Perinatal Anxiety Symptoms: Rates and Risk Factors in Mexican Women


Abstract
:1. Introduction
2. Materials and Methods
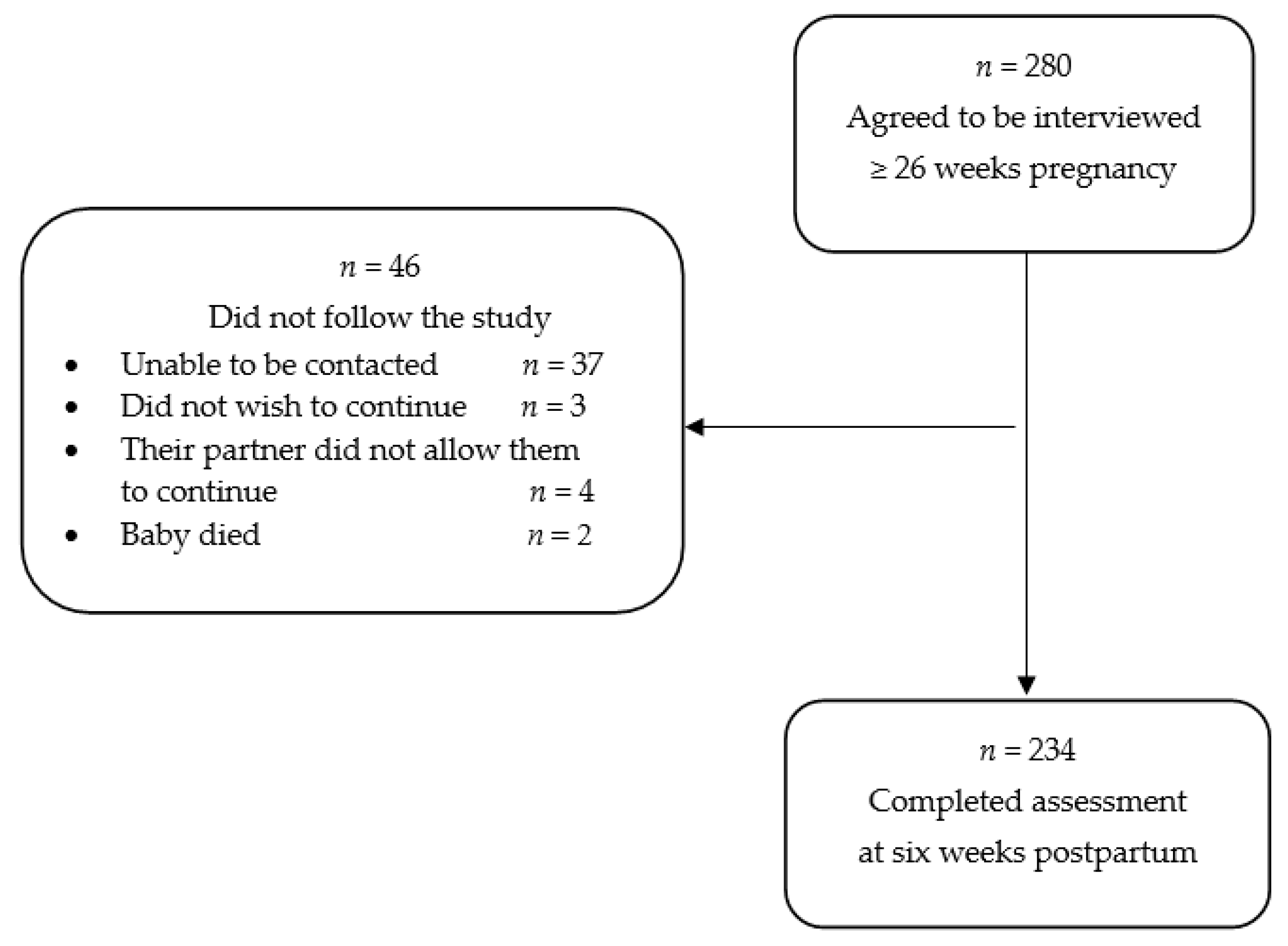
2.1. Participants
2.2. Procedures
2.3. Measures
2.4. Data Analyses
3. Results
3.1. Participants
3.2. PAS Prevalence Rates and Risk Factors
3.3. Regressions to Determine the Effects of Risk and Protective Factors on PAS
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- O’Hara, M.W.; Wisner, K.L. Perinatal mental illness: Definition, description and aetiology. Best Pract. Res. Clin. Obstet. Gynaecol. 2014, 28, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Harrison, V.; Moore, D.; Lazard, L. Supporting perinatal anxiety in the digital age; a qualitative exploration of stressors and support strategies. BMC Pregnancy Childbirth 2020, 20, 363. [Google Scholar] [CrossRef] [PubMed]
- Field, T. Prenatal anxiety effects: A review. Infant Behav. Dev. 2017, 49, 120–128. [Google Scholar] [CrossRef] [PubMed]
- Field, T. Postnatal anxiety prevalence, predictors and effects on development: A narrative review. Infant Behav. Dev. 2018, 51, 24–32. [Google Scholar] [CrossRef] [PubMed]
- Dennis, C.L.; Falah-Hassani, K.; Shiri, R. Prevalence of antenatal and postnatal anxiety: Systematic review and meta-analysis. Br. J. Psychiatry 2017, 210, 315–323. [Google Scholar] [CrossRef]
- Becerra, D.; Hernandez, G.; Porchas, F.; Castillo, J.; Nguyen, V.; Perez González, R. Immigration policies and mental health: Examining the relationship between immigration enforcement and depression, anxiety, and stress among Latino immigrants. J. Ethn. Cult. Divers. Soc. Work 2020, 29, 43–59. [Google Scholar] [CrossRef]
- Donato, K.M.; Caron, L.; Hamilton, E. Migration and mental health in Mexico: Domestic migrants, return U.S. migrants, and non-migrants. Front. Psychiatry 2019, 10, 970. [Google Scholar] [CrossRef]
- Farina, A.S.J.; Kremer, K.P.; Caldera Wimmer, S.; Villarreal-Otalera, T.; Paredes, T.; Stuart, E. Anxiety, depression, and trauma among immigrant Mexican women up to two-years post-partum. J. Immigr. Minority Health 2020. [Google Scholar] [CrossRef]
- Navarrete, L.E.; Lara, M.A.; Navarro, C.; Gomez, M.E.; Morales, F. Psychosocial factors predicting postnatal anxiety symptoms and their relation to symptoms of postpartum depression. Rev. Investig. Clin. 2012, 64, 625–633. [Google Scholar]
- Lara, M.A.; Navarrete, L.; Nieto, L. Prenatal predictors of postpartum depression and postpartum depressive symptoms in Mexican mothers: A longitudinal study. Arch. Women’s Ment. Health 2016, 19, 825–834. [Google Scholar] [CrossRef]
- Weiss-Laxer, N.S.; Johnson, S.B.; Ghazarian, S.R.; Osborne, L.M.; Riley, A.W. Maternal behavioral health symptom profiles in early family life: Complexity and context. Arch. Women’s Ment. Health 2020, 23, 429–439. [Google Scholar] [CrossRef] [PubMed]
