
Promoting the Psychological Well-Being of Healthcare Providers Facing the Burden of Adverse Events: A Systematic Review of Second Victim Support Resources

 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
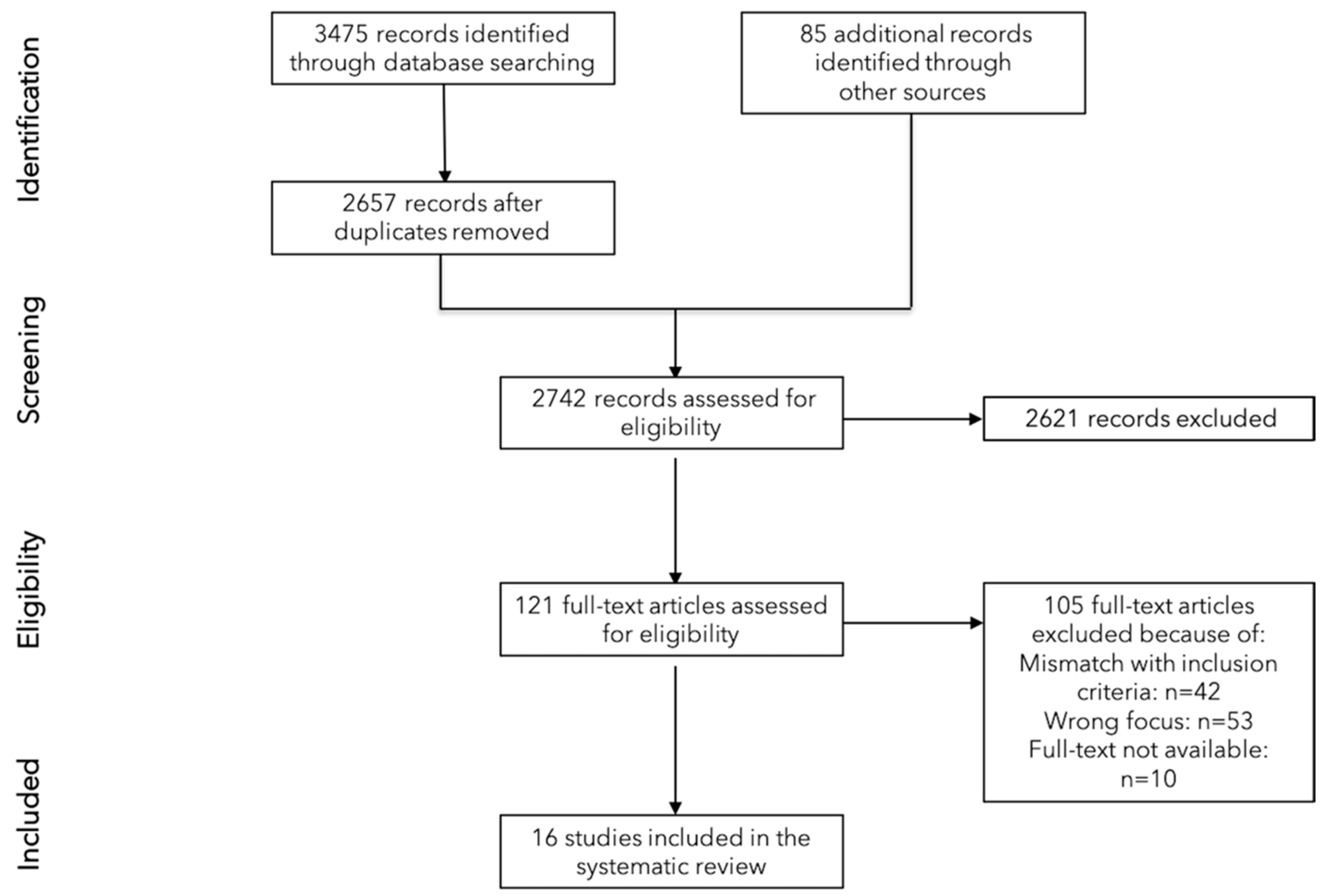
2.1. Searches
2.2. Inclusion and Exclusion Criteria
- (1)
- the development and/or the implementation and/or the evaluation of support resources for second victims (i.e., support program, toolkit, course) were described. Second victims include all healthcare providers (e.g., physicians, nurses, midwives) involved in adverse events/patient safety incidents regardless of their profession, age or other sociodemographic characteristics;
- (2)
- the support program was described in detail elucidating every step of the support strategy;
- (3)
- the support program was part of a structured intervention organized and/or promoted by their healthcare institution.
