Indian Community. Fam. Community Health 2013, 36, 172–177. [Google Scholar] [CrossRef] [PubMed]
- Rabbi, S.E.; Dey, N.C. Exploring the gap between hand washing knowledge and practices in Bangladesh: A cross-sectional comparative study. BMC Public Health 2013, 13, 89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Institute on Ageing. World’s Older Population Grows Dramatically. Available online: https://www.nih.gov/news-events/news-releases/worlds-older-population-grows-dramatically (accessed on 28 November 2020).
- Smith, D.; Inskip, P.E. Adolescent infectious disease challenges. Adolesc. Med. 2000, 11, 211–224. [Google Scholar] [PubMed]
- Brener, N.D.; Collins, J.L.; Kann, L.; Warren, C.W.; Williams, B.I. Reliability of the Youth Risk Behavior Survey Questionnaire. Am. J. Epidemiol. 1995, 141, 575–580. [Google Scholar] [CrossRef] [PubMed]
- McKittrick, T.; Jacobsen, K. Oral Hygiene and Handwashing Practices among Middle-School Students in 15 Latin American and Caribbean Countries. West Indian Med. J. 2015, 64, 266–268. [Google Scholar] [PubMed] [Green Version]
- Jacob, L.; Stubbs, B.; Koyanagi, A. Consumption of carbonated soft drinks and suicide attempts among 105,061 adolescents aged 12–15 years from 6 high-income, 22 middle-income, and 4 low-income countries. Clin. Nutr. 2020, 39, 886–892. [Google Scholar] [CrossRef] [PubMed]
- Koyanagi, A.; Stubbs, B.; Oh, H.; Veronese, N.; Smith, L.; Haro, J.M.; Vancampfort, D. Food insecurity (hunger) and suicide attempts among 179,771 adolescents attending school from 9 high-income, 31 middle-income, and 4 low-income countries: A cross-sectional study. J. Affect. Disord. 