Artificial Intelligence Model of Drive-Through Vaccination Simulation

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
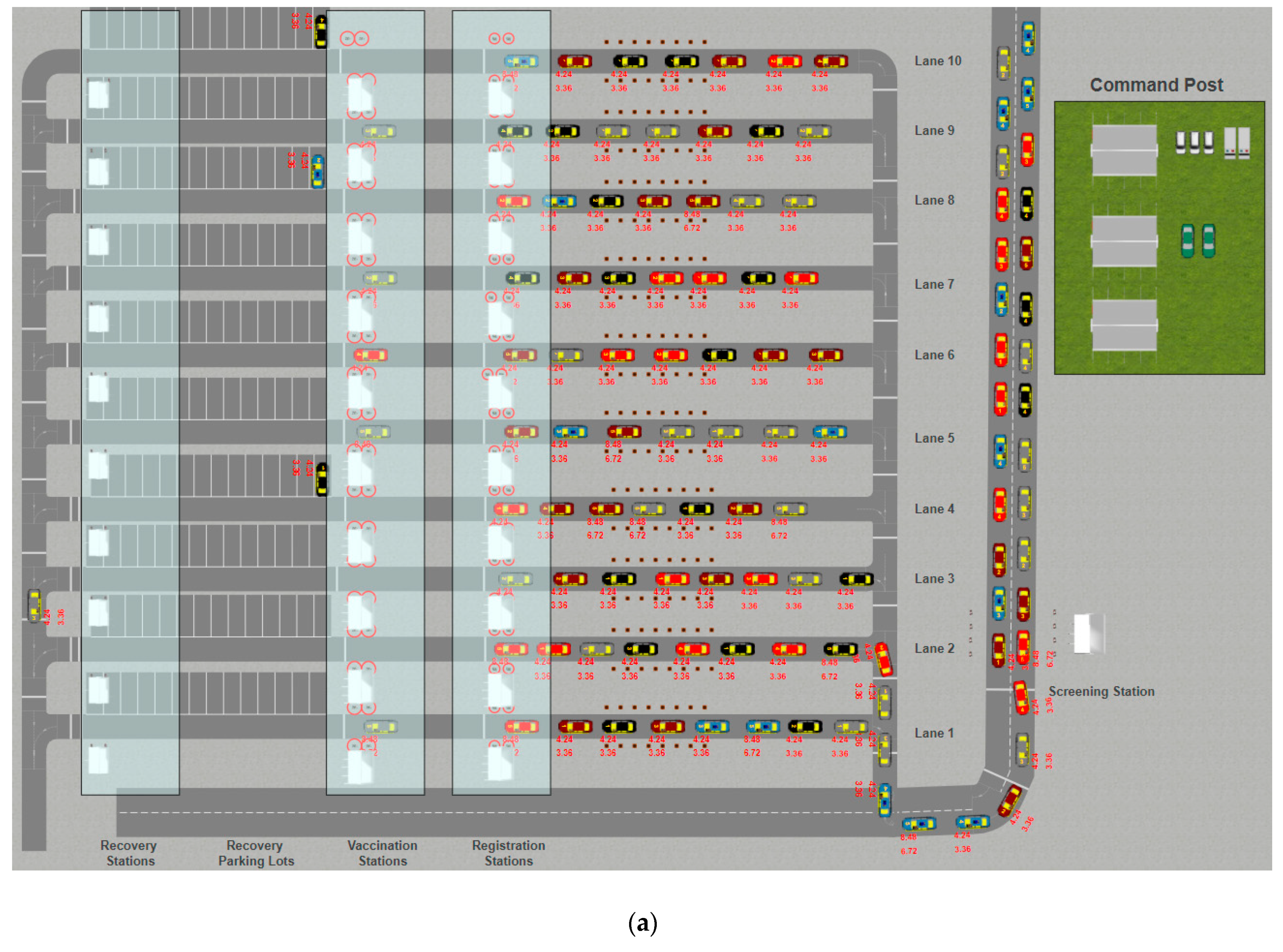
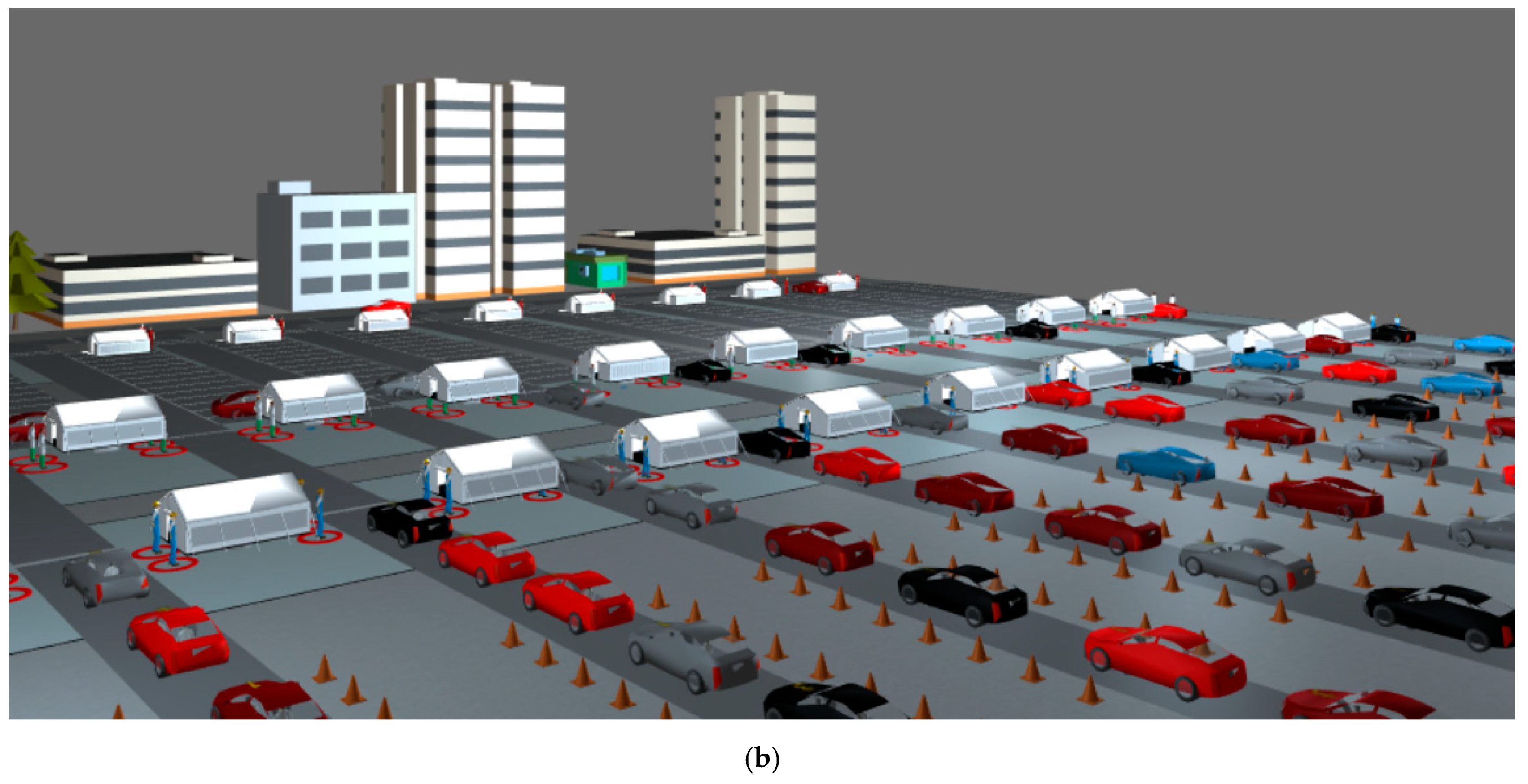
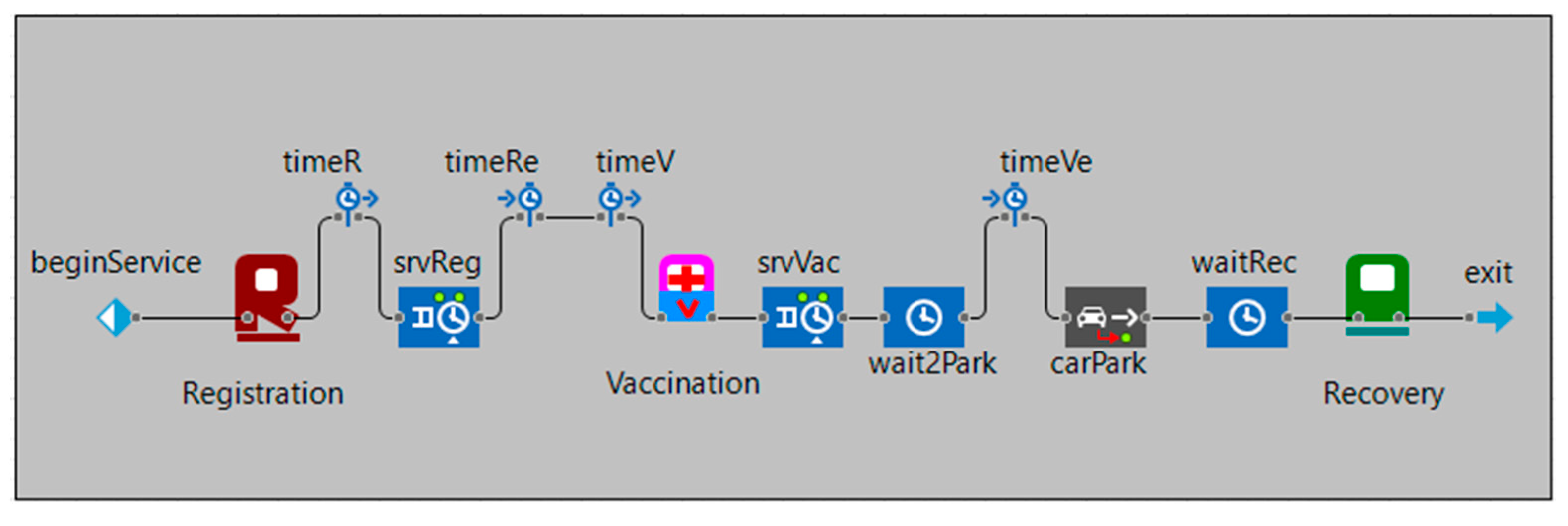
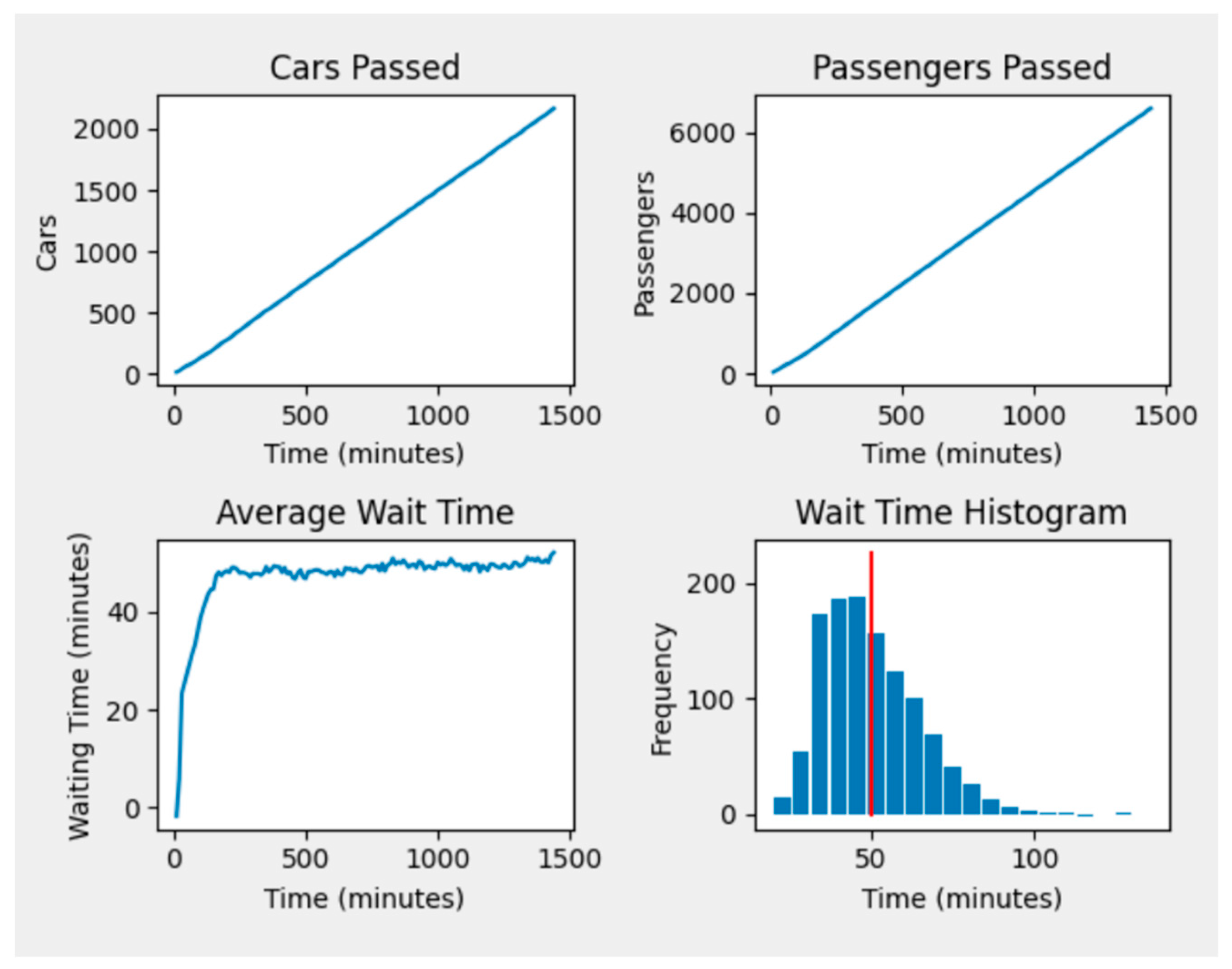
2.1. The Drive-Through Simulation
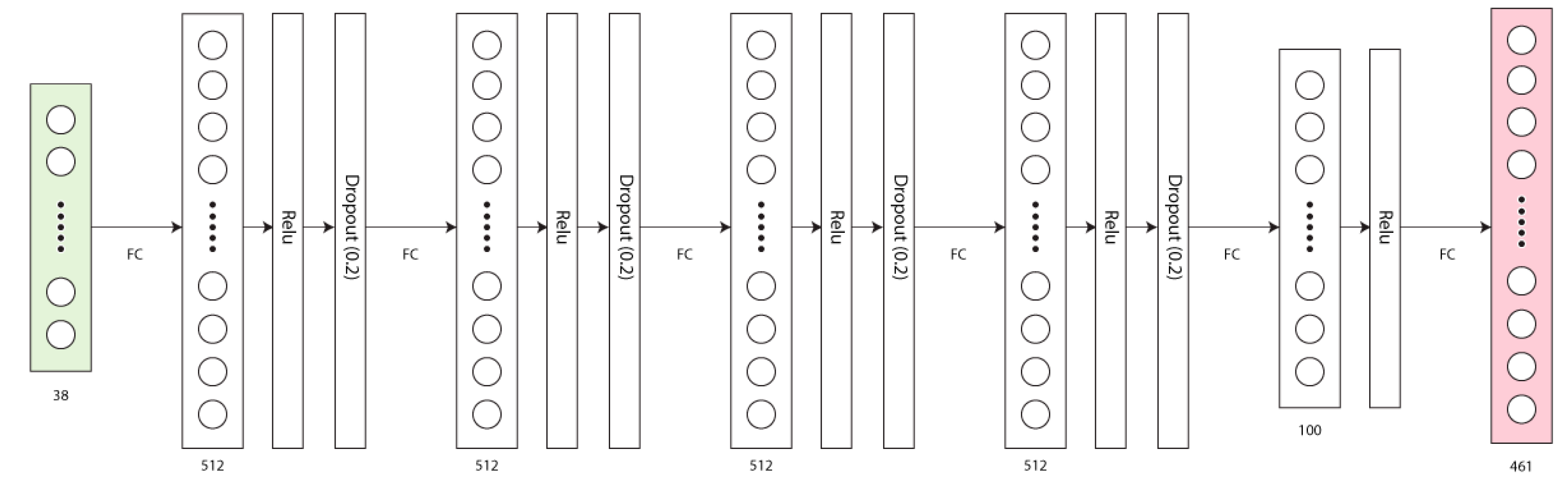
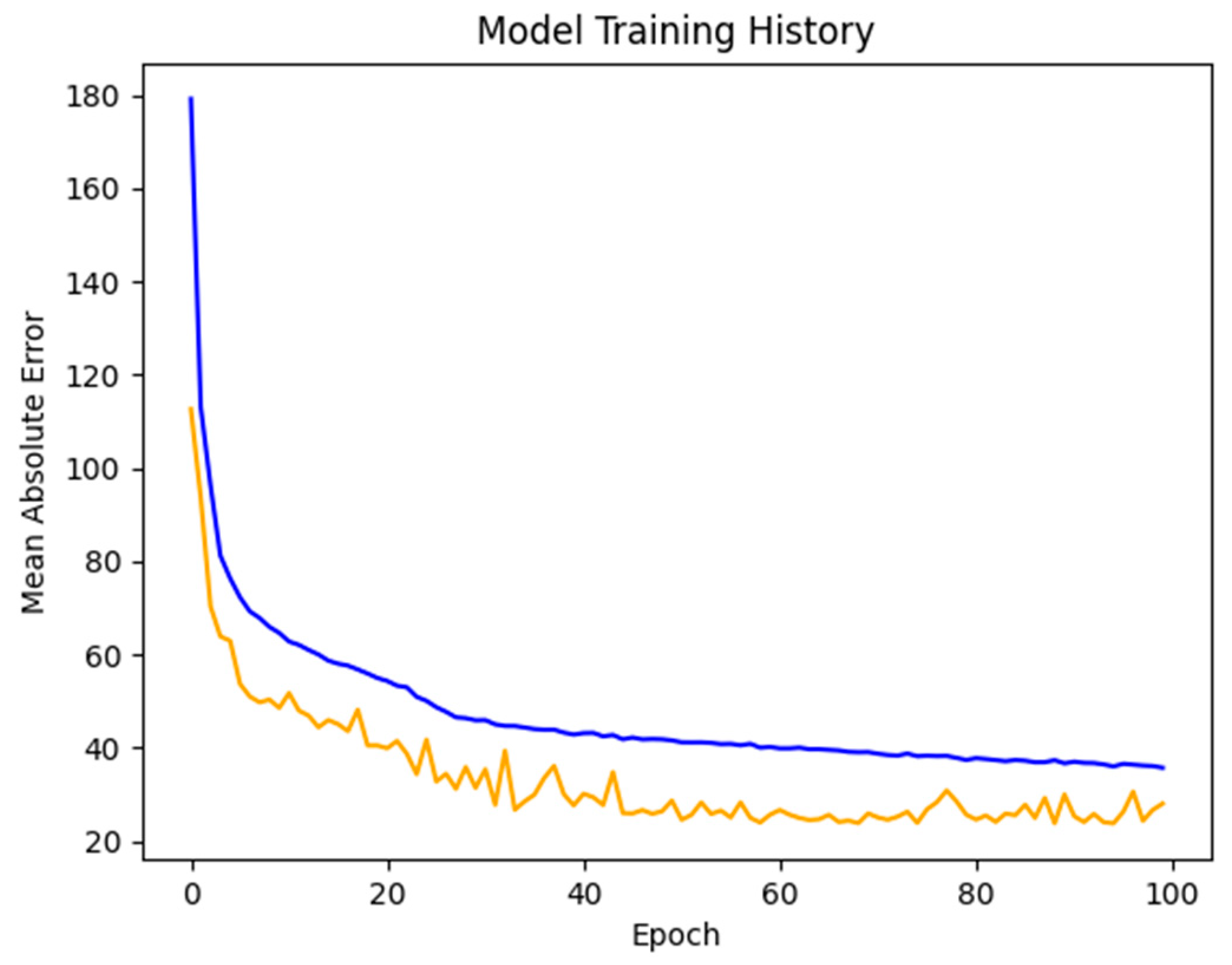
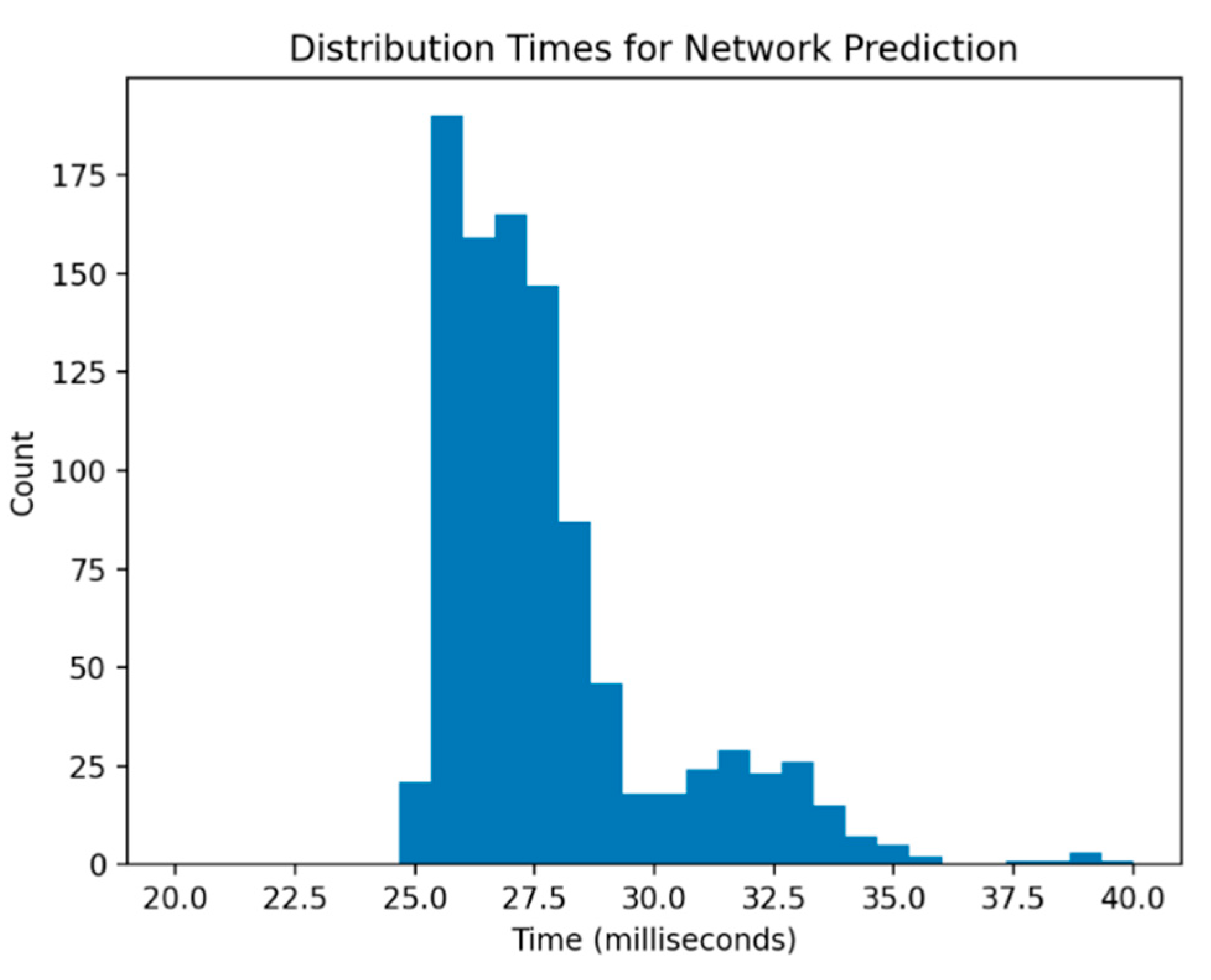
2.2. The AI Model
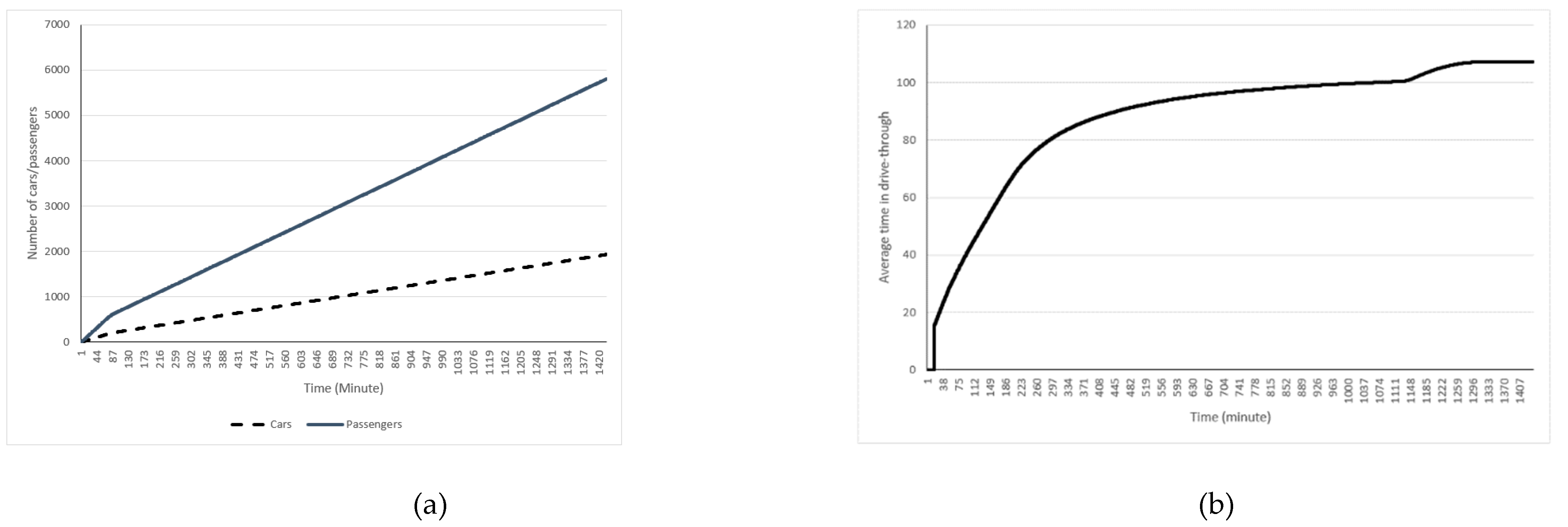
