
Food Environment in and around Primary School Children’s Schools and Neighborhoods in Two Urban Settings in Kenya

 , , and
, , and
Abstract
:1. Introduction
- (1)
- types of food places located around and within school settings and school children’s neighborhoods
- (2)
- healthy/unhealthy food availability in food places located around and within school settings and within school children’s neighborhoods
- (3)
- associations between healthy and unhealthy food availability and food place characteristics (type and size)
- (4)
- association between healthy and unhealthy food availability and neighborhood income levels.
2. Materials and Methods
2.1. Study Setting and Population
2.2. Classifying Foods into Healthy and Unhealthy Food Categories and Food Healthines Index
- Hot ready-to-eat foods and cold salads assumed were assumed to be prepared at each vendor’s site. Food such as yogurt, ice-cream, processed juices, bread, etc. assumed to be processed at a commercial site outside vendor’s location.
- Foods were classified into food groups based on their most prominent ingredient e.g., Beef stew was classified into the meats food group.
- The Government of Kenya mandates that commercially processed flours be fortified with vitamins and minerals [54]. Hence, we classified maize flours in the healthy grain category.
- Observers did not indicate milk fat levels of milk or milk products not marked as low fat. Kenya’s dairy standards requires milk fat levels of at least 3.25% and an analysis of milk content across value chain recorded milk fat levels of 3.33–3.89%, and we made the decision to classify milk and milk products with unknown fat content as whole-fat [55].
- Regular canned fish and vegetable tend to contain higher sodium levels compared to their non-processed versions and were categorized in the unhealthy food category [56].
2.3. Defining Food Availability Scores
2.4. Food Place Cashpoints
2.5. Healthy Cooking Methods
2.6. Neighborhood Income Status
2.7. Data Analysis
3. Results
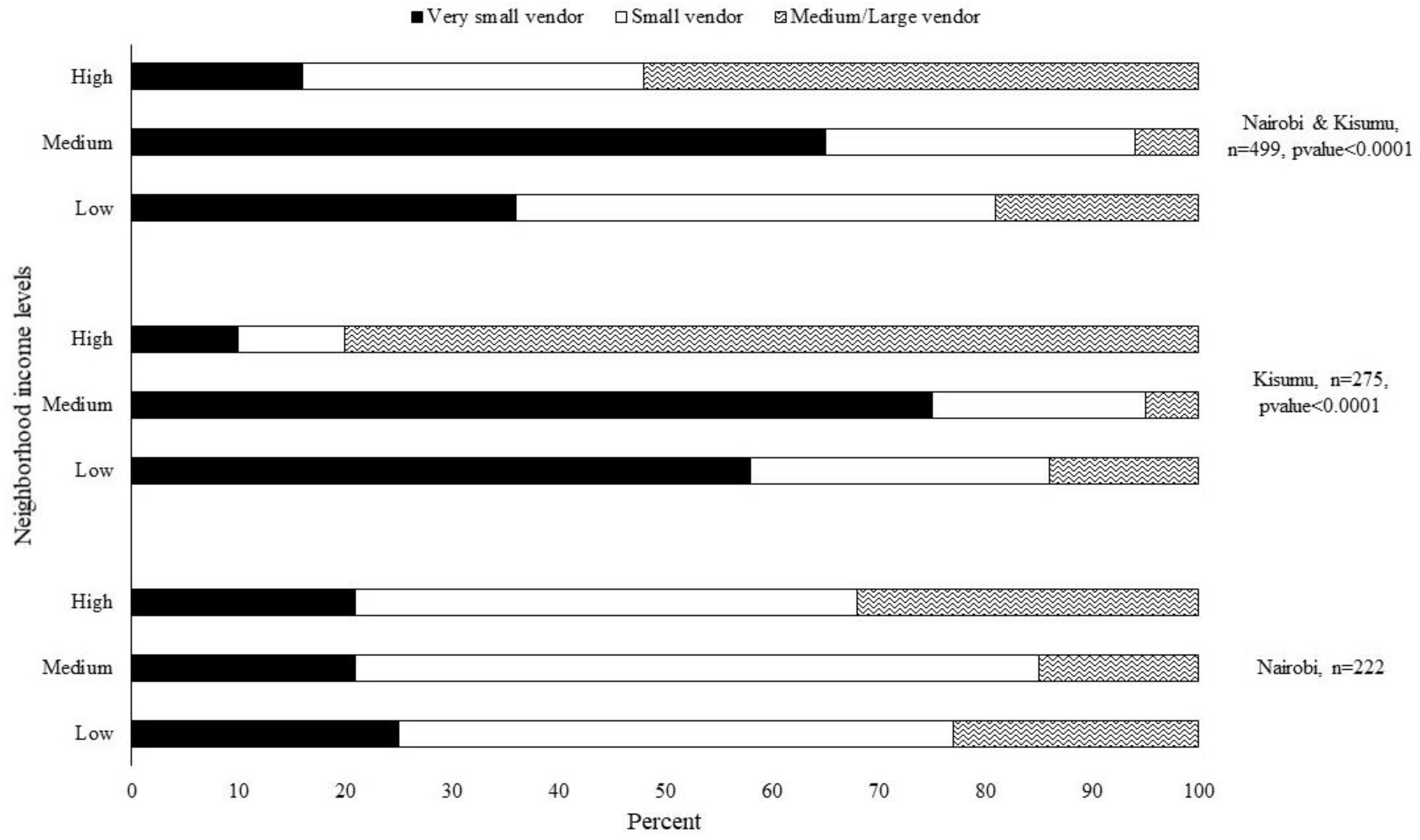
3.1. Types of Food Places
3.2. Availability of Healthy and Unhealthy Foods
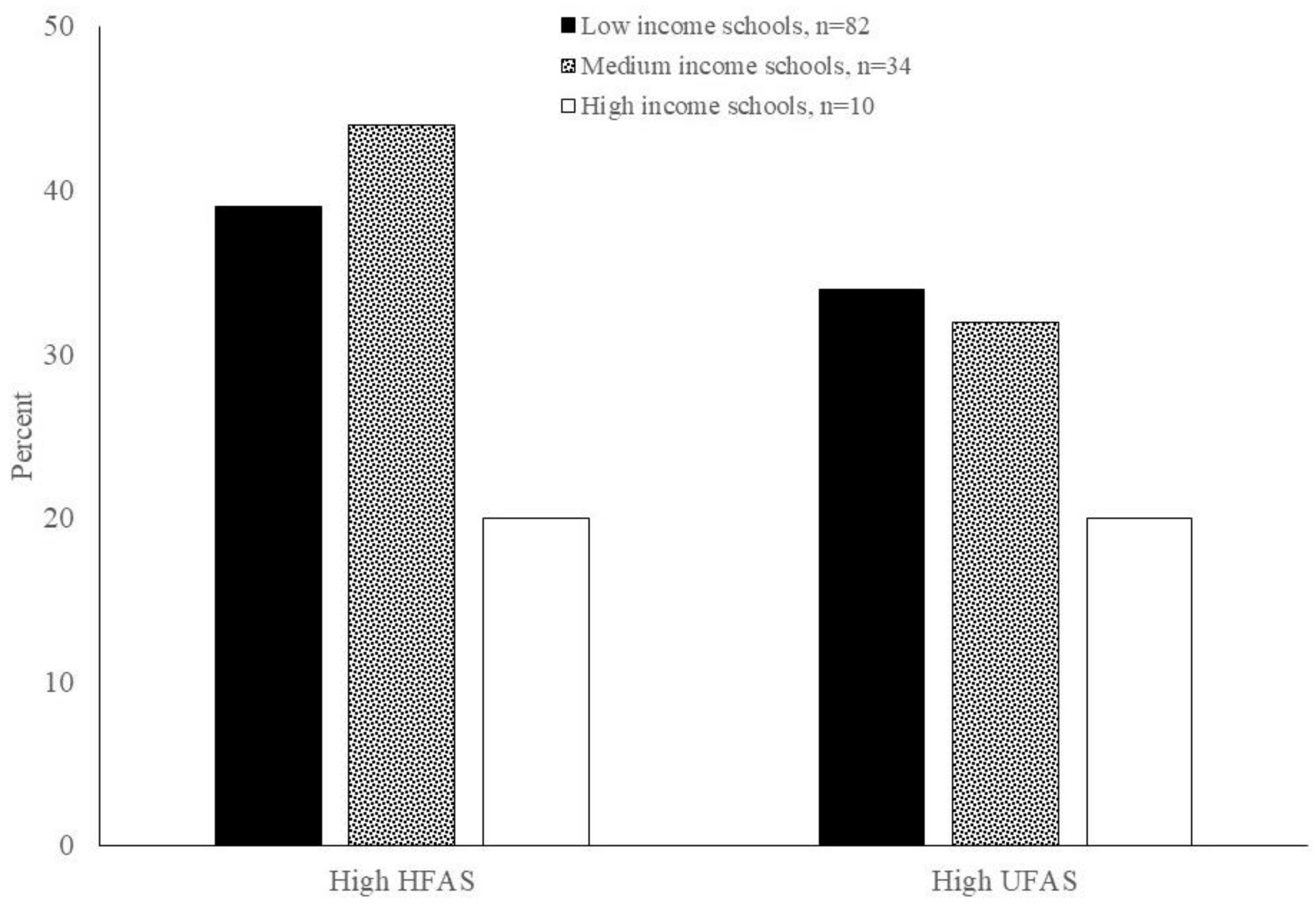
3.3. Healthy Food Availability in Food Places Located within and Near Schools
3.4. Association between Healthy/Unhealthy Food Availability and Food Place Characteristics
4. Discussion
4.1. Study Strengths and Limitations
4.2. Future Research Recommendations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Ethics Statement