2.3. Risk of Bias Assessment
2.4. Outcome Measures
- (1)
- a descriptive overview of second victims support resources developed around the world;
- (2)
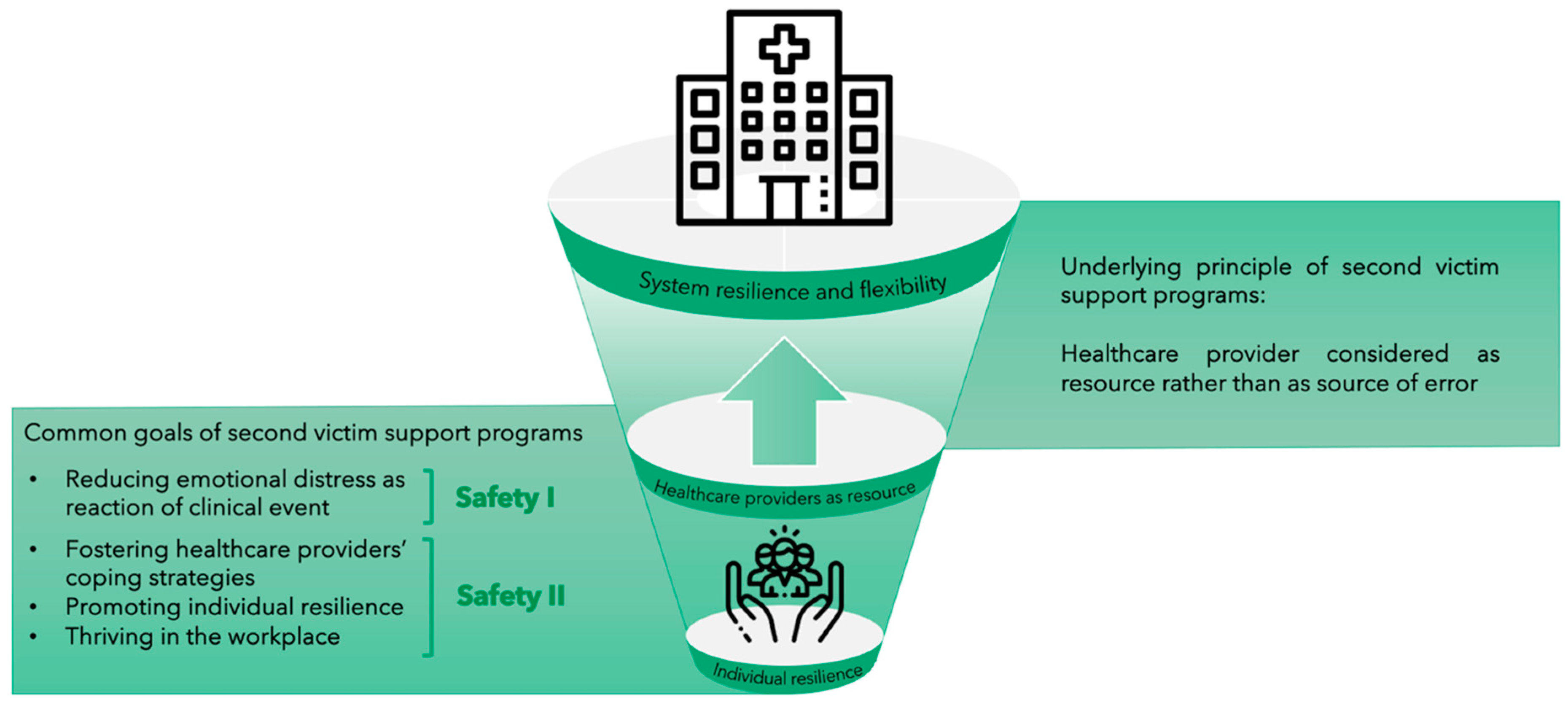
- their conceptual basis, including aspects/elements of the Safety I (i.e., mostly reactive approach focusing on identifying risks and causes of adverse outcomes, and limiting their reoccurrence) and Safety II approach (i.e., proactive approach focusing on identifying resources and key elements of a positive performance, and promoting resilience at the individual and institutional level);
- (3)
- programs’ benefits for second victims;
- (4)
- personal perceptions and experiences of peer supporters; and
