A Machine Learning Approach to Identify Predictors of Potentially Inappropriate Non-Steroidal Anti-Inflammatory Drugs (NSAIDs) Use in Older Adults with Osteoarthritis

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Study Design
2.3. Study Cohort
2.4. Measures
2.4.1. Target (i.e., Dependent) Variable: Potentially Inappropriate NSAIDs Use during Follow-Up (Yes/No)
2.4.2. Features (i.e., Independent Variables)
CV and GI Risk Categories for Older Adults
Other Features
2.5. Analytic Approach
3. Results
3.1. Sample Characteristics
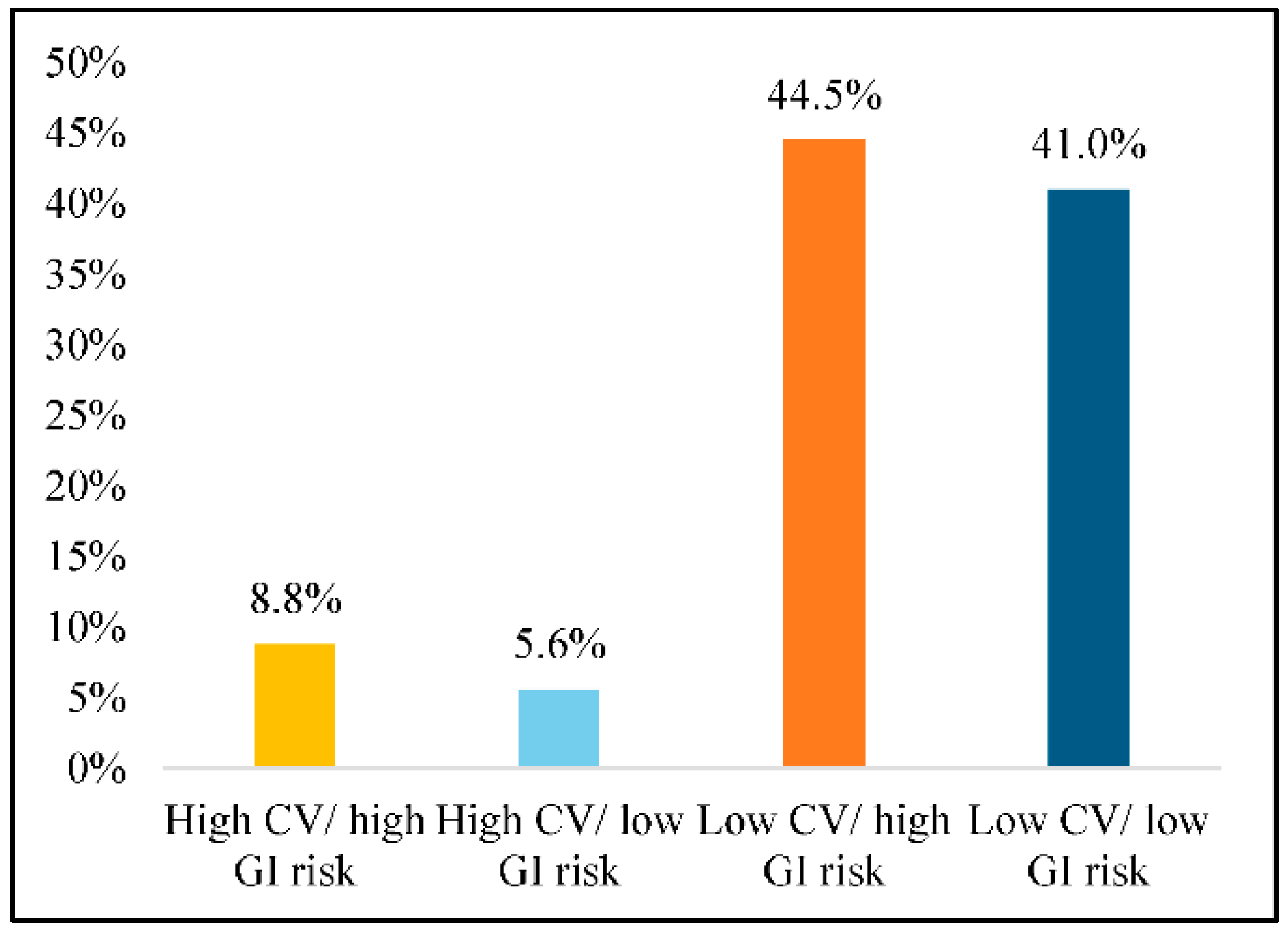
3.2. Prevalence of Potentially Inappropriate NSAIDs Use
3.3. Unadjusted Associations of Baseline Characteristics and Potentially Inappropriate NSAIDs Use
3.4. Model Performance Comparison
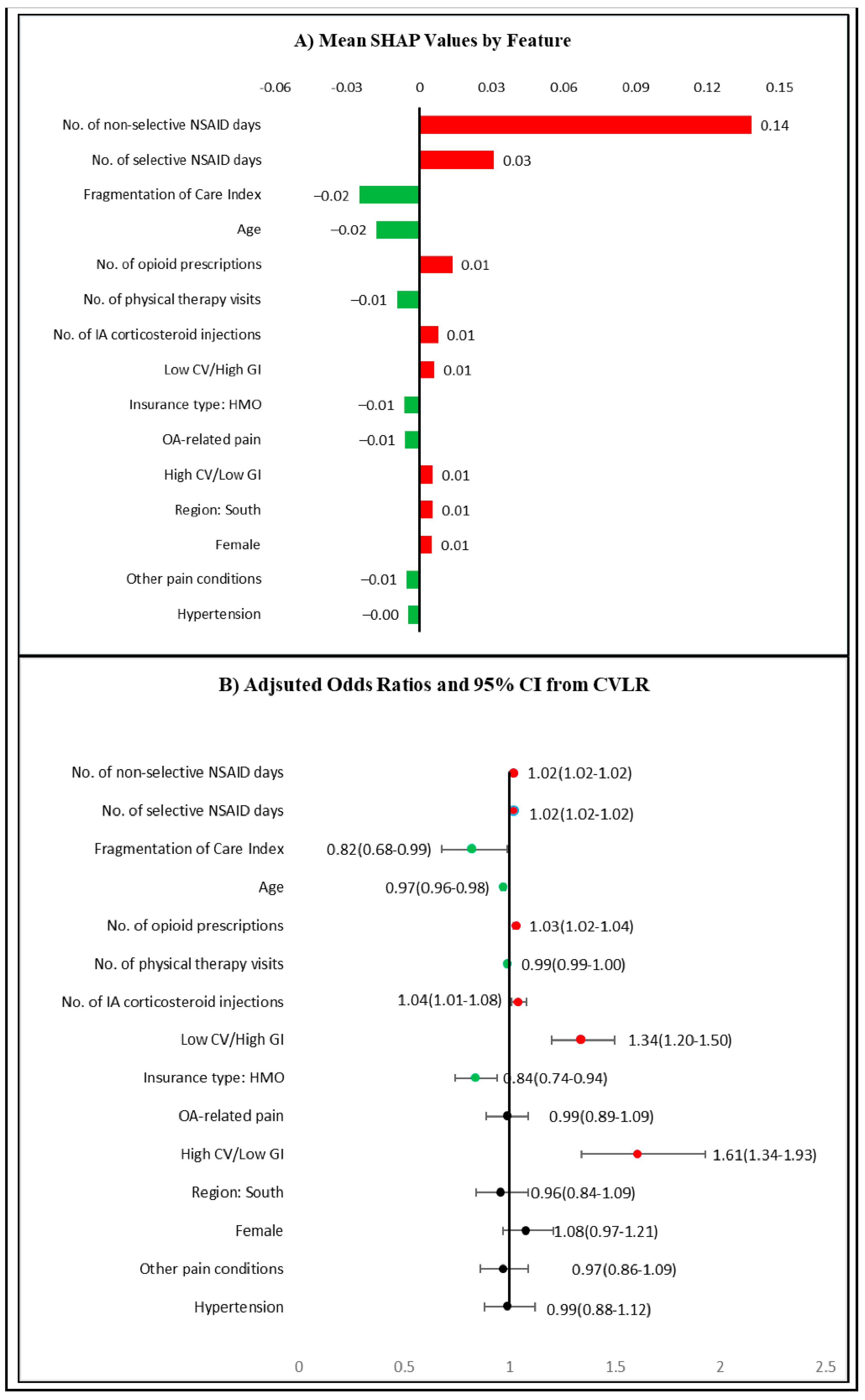
3.5. Feature Importance and Model Interpretation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zhou, Y.; Boudreau, D.M.; Freedman, A.N. Trends in the Use of Aspirin and Nonsteroidal Anti-Inflammatory Drugs in the General U.S. Population. Pharmacoepidemiol. Drug Saf. 2014, 23, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Cooper, C.; Chapurlat, R.; Al-Daghri, N.; Herrero-Beaumont, G.; Bruyère, O.; Rannou, F.; Roth, R.; Uebelhart, D.; Reginster, J.