Appendix A

{kind=link}
{kind=link}
| Food Place | Food Place Description |
|---|---|
| Supermarket | Large modern self-service stores with offering a large variety of food and non-food products with multiple cash tills. Examples of supermarkets at time of study included Tuskys, Naivas, Carrefour, Khetias, Choppies and Chandarana |
| Mini market | Similar to supermarkets but relatively smaller in size and with a limited variety of products and cash tills |
| Small shop | Modern food retail outlet housed in a permanent building that offers over-the-counter service. Small in size and sells fewer products compared to minimart. |
| Cereal shop | Either a small shop or kiosk that predominantly sells dry cereals e.g., maize, beans, peas, etc. |
| Kiosk | Most common kiosks in Kenya are semi-permanent structures often constructed from a mix iron-sheets and measure an area of about three meters square or below. Kiosks offer a limited number of raw, commercially processed or hot foods. |
| Butcher shop | Specialized shop that predominantly sells meats. Most butcher shops are similar to kiosks and small shops in size. May be semi-permanent structure or located in a permanent building |
| Open-air market seller | Stalls or vendors positioned in a legally-sanctioned open-air market place. Usually sell s, usually with a small number of wares |
| Temporary stand/Street vendor | Stall or vendors positioned on streets and side walks |
| Fast food (chain) | Modern quick service restaurants with limited dine-in or table service. Mostly located within big shopping malls. Part of restaurant chains e.g., KFC, |
| Take-out | Quick service restaurants with limited dine-in or table service, not part of a restaurant-chain |
| Restaurant | Modern restaurants that offer predominantly dine-in or table service |
| Proteins, Breads and Sides | Snacks and Breakfast | Condiments | Dairy | Fresh Produce |
|---|---|---|---|---|
| Fish: fresh, canned | Regular crisps | White sugar | Low fat milk | Fresh vegetables varieties |
| Dried fish | Baked crisps | Artificial sweetener | Full cream | Root vegetables varieties |
| Processed or canned meat | Chips (fries) | Ketchup | Raw milk | Starchy tubers varieties |
| Lean ground meat | Raw/dry-roasted nuts | Tea leaves | Pasteurized milk | Fresh fruits |
| Skinless poultry | Bhajias | Low fat/low calorie condiments | Fermented milk | Fruit salad |