- De Castro, F.; Place, J.M.; Billings, D.L.; Rivera, L.; Frongillo, E.A. Risk profiles associated with postnatal depressive symptoms among women in a publicsector hospital in Mexico: The role of sociodemographic and psychosocial factors. Arch. Women’s Ment. Health 2015, 18, 463–471. [Google Scholar] [CrossRef]
- Chen, H.H.; Chien, L.Y. A comparative study of domestic decision-making power and social support as predictors of postpartum depressive and physical symptoms between immigrant and native-born women. PLoS ONE 2020, 15, e0231340. [Google Scholar] [CrossRef] [PubMed]
- Gao, L.; Qu, J.; Wang, A.Y. Anxiety, depression and social support in pregnant women with a history of recurrent miscarriage: A cross-sectional study. J. Reprod. Infant Psychol. 2020, 38, 497–508. [Google Scholar] [CrossRef]
- Marcos-Najera, R.; Rodriguez-Munoz, M.F.; Lara, M.A.; Navarrete, L.; Le, H.N. A cross-cultural analysis of the prevalence and risk factors for prenatal depression in Spain and Mexico. Cult. Med. Psychiatry 2020. [Google Scholar] [CrossRef] [PubMed]
- Mukherjee, S.; Fennie, K.; Coxe, S.; Madhivanan, P.; Trepka, M.J. Racial and ethnic differences in the relationship between antenatal stressful life events and postpartum depression among women in the United States: Does provider communication on perinatal depression minimize the risk? Ethn. Health 2018, 23, 542–565. [Google Scholar] [CrossRef] [PubMed]
- Recto, P.; Champion, J.D. Social support and perinatal depression: The perspectives of Mexican-American adolescent mothers. Issues Ment. Health Nurs. 2020, 41, 932–939. [Google Scholar] [CrossRef] [PubMed]
- Lara, M.A.; Le, H.N.; Letechipia, G.; Hochhausen, L. Prenatal depression in Latinas in the U.S. and Mexico. Matern. Child Health J. 2009, 13, 567–576. [Google Scholar] [CrossRef]
- Clout, D.; Brown, R. Sociodemographic, pregnancy, obstetric, and postnatal predictors of postpartum stress, anxiety and depression in new mothers. J. Affect. Disord. 2015, 188, 60–67. [Google Scholar] [CrossRef]
- Ricardo-Ramírez, C.; Álvarez-Gómez, M.; Ocampo-Saldarriaga, M.V.; Tirado-Otálvaro, A.F. Prevalencia de tamizaje positivo para depresión y ansiedad en gestantes de alto riesgo obstétrico en una clínica de Medellín, entre enero y agosto de 2013. Factores de riesgo asociados. Rev. Colomb. Obstet. Ginecol. 2015, 66, 94–102. [Google Scholar] [CrossRef] [Green Version]
- Umuziga, M.P.; Adejumo, O.; Hynie, M. A cross-sectional study of the prevalence and factors associated with symptoms of perinatal depression and anxiety in Rwanda. BMC Pregnancy Childbirth 2020, 20, 68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, X.; Wang, Y.; Hu, H.; Tao, X.G.; Zhang, Y.; Shi, H. The impact of resilience on prenatal anxiety and depression among pregnant women in Shanghai. J. Affect. Disord. 2019, 250, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Johannesen-Schmidt, M.C.; Eagly, A.H. Another look at sex differences in preferred mate characteristics: The effects of endorsing the traditional female gender role. Psychol. Women Q. 2002, 26, 322–328. [Google Scholar] [CrossRef]