-Y. Safety of Oral Non-Selective Non-Steroidal Anti-Inflammatory Drugs in Osteoarthritis: What Does the Literature Say? Drugs Aging 2019, 36, 15–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kolasinski, S.L.; Neogi, T.; Hochberg, M.C.; Oatis, C.; Guyatt, G.; Block, J.; Callahan, L.; Copenhaver, C.; Dodge, C.; Felson, D.; et al. 2019 American College of Rheumatology/Arthritis Foundation Guideline for the Management of Osteoarthritis of the Hand, Hip, and Knee. Arthritis Care Res. 2020, 72, 149–162. [Google Scholar] [CrossRef] [PubMed]
- Coxib and traditional NSAID Trialists’ (CNT) Collaboration; Bhala, N.; Emberson, J.; Merhi, A.; Abramson, S.; Arber, N.; Baron, J.A.; Bombardier, C.; Cannon, C.; Farkouh, M.E.; et al. Vascular and Upper Gastrointestinal Effects of Non-Steroidal Anti-Inflammatory Drugs: Meta-Analyses of Individual Participant Data from Randomised Trials. Lancet 2013, 382, 769–779. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rahme, E.; Joseph, L.; Kong, S.X.; Watson, D.J.; LeLorier, J. Gastrointestinal Health Care Resource Use and Costs Associated with Nonsteroidal Antiinflammatory Drugs versus Acetaminophen: Retrospective Cohort Study of an Elderly Population. Arthritis Rheum. 2000, 43, 917–924. [Google Scholar] [CrossRef]
