
Effects of Mini-Basketball Training Program on Social Communication Impairment and Executive Control Network in Preschool Children with Autism Spectrum Disorder

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Study Design
2.3. Mini-Basketball Training Program
2.4. Measurement of Social Communication
2.5. rs-fMRI Data Collection and Processing
2.6. Procedure
2.7. Statistical Analysis
3. Results
3.1. Participant Characteristics
3.2. Social Communication Performance
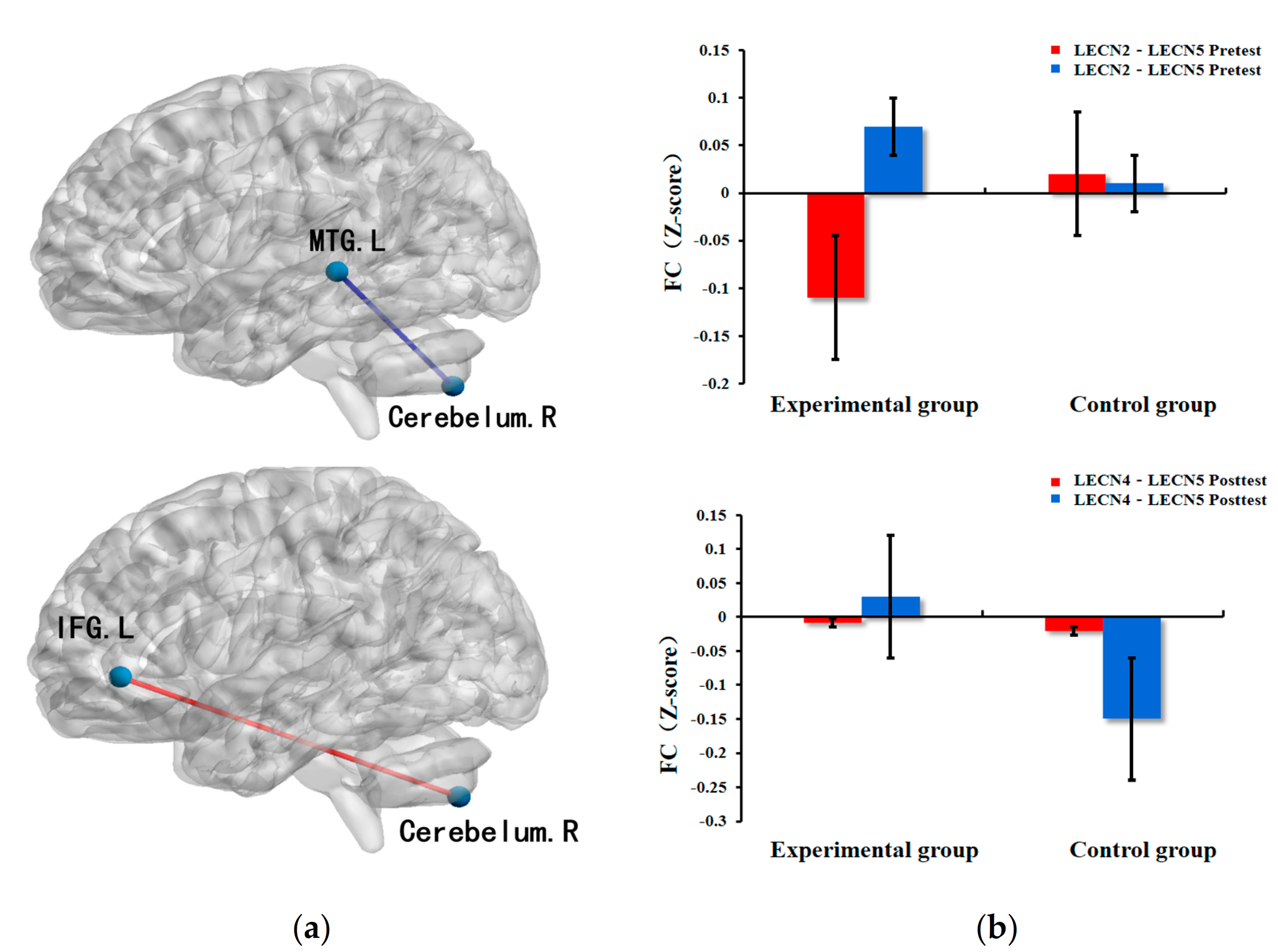
3.3. Executive Control Network
3.4. Correlation between Functional Connectivity of ECN and Behavioral Performance
4. Discussion
4.1. Behavioral Performance
4.2. Executive Control Network
4.3. Neural Mechanism of MBTP on Social Communication Impairment in Preschool Children with ASD
4.4. Limition
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Blenner, S.; Reddy, A.; Augustyn, M. Diagnosis and management of autism in childhood. BMJ 2011, 343, d6238. [Google Scholar] [CrossRef] [Green Version]
- Maenner, M.J.; Shaw, K.A.; Baio, J.; Washington, A.; Patrick, M.; DiRienzo, M.; Christensen, D.L.; Wiggins, L.D.; Pettygrove, S.; Andrews, J.G.; et al. Prevalence of Autism Spectrum Disorder among Children Aged 8 Years—Autism and Developmental Disabilities Monitoring Network, 11 Sites, United States, 2016. MMWR. Surveill. Summ. 2020, 69, 1–12. [Google Scholar] [CrossRef]
- Landa, R.J.; Holman, K.C.; Garrett-Mayer, E. Social and Communication Development in Toddlers with Early and Later Diagnosis of Autism Spectrum Disorders. Arch. Gen. Psychiatry 2007, 64, 853–864. [Google Scholar] [CrossRef]
- Padden, C.; James, J.E. Stress among Parents of Children with and without Autism Spectrum Disorder: A Comparison Involving Physiological Indicators and Parent Self-Reports. J. Dev. Phys. Disabil. 2017, 29, 567–586. [Google Scholar] [CrossRef] [Green Version]
- Baxter, A.J.; Brugha, T.S.; Erskine, H.E.; Scheurer, R.W.; Vos, T.; Scott, J.G. The epidemiology and global burden of autism spectrum disorders. Psychol. Med. 2015, 45, 601–613. [Google Scholar] [CrossRef]
- Ming, X.; Hashim, A.; Fleishman, S.; West, T.; Kang, N.; Chen, X.; Zimmerman-Bier, B. Access to specialty care in autism spectrum disorders—A pilot study of referral source. BMC Health Serv. Res. 2011, 11, 99. [Google Scholar] [CrossRef] [Green Version]
- Sotoodeh, M.S.; Arabameri, E.; Panahibakhsh, M.; Kheiroddin, F.; Mirdoozandeh, H.; Ghanizadeh, A. Effectiveness of yoga training program on the severity of autism. Complement. Ther. Clin. Pract. 2017, 28, 47–53. [Google Scholar] [CrossRef]