2019, 248, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jemal, S. Knowledge and Practices of Hand Washing among Health Professionals in Dubti Referral Hospital, Dubti, Afar, Northeast Ethiopia. Adv. Prev. Med. 2018, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bulled, N.; Poppe, K.; Ramatsisti, K.; Sitsula, L.; Winegar, G.; Gumbo, J.; Dillingham, R.; Smith, J. Assessing the environmental context of hand washing among school children in Limpopo, South Africa. Water Int. 2017, 42, 568–584. [Google Scholar] [CrossRef] [PubMed]
- UNICEF. No Soap, No Water: Billions Lack Basic Protection Against Virus. Available online: http://www.rfi.fr/en/wires/20200319-no-soap-no-water-billions-lack-basic-protection-against-virus (accessed on 28 November 2020).
- Martinez-Alvarez, M.; Jarde, A.; Usuf, E.; Brotherton, H.; Bittaye, M.; Samateh, A.L.; Antonio, M.; Vives-Tomas, J.; D’Alessandro, U.; Roca, A. COVID-19 pandemic in west Africa. Lancet Glob. Health 2020, 8, 1–2. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Country-Income | Country | Year | Response Rate (%) | N a | Male (%) | Age (Years) Mean (SD) |
|---|---|---|---|---|---|---|
| Low | Afghanistan | 2014 | 79 | 1493 | 53.4 | 14.0 (0.9) |
| Benin | 2016 | 78 | 717 | 65.6 | 14.2 (0.9) | |
| Cambodia | 2013 | 85 | 1812 | 48.4 | 14.1 (0.8) | |
| Kenya | 2003 | 84 | 2971 | 47.5 | 13.9 (1.0) | |
| Liberia | 2017 | 71 | 541 | 50.1 | 14.0 (0.9) | |
| Malawi | 2009 | 94 | 2224 | 51.5 | 14.0 (0.8) | |
| Mozambique | 2015 | 80 | 668 | 49.6 | 14.1 (0.8) | |
| Nepal | 2015 | 69 | 4616 | 47.3 | 13.8 (1.0) | |
| Senegal | 2005 | 60 | 2666 | 60.2 | 13.9 (1.0) | |
| Tanzania | 2014 | 87 | 2615 | 46.8 | 13.6 (1.0) | |
| Uganda | 2003 | 69 | 1904 | 47.4 | 14.3 (0.8) | |
| Zambia | 2004 | 70 | 1365 | 50.3 | 13.9 (1.0) | |
| Low middle | Bangladesh | 2014 | 91 | 2753 | 63.4 | 14.0 (0.8) |
| Belize | 2011 | 88 | 1600 | 48.4 | 13.6 (1.1) | |
| Bolivia | 2012 | 88 | 2804 | 49.7 | 14.0 (0.9) | |
| Djibouti | 2007 | 83 | 962 | 59.5 | 14.3 (0.8) | |
| East Timor | 2015 | 79 | 1631 | 46.3 | 14.1 (1.0) | |
| Egypt | 2011 | 85 | 2364 | 49.2 | 13.5 (0.9) | |