- Bidaut-Russell, M.; Gabriel, S.E. Adverse Gastrointestinal Effects of NSAIDs: Consequences and Costs. Best Pract. Res. Clin. Gastroenterol. 2001, 15, 739–753. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence. NSAIDs—Prescribing Issues; Clinical Knowledge Summaries. NICE, 2019. Available online: https://www.nice.org.uk/guidance (accessed on 28 December 2020).
- Helin-Salmivaara, A.; Virtanen, A.; Vesalainen, R.; Grönroos, J.M.; Klaukka, T.; Idänpään-Heikkilä, J.E.; Huupponen, R. NSAID Use and the Risk of Hospitalization for First Myocardial Infarction in the General Population: A Nationwide Case-Control Study from Finland. Eur. Heart J. 2006, 27, 1657–1663. [Google Scholar] [CrossRef] [Green Version]
- Osani, M.C.; Vaysbrot, E.E.; Zhou, M.; McAlindon, T.E.; Bannuru, R.R. Duration of Symptom Relief and Early Trajectory of Adverse Events for Oral NSAID s in Knee Osteoarthritis: A Systematic Review and Meta-analysis. Arthritis Care Res. 2020, 72, 641–651. [Google Scholar] [CrossRef]
- Center for Drug Evaluation and Research FDA Drug Safety Communication: FDA Strengthens Warning That Non-Aspirin Nonsteroidal Anti-Inflammatory Drugs (NSAIDs) Can Cause Heart Attacks or Strokes. Available online: http://www.fda.gov/drugs/drug-safety-and-availability/fda-drug-safety-communication-fda-strengthens-warning-non-aspirin-nonsteroidal-anti-inflammatory (accessed on 26 December 2020).