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- DeRoo, S.S.; Pudalov, N.J.; Fu, L.Y. Planning for a COVID-19 Vaccination Program. JAMA 2020, 323, 2458. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Evans, G.W.; Heragu, S.S. Simulation and optimization modeling for drive-through mass vaccination—A generalized approach. Simul. Model. Pr. Theory 2013, 37, 99–106. [Google Scholar] [CrossRef] [Green Version]
- Clemente-Suárez, V.J.; Hormeño-Holgado, A.; Jiménez, M.; Benitez-Agudelo, J.C.; Navarro-Jiménez, E.; Perez-Palencia, N.; Maestre-Serrano, R.; Laborde-Cárdenas, C.C.; Tornero-Aguilera, J.F. Dynamics of Population Immunity Due to the Herd Effect in the COVID-19 Pandemic. Vaccines 2020, 8, 236. [Google Scholar] [CrossRef] [PubMed]
- Gottlieb, S.; Rivers, C.; McClellan, M.; Silvis, L.; Watson, C. National Coronavirus Response: A ROAD map to Reopening; American Enterprise Institute: Washington, DC, USA, 2020; Available online: https://www.aei.org/research-products/report/national-coronavirus-response-a-road-map-to-reopening (accessed on 11 November 2020).
- Reid, D.E. What Are the Efficiencies of a Mass Vaccination Drive-Through Clinic Compared to a Walk-In Clinic? National Fire Academy: Emmitsburg, MD, USA, 2010; Available online: https://www.hsdl.org/?abstract&did=804516 (accessed on 11 November 2020).
- Wiggers, J.; van de Kracht, T.; Gupta, A.; Heragu, S.S. Design and Analysis of a Simulation Model for Drive-Through Mass Vaccination. In Proceedings of the 2011 Industrial Engineering Research Conference, Gujarat, India, 17 November 2011. [Google Scholar]
- Weiss, E.A.; Ngo, J.; Gilbert, G.H.; Quinn, J.V. Drive-Through Medicine: A Novel Proposal for Rapid Evaluation of Patients During an Influenza Pandemic. Ann. Emerg. Med. 2010, 55, 268–273. [Google Scholar] [CrossRef] [PubMed]
- Yaylali, E.; Ivy, J.S.; Taheri, J. Systems Engineering Methods for Enhancing the Value Stream in Public Health Preparedness: The Role of Markov Models, Simulation, and Optimization. Public Health Rep. 2014, 129, 145–153. [Google Scholar] [CrossRef] [PubMed]
- Schoch-Spana, M.; Brunson, E.; Long, R.; Ravi, S.; Ruth, A.; Trotochaud, M. The Public’s Role in COVID-19 Vaccination: Planning Recommendations Informed by Design Thinking and the Social, Behavioral, and Communication Sciences; Johns Hopkins Center for Health Security: Baltimore, MD, USA, 2020; Available online: https://www.centerforhealthsecurity.org/our-work/publications/the-publics-role-in-covid-19-vaccination (accessed on 11 November 2020).