| Eggs | Mandazi | Jam | Powdered milk | |
| Dry beans | High fiber breakfast cereals | Flavored milk | Cooked foods | |
| Dry lentils | Low sugar breakfast cereals | Oils and fats | Milkshake | Cooked vegetables |
| Maize or maize flour | Low fat popcorn | Vegetable oil | Yogurt | Cooked tubers |
| Refined wheat flour | Instant noodles | Olive oil | Butter | Hot coffee or tea |
| Whole wheat flour | Cake | Coconut oil | Ghee | |
| White rice | Crackers | Powdered milk | ||
| Brown rice | Sausages | Non-dairy beverages | Cheese | |
| Sorghum grains or flour | Samosas | Bottled water | ||
| Millet grains or flour | 100% fruit juice | |||
| Mixed whole grain flour | Canned fruit | Soda (regular) | ||
| Bread (refined grain) | Canned fruit (in 100% juice) | Sugar free soda | ||
| 100% whole wheat bread | Canned fruit (not in 100% juice) | Processed juice | ||
| Canned vegetables | Energy drinks | |||
| Cooking banana | Hot cocoa |
| Stew, Meat or Greens: | Staples: | Desserts, Drinks or Snacks: |
|---|---|---|
| Grilled or stewed red meat | Ugali | Baked goods |
| Red meat sandwich/burger | Stewed/boiled bananas | Fruit without sugar (includes fruit cups) |
| Matumbo (tripe) | Chapatis/rotis | 100% fruit juice |
| Grilled or stewed poultry | White rice | Fresh fruit smoothie |
| Poultry sandwich or burger | Brown rice | Yogurt |
| Grilled or stewed fish | Chips | Fermented milk (maziwa lala) |
| Dagaa/Omena | Frozen yogurt | |
| Egg, fried | Accompaniments: | Ice cream |
| Egg, boiled | Bread (refined grain) | Milkshake |
| Ndengu | 100% whole wheat bread | Energy drinks |
| Beans | Pancakes | Regular soda |
| Githeri | Mandazi | Diet soda |
| Mukimo | Samosa | Water |
| Cooked greens | Porridge (non-refined grains) | Low fat milk |
| Non-fried vegetables | Arrowroot, sweet potato | Flavored milk |
| Vegetarian sandwich | Avocado | Tea or coffee with milk |
| Tea or coffee without milk | ||
| Healthy sides: | Raw or dry-roasted nuts | |
| Kachumbari | Crisps, regular | |
| Cole slaw (no mayo) | Crisps, baked | |
| Salad | ||
| Fruits | ||
| Vegetables |
References
- Kenya National Bureau of Statistics; Ministry of Health, National AIDS Control Council; Kenya Medical Research Institute; National Council for Population and Development; The DHS Program; ICF International. Kenya Demographic and Health Survey 2014; Nairobi, Kenya, 2015. Available online: https://dhsprogram.com/pubs/pdf/FR308/FR308.pdf (accessed on 6 November 2018).