- Zhang, Y.; Jordan, J.M. Epidemiology of Osteoarthritis. Clin. Geriatr. Med. 2010, 26, 355–369. [Google Scholar] [CrossRef] [Green Version]
- Hawker, G.A.; Gignac, M.A.M.; Badley, E.; Davis, A.M.; French, M.R.; Li, Y.; Perruccio, A.V.; Power, J.D.; Sale, J.; Lou, W. A Longitudinal Study to Explain the Pain-Depression Link in Older Adults with Osteoarthritis. Arthritis Care Res. (Hoboken) 2011, 63, 1382–1390. [Google Scholar] [CrossRef]
- Zhao, X.; Shah, D.; Gandhi, K.; Wei, W.; Dwibedi, N.; Webster, L.R.; Sambamoorthi, U. Clinical, Humanistic, and Economic Burden of Osteoarthritis among Noninstitutionalized Adults in the United States. Osteoarthr. Cartil. 2019. [Google Scholar] [CrossRef] [PubMed]
- American Geriatrics Society Panel on Pharmacological Management of Persistent Pain in Older Persons Pharmacological Management of Persistent Pain in Older Persons. J. Am. Geriatr. Soc. 2009, 57, 1331–1346. [CrossRef] [PubMed]
- Griffin, M.R. Epidemiology of Nonsteroidal Anti-Inflammatory Drug-Associated Gastrointestinal Injury. Am. J. Med. 1998, 104, 23S–29S, discussion 41S–42S. [Google Scholar] [CrossRef]
- Wegman, A.; van der Windt, D.; van Tulder, M.; Stalman, W.; de Vries, T. Nonsteroidal Antiinflammatory Drugs or Acetaminophen for Osteoarthritis of the Hip or Knee? A Systematic Review of Evidence and Guidelines. J. Rheumatol. 2004, 31, 344–354. [Google Scholar] [PubMed]
- Vanderstraeten, G.; Lejeune, T.M.; Piessevaux, H.; De Bacquer, D.; Walker, C.; De Beleyr, B. Gastrointestinal Risk Assessment in Patients Requiring Non-Steroidal Anti-Inflammatory Drugs for Osteoarthritis: The GIRANO Study. J. Rehabil. Med. 2016, 48, 705–710. [Google Scholar] [CrossRef] [Green Version]
- Lanas, A.; Garcia-Tell, G.; Armada, B.; Oteo-Alvaro, A. Prescription Patterns and Appropriateness of NSAID Therapy According to Gastrointestinal Risk and Cardiovascular History in Patients with Diagnoses of Osteoarthritis. BMC Med. 2011, 9, 38. [Google Scholar] [CrossRef] [Green Version]
- Sebaldt, R.J.; Petrie, A.; Goldsmith, C.H.; Marentette, M.A. Appropriateness of NSAID and Coxib Prescribing for Patients with Osteoarthritis by Primary Care Physicians in Ontario: Results from the CANOAR Study. Am. J. Manag. Care 2004, 10, 742–750. [Google Scholar]
- Optum Clinformatics Data Mart. Available online: https://www.optum.com/content/dam/optum/resources/productSheets/Clinformatics_for_Data_Mart.pdf (accessed on 17 June 2020).
- Shrestha, S.; Dave, A.J.; Losina, E.; Katz, J.N. Diagnostic Accuracy of Administrative Data Algorithms in the Diagnosis of Osteoarthritis: A Systematic Review. BMC Med. Inform. Decis. Mak. 2016, 16, 82. [Google Scholar] [CrossRef] [Green Version]
- Chan, F.K.L.; Abraham, N.S.; Scheiman, J.M.; Laine, L. First International Working Party on Gastrointestinal and Cardiovascular Effects of Nonsteroidal Anti-inflammatory Drugs and Anti-platelet Agents Management of Patients on Nonsteroidal Anti-Inflammatory Drugs: A Clinical Practice Recommendation from the First International Working Party on Gastrointestinal and Cardiovascular Effects of Nonsteroidal Anti-Inflammatory Drugs and Anti-Platelet Agents. Am. J. Gastroenterol. 2008, 103, 2908–2918. [Google Scholar] [CrossRef]
- Hochberg, M.C.; Altman, R.D.; April, K.T.; Benkhalti, M.; Guyatt, G.; McGowan, J.; Towheed, T.; Welch, V.; Wells, G.; Tugwell, P.; et al. American College of Rheumatology 2012 Recommendations for the Use of Nonpharmacologic and Pharmacologic Therapies in Osteoarthritis of the Hand, Hip, and Knee. Arthritis Care Res. (Hoboken) 2012, 64, 465–474. [Google Scholar] [CrossRef] [Green Version]