| El Salvador | 2013 | 88 | 1615 | 50.6 | 14.0 (0.9) | |
| Eswatini | 2013 | 97 | 1318 | 39.1 | 14.1 (0.8) | |
| Ghana | 2012 | 82 | 1110 | 49.1 | 13.8 (1.0) | |
| Guatemala | 2015 | 82 | 3611 | 50.9 | 13.9 (0.9) | |
| Guyana | 2010 | 76 | 1973 | 48.6 | 14.1 (0.8) | |
| Honduras | 2012 | 79 | 1486 | 46.1 | 13.6 (1.0) | |
| India | 2007 | 83 | 7330 | 57.4 | 13.9 (0.9) | |
| Indonesia | 2015 | 94 | 8806 | 49.2 | 13.5 (1.0) | |
| Jordan | 2007 | 99.8 | 1648 | 47.3 | 14.3 (0.7) | |
| Kiribati | 2011 | 85 | 1340 | 45.5 | 14.0 (0.9) | |
| Laos | 2015 | 70 | 1644 | 47.8 | 14.5 (0.8) | |
| Maldives | 2009 | 80 | 1981 | 47.9 | 14.4 (0.7) | |
| Mauritania | 2010 | 70 | 1285 | 53.2 | 14.2 (0.9) | |
| Mongolia | 2013 | 88 | 3707 | 49.4 | 13.7 (1.0) | |
| Morocco | 2016 | 91 | 3975 | 50.9 | 13.6 (1.1) | |
| Myanmar | 2016 | 86 | 2237 | 46.3 | 13.6 (0.9) | |
| Northern Macedonia | 2007 | 93 | 1550 | 51.6 | 13.9 (0.9) | |
| Pakistan | 2009 | 76 | 4998 | 60.8 | 14.1 (0.8) | |
| Philippines | 2015 | 79 | 6162 | 48.1 | 13.9 (0.9) | |
| Samoa | 2011 | 79 | 2200 | 47.4 | 14.0 (0.8) | |
| Solomon Islands | 2011 | 85 | 925 | 52.1 | 14.1 (0.9) | |
| Sri Lanka | 2016 | 89 | 2254 | 49.3 | 13.9 (0.9) | |
| Sudan | 2012 | 77 | 1401 | 51.9 | 14.2 (0.8) | |
| Syria | 2010 | 97 | 2929 | 51.2 | 13.6 (1.0) | |
| Tunisia | 2008 | 83 | 2549 | 49.7 | 13.6 (1.0) | |
| Vanuatu | 2016 | 57 | 1288 | 47.8 | 14.1 (0.9) | |
| Vietnam | 2013 | 96 | 1743 | 46.6 | 14.5 (0.6) | |
| Yemen | 2014 | 75 | 1553 | 56.3 | 13.8 (1.0) | |
| Upper middle | Algeria | 2011 | 98 | 3484 | 45.8 | 13.6 (1.1) |
| Antigua & Barbuda | 2009 | 67 | 1235 | 51.4 | 13.9 (0.9) | |
| Argentina | 2012 | 71 | 21,528 | 47.7 | 13.9 (0.9) | |
| Botswana | 2005 | 95 | 1397 | 46.2 | 14.3 (0.8) | |
| Costa Rica | 2009 | 72 | 2265 | 49.6 | 14.0 (0.9) | |
| Dominican Republic | 2016 | 63 | 954 | 48.6 | 14.3 (1.0) | |
| Grenada | 2008 | 78 | 1299 | 42.7 | 13.7 (1.1) | |