- Lara, M.A. Inventario de Masculinidad-Femineidad: IMAFE; El Manual Moderno: Mexico City, Mexico, 1993. [Google Scholar]
- Albuja, A.F.; Lara, M.A.; Navarrete, L.; Nieto, L. Social support and postpartum depression revisited: The traditional female role as moderator among Mexican women. Sex Roles 2017, 77, 209–220. [Google Scholar] [CrossRef]
- Derogatis, L.R. Administration, Scoring and Procedures Manual-I for the Revised Version SCL-90R; Johns Hopkins University School of Medicine: Baltimore, MD, USA, 1977. [Google Scholar]
- Cruz-Fuentes, C.; López, L.; Blas-Gracia, C.; González, L.; Chávez, R. Datos sobre la validez y la confiabilidad de la Symptom Check List (SCL-90) en una muestra de sujetos mexicanos. Salud Ment. 2005, 28, 72–81. [Google Scholar]
- Lara, C.; Espinosa, I.; Cárdenas, M.L.; Fócil, M.; Cavazos, J. Confiabilidad y validez de la SCL-90 en la evaluación de psicopatología en mujeres. Salud Ment. 2005, 28, 42–50. [Google Scholar]
- Meades, R.; Ayers, S. Anxiety measures validated in perinatal populations: A systematic review. J. Affect. Disord. 2011, 133, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B. Validation and utility of a self-report version of PRIME-MD: The PHQ primary care study. Primary care evaluation of mental disorders. Patient Health Questionnaire. JAMA 1999, 282, 1737–1744. [Google Scholar] [CrossRef] [Green Version]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Familiar, I.; Ortiz-Panozo, E.; Hall, B.; Vieitez, I.; Romieu, I.; Lopez-Ridaura, R.; Lajous, M. Factor structure of the Spanish version of the Patient Health Questionnaire-9 in Mexican women. Int. J. Methods Psychiatr. Res. 2015, 24, 74–82. [Google Scholar] [CrossRef]
- Gaxiola Romero, J.C.; Frías Armenta, M.; Hurtado Abril, M.F.; Salcido Noriega, L.C.; Figueroa Franco, M. Validación del inventario de resiliencia (IRES) en una muestra del noroeste de México. Enseñanza Investig. Psicol. 2011, 16, 73–83. [Google Scholar]
- Nieto, L.; Lara, M.A.; Navarrete, L.; Duenas, K.; Rodriguez, K. Psychometric properties of the resilience inventory for pregnant Mexican women. Summa Psicol. 2018, 15, 35–42. [Google Scholar] [CrossRef]
- Lara, M.A.; Navarro, C.; Navarrete, L. The influence of life events and social support in a psycho-educational intervention for women with depression. Salud Pública Mex. 2004, 46, 378–387. [Google Scholar] [CrossRef]
- Holmes, T.H.; Rahe, R.H. The social readjustment rating scale. J. Psychosom. Res. 1967, 11, 213–218. [Google Scholar] [CrossRef]