- Lanas, A.; Tornero, J.; Zamorano, J.L. Assessment of Gastrointestinal and Cardiovascular Risk in Patients with Osteoarthritis Who Require NSAIDs: The LOGICA Study. Ann. Rheum. Dis. 2010, 69, 1453–1458. [Google Scholar] [CrossRef] [PubMed]
- Boyapati, R.; Ong, S.Y.; Ye, B.; Kruavit, A.; Lee, N.; Vaughan, R.; Nandurkar, S.; Gibson, P.; Garg, M. One Fifth of Hospitalizations for Peptic Ulcer-Related Bleeding Are Potentially Preventable. World J. Gastroenterol. 2014, 20, 10504–10511. [Google Scholar] [CrossRef] [PubMed]
- Lanza, F.L.; Chan, F.K.L.; Quigley, E.M.M. Practice Parameters Committee of the American College of Gastroenterology Guidelines for Prevention of NSAID-Related Ulcer Complications. Am. J. Gastroenterol. 2009, 104, 728–738. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, D.L.; Scheiman, J.; Abraham, N.S.; Antman, E.M.; Chan, F.K.L.; Furberg, C.D.; Johnson, D.A.; Mahaffey, K.W.; Quigley, E.M. American College of Cardiology Foundation Task Force on Clinical Expert Consensus Documents ACCF/ACG/AHA 2008 Expert Consensus Document on Reducing the Gastrointestinal Risks of Antiplatelet Therapy and NSAID Use: A Report of the American College of Cardiology Foundation Task Force on Clinical Expert Consensus Documents. Circulation 2008, 118, 1894–1909. [Google Scholar] [CrossRef]
- García Rodríguez, L.A.; Jick, H. Risk of Upper Gastrointestinal Bleeding and Perforation Associated with Individual Non-Steroidal Anti-Inflammatory Drugs. Lancet 1994, 343, 769–772. [Google Scholar] [CrossRef]
- Gabriel, S.E.; Jaakkimainen, L.; Bombardier, C. Risk for Serious Gastrointestinal Complications Related to Use of Nonsteroidal Anti-Inflammatory Drugs. A Meta-Analysis. Ann. Intern. Med. 1991, 115, 787–796. [Google Scholar] [CrossRef]
- Aday, L.A.; Andersen, R. A Framework for the Study of Access to Medical Care. Health Serv Res 1974, 9, 208–220. [Google Scholar]
- Liu, C.W.; Einstadter, D.; Cebul, R.D. Care Fragmentation and Emergency Department Use among Complex Patients with Diabetes. Am. J. Manag. Care 2010, 16, 413–420. [Google Scholar]
- Boulesteix, A.-L.; Schmid, M. Machine Learning versus Statistical Modeling. Biom. J. 2014, 56, 588–593. [Google Scholar] [CrossRef]
- Borstelmann, S.M. Machine Learning Principles for Radiology Investigators. Acad. Radiol. 2020, 27, 13–25. [Google Scholar] [CrossRef] [Green Version]
- Chen, T.; Guestrin, C. XGBoost: A Scalable Tree Boosting System. In Proceedings of the 22nd ACM SIGKDD International Conference on Knowledge Discovery and Data Mining; ACM: San Francisco, CA, USA, 2016; pp. 785–794. [Google Scholar]
- Zhang, Z.; Ho, K.M.; Hong, Y. Machine Learning for the Prediction of Volume Responsiveness in Patients with Oliguric Acute Kidney Injury in Critical Care. Crit. Care 2019, 23, 112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lundberg, S.M.; Lee, S.-I. A Unified Approach to Interpreting Model Predictions. In Proceedings of the Advances in Neural Information Processing Systems 30; Guyon, I., Luxburg, U.V., Bengio, S., Wallach, H., Fergus, R., Vishwanathan, S., Garnett, R., Eds.; Advances in Neural Information Processing Systems 30 (NIPS 2017): Long Beach, CA, USA, 2017. [Google Scholar]