| Iraq | 2012 | 88 | 1533 | 54.7 | 13.9 (1.0) | |
| Lebanon | 2017 | 82 | 3347 | 47.4 | 13.6 (1.0) | |
| Libya | 2007 | 98 | 1891 | 49.2 | 13.6 (1.0) | |
| Malaysia | 2012 | 89 | 16,273 | 49.5 | 14.0 (0.9) | |
| Mauritius | 2017 | 84 | 1955 | 45.8 | 13.9 (0.8) | |
| Namibia | 2013 | 89 | 1936 | 42.9 | 14.1 (0.9) | |
| Paraguay | 2017 | 87 | 1972 | 47.5 | 13.9 (1.0) | |
| Peru | 2010 | 85 | 2359 | 49.9 | 14.1 (0.8) | |
| St. Lucia | 2007 | 82 | 1072 | 44.5 | 13.7 (1.1) | |
| St. Vincent & the Grenadines | 2007 | 84 | 1188 | 46.2 | 13.5 (1.0) | |
| Suriname | 2016 | 83 | 1453 | 46.1 | 13.8 (1.0) | |
| Thailand | 2015 | 89 | 4132 | 49.6 | 13.7 (1.0) | |
| Tonga | 2017 | 90 | 2067 | 51.4 | 13.6 (1.1) | |
| Tuvalu | 2013 | 90 | 679 | 48.9 | 13.3 (1.1) | |
| High | Bahamas | 2013 | 78 | 1308 | 47.3 | 13.4 (1.0) |
| Barbados | 2011 | 73 | 1504 | 51.1 | 14.1 (0.8) | |
| Brunei Darussalam | 2014 | 65 | 1824 | 48.2 | 14.0 (0.9) | |
| Cayman Islands | 2007 | 79 | 1147 | 52.0 | 13.5 (1.0) | |
| Curaçao | 2015 | 83 | 1498 | 49.8 | 13.9 (1.1) | |
| French Polynesia | 2015 | 70 | 1902 | 49.7 | 13.7 (1.0) | |
| Kuwait | 2015 | 78 | 2034 | 49.4 | 14.1 (0.9) | |
| Oman | 2015 | 92 | 1669 | 47.1 | 14.2 (0.8) | |
| Qatar | 2011 | 87 | 1781 | 47.2 | 13.4 (1.0) | |
| St. Kitts & Nevis | 2011 | 70 | 1471 | 50.2 | 14.1 (0.8) | |
| Trinidad & Tobago | 2017 | 89 | 2763 | 48.3 | 13.6 (1.1) | |
| United Arab Emirates | 2016 | 80 | 3471 | 48.1 | 13.9 (1.0) | |
| Uruguay | 2012 | 77 | 2869 | 46.3 | 14.1 (0.8) |
| Country-Income | Country | % | 95%CI | % | 95%CI | % | 95%CI |
|---|---|---|---|---|---|---|---|
| Low | Afghanistan | 6.0 | [4.4,8.2] | 5.6 | [3.6,8.6] | 11.6 | [8.0,16.6] |
| Benin | 6.4 | [4.3,9.2] | 10.6 | [5.6,19.2] | 18.5 | [13.2,25.3] | |
| Cambodia | 2.1 | [1.5,3.0] | 3.0 | [2.2,4.2] | 2.9 | [2.2,3.7] | |
| Kenya | 8.6 | [7.0,10.5] | 13.9 | [11.9,16.1] | 16.6 | [14.1,19.5] | |