- Ministry of Health, Community Development, Gender, Elderly and Children (MoHCDGEC); Ministry of Health (MoH); National Bureau of Statistics (NBS); Office of Chief Government Statistician (OCGS); ICF. Tanzania Demographic and Health Survey and Malaria Indicator Survey (TDHS-MIS) 2015–2016; MoHCDGEC; MoH; NBS; OCGS; ICF: Dar es Salaam, Tanzania; Rockville, MD, USA, 2016. Available online: https://dhsprogram.com/pubs/pdf/FR321/FR321.pdf (accessed on 12 June 2019).
- Uganda Bureau of Statistics (UBOS); ICF. Uganda Demographic and Health Survey 2016; UBOS; ICF: Kampala, Uganda; Rockville, MD, USA, 2018; Available online: https://dhsprogram.com/pubs/pdf/FR333/FR333.pdf (accessed on 3 September 2020).
- Ajayi, I.O.; Adebamowo, C.; Adami, H.-O.; Dalal, S.; Diamond, M.B.; Bajunirwe, F.; Guwatudde, D.; Njelekela, M.; Nankya-Mutyoba, J.; Chiwanga, F.S.; et al. Urban–rural and geographic differences in overweight and obesity in four sub-Saharan African adult populations: A multi-country cross-sectional study. BMC Public Health 2016, 16, 1126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pallangyo, P.; Mkojera, Z.S.; Hemed, N.R.; Swai, H.J.; Misidai, N.; Mgopa, L.; Bhalia, S.; Millinga, J.; Mushi, T.L.; Kabeya, L.; et al. Obesity epidemic in urban Tanzania: A public health calamity in an already overwhelmed and fragmented health system. BMC Endocr. Disord. 2020, 20, 147. [Google Scholar] [CrossRef]
- Kyallo, F.; Makokha, A.; Mwangi, A.M. Overweight and obesity among public and private primary school children in Nairobi, Kenya. Health 2013, 5, 85–90. [Google Scholar] [CrossRef] [Green Version]
- Muthuri, S.K.; Wachira, L.-J.M.; Onywera, V.O.; Tremblay, M.S. Correlates of Objectively Measured Overweight/Obesity and Physical Activity in Kenyan School Children: Results from ISCOLE-Kenya. BMC Public Health 2014, 14, 1–11. Available online: http://0-bmcpublichealth-biomedcentral-com.brum.beds.ac.uk/articles/10.1186/1471-2458-14-436 (accessed on 29 November 2018). [CrossRef] [PubMed] [Green Version]
- FAO. Influencing Food Environments for Healthy Diets; FAO: Rome, Italy, 2016; Available online: http://www.fao.org/3/a-i6484e.pdf (accessed on 1 September 2019).
- Global Panel. Improving Nutrition through Enhanced Food Environments; Report No.: 7; Global Panel on Agriculture and Food Systems for Nutrition: London, UK, 2017; Available online: https://glopan.org/sites/default/files/Downloads/FoodEnvironmentsBrief.pdf (accessed on 1 September 2019).
- Development Initiatives. Global Nutrition Report 2017: Nourishing the SDGs; Development Initiatives: Bristol, UK, 2017; Available online: https://globalnutritionreport.org/reports/2017-global-nutrition-report/ (accessed on 1 September 2019).
- Turner, C.; Kadiyala, S.; Aggarwal, A.; Coates, J.; Drewnowski, A.; Hawkes, C.; Herforth, A.; Kalamatianou, S.; Walls, H. Concepts and Methods for Food Environment Research in Low and Middle Income Countries; Agriculture, Nutrition and Health Academy Food Environment Working Group (ANH-FEWG), Innovative Methods and Metrics for Agriculture and Nutrition Actions (IMMANA) Programme: London, UK, 2017; Available online: https://anh-academy.org/sites/default/files/FEWG_TechnicalBrief_low.pdf (accessed on 1 September 2019).