- By the 2019 American Geriatrics Society Beers Criteria® Update Expert Panel. American Geriatrics Society 2019 Updated AGS Beers Criteria® for Potentially Inappropriate Medication Use in Older Adults: 2019 AGS BEERS CRITERIA® UPDATE EXPERT PANEL. J. Am. Geriatr. Soc. 2019, 67, 674–694. [Google Scholar] [CrossRef] [PubMed]
- Fries, J.F.; Williams, C.A.; Bloch, D.A.; Michel, B.A. Nonsteroidal Anti-Inflammatory Drug-Associated Gastropathy: Incidence and Risk Factor Models. Am. J. Med. 1991, 91, 213–222. [Google Scholar] [CrossRef]
- Smith, S.R.; Deshpande, B.R.; Collins, J.E.; Katz, J.N.; Losina, E. Comparative Pain Reduction of Oral Non-Steroidal Anti-Inflammatory Drugs and Opioids for Knee Osteoarthritis: Systematic Analytic Review. Osteoarthr. Cartil. 2016, 24, 962–972. [Google Scholar] [CrossRef] [Green Version]
- Bouck, Z.; Mecredy, G.C.; Ivers, N.M.; Barua, M.; Martin, D.; Austin, P.C.; Tepper, J.; Bhatia, R.S. Frequency and Associations of Prescription Nonsteroidal Anti-Inflammatory Drug Use Among Patients With a Musculoskeletal Disorder and Hypertension, Heart Failure, or Chronic Kidney Disease. JAMA Intern. Med. 2018, 178, 1516–1525. [Google Scholar] [CrossRef] [Green Version]
- Arain, A.; Rasheed, M.; Sallam, N.; Sarwar, Z.; Khan, M. Patient’s Knowledge and Use of Oral Non-Steroidal Anti-Inflammatory Drugs in a Rheumatology Clinic. Kans. J. Med. 2019, 12, 132–135. [Google Scholar] [CrossRef]
- Wynne, H.A.; Long, A. Patient Awareness of the Adverse Effects of Non-Steroidal Anti-Inflammatory Drugs (NSAIDs). Br. J. Clin. Pharmacol. 1996, 42, 253–256. [Google Scholar] [CrossRef]
- Gibson, J.C. A Survey of Patients Knowledge of NSAID Side Effects. BMJ 2020, 329, 15. [Google Scholar] [CrossRef] [Green Version]
- Louder, A.M.; Joshi, A.V.; Ball, A.T.; Cappelleri, J.C.; Deminski, M.C.; Sanchez, R.J. Impact of Celecoxib Restrictions in Medicare Beneficiaries with Arthritis. Am. J. Manag. Care 2011, 17, 503–512. [Google Scholar]
- Carlton, R.I.; Bramley, T.J.; Nightengale, B.; Conner, T.M.; Zacker, C. Review of Outcomes Associated With Formulary Restrictions: Focus on Step Therapy. Am. J. Pharm. Benefits 2010, 2, 50–58. [Google Scholar]
- Kingsbury, S.R.; Hensor, E.M.; Walsh, C.A.; Hochberg, M.C.; Conaghan, P.G. How Do People with Knee Osteoarthritis Use Osteoarthritis Pain Medications and Does This Change over Time? Data from the Osteoarthritis Initiative. Arthritis Res. Ther. 2013, 15, R106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marcum, Z.A.; Perera, S.; Donohue, J.M.; Boudreau, R.M.; Newman, A.B.; Ruby, C.M.; Studenski, S.A.; Kwoh, C.K.; Simonsick, E.M.; Bauer, D.C.; et al. Analgesic Use for Knee and Hip Osteoarthritis in Community-Dwelling Elders. Pain Med. 2011, 12, 1628–1636. [Google Scholar] [CrossRef] [PubMed]
- Slater, D.; Kunnathil, S.; McBride, J.; Koppala, R. Pharmacology of Nonsteroidal Antiinflammatory Drugs and Opioids. Semin. Intervent. Radiol. 2010, 27, 400–411. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blamey, R.; Jolly, K.; Greenfield, S.; Jobanputra, P. Patterns of Analgesic Use, Pain and Self-Efficacy: A Cross-Sectional Study of Patients Attending a Hospital Rheumatology Clinic. BMC Musculoskelet. Disord. 2009, 10, 137. [Google Scholar] [CrossRef] [Green Version]
- Ghouri, A.; Conaghan, P.G. Update on Novel Pharmacological Therapies for Osteoarthritis. Ther. Adv. Musculoskelet. Dis. 2019, 11. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gastrointestinal Risk Factors (at Least One of the Following) | Cardiovascular Risk Factors (at Least One of the Following) |
|---|---|