- Pan, C.-Y. Effects of water exercise swimming program on aquatic skills and social behaviors in children with autism spectrum disorders. Autism 2010, 14, 9–28. [Google Scholar] [CrossRef]
- Cai, K.; Yu, Q.; Herold, F.; Liu, Z.; Wang, J.; Zhu, L.; Xiong, X.; Chen, A.; Müller, P.; Kramer, A.F.; et al. Mini-Basketball Training Program Improves Social Communication and White Matter Integrity in Children with Autism. Brain Sci. 2020, 10, 803. [Google Scholar] [CrossRef]
- Bahrami, F.; Movahedi, A.; Marandi, S.M.; Sorensen, C. The Effect of Karate Techniques Training on Communication Deficit of Children with Autism Spectrum Disorders. J. Autism Dev. Disord. 2016, 46, 978–986. [Google Scholar] [CrossRef]
- Bass, M.M.; Duchowny, C.A.; Llabre, M.M. The Effect of Therapeutic Horseback Riding on Social Functioning in Children with Autism. J. Autism Dev. Disord. 2009, 39, 1261–1267. [Google Scholar] [CrossRef]
- Ketcheson, L.; Hauck, J.L.; Ulrich, D. The levels of physical activity and motor skills in young children with and without autism spectrum disorder, aged 2–5 years. Autism 2018, 22, 414–423. [Google Scholar] [CrossRef]
- Reinders, N.J.; Branco, A.; Wright, K.; Fletcher, P.C.; Bryden, P.J. Scoping Review: Physical Activity and Social Functioning in Young People with Autism Spectrum Disorder. Front. Psychol. 2019, 10, 120. [Google Scholar] [CrossRef] [Green Version]
- Cai, K.-L.; Wang, J.-G.; Liu, Z.-M.; Zhu, L.-N.; Xiong, X.; Klich, S.; Maszczyk, A.; Chen, A.-G. Mini-Basketball Training Program Improves Physical Fitness and Social Communication in Preschool Children with Autism Spectrum Disorders. J. Hum. Kinet. 2020, 73, 267–278. [Google Scholar] [CrossRef]
- Wang, J.-G.; Cai, K.-L.; Liu, Z.-M.; Herold, F.; Zou, L.; Zhu, L.-N.; Xiong, X.; Chen, A.-G. Effects of Mini-Basketball Training Program on Executive Functions and Core Symptoms among Preschool Children with Autism Spectrum Disorders. Brain Sci. 2020, 10, 263. [Google Scholar] [CrossRef]
- Zhu, Y.; Xu, C.; Wan, Q.; Guo, L.Y.; Sean, X.C. Effects of Adapted Physical Exercise Intervention on Visual Working Memory in Children with Autism Spectrum Disorder. China Sport Sci. Technol. 2017, 53, 55–62. [Google Scholar] [CrossRef]
- Ma, Z.H.; Cao, Q.J.; Yan, C.G.; Mei, T.; Lu, B.; Liu, J.R.; Yang, L.; Wang, H.; Tang, X.Z.; Ji, Y.Z.; et al. Functional connectivity characteristics of executive control network in patients with high-functioning autism aged 6–18 years. Chinese Ment. Health J. 2019, 33, 401–405. [Google Scholar] [CrossRef]