- Casagrande, S.S.; Whitt-Glover, M.C.; Lancaster, K.J.; Odoms-Young, A.M.; Gary, T.L. Built Environment and Health Behaviors among African Americans. Am. J. Prev. Med. 2009, 36, 174–181. [Google Scholar] [CrossRef] [PubMed]
- Fox, M.K.; Dodd, A.H.; Wilson, A.; Gleason, P.M. Association between School Food Environment and Practices and Body Mass Index of US Public School Children. J. Am. Diet. Assoc. 2009, 109, S108–S117. [Google Scholar] [CrossRef] [PubMed]
- Christiansen, K.M.H.; Qureshi, F.; Schaible, A.; Park, S.; Gittelsohn, J. Environmental Factors That Impact the Eating Behaviors of Low-income African American Adolescents in Baltimore City. J. Nutr. Educ. Behav. 2013, 45, 652–660. [Google Scholar] [CrossRef] [PubMed]
- Morland, K.; Wing, S.; Roux, A.D. The Contextual Effect of the Local Food Environment on Residents’ Diets: The Atherosclerosis Risk in Communities Study. Am. J. Public Health 2002, 92, 1761–1768. [Google Scholar] [CrossRef] [PubMed]
- Pitt, E.; Gallegos, D.; Comans, T.; Cameron, C.; Thornton, L. Exploring the influence of local food environments on food behaviours: A systematic review of qualitative literature. Public Health Nutr. 2017, 20, 2393–2405. [Google Scholar] [CrossRef] [Green Version]
- Duran, A.C.; De Almeida, S.L.; Maria do Rosario, D.O.; Jaime, P.C. The role of the local retail food environment in fruit, vegetable and sugar-sweetened beverage consumption in Brazil. Public Health Nutr. 2016, 19, 1093–1102. [Google Scholar] [CrossRef] [Green Version]
- Shareck, M.; Lewis, D.; Smith, N.R.; Clary, C.; Cummins, S. Associations between home and school neighbourhood food environments and adolescents’ fast-food and sugar-sweetened beverage intakes: Findings from the Olympic Regeneration in East London (ORiEL) Study. Public Health Nutr. 2018, 21, 2842–2851. [Google Scholar] [CrossRef] [Green Version]
- Barrett, M.; Crozier, S.; Lewis, D.; Godfrey, K.; Robinson, S.; Cooper, C.; Inskip, H.; Baird, J.; Vogel, C. Greater access to healthy food outlets in the home and school environment is associated with better dietary quality in young children. Public Health Nutr. 2017, 20, 3316–3325. [Google Scholar] [CrossRef]
- Turner, C.; Kalamatianou, S.; Drewnowski, A.; Kulkarni, B.; Kinra, S.; Kadiyala, S. Food Environment Research in Low- and Middle-Income Countries: A Systematic Scoping Review. Adv. Nutr. 2020, 11(2), 387–397. [Google Scholar] [CrossRef] [PubMed]
- Spires, M.; Berggreen-Clausen, A.; Kasujja, F.X.; Delobelle, P.; Puoane, T.; Sanders, D.; Daivadanam, M. Snapshots of Urban and Rural Food Environments: EPOCH-Based Mapping in a High-, Middle-, and Low-Income Country from a Non-Communicable Disease Perspective. Nutrients 2020, 12, 484. [Google Scholar] [CrossRef] [Green Version]
- Khonje, M.G.; Qaim, M. Modernization of African Food Retailing and (Un)healthy Food Consumption. Sustainability 2019, 11, 4306. [Google Scholar] [CrossRef] [Green Version]
- Rischke, R.; Kimenju, S.C.; Klasen, S.; Qaim, M. Supermarkets and food consumption patterns: The case of small towns in Kenya. Food Policy 2015, 52, 9–21. [Google Scholar] [CrossRef]
- Das Nair, R.; Chisoro, S.; UNU-WIDER. The Expansion of Regional Supermarket Chains: Changing Models of Retailing and the Implications for Local Supplier Capabilities in South Africa, Botswana, Zambia, and Zimbabwe, 114th ed.; WIDER Working Paper; UNU-WIDER: Helsinki, Finland, 2015; Volume 2015, Available online: https://www.wider.unu.edu/node/9464 (accessed on 16 October 2020).
- Veselinovic, M. How Africa is Giving Fast Food a New Spin. CNN. Available online: https://www.cnn.com/2015/12/11/africa/fast-food-in-africa/index.html (accessed on 16 October 2020).
- Baker, P.; Friel, S. Food systems transformations, ultra-processed food markets and the nutrition transition in Asia. Glob. Health 2016, 12, 80. [Google Scholar] [CrossRef] [Green Version]
- Downs, S.M.; Ahmed, S.; Fanzo, J.; Herforth, A. Food Environment Typology: Advancing an Expanded Definition, Framework, and Methodological Approach for Improved Characterization of Wild, Cultivated, and Built Food Environments toward Sustainable Diets. Foods 2020, 9, 532. [Google Scholar] [CrossRef] [Green Version]
- Weaver, C.M.; Dwyer, J.; Fulgoni, V.L.; King, J.C.; A Leveille, G.; Macdonald, R.S.; Ordovas, J.; Schnakenberg, D. Processed foods: Contributions to nutrition. Am. J. Clin. Nutr. 2014, 99, 1525–1542. [Google Scholar] [CrossRef]
- Monteiro, C.A.; Levy, R.B.; Claro, R.M.; De Castro, I.R.R.; Cannon, G. Increasing consumption of ultra-processed foods and likely impact on human health: Evidence from Brazil. Public Health Nutr. 2010, 14, 5–13. [Google Scholar] [CrossRef]
- Steele, E.M.; Baraldi, L.G.; da Costa Louzada, M.L.; Moubarac, J.C.; Mozaffarian, D.; Monteiro, C.A. Ultra-processed foods and added sugars in the US diet: Evidence from a nationally representative cross-sectional study. BMJ Open 2016, 6, e009892. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poti, J.M.; Mendez, M.A.; Ng, S.W.; Popkin, B.M. Is the degree of food processing and convenience linked with the nutritional quality of foods purchased by US households? Am. J. Clin. Nutr. 2015, 101, 1251–1262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bleiweiss-Sande, R.; Chui, K.; Evans, E.W.; Goldberg, J.; Amin, S.; Sacheck, J. Robustness of Food Processing Classification Systems. Nutrients 2019, 11, 1344. [Google Scholar] [CrossRef] [Green Version]
- Monteiro, C.; Canon, G.; Lawrence, M.; Costa Louzada, M.; Pereira Machado, P. Ultra-Processed Foods, Diet Quality, and Health Using the NOVA Classification System; FAO: Rome, Italy, 2019; Available online: http://www.fao.org/3/ca5644en/ca5644en.pdf (accessed on 31 March 2021).