- (5)
- challenges encountered during the implementation of the support resources.
2.5. Data Extraction and Synthesis
3. Results
3.1. Risk of Bias Assessment
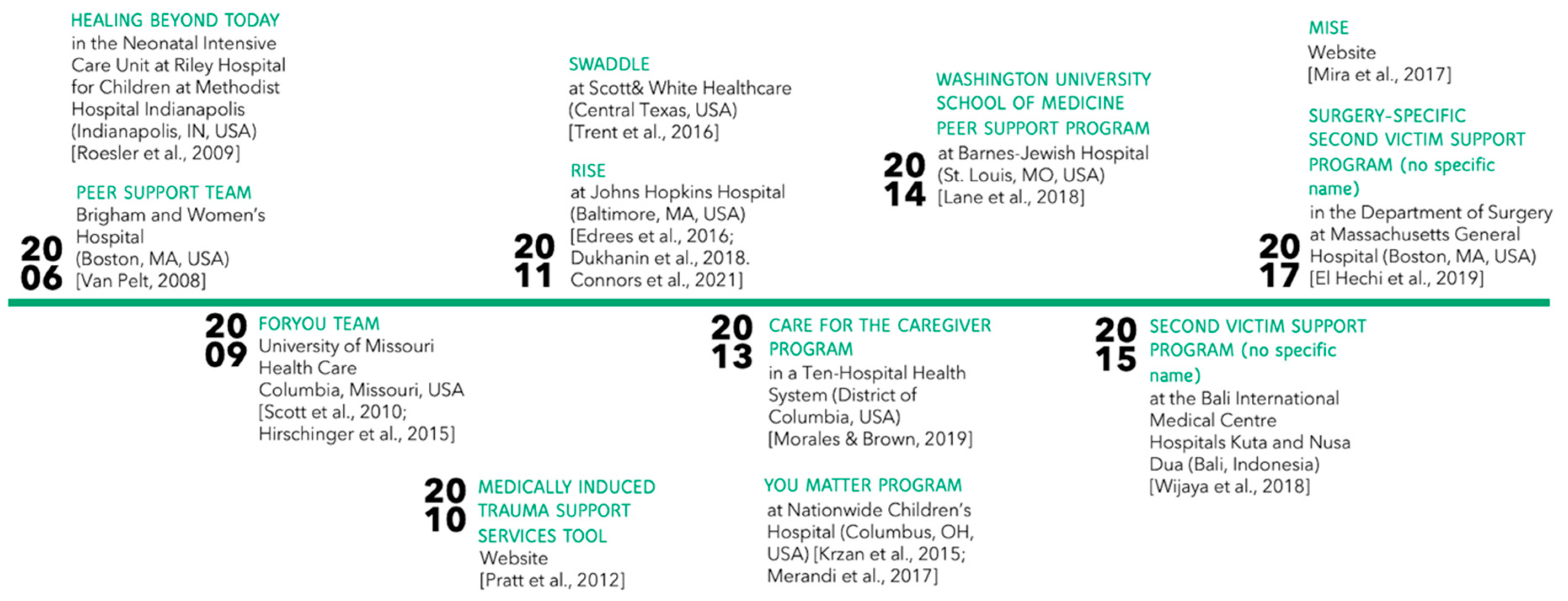
3.2. Second Victim Support Resources
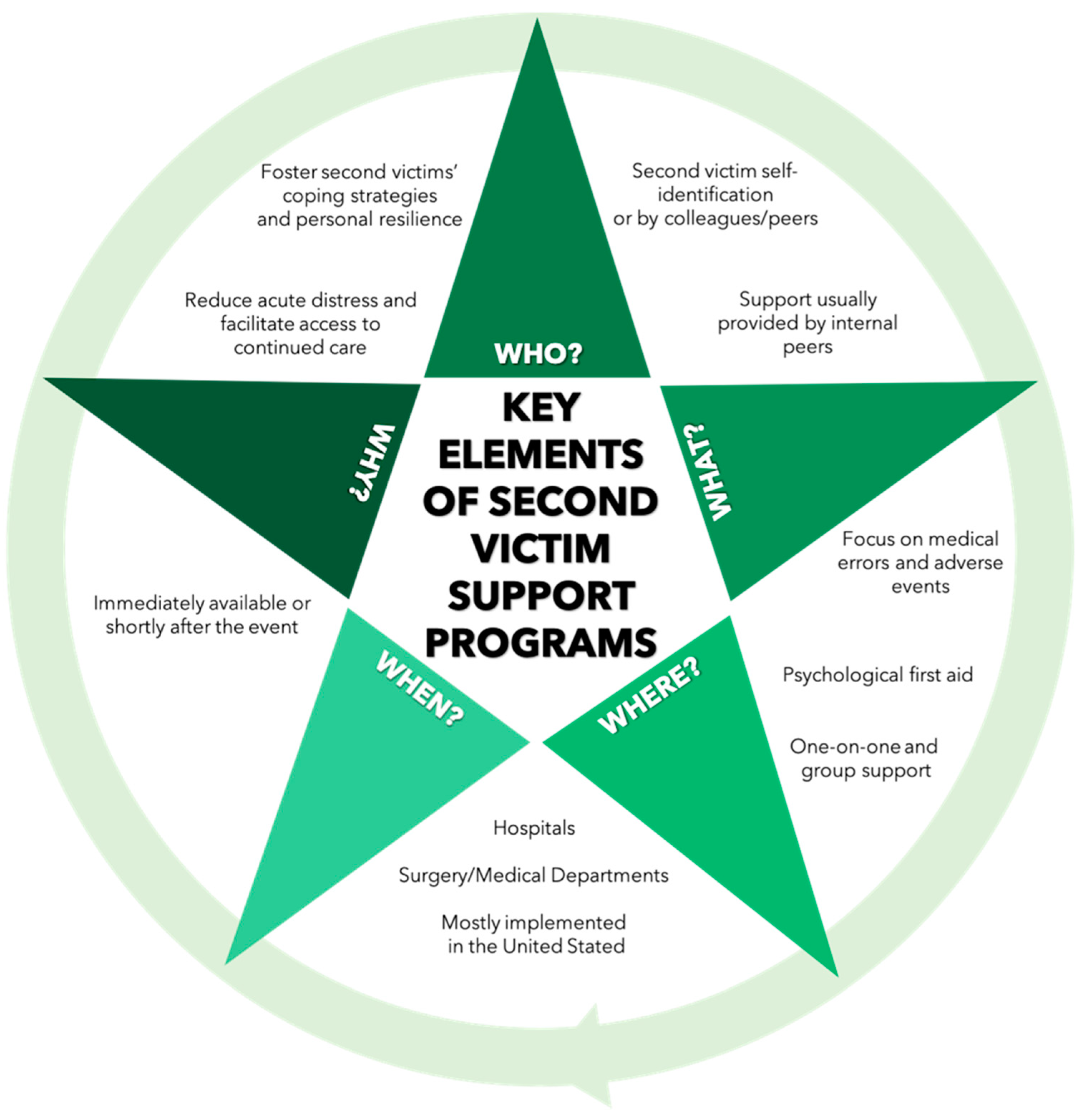
3.2.1. Main Characteristics
3.2.2. Conceptual Basis of Second Victim Support Resources
Incorporated Elements of Safety I and Safety II
3.2.3. Descriptive Statistics of Support Encounters
3.2.4. Descriptive Statistics of Supported Staff and Peer Supporters
3.3. Benefits of Support Programs for Second Victims
3.4. Personal Perceptions and Experiences of Peer Supporters