- Elton, A.; Di Martino, A.; Hazlett, H.C.; Gao, W. Neural Connectivity Evidence for a Categorical-Dimensional Hybrid Model of Autism Spectrum Disorder. Biol. Psychiatry 2016, 80, 120–128. [Google Scholar] [CrossRef] [Green Version]
- Chen, A.G.; Zhu, L.N.; Xiong, X.; Li, Y. Effects of Aerobic Exercise on Executive Control and its Brain Network in Deaf Children. Sports Sci. 2016, 37, 94–101. [Google Scholar] [CrossRef]
- Liu, J.; Chen, L.; Tu, Y.; Chen, X.; Hu, K.; Tu, Y.; Lin, M.; Xie, G.; Chen, S.; Huang, J.; et al. Different exercise modalities relieve pain syndrome in patients with knee osteoarthritis and modulate the dorsolateral prefrontal cortex: A multiple mode MRI study. Brain, Behav. Immun. 2019, 82, 253–263. [Google Scholar] [CrossRef]
- Chen, A.G.; Zhu, L.N.; Xiong, X.; Li, Y. Acute aerobic exercise alters executive control network in preadolescent children. Rev. Psicol. Deporte 2017, 26, 132–137. [Google Scholar]
- Hodges, H.; Fealko, C.; Soares, N. Autism spectrum disorder: Definition, epidemiology, causes, and clinical evaluation. Transl. Pediatr. 2020, 9, S55–S65. [Google Scholar] [CrossRef] [PubMed]
- Veatch, O.J.; Sutcliffe, J.S.; Warren, Z.E.; Keenan, B.T.; Potter, M.H.; Malow, B.A. Shorter sleep duration is associated with social impairment and comorbidities in ASD. Autism Res. 2017, 10, 1221–1238. [Google Scholar] [CrossRef] [PubMed]
- Marshall, J.V.; Ware, R.S.; Ziviani, J.M.; Hill, R.J.; Dodrill, P.M.M. Efficacy of interventions to improve feeding difficulties in children with autism spectrum disorders: A systematic review and meta-analysis. Child Care Heath Dev. 2015, 41, 278–302. [Google Scholar] [CrossRef]
- Tyler, K.; Macdonald, M.; Menear, K. Physical Activity and Physical Fitness of School-Aged Children and Youth with Autism Spectrum Disorders. Autism Res. Treat. 2014, 2014, 312163. [Google Scholar] [CrossRef]
- Schopler, E.; Reichler, R.J.; DeVellis, R.F.; Daly, K. Toward objective classification of childhood autism: Childhood Autism Rating Scale (CARS). J. Autism Dev. Disord. 1980, 10, 91–103. [Google Scholar] [CrossRef]
- Owens, J.A.; Spirito, A.; McGuinn, M. The Children’s Sleep Habits Questionnaire (CSHQ): Psychometric properties of a survey instrument for school-aged children. Sleep 2000, 23, 1043–1051. [Google Scholar] [CrossRef]
- Wardle, J.; Guthrie, C.A.; Sanderson, S.; Rapoport, L. Development of the Children’s Eating Behaviour Questionnaire. J. Child Psychol. Psychiatry 2001, 42, 963–970. [Google Scholar] [CrossRef] [Green Version]