- Briefel, R.R.; Crepinsek, M.K.; Cabili, C.; Wilson, A.; Gleason, P.M. School Food Environments and Practices Affect Dietary Behaviors of US Public School Children. J. Am. Diet. Assoc. 2009, 109, S91–S107. [Google Scholar] [CrossRef]
- Micha, R.; Karageorgou, D.; Bakogianni, I.; Trichia, E.; Whitsel, L.P.; Story, M.; Peñalvo, J.L.; Mozaffarian, D. Effectiveness of school food environment policies on children’s dietary behaviors: A systematic review and meta-analysis. PLoS ONE 2018, 13, e0194555. [Google Scholar] [CrossRef]
- Khonje, M.G.; Ecker, O.; Qaim, M. Effects of Modern Food Retailers on Adult and Child Diets and Nutrition. Nutrients 2020, 12, 1714. [Google Scholar] [CrossRef]
- Wojcicki, J.; Elwan, D. Primary School Nutrition and Tuck Shops in Hhoho, Swaziland. J. Child Nutr. Manag. 2014, 38. Available online: https://schoolnutrition.org/5--News-and-Publications/4--The-Journal-of-Child-Nutrition-and-Management/Spring-2014/Volume-38,-Issue-1,-Spring-2014---Wojcicki,-Elwan/ (accessed on 21 July 2020).
- Kroll, F.; Swart, E.C.; Annan, R.A.; Thow, A.M.; Neves, D.; Apprey, C.; Aduku, L.N.E.; Agyapong, N.A.F.; Moubarac, J.-C.; Du Toit, A.; et al. Mapping Obesogenic Food Environments in South Africa and Ghana: Correlations and Contradictions. Sustainability 2019, 11, 3924. [Google Scholar] [CrossRef] [Green Version]
- Campbell, E.A.; Shapiro, M.J.; Welsh, C.; Bleich, S.N.; Cobb, L.K.; Gittelsohn, J. Healthy Food Availability Among Food Sources in Rural Maryland Counties. J. Hunger. Environ. Nutr. 2017, 12, 328–341. [Google Scholar] [CrossRef] [Green Version]
- Hilmers, A.; Hilmers, D.C.; Dave, J. Neighborhood Disparities in Access to Healthy Foods and Their Effects on Environmental Justice. Am. J. Public Health 2012, 102, 1644–1654. [Google Scholar] [CrossRef]
- 2019 Kenya Population and Housing Census. Volume II: Distribution of Population and Administrative Units; Kenya National Bureau of Statistics (KNBS). Available online: http://housingfinanceafrica.org/app/uploads/VOLUME-II-KPHC-2019.pdf (accessed on 6 October 2020).
- Da Cruz, F.; Sommer, K.; Tempra, O. Nairobi Urban Sector Profile; UN-HABITAT: Nairobi, Kenya, 2006; Available online: https://www.worldurbancampaign.org/sites/default/files/kenya_-_nairobi.pdf (accessed on 6 October 2020).
- Gulyani, S.; Ayres, W.; Struyk, R.; Zinnes, C. Kenya State of the Cities: Baseline Survey; World Bank Group: Washington, DC, USA, 2014; Available online: http://microdata.worldbank.org/index.php/catalog/2796/download/39725 (accessed on 6 October 2020).
- Owuor, S. The State of Household Food Security in Nairobi, Kenya. Hungry Cities PartnershiP. 2018. Available online: https://hungrycities.net/wp-content/uploads/2018/07/HCP11.pdf (accessed on 6 October 2020).
- Opiyo, P.; Obange, N.; Ogindo, H.; Wagah, G. The Characteristics, Extent and Drivers of Urban Food Poverty in Kisumu, Kenya; (Consuming Urban Poverty Project Working Paper); Report No.: 4; African Centre for Cities, University of Cape Town: Cape Town, South Africa, 2018; Available online: https://consumingurbanpoverty.files.wordpress.com/2019/01/cup-wp-4-kisumufoodpoverty-1.pdf (accessed on 26 August 2020).
- Zuilkowski, S.S.; Piper, B.; Ong’Ele, S.; Kiminza, O. Parents, quality, and school choice: Why parents in Nairobi choose low-cost private schools over public schools in Kenya’s free primary education era. Oxf. Rev. Educ. 2017, 44, 258–274. [Google Scholar] [CrossRef]
- Berenson, M.L.; Levine, D.M.; Szabat, K. Estimation and Sample Size Determination for Finite Populations. Basic Business Statistics: Global Edition. Available online: https://www.alnap.org/help-library/estimation-and-sample-size-determination-for-finite-populations-basic-business (accessed on 9 November 2018).