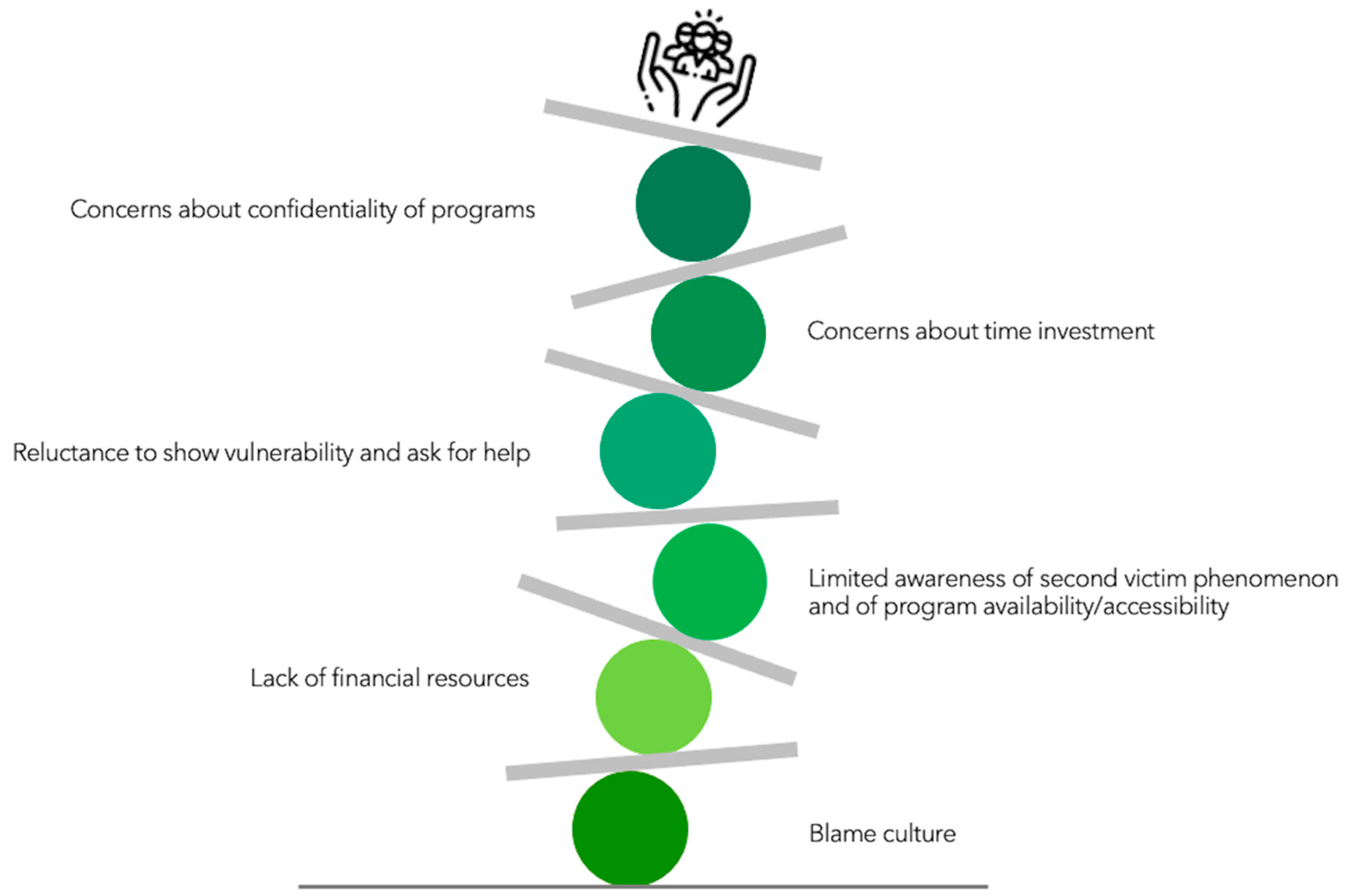
3.5. Challenges Encountered during Implementation of the Programs
4. Discussion
4.1. Recommendations for Clinical Practice
4.2. Limitations
4.3. Future Research Directions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Veazie, S.; Peterson, K.; Bourne, D. Evidence Brief: Implementation of High Reliability Organization Principles; Evidence Synthesis Program; Health Services Research and Development Service, Office of Research and Development, Department of Veterans Affairs: Washington, DC, USA, 2019; VA ESP Project #09-199. Available online: https://www.hsrd.research.va.gov/publications/esp/reports.cfm (accessed on 7 April 2021).