- Lara, M.A.; Navarro, C.; Navarrete, L. Outcome results of a psycho-educational intervention in pregnancy to prevent PPD: A randomized control trial. J. Affect. Disord. 2010, 122, 109–117. [Google Scholar] [CrossRef] [PubMed]
- Genovez, M.; Le, H. Identification of Salvadoran pregnant women at risk for postpartum depression. In Proceedings of the Poster Presentation, 25th Annual Conference Postpartum Support International, Seattle, WA, USA, 16 September 2011; pp. 14–18. [Google Scholar]
- Records, K.; Rice, M.; Beck, C.T. Psychometric assessment of the postpartum depression predictors inventory-revised. J. Nurs. Meas. 2007, 15, 189–202. [Google Scholar] [CrossRef] [PubMed]
- Ibarra-Yruegas, B.; Lara, M.A.; Navarrete, L.; Nieto, L.; Kawas Valle, O. Psychometric properties of the Postpartum Depression Predictors Inventory-revised for pregnant women in Mexico. J. Health Psychol. 2018, 23, 1415–1423. [Google Scholar] [CrossRef]
- Martínez-Gómez, J.A.; Guerrero-Rodríguez, S.I.; Rey-Anacona, C.A. Assessment of construct validity and reliability of the inventory of masculinity and femininity in adolescents and young Colombian adults. Av. Psicol. Latinoam. 2012, 30, 170–181. [Google Scholar]
- Rey, C.A. Pro-social skills, gender personality traits and acceptance of violence toward women in adolescents who have witnessed violence in their parents/Habilidades prosociales, rasgos de personalidad de género y aceptación de la violencia hacia la mujer, en adolescentes que han presenciado violencia entre sus padres. Acta Colomb. Psicol. 2008, 11, 107–119. [Google Scholar]
- Feligreras-Alcala, D.; Frias-Osuna, A.; Del-Pino-Casado, R. Personal and family resources related to depressive and anxiety symptoms in women during puerperium. Int. J. Environ. Res. Public Health 2020, 17, 5230. [Google Scholar] [CrossRef]
- Aktan, N.M. Social support and anxiety in pregnant and postpartum women: A secondary analysis. Clin. Nurs. Res. 2012, 21, 183–194. [Google Scholar] [CrossRef] [PubMed]
- Razurel, C.; Kaiser, B.; Antonietti, J.P.; Epiney, M.; Sellenet, C. Relationship between perceived perinatal stress and depressive symptoms, anxiety, and parental self-efficacy in primiparous mothers and the role of social support. Women Health 2017, 57, 154–172. [Google Scholar] [CrossRef] [PubMed]
- United Nations International Children’s Emergency Fund. Progress for Every Child in the SDG Era Country Profile; UNICEF: Mexico City, Mexico, 2016. [Google Scholar]