- Lee, E.K.; Pietz, F.; Benecke, B.; Mason, J.; Burel, G. Advancing Public Health and Medical Preparedness with Operations Research. Interfaces 2013, 43, 79–98. [Google Scholar] [CrossRef]
- Carrico, R.M.; McKinney, W.P.; Watson, J.N.A.; Wiemken, T.; Myers, J. Drive-thru influenza immunization: Fifteen years of experience. J. Emerg. Manag. 2012, 10, 228. [Google Scholar] [CrossRef]
- Flynn, E.F.; Kuhn, E.; Shaik, M.; Tarr, E.; Scattolini, N.; Ballantine, A. Drive-Through COVID-19 Testing During the 2020 Pandemic: A Safe, Efficient, and Scalable Model for Pediatric Patients and Health Care Workers. Acad. Pediatr. 2020, 20, 753–755. [Google Scholar] [CrossRef]
- Stockley, S.; King, K.; Leach, J. Delivering Mass Vaccinations During COVID-19. A Logistical Guide for General Practice; Royal College of General Practitioners: London, UK, 2020; Available online: https://www.rcgp.org.uk/-/media/Files/Policy/A-Z-policy/2020/covid19/RCGP-guidance/RCGP-Mass-Vaccination-at-a-time-of-COVID-V15.ashx (accessed on 11 November 2020).
- Shim, E.; Meyers, L.A.; Galvani, A.P. Optimal H1N1 vaccination strategies based on self-interest versus group interest. BMC Public Health 2011, 11, S4. [Google Scholar] [CrossRef] [Green Version]
- Nicola, M.; Sohrabi, C.; Mathew, G.; Kerwan, A.; Al-Jabir, A.; Griffin, M.F.; Agha, M.; Agha, R. Health policy and leadership models during the COVID-19 pandemic: A review. Int. J. Surg. 2020, 81, 122–129. [Google Scholar] [CrossRef]
- Hussain, R.; Dawoud, D.; Babar, Z.-U.-D. Drive-thru pharmacy services: A way forward to combat COVID-19 pandemic. Res. Soc. Adm. Pharm. 2021, 17, 1920–1924. [Google Scholar] [CrossRef] [PubMed]
- Qeadan, F.; Honda, T.; Gren, L.H.; Dailey-Provost, J.; Benson, L.S.; Vanderslice, J.A.; Porucznik, C.A.; Waters, A.B.; Lacey, S.; Shoaf, K. Naive Forecast for COVID-19 in Utah Based on the South Korea and Italy Models-the Fluctuation between Two Extremes. Int. J. Environ. Res. Public Health 2020, 17, 2750. [Google Scholar] [CrossRef] [PubMed]
- Turrentine, M.; Ramirez, M.; Monga, M.; Gandhi, M.; Swaim, L.; Tyer-Viola, L.; Birsinger, M.; Belfort, M. Rapid Deployment of a Drive-Through Prenatal Care Model in Response to the Coronavirus Disease 2019 (COVID-19) Pandemic. Obstet. Gynecol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Bailey, L.C.; Barrett, N.R.; Thorne, M.; Ford, F.M.; Elizabeth, W.; Psevdos, G. Successful Drive-thru Point-of-Distribution Influenza Vaccination Program for Veterans Affairs Medical Center Employees. Am. J. Infect. Control. 2020, 48, S31. [Google Scholar] [CrossRef]
- Lee, D.; Lee, J. Testing on the move: South Korea’s rapid response to the COVID-19 pandemic. Transp. Res. Interdiscip. Perspect. 2020, 5, 100111. [Google Scholar] [CrossRef]
- Wessex Local Medical Committees. Operational Aspects of Influenza Immunisation 2020/21; Wessex Local Medical Committees: Hampshire, UK, 2020. [Google Scholar]
- Knox, C.; Davenport, D. Dispensing Emergency Medications and Supplies. In Public Health Practice; Fielding, J.E., Teutsch, S.M., Eds.; Oxford University Press (OUP): Oxford, UK, 2012; pp. 243–253. [Google Scholar]
- Aaby, K.; Abbey, R.L.; Herrmann, J.W.; Treadwell, M.; Jordan, C.S.; Wood, K. Embracing Computer Modeling to Address Pandemic Influenza in the 21st Century. J. Public Health Manag. Pr. 2006, 12, 365–372. [Google Scholar] [CrossRef] [Green Version]
- Pate, J. Drive-Thru PODs: An Alternate Method of Mass Prophylaxis; Public Health Meeting: Washington, DC, USA, 2007. [Google Scholar]
- Beeler, M.F.; Aleman, D.M.; Carter, M.W. A simulation case study to improve staffing decisions at mass immunization clinics for pandemic influenza. J. Oper. Res. Soc. 2014, 65, 497–511. [Google Scholar] [CrossRef]
- Fryhofer, S.A.; Fryhofer, G.W. Vaccination-Induced Bursitis: Technique Matters. Ann. Intern. Med. 2020, 173, 308–310. [Google Scholar] [CrossRef]
- Hupert, N.; Mushlin, A.I.; Callahan, M.A. Modeling the Public Health Response to Bioterrorism: Using Discrete Event Simulation to Design Antibiotic Distribution Centers. Med. Decis. Mak. 2002, 22, 17–25. [Google Scholar] [CrossRef]
- Hupert, N.; Xiong, W.; King, K.; Castorena, M.; Hawkins, C.; Wu, C.; Muckstadt, J.A. Uncertainty and Operational Considerations in Mass Prophylaxis Workforce Planning. Disaster Med. Public Health Prep. 2009, 3, S121–S131. [Google Scholar] [CrossRef]
- Hernandez, I.; Ramirez-Marquez, J.E.; Starr, D.; McKay, R.; Guthartz, S.; Motherwell, M.; Barcellona, J. Optimal staffing strategies for points of dispensing. Comput. Ind. Eng. 2015, 83, 172–183. [Google Scholar] [CrossRef]
- Ramirez-Nafarrate, A.; Lyon, J.D.; Fowler, J.; Araz, O.M. Point-of-Dispensing Location and Capacity Optimization via a Decision Support System. Prod. Oper. Manag. 2015, 24, 1311–1328. [Google Scholar] [CrossRef]
- Hudgeons, A. Dispensing Medical Countermeasures in Public Health Emergencies via Home Health Agencies and Points of Distribution. Master’s Thesis, University of Arkansas, Fayetteville, AR, USA, 2018. Available online: http://scholarworks.uark.edu/ineguht/59 (accessed on 11 November 2020).