- Khatri, N.; Brown, G.D.; Hicks, L.L. From a blame culture to a just culture in health care. Health Care Manag. Rev. 2009, 34, 312–322. [Google Scholar] [CrossRef] [PubMed]
- Parker, J.; Davies, B. No Blame No Gain? From a No Blame Culture to a Responsibility Culture in Medicine. J. Appl. Philos. 2020, 37, 646–660. [Google Scholar] [CrossRef] [PubMed]
- Busch, I.M.; Moretti, F.; Purgato, M.; Barbui, C.; Wu, A.W.; Rimondini, M. Psychological and Psychosomatic Symptoms of Second Victims of Adverse Events: A Systematic Review and Meta-Analysis. J. Patient Saf. 2020, 16, e61–e74. [Google Scholar] [CrossRef]
- Burlison, J.D.; Quillivan, R.R.; Scott, S.D.; Johnson, S.; Hoffman, J.M. The Effects of the Second Victim Phenomenon on Work-Related Outcomes: Connecting Self-Reported Caregiver Distress to Turnover Intentions and Absenteeism. J. Patient Saf. 2021, 17, 195–199. [Google Scholar] [CrossRef]
- Baas, M.A.M.; Scheepstra, K.W.F.; Stramrood, C.A.I.; Evers, R.; Dijksman, L.M.; van Pampus, M.G. Work-related adverse events leaving their mark: A cross-sectional study among Dutch gynecologists. BMC Psychiatry 2018, 18, 73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stehman, C.R.; Testo, Z.; Gershaw, R.S.; Kellogg, A.R. Burnout, Drop Out, Suicide: Physician Loss in Emergency Medicine, Part I. West. J. Emerg. Med. 2019, 20, 485–494. [Google Scholar] [CrossRef] [Green Version]
- Wu, A.W. Medical error: The second victim. The doctor who makes the mistake needs help too. BMJ 2000, 320, 726–727. [Google Scholar] [CrossRef]
- Clarkson, M.D.; Haskell, H.; Hemmelgarn, C.; Skolnik, P.J. Abandon the term “second victim”. BMJ 2019, 364, l1233. [Google Scholar] [CrossRef]
- Busch, I.M.; Moretti, F.; Purgato, M.; Barbui, C.; Wu, A.W.; Rimondini, M. Dealing with Adverse Events: A Meta-analysis on Second Victims’ Coping Strategies. J Patient Saf. 2020, 16, e51–e60. [Google Scholar] [CrossRef]
- Seys, D.; Scott, S.; Wu, A.; Van Gerven, E.; Vleugels, A.; Euwema, M.; Panella, M.; Conway, J.; Sermeus, W.; Vanhaecht, K. Supporting involved health care professionals (second victims) following an adverse health event: A literature review. Int. J. Nurs. Stud. 2013, 50, 678–687. [Google Scholar] [CrossRef] [Green Version]
- Ozeke, O.; Aras, S.; Baser, K.; Sen, F.; Kirbas, O.; Cay, S.; Ozcan, F.; Topaloglu, S.; Aras, D.; Aydogdu, S. Defensive medicine due to different fears by patients and physicians in geriatric atrial fibrillation patients and second victim syndrome. Int. J. Cardiol. 2016, 212, 251–252. [Google Scholar] [CrossRef]
- World Health Organization. Global Patient Safety Action Plan 2021–2030. Towards Zero Patients Harm in Healthcare. First Draft August 2020. Available online: https://www.who.int/docs/default-source/patient-safety/1st-draft-global-patient-safety-action-plan-august-2020.pdf?sfvrsn=9b1552d2_4 (accessed on 23 March 2021).
- Hollnagel, E.; Wears, R.L.; Braithwaite, J. From Safety-I to Safety-II: A White Paper. Published Simultaneously by the University of Southern Denmark, University of Florida, USA, and Macquarie University, Australia: The Resilient Health Care Net. 2015. Available online: https://www.england.nhs.uk/signuptosafety/wp-content/uploads/sites/16/2015/10/safety-1-safety-2-whte-papr.pdf (accessed on 7 March 2021).
- Stone, M. Second victim support programs for healthcare organizations. Nurs. Manag. 2020, 51, 38–45. [Google Scholar] [CrossRef] [PubMed]
- Wade, L.; Fitzpatrick, E.; Williams, N.; Parker, R.; Hurley, K.F. Organizational Interventions to Support Second Victims in Acute Care Settings: A Scoping Study. J. Patient Saf. 2020. [Google Scholar] [CrossRef] [Green Version]
- Munn, Z.; Peters, M.D.J.; Stern, C.; Tufanaru, C.; McArthur, A.; Aromataris, E. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med. Res. Methodol. 2018, 18, 143. [Google Scholar] [CrossRef] [PubMed]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.T.; Deeks, J.J. Chapter 7: Selecting studies and collecting data. In Cochrane Handbook for Systematic Reviews of Interventions, Version 5.1.0; Higgins, J.P.T., Green, S., Eds.; The Cochrane Collaboration: London, UK, 2011; Available online: www.handbook.cochrane.org (accessed on 21 February 2021).
- The Joanna Briggs Institute. The Joanna Briggs Institute Critical Appraisal tools for use in JBI Systematic Reviews. Checklist for Text and Opinion Papers. Available online: http://joannabriggs.org/assets/docs/critical-appraisal-tools/JBI_Critical_Appraisal-Checklist_for_Prevalence_Studies2017.pdf (accessed on 14 December 2020).
- Mixed Method Appraisal Tool. Available online: http://mixedmethodsappraisaltoolpub-lic.pbworks.com/w/file/fetch/127916259/MMAT_2018_criteria-manual_2018-08-01_ENG.pdf (accessed on 14 December 2020).