- Lara-Cinisomo, S.; Clark, C.T.; Wood, J. Increasing diagnosis and treatment of perinatal depression in Latinas and African American women: Addressing stigma is not enough. Women’s Health Issues 2018, 28, 201–204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caballero, M.; Leyva-Flores, R.; Ochoa-Marin, S.C.; Zarco, A.; Guerrero, C. Women who are left behind: The impact of international migration on the process of seeking health care. Salud Pública Mex. 2008, 50, 241–250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lancaster, C.A.; Gold, K.J.; Flynn, H.A.; Yoo, H.; Marcus, S.M.; Davis, M.M. Risk factors for depressive symptoms during pregnancy: A systematic review. Am. J. Obstet. Gynecol. 2010, 202, 5–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leahy-Warren, P.; McCarthy, G.; Corcoran, P. First-time mothers: Social support, maternal parental self-efficacy and postnatal depression. J. Clin. Nurs. 2012, 21, 388–397. [Google Scholar] [CrossRef] [PubMed]
- Ramakrishna, S.; Cooklin, A.R.; Leach, L.S. Comorbid anxiety and depression: A community-based study examining symptomology and correlates during the postpartum period. J. Reprod. Infant Psychol. 2019, 37, 468–479. [Google Scholar] [CrossRef] [Green Version]
- Choi, K.W.; Kim, Y.K.; Jeon, H.J. Comorbid anxiety and depression: Clinical and conceptual consideration and transdiagnostic treatment. Adv. Exp. Med. Biol. 2020, 1191, 219–235. [Google Scholar] [CrossRef]
- Dagher, R.K.; Bruckheim, H.E.; Colpe, L.J.; Edwards, E.; White, D.B. Perinatal depression: Challenges and opportunities. J. Women’s Health 2020. [Google Scholar] [CrossRef]
- Woody, C.A.; Ferrari, A.J.; Siskind, D.J.; Whiteford, H.A.; Harris, M.G. A systematic review and meta-regression of the prevalence and incidence of perinatal depression. J. Affect. Disord. 2017, 219, 86–92. [Google Scholar] [CrossRef] [Green Version]
- Lara-Cinisomo, S.; Grewen, K.M.; Girdler, S.S.; Wood, J.; Meltzer-Brody, S. Perinatal depression, adverse life events, and hypothalamic-adrenal-pituitary axis response to cold pressor stress in Latinas: An exploratory study. Women’s Health Issues 2017, 27, 673–682. [Google Scholar] [CrossRef] [PubMed]
- Lara-Cinisomo, S.; McKenney, K.; Di Florio, A.; Meltzer-Brody, S. Associations between postpartum depression, breastfeeding, and oxytocin levels in Latina mothers. Breastfeed. Med. 2017, 12, 436–442. [Google Scholar] [CrossRef] [PubMed]
- Mukherjee, S.; Trepka, M.J.; Pierre-Victor, D.; Bahelah, R.; Avent, T. Racial/ethnic disparities in antenatal depression in the United States: A systematic review. Matern. Child Health J. 2016, 20, 1780–1797. [Google Scholar] [CrossRef] [PubMed]
- Lara-Cinisomo, S.; Wood, J.; Fujimoto, E. A systematic review of cultural orientation and perinatal depression in Latina women: Are acculturation, Marianismo, and religiosity risks or protective factors? Arch. Women’s Ment. Health 2019, 22, 557–567. [Google Scholar] [CrossRef] [PubMed]
- Hackett, R.A.; Steptoe, A.; Jackson, S.E. Sex discrimination and mental health in women: A prospective analysis. Health Psychol. 2019, 38, 1014–1024. [Google Scholar] [CrossRef]
- Navarro, D.M.; Robles, J.N.; Hernández, L.O. La mujer en México: Inequidad, pobreza y violencia. Rev. Mex. Cienc. Políticas Soc. 2014, 59, 117–146. [Google Scholar] [CrossRef] [Green Version]