- Holt, D.; Littlewood, D. The informal economy as a route to market in sub-Saharan Africa–observations amongst Kenyan informal economy entrepreneurs. In The Routledge Companion to Business in Africa; Routledge: London, UK, 2014; pp. 198–217. Available online: http://repository.essex.ac.uk/10455/1/IE%20chapter_opaacv.pdf (accessed on 6 April 2021).
- Kamau, C. Kenya’s Retail Sector Adapting to Competition; (Retail Foods); Office of Agricultural Affairs, Embassy of the United States of America: Nairobi, Kenya, 2017. Available online: https://www.fas.usda.gov/data/kenya-kenyas-retail-sector-adapting-competition (accessed on 18 March 2021).
- Gittelsohn, J.; Franceschini, M.C.; Rasooly, I.R.; Ries, A.V.; Ho, L.S.; Pavlovich, W.; Santos, V.T.; Jennings, S.M.; Frick, K.D. Understanding the Food Environment in a Low-Income Urban Setting: Implications for Food Store Interventions. J. Hunger. Environ. Nutr. 2008, 2, 33–50. [Google Scholar] [CrossRef]
- Lee, S.H.; Rowan, M.T.; Powell, L.M.; Newman, S.; Klassen, A.C.; Frick, K.D.; Anderson, J.; Gittelsohn, J. Characteristics of Prepared Food Sources in Low-Income Neighborhoods of Baltimore City. Ecol. Food Nutr. 2010, 49, 409–430. [Google Scholar] [CrossRef] [Green Version]
- Ministry of Health (MOH). National Guidelines for Healthy Diets and Physical Activity; Ministry of Health; Government of Kenya: 2017. Available online: http://www.fao.org/nutrition/education/food-dietary-guidelines/regions/countries/kenya/en/ (accessed on 16 August 2019).
- Vandevijvere, S.; Swinburn, B. Healthy Food Environment Policy Index (Food EPI). Extent of Implementation of Food Environment Policies by Governments Compared to International Best Practice & Priority Recommendations. The University of Auckland. 2017. Available online: https://www.informas.org/ (accessed on 5 April 2021).
- Enzama, W.; Afidra, R.; Johnson, R.; Verster, A. Africa Maize Fortification Strategy 2017–2026; Smarter Futures. 2017. Available online: https://www.smarterfutures.net/wp-content/uploads/2017/01/maize_FINAL_spreads.pdf (accessed on 7 April 2021).
- Nyokabi, S.N.; de Boer, I.J.M.; Luning, P.A.; Korir, L.; Lindahl, J.; Bett, B.; Oosting, S.J. Milk quality along dairy farming systems and associated value chains in Kenya: An analysis of composition, contamination and adulteration. Food Control 2021, 119, 107482. [Google Scholar] [CrossRef]
- Elliot, P.; Brown, I. Sodium Intakes around the World; World Health Organization (WHO): Geneva, Switzerland, 2007; Available online: https://www.who.int/dietphysicalactivity/Elliot-brown-2007.pdf (accessed on 22 March 2021).
- Franco, M.; Diez Roux, A.V.; Glass, T.A.; Caballero, B.; Brancati, F.L. Neighborhood Characteristics and Availability of Healthy Foods in Baltimore. Am. J. Prev. Med. 2008, 35, 561–567. [Google Scholar] [CrossRef]
- Creel, J.S.; Sharkey, J.R.; McIntosh, A.; Anding, J.; Huber, J.C. Availability of healthier options in traditional and nontraditional rural fast-food outlets. BMC Public Health 2008, 8, 395. [Google Scholar] [CrossRef] [Green Version]
- Campbell, K.B.; Rising, J.A.; Klopp, J.M.; Mbilo, J.M. Accessibility across transport modes and residential developments in Nairobi. J. Transp. Geogr. 2019, 74, 77–90. [Google Scholar] [CrossRef]
- Cities of Hope? Governance, Economic and Human Challenges of Kenya’s Five Largest Cities; World Bank: Washington, DC, USA, 2008; Available online: http://documents1.worldbank.org/curated/en/485151468276389932/pdf/469880ESW0Whit10Cities0Report0Final.pdf (accessed on 2 November 2020).