- Connors, C.A.; Dukhanin, V.; Norvell, M.; Wu, A.W. RISE: Exploring Volunteer Retention and Sustainability of a Second Victim Support Program. J. Healthc. Manag. 2021, 66, 19–32. [Google Scholar]
- Dukhanin, V.; Edrees, H.H.; Connors, C.A.; Kang, E.; Norvell, M.; Wu, A.W. Case: A second victim support program in pediatrics: Successes and challenges to implementation. J. Pediatr. Nurs. 2018, 41, 54–59. [Google Scholar] [CrossRef] [PubMed]
- Edrees, H.; Connors, C.; Paine, L.; Norvell, M.; Taylor, H.; Wu, A.W. Implementing the RISE second victim support programme at the Johns Hopkins Hospital: A case study. BMJ Open 2016, 6, e011708. [Google Scholar] [CrossRef] [Green Version]
- El Hechi, M.W.; Bohnen, J.D.; Westfal, M.; Han, K.; Cauley, C.; Wright, C.; Schulz, J.; Mort, E.; Ferris, T.; Lillemoe, K.D.; et al. Design and Impact of a Novel Surgery-Specific Second Victim Peer Support Program. J. Am. Coll. Surg. 2020, 230, 926–933. [Google Scholar] [CrossRef]
- Hirschinger, L.E.; Scott, S.D.; Hahn-Cover, K. Clinician Support. Five Years of Lessons Learned. PHQH. 2015. Available online: https://www.psqh.com/analysis/clinician-support-five-years-of-lessons-learned/ (accessed on 27 September 2020).
- Krzan, K.D.; Merandi, J.; Morvay, S.; Mirtallo, J. Implementation of a “second victim” program in a pediatric hospital. Am. J. Health Syst. Pharm. 2015, 72, 563–567. [Google Scholar] [CrossRef] [PubMed]
- Lane, M.A.; Newman, B.M.; Taylor, M.Z.; O’Neill, M.; Ghetti, C.; Woltman, R.M.; Waterman, A.D. Supporting Clinicians after Adverse Events: Development of a Clinician Peer Support Program. J. Patient Saf. 2018, 14, e56–e60. [Google Scholar] [CrossRef] [PubMed]
- Merandi, J.; Liao, N.; Lewe, D.; Morvay, S.; Stewart, B.; Catt, C.; Scott, S.D. Deployment of a Second Victim Peer Support Program: A Replication Study. Pediatr. Qual. Saf. 2017, 2, e031. [Google Scholar] [CrossRef] [PubMed]
- Mira, J.J.; Carrillo, I.; Guilabert, M.; Lorenzo, S.; Pérez-Pérez, P.; Silvestre, C.; Ferrús, L. Spanish Second Victim Research Team. The Second Victim Phenomenon after a Clinical Error: The Design and Evaluation of a Website to Reduce Caregivers’ Emotional Responses after a Clinical Error. J. Med. Internet Res. 2017, 19, e203. [Google Scholar] [CrossRef] [PubMed]
- Morales, C.L.; Brown, M.M. Creating a Care for the Caregiver Program in a Ten-Hospital Health System. Crit. Care Nurs. Clin. N. Am. 2019, 31, 461–473. [Google Scholar] [CrossRef]
- Pratt, S.; Kenney, L.; Scott, S.D.; Wu, A.W. How to develop a second victim support program: A toolkit for health care organizations. Jt. Comm. J. Qual. Patient Saf. 2012, 38, 235–240. [Google Scholar] [CrossRef]
- Roesler, R.; Ward, D.; Short, M. Supporting staff recovery and reintegration after a critical incident resulting in infant death. Adv. Neonatal Care 2009, 9, 163–171. [Google Scholar] [CrossRef]
- Scott, S.D.; Hirschinger, L.E.; Cox, K.R.; McCoig, M.; Hahn-Cover, K.; Epperly, K.M.; Phillips, E.C.; Hall, L.W. Caring for our own: Deploying a systemwide second victim rapid response team. Jt. Comm. J. Qual. Patient Saf. 2010, 36, 233–240. [Google Scholar] [CrossRef]
- Trent, M.; Waldo, K.; Wehbe-Janek, H.; Williams, D.; Hegefeld, W.; Havens, L. Impact of health care adversity on providers: Lessons learned from a staff support program. J. Healthc. Risk Manag. 2016, 36, 27–34. [Google Scholar] [CrossRef]
- Van Pelt, F. Peer support: Healthcare professionals supporting each other after adverse medical events. Qual. Saf. Health Care 2008, 17, 249–252. [Google Scholar] [CrossRef]
- Wijaya, M.A.; Mohamad, A.R.; Hafizzurachman, M. Second victim support program and patient safety culture: A quasi experimental study in Bali International Medical Centre (BIMC) Hospital. Bali Med. J. 2018, 7, 220–226. [Google Scholar] [CrossRef]
- Busch, I.M.; Scott, S.D.; Connors, C.; Story, A.R.; Acharya, B.; Wu, A.W. The Role of Institution-Based Peer Support for Health Care Workers Emotionally Affected by Workplace Violence. Jt. Comm. J. Qual. Patient Saf. 2021, 47, 146–156. [Google Scholar]
- Mitchell, J. Critical Incident Stress Management (CISM): Group Crisis Intervention, 4th ed.; International Critical Incident Stress Foundation: Ellicot City, MD, USA, 2006. [Google Scholar]
- Mitchell, J. Advanced Group Crisis Intervention: Strategies and Tactics for Complex Situations, 3rd ed.; International Critical Incident Stress Foundation: Ellicot City, MD, USA, 2006. [Google Scholar]
- Bisson, J.I.; Brayne, M.; Ochberg, F.M.; Everly, G.S., Jr. Early psychosocial intervention following traumatic events. Am. J. Psychiatry 2007, 164, 1016–1019. [Google Scholar] [CrossRef]
- Everly, G.S., Jr.; Flynn, B. Principles and practical procedures for acute psychological first aid training for personnel without mental health experience. Int. J. Emerg. Ment. Health 2006, 8, 93–100. [Google Scholar] [PubMed]
- Leitch, L.; Sutton, L. An Introduction to the Social Resilience Model. 2017. Available online: https://www.thresholdglobalworks.com/about/social-resilience/ (accessed on 18 March 2021).