| Liberia | 12.3 | [9.2,16.4] | 6.3 | [4.1,9.6] | 9.6 | [6.9,13.3] | |
| Malawi | 4.1 | [2.2,7.6] | 5.3 | [3.3,8.4] | 16.7 | [13.5,20.4] | |
| Mozambique | 7.4 | [4.9,11.1] | 7.8 | [4.9,12.1] | 11.7 | [7.1,18.7] | |
| Nepal | 4.0 | [2.8,5.7] | 4.4 | [3.3,5.8] | 4.8 | [3.8,6.2] | |
| Senegal | 10.2 | [4.9,20.0] | 10.0 | [4.8,19.7] | 14.7 | [9.4,22.4] | |
| Tanzania | 7.3 | [6.1,8.7] | 17.3 | [14.3,20.8] | 20.7 | [18.2,23.4] | |
| Uganda | 6.3 | [5.0,8.0] | 8.0 | [6.1,10.5] | 14.7 | [12.2,17.7] | |
| Zambia | 12.5 | [10.3,15.1] | 15.4 | [12.9,18.3] | 20.8 | [18.1,23.8] | |
| Lower middle | Bangladesh | 3.1 | [1.8,5.2] | 1.9 | [0.8,4.4] | 5.0 | [2.8,8.6] |
| Belize | 3.7 | [3.1,4.4] | 1.6 | [1.2,2.2] | 4.6 | [3.6,5.8] | |
| Bolivia | 10.8 | [9.4,12.4] | 7.3 | [6.1,8.7] | 16.0 | [13.8,18.5] | |
| Djibouti | 6.0 | [4.6,7.7] | 12.9 | [11.4,14.6] | 11.7 | [9.4,14.5] | |
| East Timor | 20.9 | [18.8,23.2] | 27.5 | [24.5,30.8] | 18.9 | [16.4,21.6] | |
| Egypt | 12.9 | [10.5,15.7] | 9.3 | [6.9,12.5] | 7.8 | [5.7,10.6] | |
| El Salvador | 5.3 | [4.1,6.8] | 4.0 | [2.7,6.1] | 5.7 | [4.5,7.3] | |
| Eswatini | 3.6 | [2.3,5.5] | 2.8 | [2.3,3.5] | 11.6 | [10.0,13.4] | |
| Ghana | 7.5 | [4.6,12.2] | 7.8 | [5.0,11.8] | 10.6 | [8.6,13.1] | |
| Guatemala | 4.5 | [2.8,7.1] | 2.7 | [1.5,4.7] | 5.7 | [4.2,7.6] | |
| Guyana | 9.2 | [7.4,11.3] | 6.4 | [4.8,8.4] | 10.7 | [8.5,13.3] | |
| Honduras | 7.5 | [6.4,8.7] | 5.2 | [4.0,6.7] | 58.6 | [54.9,62.3] | |
| India | 5.9 | [5.0,7.1] | 3.3 | [2.7,4.1] | 13.0 | [11.4,14.7] | |
| Indonesia | 2.5 | [2.0,3.0] | 2.3 | [1.8,2.9] | 3.9 | [3.3,4.7] | |
| Jordan | 6.8 | [5.5,8.3] | 7.0 | [5.0,9.7] | 9.2 | [7.4,11.5] | |
| Kiribati | 20.6 | [16.3,25.7] | 16.1 | [13.1,19.5] | 15.4 | [13.2,17.9] | |
| Laos | 1.9 | [1.1,3.2] | 3.8 | [2.5,5.9] | 8.5 | [6.7,10.7] | |
| Maldives | 8.5 | [7.1,10.1] | 4.7 | [3.7,5.8] | 7.2 | [5.9,8.8] | |