- Rafful, C.; Medina-Mora, M.E.; Borges, G.; Benjet, C.; Orozco, R. Depression, gender, and the treatment gap in Mexico. J. Affect. Disord. 2012, 138, 165–169. [Google Scholar] [CrossRef]
- Diaz-Loving, R.; Aragon, S.R.; Aragóon, R.S. Rasgos instrumentales (masculinos) y expresivos (femeninos). Rev. Latinoam. Psicol. 2001, 33, 131–139. [Google Scholar]
- DiGirolamo, A.M.; de Snyder, N.S. Women as primary caregivers in Mexico: Challenges to well-being. Salud Pública Mex. 2008, 50, 516–522. [Google Scholar] [CrossRef] [Green Version]
- Michl, L.C.; McLaughlin, K.A.; Shepherd, K.; Nolen-Hoeksema, S. Rumination as a mechanism linking stressful life events to symptoms of depression and anxiety: Longitudinal evidence in early adolescents and adults. J. Abnorm. Psychol. 2013, 122, 339–352. [Google Scholar] [CrossRef] [Green Version]
- Gress-Smith, J.L.; Roubinov, D.S.; Tanaka, R.; Cmic, K.; Gonzales, N.; Enders, C.; Luecken, L.J. Prenatal expectations in Mexican American women: Development of a culturally sensitive measure. Arch. Womens Ment. Health 2013, 16, 303–314. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Negron, R.; Martin, A.; Almog, M.; Balbierz, A.; Howell, E.A. Social support during the postpartum period: Mothers’ views on needs, expectations, and mobilization of support. Matern. Child Health J. 2013, 17, 616–623. [Google Scholar] [CrossRef] [Green Version]
- Razurel, C.; Kaiser, B. The role of satisfaction with social support on the psychological health of primiparous mothers in the perinatal period. Women Health 2015, 55, 167–186. [Google Scholar] [CrossRef] [PubMed]
- Stein, G.L.; Guzman, L.E. Prevention and intervention research with Latino families: A translational approach. Fam. Process 2015, 54, 280–292. [Google Scholar] [CrossRef] [PubMed]
- Le, H.N.; Zmuda, J.; Perry, D.F.; Muñoz, R.F. Transforming an evidence-based intervention to prevent perinatal depression for low-income Latina immigrants. Am. J. Orthopsychiatry 2010, 80, 34–45. [Google Scholar] [CrossRef] [PubMed]
- Baker-Ericzén, M.J.; Connelly, C.D.; Hazen, A.L.; Dueñas, C.; Landsverk, J.A.; Horwitz, S.M. A collaborative care telemedicine intervention to overcome treatment barriers for Latina women with depression during the perinatal period. Fam. Syst. Health 2012, 30, 224–240. [Google Scholar] [CrossRef] [Green Version]
- Marsiglia, F.F.; Kulis, S.; Garcia Perez, H.; Bermudez-Parsai, M. Hopelessness, family stress, and depression among Mexican-heritage mothers in the southwest. Health Soc. Work 2011, 36, 7–18. [Google Scholar] [CrossRef] [Green Version]
- Garcia-Gonzalez, J.; Ventura-Miranda, M.I.; Requena-Mullor, M.; Parron-Carreño, T.; Alarcon-Rodriguez, R. State-trait anxiety levels during pregnancy and foetal parameters following intervention with music therapy. J. Affect. Disord. 2018, 232, 17–22. [Google Scholar] [CrossRef]