- Lambert, J.M.; Copeland, B.A.; Karp, E.L.; Finley, C.I.; Houchins-Juarez, N.J.; Ledford, J.R. Chaining Functional Basketball Sequences (with Embedded Conditional Discriminations) in an Adolescent with Autism. Behav. Anal. Pr. 2016, 9, 199–210. [Google Scholar] [CrossRef] [Green Version]
- Fotrousi, F.; Bagherly, J.; Ghasemi, A. The Compensatory Impact of Mini-Basketball Skills on the Progress of Fundamental Movements in Children. Procedia-Soc. Behav. Sci. 2012, 46, 5206–5210. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Z.Y.; Deng, S.H. Case Study on Sports Games Intervention of Autistic Children. China Sport Sci. Technol. 2010, 30, 386–390. [Google Scholar] [CrossRef]
- Ferreira, J.P.; Ghiarone, T.; Júnior, C.R.C.; Furtado, G.E.; Carvalho, H.M.; Machado-Rodrigues, A.M.; Toscano, C.V.A. Effects of Physical Exercise on the Stereotyped Behavior of Children with Autism Spectrum Disorders. Medicina 2019, 55, 685. [Google Scholar] [CrossRef] [Green Version]
- Constantino, J.; Gruber, C.P. The Social Responsiveness Scale (SRS) Manual; Western Psychological Services: Los Angeles, CA, USA, 2005. [Google Scholar]
- Pan, C.-Y. The efficacy of an aquatic program on physical fitness and aquatic skills in children with and without autism spectrum disorders. Res. Autism Spectr. Disord. 2011, 5, 657–665. [Google Scholar] [CrossRef]
- Rivera, P.; Renziehausen, J.; Garcia, J.M. Effects of an 8-Week Judo Program on Behaviors in Children with Autism Spectrum Disorder: A Mixed-Methods Approach. Child Psychiatry Hum. Dev. 2020, 51, 734–741. [Google Scholar] [CrossRef]
- Adolphs, R. The neurobiology of social cognition. Curr. Opin. Neurobiol. 2001, 11, 231–239. [Google Scholar] [CrossRef]
- Ferraioli, S.J.; Harris, S.L. Treatments to Increase Social Awareness and Social Skills; Springer: Boston, MA, USA, 2010; pp. 171–196. [Google Scholar]
- Taub, D.E.; Greer, K.R. Physical activity as a normalizing experience for school-age children: With physical disa-bilities: Implications for legitimation of social identity and enhancement for social ties. J. Sport Soc. Issues 2000. [Google Scholar] [CrossRef]
- Prehn, K.; Lesemann, A.; Krey, G.; Witte, A.V.; Köbe, T.; Grittner, U.; Flöel, A. Using resting-state fMRI to assess the effect of aerobic exercise on functional connectivity of the DLPFC in older overweight adults. Brain Cogn. 2019, 131, 34–44. [Google Scholar] [CrossRef]
- Geschwind, D.H.; Levitt, P. Autism spectrum disorders: Developmental disconnection syndromes. Curr. Opin. Neurobiol. 2007, 17, 103–111. [Google Scholar] [CrossRef]
- Courchesne, E.; Pierce, K. Why the frontal cortex in autism might be talking only to itself: Local over-connectivity but long-distance disconnection. Curr. Opin. Neurobiol. 2005, 15, 225–230. [Google Scholar] [CrossRef]