| Complicated peptic ulcer disease | Angina |
| Uncomplicated peptic ulcer disease | Stroke |
| Dyspepsia | Myocardial infarction |
| Gastroesophageal reflux disorder | Congestive heart failure |
| Concomitant use of one of the following drugs with NSAIDs a: Corticosteroids Antiplatelets Selective serotonin reuptake inhibitors Aspirin b Anticoagulants |
| Variable | N/Mean | Percentage/SD | |
|---|---|---|---|
| All | 44,990 | 100.0 | |
| Age | |||
| 65–69 | 10,315 | 22.9 | |
| 70–74 | 11,330 | 25.2 | |
| 75–79 | 8957 | 19.9 | |
| 80+ | 14,388 | 32.0 | |
| Sex | |||
| Female | 29,853 | 66.4 | |
| Male | 15,137 | 33.6 | |
| Region | |||
| Northeast | 6034 | 13.4 | |
| Midwest | 10,862 | 24.1 | |
| South | 16,410 | 36.5 | |
| West | 11,684 | 26.0 | |
| Insurance Type | |||
| HMO | 16,314 | 36.3 | |
| Other | 28,676 | 63.7 | |
| Other Pain Conditions | |||
| Yes | 15,733 | 35.0 | |
| No | 29,257 | 65.0 | |
| OA-related pain | |||
| Yes | 24,880 | 55.3 | |
| No | 20,110 | 44.7 | |
| Anxiety | |||
| Yes | 6285 | 14.0 | |
| No | 38,705 | 86.0 | |
| Substance abuse disorder | |||
| Yes | 3354 | 7.5 | |
| No | 41,636 | 92.5 | |
| Depression | |||
| Yes | 7620 | 16.9 | |
| No | 37,370 | 83.1 | |
| Fragmentation of care index | 0.44 | 0.28 | |
| Number of IA hyaluronic acid injections | |||
| 0.2 | 0.9 | ||
| Number of IA corticosteroid injections | |||
| 0.8 | 1.5 | ||
| Number of physical therapy visits | |||
| 4.4 | 12.0 | ||
| Number of opioid prescriptions | |||
| 2.0 | 4.2 | ||
| Any NSAIDs use | |||
| Yes | 11,891 | 21.6 | |
| No | 33,099 | 78.4 | |
| CV/GI Risk | |||
| High CV/high GI | 3383 | 7.5 | |
| High CV/low GI | 4233 | 9.4 | |
| Low CV/high GI | 12,145 | 27.0 | |
| Low CV/low GI | 25,229 | 56.1 | |
| Number of days of non-selective NSAIDs use | |||
| 29.3 | 79.5 | ||
| Number of days of selective NSAIDs use | |||
| 5.8 | 38.7 | ||
| Potentially inappropriate NSAIDs use at follow-up | |||
| Yes | 5772 | 12.8 | |
| No | 39,218 | 87.2 | |
| XGBoost | Cross-Validated Logistic Regression | |
|---|---|---|
| Accuracy | 0.93 | 0.93 |
| Precision | 0.81 | 0.83 |
| Recall | 0.63 | 0.58 |
| F1 Score | 0.71 | 0.68 |
| Specificity | 0.98 | 0.98 |
| Kappa | 0.67 | 0.64 |
| AUROC | 0.92 | 0.91 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Patel, J.; Ladani, A.; Sambamoorthi, N.; LeMasters, T.; Dwibedi, N.; Sambamoorthi, U. A Machine Learning Approach to Identify Predictors of Potentially Inappropriate Non-Steroidal Anti-Inflammatory Drugs (NSAIDs) Use in Older Adults with Osteoarthritis. Int. J. Environ. Res. Public Health 2021, 18, 155. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18010155
Patel J, Ladani A, Sambamoorthi N, LeMasters T, Dwibedi N, Sambamoorthi U. A Machine Learning Approach to Identify Predictors of Potentially Inappropriate Non-Steroidal Anti-Inflammatory Drugs (NSAIDs) Use in Older Adults with Osteoarthritis. International Journal of Environmental Research and Public Health. 2021; 18(1):155. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18010155
Chicago/Turabian StylePatel, Jayeshkumar, Amit Ladani, Nethra Sambamoorthi, Traci LeMasters, Nilanjana Dwibedi, and Usha Sambamoorthi. 2021. "A Machine Learning Approach to Identify Predictors of Potentially Inappropriate Non-Steroidal Anti-Inflammatory Drugs (NSAIDs) Use in Older Adults with Osteoarthritis" International Journal of Environmental Research and Public Health 18, no. 1: 155. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18010155