- Hepp, P.; Hagenbeck, C.; Gilles, J.; Wolf, O.T.; Goertz, W.; Janni, W.; Balan, P.; Fleisch, M.; Fehm, T.; Schaal, N.K. Effects of music intervention during caesarean delivery on anxiety and stress of the mother a controlled, randomised study. BMC Pregnancy Childbirth 2018, 18, 435. [Google Scholar] [CrossRef] [Green Version]
- Lara-Cinisomo, S.; Wisner, K.L. (Eds.) Perinatal Depression Among Spanish-Speaking Women: A global Perspective on Prevalence, Treatment, and Outcomes; Springer: New York, NY, USA, 2014. [Google Scholar] [CrossRef]


{kind=link}
| SD | |||
|---|---|---|---|
| Age | 28.9 | 6.2 | |
| Monthly family income | 498.7 | 502.3 | |
| Educational attainment (years) | 12.7 | 3.8 | |
| Number of children | 0.81 | 0.89 | |
| n | % | ||
| Marital status | Partnered | 223 | 79.6 |
| Single | 57 | 20.4 | |
| Delivery | Vaginal | 85 | 36.3 |
| Cesarean | 149 | 63.7 | |
| Resilience during pregnancy | Low | 57 | 20.4 |
| High | 223 | 79.6 | |
| Traditional female role during pregnancy | Low | 206 | 73.6 |
| High | 74 | 26.4 | |
| Marital satisfaction during pregnancy | Low | 68 | 24.3 |
| High | 212 | 75.7 | |
| Social support during pregnancy | Low | 42 | 15.0 |
| High | 238 | 85.0 | |
| Stressful life events during pregnancy | With events | 59 | 21.1 |
| Without events | 221 | 78.9 | |
| Depressive symptoms during pregnancy | With symptoms | 57 | 20.4 |
| Without symptoms | 223 | 79.6 | |
| Social support during the postpartum period | Low | 40 | 17.1 |
| High | 194 | 82.9 | |
| Stressful life events during the postpartum period | With events | 45 | 16.1 |
| Without events | 189 | 67.5 | |
| Depressive symptoms during the postpartum period | With symptoms | 40 | 20.1 |
| Without symptoms | 194 | 79.9 |
| Pregnancy (n = 280) | Sixth Week Postpartum (n = 234) | |
|---|---|---|
| n (%) | n (%) | |
| With anxiety symptoms | 62 (22.1) | 41 (17.5) |
| Without anxiety symptoms | 218 (77.9) | 193 (82.5) |
| Variables | Time 1. Pregnancy (n = 280) | Time 2. Sixth Week Postpartum (n = 234) |
|---|---|---|
| OR (95% CI) | OR (95% CI) | |
| Age | 0.99 (0.95–1.04) | 0.97 (0.92–1.03) |
| Monthly family income | 0.99 (0.89–1.03) | 0.99 (0.84–1.49) |
| Single | 2.59 (1.37–4.90) * | 2.25 (1.05–4.80) * |
| Educational attainment | 0.95 (0.89–1.03) | 0.89 (0.81–0.97) * |
| Number of children | 1.10 (0.81–1.50) | 1.31 (0.78–1.63) |
| Cesarean delivery | -- | 1.15 (0.57–2.29) |
| Low resilience during pregnancy | 2.87 (1.52–5.41) ** | 2.24 (1.03–4.89) * |
| Traditional female role during pregnancy | 4.07 (2.23–7.41) ** | 1.95 (0.95–4.01) |
| Low marital satisfaction during pregnancy | 4.03 (2.19–7.40) ** | 2.43 (1.17–2.42) * |
| Low social support during pregnancy | 6.17 (3.07–12.41) ** | 6.63 (2.85–15.42) ** |