- Fatemi, S.H.; Aldinger, K.A.; Ashwood, P.; Bauman, M.L.; Blaha, C.D.; Blatt, G.J.; Chauhan, A.; Chauhan, V.; Dager, S.R.; Dickson, P.E.; et al. Consensus Paper: Pathological Role of the Cerebellum in Autism. Cerebellum 2012, 11, 777–807. [Google Scholar] [CrossRef] [Green Version]
- Manto, M.; Bower, J.M.; Conforto, A.B.; Delgado-García, J.M.; Da Guarda, S.N.F.; Gerwig, M.; Habas, C.; Hagura, N.; Ivry, R.B.; Mariën, P.; et al. Consensus Paper: Roles of the Cerebellum in Motor Control—The Diversity of Ideas on Cerebellar Involvement in Movement. Cerebellum 2012, 11, 457–487. [Google Scholar] [CrossRef] [PubMed]
- Diamond, A. Close Interrelation of Motor Development and Cognitive Development and of the Cerebellum and Prefrontal Cortex. Child Dev. 2000, 71, 44–56. [Google Scholar] [CrossRef]
- Schlosser, R.; Hutchinson, M.; Joseffer, S.; Rusinek, H.; Saarimaki, A.; Stevenson, J.; Dewey, S.L.; Brodie, J.D. Functional magnetic resonance imaging of human brain activity in a verbal fluency task. J. Neurol. Neurosurg. Psychiatry 1998, 64, 492–498. [Google Scholar] [CrossRef] [Green Version]
- Raichle, M.E.; Fiez, J.A.; Videen, T.O.; MacLeod, A.-M.K.; Pardo, J.V.; Fox, P.T.; Petersen, S.E. Practice-related Changes in Human Brain Functional Anatomy during Nonmotor Learning. Cereb. Cortex 1994, 4, 8–26. [Google Scholar] [CrossRef]
- Hetzler, B.E.; Griffin, J.L. Infantile autism and the temporal lobe of the brain. J. Autism Dev. Disord. 1981, 11, 317–330. [Google Scholar] [CrossRef]
- Xu, J.; Wang, C.; Xu, Z.; Li, T.; Chen, F.; Chen, K.; Gao, J.; Wang, J.; Hu, Q. Specific Functional Connectivity Patterns of Middle Temporal Gyrus Subregions in Children and Adults with Autism Spectrum Disorder. Autism Res. 2019, 13, 410–422. [Google Scholar] [CrossRef]
- Eli, R.; Ezhu, X.; Eyin, S.; Eniu, Y.; Ezheng, Z.; Ehuang, X.; Ewang, B.; Eli, J. Multimodal intervention in older adults improves resting-state functional connectivity between the medial prefrontal cortex and medial temporal lobe. Front. Aging Neurosci. 2014, 6, 39. [Google Scholar] [CrossRef]
- Blakemore, S.-J. The social brain in adolescence. Nat. Rev. Neurosci. 2008, 9, 267–277. [Google Scholar] [CrossRef]
- Adolphs, R. Cognitive neuroscience of human social behaviour. Nat. Rev. Neurosci. 2003, 4, 165–178. [Google Scholar] [CrossRef]
- Brothers, L.; Ring, B.; Kling, A. Response of neurons in the macaque amygdala to complex social stimuli. Behav. Brain Res. 1990, 41, 199–213. [Google Scholar] [CrossRef]