| Mauritania | 7.6 | [6.2,9.2] | 24.4 | [17.8,32.4] | 12.1 | [9.4,15.6] | |
| Mongolia | 6.9 | [5.9,8.0] | 10.5 | [8.9,12.3] | 3.0 | [2.4,3.8] | |
| Morocco | 4.8 | [4.1,5.5] | 6.2 | [5.1,7.6] | 10.4 | [8.6,12.5] | |
| Myanmar | 6.7 | [5.5,8.2] | 8.4 | [6.8,10.4] | 5.8 | [4.7,7.1] | |
| Northern Macedonia | 2.1 | [1.5,3.0] | 2.1 | [1.4,3.2] | 3.8 | [2.7,5.3] | |
| Pakistan | 3.4 | [2.7,4.4] | 3.4 | [2.5,4.6] | 8.0 | [6.3,10.2] | |
| Philippines | 7.7 | [4.9,11.8] | 6.3 | [3.9,10.0] | 7.9 | [5.4,11.5] | |
| Samoa | 14.6 | [12.9,16.4] | 17.1 | [14.9,19.5] | 19.3 | [17.1,21.7] | |
| Solomon Islands | 8.6 | [7.2,10.2] | 8.9 | [6.9,11.5] | 10.3 | [7.4,14.0] | |
| Sri Lanka | 2.7 | [1.9,3.9] | 3.0 | [2.1,4.1] | 7.1 | [5.6,9.0] | |
| Sudan | 7.5 | [6.0,9.4] | 11.9 | [9.9,14.1] | 20.9 | [16.7,25.9] | |
| Syria | 9.2 | [7.5,11.3] | 3.8 | [2.5,5.8] | 6.7 | [5.1,8.8] | |
| Tunisia | 6.0 | [5.2,6.9] | 4.0 | [3.2,4.9] | 4.7 | [3.7,5.9] | |
| Vanuatu | 4.2 | [3.3,5.5] | 5.1 | [3.9,6.6] | 6.4 | [5.1,8.1] | |
| Vietnam | 7.0 | [5.4,9.0] | 2.2 | [1.5,3.3] | 8.5 | [6.5,10.9] | |
| Yemen | 7.2 | [5.1,10.1] | 11.2 | [9.6,13.0] | 15.3 | [12.7,18.4] | |
| Upper middle | Algeria | 5.6 | [4.9,6.4] | 3.1 | [2.5,3.8] | 5.1 | [4.4,5.8] |
| Antigua & Barbuda | 12.2 | [10.5,14.2] | 5.1 | [3.9,6.7] | 7.1 | [5.7,8.9] | |
| Argentina | 11.2 | [10.1,12.4] | 5.9 | [5.0,7.0] | 6.2 | [5.5,7.1] | |
| Botswana | 4.5 | [3.3,6.1] | 5.1 | [4.3,6.2] | 17.0 | [13.9,20.7] | |
| Costa Rica | 9.6 | [8.3,11.1] | 2.2 | [1.7,2.8] | 5.4 | [4.5,6.5] | |
| Dominica | 14.1 | [10.1,19.2] | 5.3 | [3.7,7.7] | 8.6 | [5.8,12.6] | |
| Grenada | 11.4 | [9.5,13.6] | 3.5 | [2.8,4.4] | 10.1 | [8.4,12.1] | |
| Iraq | 7.3 | [5.6,9.6] | 8.1 | [6.3,10.3] | 4.0 | [3.0,5.4] | |
| Lebanon | 4.1 | [3.3,5.0] | 1.6 | [1.1,2.4] | 2.2 | [1.9,2.7] | |
| Libya | 8.1 | [6.3,10.4] | 6.8 | [5.5,8.5] | 7.4 | [5.9,9.1] | |