- Halifax, J. GRACE for Nurses: Cultivating Compassion in Nurse/Patient Interactions. J. Nurs. Educ. Pract. 2014, 4, 121–128. [Google Scholar]
- Watson, J. Nursing—The Philosophy and Science of Caring, 2nd ed.; F.A. Davis Company: Boulder, CO, USA, 2008. [Google Scholar]
- Agency for Healthcare Research and Quality. Communication and Optimal Resolution (CANDOR) Toolkit. 2017. Available online: http://www.ahrq.gov/professionals/quality-patient-safety/patient-safety-resources/resources/candor/introduction.html (accessed on 7 March 2021).
- Devencenzi, T.; O’Keefe, J. To err is human: Supporting the patient care provide in the aftermath of an unanticipated adverse clinical outcome. Int. J. Emerg. Ment. Health 2006, 8, 131–135. [Google Scholar]
- Scott, S.D.; Hirschinger, L.E.; Cox, K.R.; McCoig, M.; Brandt, J.; Hall, L. The natural history of recovery for the health care provider “second victim” after adverse patient events. Qual. Saf. Health Care 2009, 18, 325–330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scott, S.D. The Second Victim Phenomenon: A Harsh Reality of Health Care profEssions. 2011. Available online: https://psnet.ahrq.gov/perspective/second-victim-phenomenon-harsh-reality-health-care-professions#tableback (accessed on 12 March 2021).
- Radhakrishna, S. Culture of blame in the National Health Service; consequences and solutions. Br. J. Anaesth. 2015, 115, 653–655. [Google Scholar] [CrossRef] [Green Version]
- Reis, C.T.; Paiva, S.G.; Sousa, P. The patient safety culture: A systematic review by characteristics of hospital survey on patient safety culture dimensions. Int. J. Qual. Health Care 2018, 30, 660–677. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, A.W.; Sexton, J.; Pham, J.C. Health care providers: The second victim of medical error. In Patient Safety in Emergency Medicine; Croskerry, P., Cosby, S.K., Schenkel, S.M., Wears, R., Eds.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2008. [Google Scholar]
- The Joint Commission, Division of Healthcare Improvement. Supporting second victims. Quick. Saf. 2018, 39, 1–3. [Google Scholar]
- Braithwaite, J.; Wears, R.L.; Hollnagel, E. Resilient health care: Turning patient safety on its head. Int. J. Qual. Health Care 2015, 27, 418–420. [Google Scholar] [CrossRef] [PubMed]
- Brymer, M.; Jacobs, A.; Layne, C.; Pynoos, R.; Ruzek, J.; Steinberg, A.; Vernberg, E.; Watson, P. National Child Traumatic Stress Network/National Center for PTSD Psychological First Aid: Field Operations Guide, 2nd ed. 2006. Available online: https://www.nctsn.org/resources/psychological-first-aid-pfa-field-operations-guide-2nd-edition (accessed on 7 March 2021).
- Everly, G.S., Jr.; Lating, J.M.; Sherman, M.F.; Goncher, I. The Potential Efficacy of Psychological First Aid on Self-Reported Anxiety and Mood: A Pilot Study. J. Nerv. Ment. Dis. 2016, 204, 233–235. [Google Scholar] [CrossRef] [PubMed]
- Carthey, J.; Clarke, J. The ‘How to Guide’ for Implementing Human Factors in Healthcare. Available online: https://chfg.org/how-to-guide-to-human-factors-volume-1/ (accessed on 7 March 2021).
- Wu, A.W.; Busch, I.M. Patient safety: A new basic science for professional education. GMS J. Med. Educ. 2019, 36, Doc21. [Google Scholar] [PubMed]
- Wu, A.W. Health worker well-being and resilience: A Red Ball issue for the COVID-19 response. J. Patient Saf. Risk Manag. 2020, 25, 164–165. [Google Scholar] [CrossRef]
- Wu, A.W.; Connors, C.; Everly, G.S., Jr. COVID-19: Peer Support and Crisis Communication Strategies to Promote Institutional Resilience. Ann. Intern Med. 2020, 172, 822–823. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Busch, I.M.; Saxena, A.; Wu, A.W. Putting the Patient in Patient Safety Investigations: Barriers and Strategies for Involvement. J. Patient Saf. 2020. [Google Scholar] [CrossRef] [PubMed]
- Iedema, R.; Allen, S. Anatomy of an incident disclosure: The importance of dialogue. Jt. Comm. J. Qual. Patient Saf. 2012, 38, 435–442. [Google Scholar] [CrossRef]
- Denver Health Foundation. Stories. Available online: https://www.denverhealthfoundation.org/rise-program-supports-staff-during-pandemic/ (accessed on 7 March 2021).