- Pelphrey, K.A.; Morris, J.P.; McCarthy, G. Neural basis of eye gaze processing deficits in autism. Brain 2005, 128, 1038–1048. [Google Scholar] [CrossRef] [PubMed]
- Williams, J.H.; Waiter, G.D.; Gilchrist, A.; Perrett, D.I.; Murray, A.D.; Whiten, A. Neural mechanisms of imitation and ‘mirror neuron’ functioning in autistic spectrum disorder. Neuropsychologia 2006, 44, 610–621. [Google Scholar] [CrossRef] [PubMed]
- Pierce, K.; Haist, F.; Sedaghat, F.; Courchesne, E. The brain response to personally familiar faces in autism: Findings of fusiform activity and beyond. Brain 2004, 127, 2703–2716. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, A.T.; Lee, S.S.; Sigman, M.; Dapretto, M. Reading Affect in the Face and Voice. Arch. Gen. Psychiatry 2007, 64, 698–708. [Google Scholar] [CrossRef]
- Whitney, C.; Jefferies, E.; Kircher, T. Heterogeneity of the Left Temporal Lobe in Semantic Representation and Control: Priming Multiple versus Single Meanings of Ambiguous Words. Cereb. Cortex 2010, 21, 831–844. [Google Scholar] [CrossRef] [Green Version]
- Levisohn, L.; Cronin-Golomb, A.; Schmahmann, J.D. Neuropsychological consequences of cerebellar tumour resection in children. Brain 2000, 123, 1041–1050. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| ROI | Brain Hemispheres | Primary Regions | Brodmann’ Area |
|---|---|---|---|
| RECN1 | Right | orbitofrontal gyrus/dorsolateral prefrontal cortex | 8/9 |
| RECN2 | Right | frontal pole/inferior frontal gyrus | 10/46/47 |
| RECN3 | Right | inferior parietal lobule | 7/39/40 |
| RECN4 | Right | middle temporal gyrus | 20/37 |
| RECN5 | Left | cerebellum | – |
| RECN6 | Right | caudate nucleus | – |
| LECN1 | Left | orbitofrontal gyrus/dorsolateral prefrontal cortex | 8/9/46 |
| LECN2 | Left | frontal pole/inferior frontal gyrus | 10/45/47 |
| LECN3 | Left | inferior parietal lobule | 7/39/40 |
| LECN4 | Left | middle temporal gyrus | 20/37 |
| LECN5 | Right | cerebellum | – |
| LECN6 | Left | thalamus | – |
| Control Group | Experiment Group | |
|---|---|---|
| N | 15 | 15 |
| Gender(male/female) | 12/3 | 13/2 |
| Age | 5.03 ± 0.55 | 4.67 ± 0.70 |
| BMI | 15.75 ± 0.67 | 15.88 ± 1.80 |
| CARS a | 38.13 ± 4.47 | 39.80 ± 5.24 |
| CSHQ b | 56.47 ± 5.04 | 58.60 ± 12.29 |
| CEBQ c | 55.20 ± 8.25 | 54.40 ± 20.05 |
| 20-m shuttle run (s) | 13.31 ± 4.16 | 11.83 ± 2.23 |
| Standing long jump (cm) | 50.23 ± 28.75 | 37.00 ± 21.86 |
| Sit-and-reach (cm) | 17.55 ± 6.09 | 19.61 ± 2.43 |
| Balance beam (s) | 21.92 ± 36.00 | 19.90 ± 11.10 |
| Experiment Group (n = 15) | Control Group (n = 15) | |||
|---|---|---|---|---|
| Baseline | Post-Test | Baseline | Post-Test | |