| Malaysia | 5.0 | [4.5,5.6] | 6.0 | [5.3,6.7] | 13.6 | [12.7,14.6] | |
| Mauritius | 13.9 | [11.1,17.4] | 4.0 | [2.7,6.0] | 8.2 | [6.1,10.8] | |
| Namibia | 5.5 | [4.4,6.8] | 6.4 | [5.1,8.0] | 10.8 | [8.8,13.1] | |
| Paraguay | 8.0 | [6.6,9.7] | 2.6 | [1.9,3.5] | 6.1 | [5.0,7.4] | |
| Peru | 4.9 | [3.8,6.2] | 6.6 | [5.5,7.9] | 7.5 | [6.0,9.4] | |
| St. Lucia | 16.5 | [14.0,19.3] | 4.4 | [3.4,5.6] | 11.1 | [9.1,13.4] | |
| St. Vincent & the Grenadines | 8.7 | [6.7,11.3] | 4.1 | [3.0,5.5] | 8.3 | [6.6,10.3] | |
| Suriname | 11.2 | [8.8,14.2] | 4.3 | [3.0,6.1] | 8.1 | [6.7,9.9] | |
| Thailand | 14.9 | [12.5,17.7] | 6.5 | [5.4,7.9] | 14.4 | [12.3,16.9] | |
| Tonga | 14.9 | [12.9,17.0] | 7.8 | [6.5,9.4] | 20.2 | [18.2,22.4] | |
| Tuvalu | 38.5 | [34.9,42.4] | 17.7 | [15.0,20.8] | 18.0 | [15.2,21.0] | |
| High | Bahamas | 15.6 | [13.5,18.0] | 4.5 | [3.4,5.8] | 8.7 | [7.2,10.4] |
| Barbados | 14.3 | [11.9,17.1] | 1.7 | [1.2,2.5] | 7.9 | [6.4,9.7] | |
| Brunei Darussalam | 3.5 | [2.7,4.5] | 2.9 | [1.9,4.4] | 9.7 | [8.1,11.5] | |
| Cayman Islands | 10.8 | [9.1,12.8] | 4.4 | [3.4,5.8] | 5.9 | [4.7,7.5] | |
| Curaçao | 12.2 | [10.2,14.4] | 3.6 | [2.6,4.8] | 6.5 | [5.1,8.3] | |
| French Polynesia | 8.4 | [6.5,10.7] | 5.7 | [4.2,7.8] | 11.5 | [9.8,13.6] | |
| Kuwait | 10.7 | [9.0,12.7] | 6.2 | [4.8,8.0] | 7.4 | [5.6,9.8] | |
| Oman | 7.9 | [5.9,10.4] | 8.8 | [6.8,11.2] | 7.4 | [5.6,9.8] | |
| Qatar | 17.0 | [13.8,20.8] | 15.1 | [12.3,18.4] | 16.4 | [13.0,20.4] | |
| St. Kitts & Nevis | 11.6 | [10.1,13.4] | 2.9 | [2.1,3.9] | 6.7 | [5.5,8.1] | |
| Trinidad & Tobago | 14.7 | [12.9,16.7] | 3.5 | [2.2,5.5] | 11.7 | [9.4,14.5] | |
| United Arab Emirates | 8.1 | [6.9,9.6] | 3.2 | [2.5,4.3] | 4.3 | [3.5,5.3] | |
| Uruguay | 12.5 | [10.8,14.5] | 6.9 | [5.5,8.5] | 3.6 | [2.7,4.8] |
| Outcome | Country-Income | OR (95%CI) | I2 (%) |
|---|---|---|---|
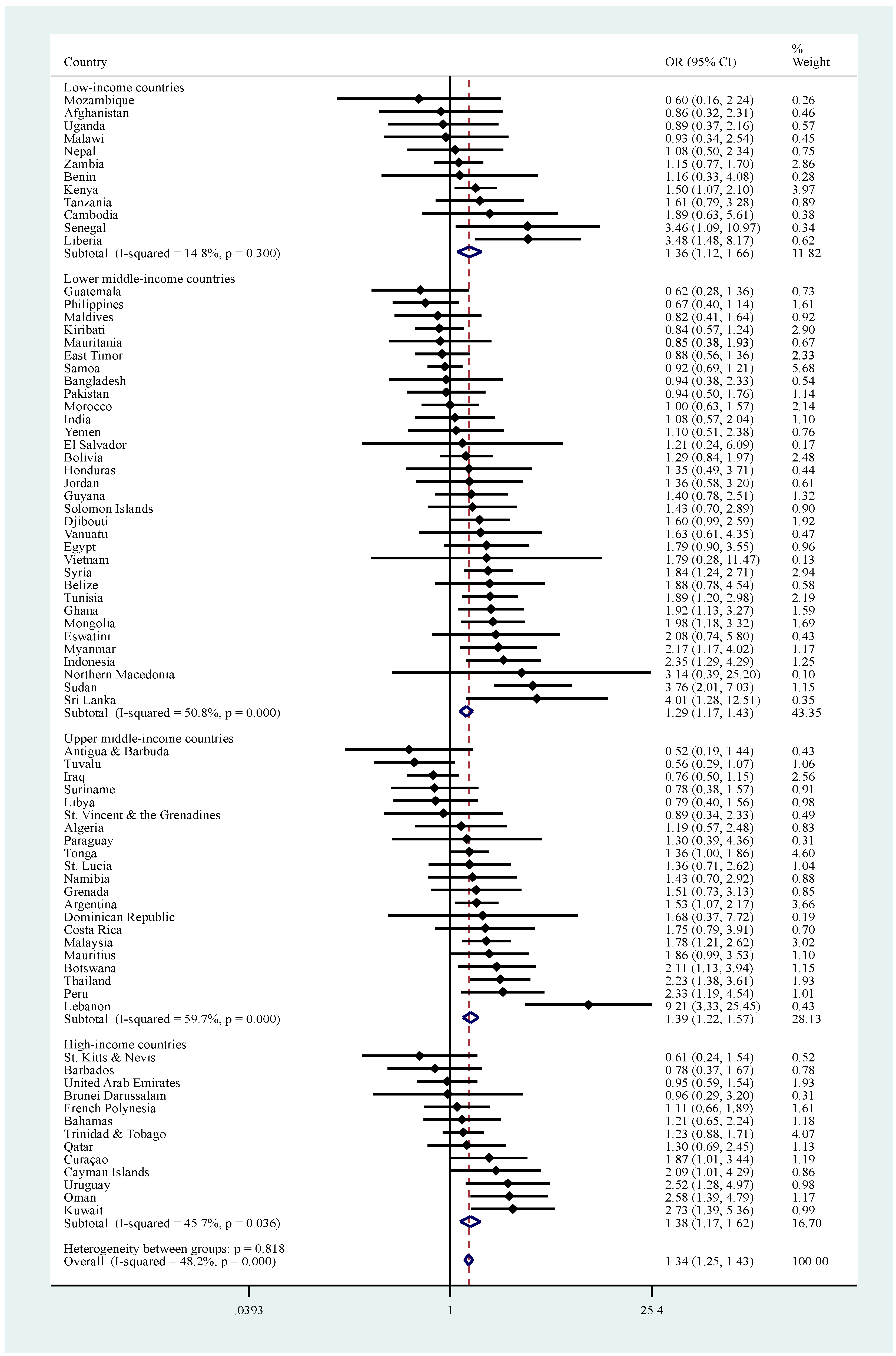