- Moran, D.; Wu, A.W.; Connors, C.; Chappidi, M.R.; Sreedhara, S.K.; Selter, J.H.; Padula, W.V. Cost-Benefit Analysis of a Support Program for Nursing Staff. J. Patient Saf. 2020, 16, e250–e254. [Google Scholar] [CrossRef]
- Busch, I.M.; Moretti, F.; Mazzi, M.; Wu, A.W.; Rimondini, M. What We Have Learned from Two Decades of Epidemics and Pandemics: A Systematic Review and Meta-Analysis of the Psychological Burden of Frontline Healthcare Workers. Psychother. Psychosom. 2021, 90, 178–190. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| MMAT TOOL | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Qualitative Studies | |||||||||||
| 1. Is the qualitative approach appropriate to answer the research question? | 2. Are the qualitative data collection methods adequate to address the research question? | 3. Are the findings adequately derived from the data? | 4. Is the interpretation of results sufficiently substantiated by data? | 5. Is there coherence between qualitative data sources, collection analysis, and interpretation? | |||||||
| Trent et al., 2016 [36] (SWADDLE) | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||
| Quantitative non-randomized studies | |||||||||||
| 1. Are the participants representative of the target population? | 2. Are measurements appropriate regarding both the outcome and intervention (or exposure)? | 3. Are there complete outcome data? | 4. Are the confounders accounted for in the design and analysis? | 5. During the study period, is the intervention administered (or exposure occurred) as intended? | |||||||
| Wijaya et al., 2018 [38] (no specific name given) | ✓ | ✓ | ✗ | ✓ | ✓ | ||||||
| Quantitative descriptive studies | |||||||||||
| 1. Is the sampling strategy relevant to address the research question? | 2. Is the sample representative of the target population? | 3. Are the measurements appropriate? | 4. Is the risk of nonresponse bias low? (for case series and case report: are there complete data on the cases?) | 5. Is the statistical analysis appropriate to answer the research question? | |||||||
| Hirschinger et al., 2015 [27] (forYOU Team) | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||
| Krzan et al., 2015 [28] (YouMatter Program) | ✓ | ✓ | ✓ | ✓ | ✗ | ||||||
| Lane et al., 2018 [29] (WUSM Peer Support Program) | ✓ | ✓ | ✓ | ✗ | ✗ | ||||||
| Merandi et al., 2017 [30] (YouMatter Program) | ✓ | ✓ | ✓ | ✓ | ✗ | ||||||
| Mira et al., 2017 [31] (MISE) | ✓ | ✓ | ✓ | ✓ | ✗ | ||||||
| Mixed methods studies | |||||||||||
| 1. Is there an adequate rationale for using a mixed methods design to address the research question? | 2. Are the different components of the study effectively integrated to answer the research questions? | 3. Are the outputs of the integration of qualitative and quantitative components adequately interpreted? | 4. Are divergences and inconsistencies between quantitative and qualitative results adequately addressed? | 5. Do the different components of the study adhere to the quality criteria of each tradition of the methods involved? | |||||||
| Connors et al., 2021 [23] (RISE) | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||
| Dukhanin et al., 2018 [24] (RISE) | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||
| Edrees et al., 2016 [25] (RISE) | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||
| El Hechi et al., 2019 [26] (Surgery-Specific Second Victim Support Program) | ✓ | ✓ | ✓ | ✓ | ✗ | ||||||
| Scott et al., 2010 [35] (forYOU Team) | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||
| JBI CRITICAL APPRAISAL CHECKLIST FOR TEXT AND OPINION PAPERS | |||||||||||
| 1. Source of opinion identified | 2. Source of opinion having a standing in the field | 3. Interests of the relevant population as central focus of the opinion | 4. Stated position as result of analytical process and logic in the expressed opinion | 5. Reference to the extant literature | 6. Incongruence with the literature/sources logically defended | ||||||
| Morales & Brown, 2019 [32] (Care for the Caregiver Program) | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||||
| Pratt et al., 2012 [33] (Medically Induced Trauma Support Services Tool) | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||||
| Roesler et al., 2009 [34] (Healing Beyond Today) | ✓ | ✓ | ✓ | ✓ | ✗ | ✗ | |||||
| Van Pelt, 2008 [37] (Peer Support Team) | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Busch, I.M.; Moretti, F.; Campagna, I.; Benoni, R.; Tardivo, S.; Wu, A.W.; Rimondini, M. Promoting the Psychological Well-Being of Healthcare Providers Facing the Burden of Adverse Events: A Systematic Review of Second Victim Support Resources. Int. J. Environ. Res. Public Health 2021, 18, 5080. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18105080
Busch IM, Moretti F, Campagna I, Benoni R, Tardivo S, Wu AW, Rimondini M. Promoting the Psychological Well-Being of Healthcare Providers Facing the Burden of Adverse Events: A Systematic Review of Second Victim Support Resources. International Journal of Environmental Research and Public Health. 2021; 18(10):5080. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18105080
Chicago/Turabian StyleBusch, Isolde Martina, Francesca Moretti, Irene Campagna, Roberto Benoni, Stefano Tardivo, Albert W. Wu, and Michela Rimondini. 2021. "Promoting the Psychological Well-Being of Healthcare Providers Facing the Burden of Adverse Events: A Systematic Review of Second Victim Support Resources" International Journal of Environmental Research and Public Health 18, no. 10: 5080. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18105080