| SRS-2 T-score | 89.70 ± 25.89 | 81.50 ± 4.55 | 85.30 ± 20.04 | 97.30 ± 21.35 |
| Social cognition | 19.50 ± 5.59 | 16.50 ± 6.07 | 17.30 ± 3.56 | 19.30 ± 3.89 |
| Social communication | 31.70 ± 1.86 | 28.40 ± 9.66 | 30.90 ± 8.06 | 35.70 ± 8.09 |
| Social motivation | 14.40 ± 4.72 | 12.30 ± 3.84 | 14.40 ± 4.39 | 14.50 ± 4.19 |
| Autistic mannerisms | 12.30 ± 5.04 | 13.20 ± 5.62 | 12.30 ± 5.36 | 16.40 ± 6.15 |
| Social awareness | 11.90 ± 2.80 | 11.20 ± 3.61 | 10.50 ± 2.45 | 11.40 ± 2.59 |
| RECN1 | RECN2 | RECN3 | RECN4 | RECN5 | RECN6 | LECN1 | LECN2 | LECN3 | LECN4 | LECN5 | LECN6 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| RECN1 | ||||||||||||
| RECN2 | 0.67 | |||||||||||
| RECN3 | 0.51 | 0.19 | ||||||||||
| RECN4 | 0.73 | 0.96 | 0.48 | |||||||||
| RECN5 | 0.77 | 0.71 | 0.80 | 0.37 | ||||||||
| RECN6 | 0.76 | 0.22 | 1.00 | 0.61 | 0.90 | |||||||
| LECN1 | 0.45 | 0.90 | 0.63 | 0.24 | 0.61 | 0.87 | ||||||
| LECN2 | 0.78 | 0.34 | 0.75 | 0.76 | 0.40 | 0.73 | 0.41 | |||||
| LECN3 | 0.38 | 0.77 | 0.57 | 0.65 | 0.46 | 0.45 | 0.41 | 0.87 | ||||
| LECN4 | 0.48 | 0.91 | 0.08 | 0.81 | 0.67 | 0.66 | 0.24 | 0.25 | 0.20 | |||
| LECN5 | 0.17 | 0.06 | 0.30 | 0.16 | 0.78 | 0.76 | 0.50 | 0.03 * | 0.05 | 0.01 * | ||
| LECN6 | 0.05 | 0.79 | 0.73 | 0.61 | 0.32 | 0.81 | 0.73 | 0.43 | 0.31 | 0.98 | 0.50 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, S.; Liu, Z.; Xiong, X.; Cai, K.; Zhu, L.; Dong, X.; Wang, J.; Zhu, H.; Shi, Y.; Chen, A. Effects of Mini-Basketball Training Program on Social Communication Impairment and Executive Control Network in Preschool Children with Autism Spectrum Disorder. Int. J. Environ. Res. Public Health 2021, 18, 5132. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18105132
Yang S, Liu Z, Xiong X, Cai K, Zhu L, Dong X, Wang J, Zhu H, Shi Y, Chen A. Effects of Mini-Basketball Training Program on Social Communication Impairment and Executive Control Network in Preschool Children with Autism Spectrum Disorder. International Journal of Environmental Research and Public Health. 2021; 18(10):5132. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18105132
Chicago/Turabian StyleYang, Sixin, Zhimei Liu, Xuan Xiong, Kelong Cai, Lina Zhu, Xiaoxiao Dong, Jingui Wang, Hao Zhu, Yifan Shi, and Aiguo Chen. 2021. "Effects of Mini-Basketball Training Program on Social Communication Impairment and Executive Control Network in Preschool Children with Autism Spectrum Disorder" International Journal of Environmental Research and Public Health 18, no. 10: 5132. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18105132