| Before eating | Low | 1.36 [1.12,1.66] | 14.8 |
| Lower middle a | 1.29 [1.17,1.43] | 50.8 | |
| Upper middle | 1.39 [1.22,1.57] | 59.7 | |
| High | 1.38 [1.17,1.62] | 45.7 | |
| Overall | 1.34 [1.25,1.43] | 48.2 | |
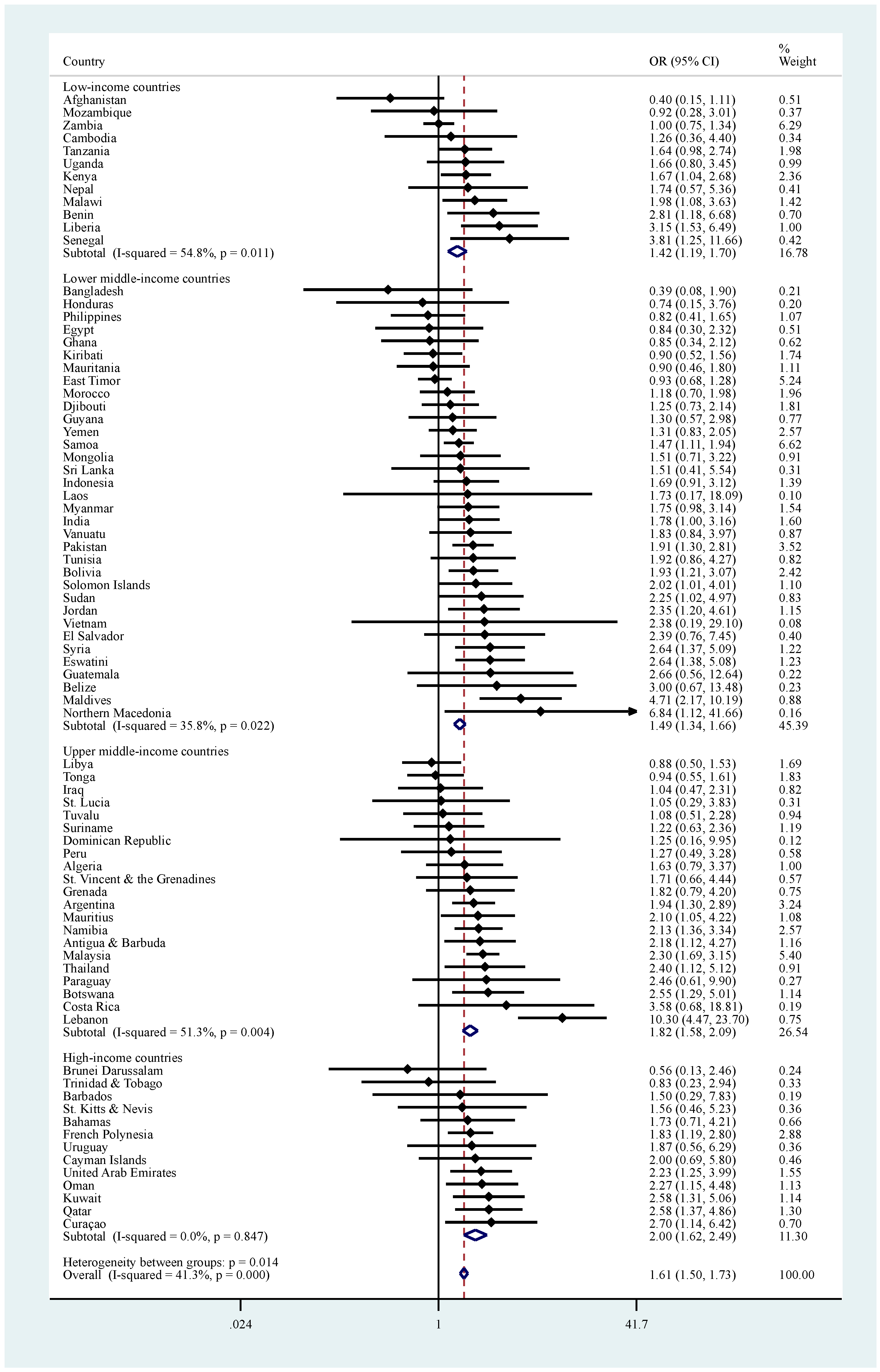
| After using toilet | Low | 1.42 [1.19,1.70] | 54.8 |
| Lower middle | 1.49 [1.34,1.66] | 35.8 | |
| Upper middle | 1.82 [1.58,2.09] | 51.3 | |
| High | 2.00 [1.62,2.49] | 0.0 | |
| Overall | 1.61 [1.50,1.73] | 41.3 | |
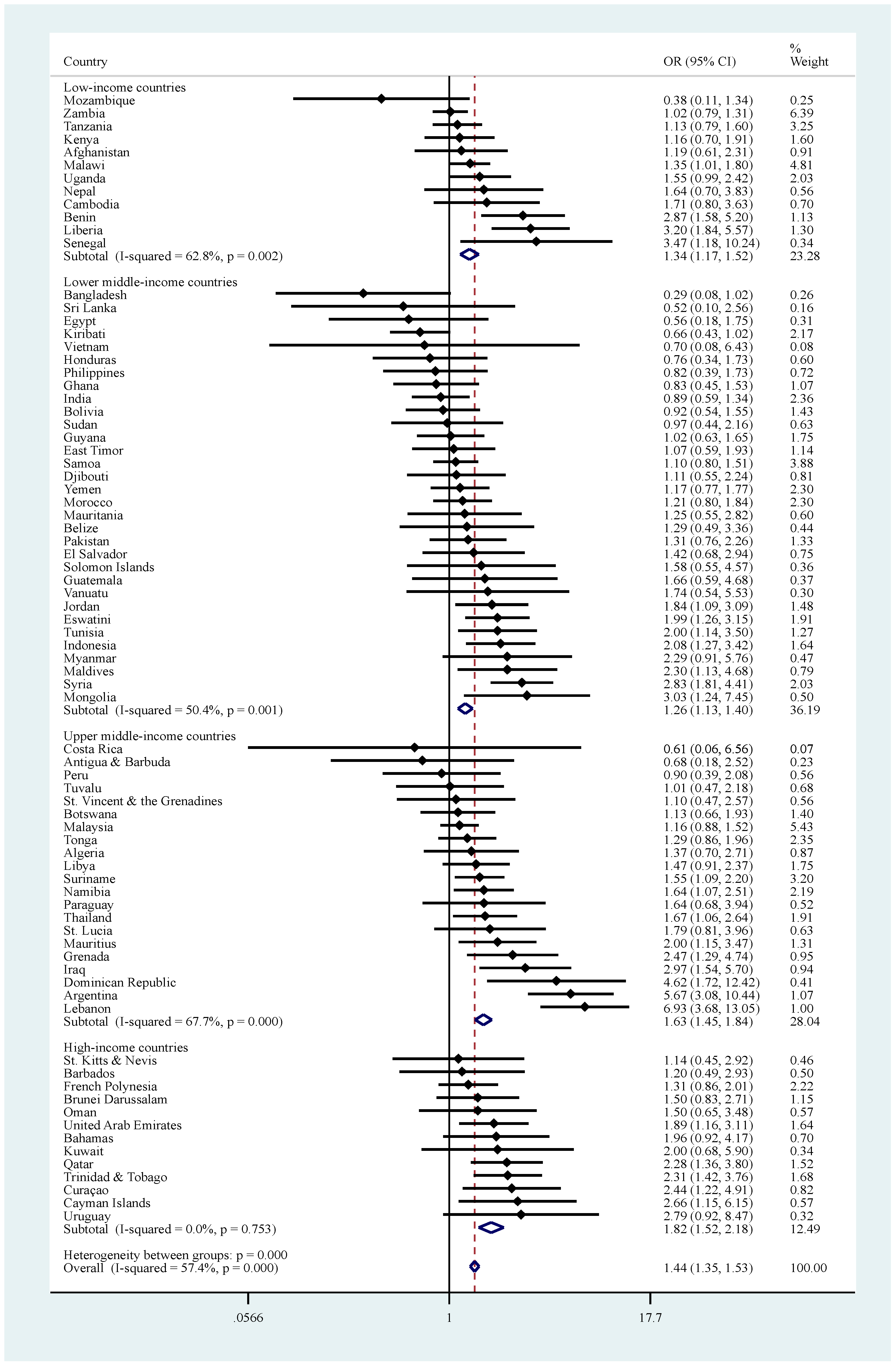
| Soap | Low | 1.34 [1.17,1.52] | 62.8 |
| Lower middle b | 1.26 [1.13,1.40] | 50.4 | |
| Upper middle | 1.63 [1.45,1.84] | 67.7 | |
| High | 1.82 [1.52,2.18] | 0.0 | |
| Overall | 1.44 [1.35,1.53] | 57.4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Smith, L.; Butler, L.; Tully, M.A.; Jacob, L.; Barnett, Y.; López-Sánchez, G.F.; López-Bueno, R.; Shin, J.I.; McDermott, D.; Pfeifer, B.A.; et al. Hand-Washing Practices among Adolescents Aged 12–15 Years from 80 Countries. Int. J. Environ. Res. Public Health 2021, 18, 138. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18010138
Smith L, Butler L, Tully MA, Jacob L, Barnett Y, López-Sánchez GF, López-Bueno R, Shin JI, McDermott D, Pfeifer BA, et al. Hand-Washing Practices among Adolescents Aged 12–15 Years from 80 Countries. International Journal of Environmental Research and Public Health. 2021; 18(1):138. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18010138
Chicago/Turabian StyleSmith, Lee, Laurie Butler, Mark A Tully, Louis Jacob, Yvonne Barnett, Guillermo F. López-Sánchez, Rubén López-Bueno, Jae Il Shin, Daragh McDermott, Briona A. Pfeifer, and et al. 2021. "Hand-Washing Practices among Adolescents Aged 12–15 Years from 80 Countries" International Journal of Environmental Research and Public Health 18, no. 1: 138. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18010138