- Asgary, A.; Najafabadi, M.M.; Karsseboom, R.; Wu, J. A Drive-through Simulation Tool for Mass Vaccination during COVID-19 Pandemic. Healthcare 2020, 8, 469. [Google Scholar] [CrossRef] [PubMed]
- Obsie, E.Y.; Qu, H.; Drummond, F. Wild blueberry yield prediction using a combination of computer simulation and machine learning algorithms. Comput. Electron. Agric. 2020, 178, 105778. [Google Scholar] [CrossRef]
- Sanchez, S.M.; Sanchez, P.J.; Wan, H. Work smarter, not harder: A tutorial on designing and conducting simulation experiments. In Proceedings of the 2018 Winter Simulation Conference (WSC), Gothenburg, Sweden, 9–12 December 2018; Institute of Electrical and Electronics Engineers (IEEE): Piscataway, NJ, USA, 2018; pp. 237–251. [Google Scholar]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Value |
|---|---|
| Lane 1-Lane10 | Open |
| Minimum number of passengers in cars | 1 |
| Maximum number of passengers in cars | 5 |
| Number of cars coming to drive through per min | 5 |
| Average registration time (min) | 4.24 |
| Average vaccination time (min) | 3.26 |
| Average recovery time (min) | 4 |
| Number of staff in each station in lane 1-lane10 | 4 |
| Assign High Occupancy Lanes (HOV) | FALSE |
| Fraction of cars pre-registered for vaccination (0–1) | 50 |
| Pre-registration impact factor (0–1) | 0.5 |
| Consider pre-registration | TRUE |
| Low occupancy vehicle | FALSE |
| Fraction of non-adult passengers | 0.15 |
| Fraction of cars rejected at screening | 0.01 |
| Shift hours | 8 |
| Number of shifts | 3 |
| Average screening time | 0.5 |
| Minimum screening time | 0.25 |
| Maximum screening time | 0.5 |
| Dynamically learn and adjust cars going to each lane | TRUE |
| Use schedule for incoming cars | FALSE |
| Parameter | Range | Notes |
|---|---|---|
| Average recovery time (min) | 5–10 | |
| Average registration time (min) | 2–7 | |
| Average screening time | 0.25–1 | |
| Maximum screening time | 1 | fixed |
| Minimum screening time | 0.25 | fixed |
| Average vaccination time (min) | 2–7 | |
| Maximum number of passengers in cars | 5–7 | integer only |
| Minimum number of passengers in cars | 1 | fixed |
| Fraction of non-adult passengers | 0.15–0.30 | |
| Number of cars coming to drive through per minute | 0.5–5 | |
| Fraction of cars rejected at screening | 0.01 | fixed |
| Shift hours | 6, 8 or 12 | |
| Number of shifts | 2, 3 or 4 | Depending on shift hours such that total hours = 24 |
| Days | 1 | fixed |
| Lanes 1–10 | True or False | At least 1 lane is always open |
| Number of staff in each lane | 1–4 | Can differ lane to lane, integer only |
| Consider pre-registration | True or False | |
| Assign High Occupancy Lanes (HOV) | True or False | |
| Dynamically learn and adjust cars going to each lane | True or False | Can only be true if HOV is open |
| Low occupancy vehicle | True or False | Can only be true if HOV is open |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Asgary, A.; Valtchev, S.Z.; Chen, M.; Najafabadi, M.M.; Wu, J. Artificial Intelligence Model of Drive-Through Vaccination Simulation. Int. J. Environ. Res. Public Health 2021, 18, 268. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18010268
Asgary A, Valtchev SZ, Chen M, Najafabadi MM, Wu J. Artificial Intelligence Model of Drive-Through Vaccination Simulation. International Journal of Environmental Research and Public Health. 2021; 18(1):268. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18010268
Chicago/Turabian StyleAsgary, Ali, Svetozar Zarko Valtchev, Michael Chen, Mahdi M. Najafabadi, and Jianhong Wu. 2021. "Artificial Intelligence Model of Drive-Through Vaccination Simulation" International Journal of Environmental Research and Public Health 18, no. 1: 268. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18010268