| Stressful life events during pregnancy | 8.40 (4.40–16.02) ** | 3.47 (1.66–7.27) ** |
| Depressive symptoms during pregnancy | 6.63 (3.49–12.58) ** | 4.55 (2.15–9.59) ** |
| Low social support during the postpartum period | -- | 2.85 (1.31–6.18) * |
| Stressful life events during the postpartum period | -- | 7.39 (3.50–15.60) ** |
| Depressive symptoms during the postpartum period | -- | 11.25 (5.14–24.61) ** |
| Pregnancy (n = 280) | ||
|---|---|---|
| OR | 95% CI | |
| Age | 1.01 | 0.95–1.08 |
| Monthly family income | 0.99 | 0.93–1.10 |
| Educational attainment | 1.06 | 0.94–1.20 |
| Number of children | 0.85 | 1.50–6.68 |
| Single | 1.72 | 0.70–4.25 |
| Low resilience during pregnancy | 1.16 | 0.48–2.78 |
| Traditional female role during pregnancy | 2.28 * | 1.06–4.88 |
| Low marital satisfaction during pregnancy | 1.32 | 0.54–3.25 |
| Low social support during pregnancy | 2.25 | 0.92–5.50 |
| Stressful life events during pregnancy | 4.35 ** | 2.02–9.37 |
| Depressive symptoms during pregnancy | 3.82 ** | 1.72–8.48 |
| Six Weeks Postpartum (n = 234) | ||
|---|---|---|
| OR | 95% CI | |
| Age | 0.94 | 0.86–1.03 |
| Monthly family income | 0.99 | 0.96–1.22 |
| Educational attainment | 0.84 * | 0.72–0.99 |
| Number of children | 0.82 | 0.32–2.11 |
| Single | 3.03 | 0.92–9.80 |
| Cesarean delivery section | 1.01 | 0.37–2.68 |
| Low resilience during pregnancy | 2.00 | 0.65–6.11 |
| Traditional female role during pregnancy | 0.90 | 0.31–3.08 |
| Low marital satisfaction during pregnancy | 5.06 | 1.50–20.84 |
| Low social support during pregnancy | 2.25 * | 0.92–5.50 |
| Stressful life events during pregnancy | 0.98 | 0.31–3.08 |
| Depressive symptoms during pregnancy | 1.89 | 0.66–5.37 |
| Low social support during the postpartum period | 0.30 | 0.07–1.19 |
| Stressful life events during the postpartum period | 5.42 ** | 1.84–15.89 |
| Depressive symptoms during the postpartum period | 9.03 ** | 3.24–15.12 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Juarez Padilla, J.; Lara-Cinisomo, S.; Navarrete, L.; Lara, M.A. Perinatal Anxiety Symptoms: Rates and Risk Factors in Mexican Women. Int. J. Environ. Res. Public Health 2021, 18, 82. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18010082
Juarez Padilla J, Lara-Cinisomo S, Navarrete L, Lara MA. Perinatal Anxiety Symptoms: Rates and Risk Factors in Mexican Women. International Journal of Environmental Research and Public Health. 2021; 18(1):82. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18010082
Chicago/Turabian StyleJuarez Padilla, Janeth, Sandraluz Lara-Cinisomo, Laura Navarrete, and Ma. Asunción Lara. 2021. "Perinatal Anxiety Symptoms: Rates and Risk Factors in Mexican Women" International Journal of Environmental Research and Public Health 18, no. 1: 82. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18010082