- Bridle-Fitzpatrick, S. Food deserts or food swamps? A mixed-methods study of local food environments in a Mexican city. Soc. Sci. Med. 2015, 142, 202–213. [Google Scholar] [CrossRef]
- Trübswasser, U.; Baye, K.; Holdsworth, M.; Loeffen, M.; Feskens, E.J.; Talsma, E.F. Assessing factors influencing adolescents’ dietary behaviours in urban Ethiopia using participatory photography. Public Health Nutr. 2020, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Larson, N.I.; Story, M.T.; Nelson, M.C. Neighborhood environments: Disparities in access to healthy foods in the U.S. Am. J. Prev. Med. 2009, 36, 74–81.e10. [Google Scholar] [CrossRef] [PubMed]
- Neckerman, K.M.; Bader, M.D.M.; Richards, C.A.; Purciel, M.; Quinn, J.W.; Thomas, J.S.; Warbelow, C.; Weiss, C.C.; Lovasi, G.S.; Rundle, A. Disparities in the Food Environments of New York City Public Schools. Am. J. Prev. Med. 2010, 39, 195–202. [Google Scholar] [CrossRef] [Green Version]
- Chan Sun, M.; Lalsing, Y.; Subratty, A.H. Primary school food environment in Mauritius. Nutr. Food Sci. 2009, 39, 251–259. [Google Scholar] [CrossRef]
- Wiles, N.L.; Green, J.M.; Veldman, F.J. Tuck-shop purchasing practices of Grade 4 learners in Pietermaritzburg and childhood overweight and obesity. South Afr. J. Clin. Nutr. 2013, 26, 37–42. [Google Scholar] [CrossRef]
- Faber, M.; Laurie, S.; Maduna, M.; Magudulela, T.; Muehlhoff, E. Is the school food environment conducive to healthy eating in poorly resourced South African schools? Public Health Nutr. 2013, 17, 1214–1223. [Google Scholar] [CrossRef] [Green Version]
- Oogarah-Pratap, B.; Heerah-Booluck, B.J. Children’s consumption of snacks at school in Mauritius. Nutr. Food Sci. 2005, 35, 15–19. [Google Scholar] [CrossRef]
- Rathi, N.; Riddell, L.; Worsley, A. Parents’ and Teachers’ Views of Food Environments and Policies in Indian Private Secondary Schools. Int. J. Environ. Res. Public Health 2018, 15, 1532. [Google Scholar] [CrossRef] [Green Version]
- Ministry of Education (MOE), Ministry of Health (MOH), Ministry of Agriculture, Livestock and Fisheries (MOALF). National School Meals and Nutrition Strategy: 2017–2022. Available online: https://reliefweb.int/sites/reliefweb.int/files/resources/WFP-0000070917.pdf (accessed on 14 April 2019).
- Monteiro, C.; Cannon, G.; Levy, R.; Moubarac, J.-C.; Jaime, P.; Martins, A.; Canella, D.; Louzada, M.; Parra, D. NOVA. The star shines bright. World Nutr. 2016, 7, 28–38. [Google Scholar]


| Food Group | Examples of Healthy Foods | Examples of Unhealthy Foods |
|---|---|---|
| Vegetables | Raw vegetables (e.g., kales, cabbages, tomatoes, onions, carrots, beets, arrowroots potatoes, green bananas and kachumbari/salsa), cooked greens, baked crisps | Chips, regular crisps, chips, bhajia, samosa, vegetable sandwich, canned vegetables |
| Fruits | Fresh fruit, fruit salad, canned fruit in 100% juice, 100% fruit juice | Canned fruit not in 100% fruit juice |
| Legumes, nuts & seeds | Beans, lentils, raw or dry-roasted nuts, green grams (mung beans), githeri, mukimo | |
| Meat | Lean ground beef, tripe | Red meat, canned meat, sausage, red meat sandwich/burger |
| Fish | Fresh, dried, grilled or stewed fish, omena (dagaa) | Canned fish |
| Poultry | Skinless poultry, grilled or stewed poultry, eggs | Poultry sandwich |
| Grains | Whole wheat flour, whole wheat bread, porridge, ugali, brown rice, sorghum, millet, mixed grain flour, maize or maize flour, low fat popcorn, refined wheat flour | White rice, white bread, baked goods, pancakes chapati, mandazi, |
| Dairy | Low fat milk, tea or coffee with milk | Milk (full fat, flavored, fermented), milkshake, yoghurt, ice-cream, frozen yogurt, milkshake, pasteurized milk |
| Non-dairy drinks | Bottled or plain water, hot cocoa, tea or coffee without milk, sugar-free/diet soda | Regular soda, processed juice, energy drinks |
| Oils and fats | Vegetable oil or fats (includes margarines), olive oil, coconut oil | Butter, ghee |
| Condiments | Tea leaves | Sugar, ketchup, jam |
| Food Place | Size | Nairobi and Kisumu | Nairobi | Kisumu |
|---|---|---|---|---|
| Retail food outlets: | n = 364 | n = 143 | n = 221 | |
| Supermarket | Large | 9 | 13 | 6 |
| Mini market | Medium | 2 | 3 | 1 |
| Small shop | Small | 12 | 19 | 8 |
| Cereal shop | Small | 6 | 15 | 1 |
| Kiosk | Small | 6 | 9 | 3 |
| Butcher | Small | 10 | 14 | 7 |
| Open-air market seller | Very small | 48 | 21 | 66 |
| Temporary stand/Street vendor | Very small | 7 | 6 | 8 |
| Prepared food sources: | n = 144 | n = 84 | n = 60 | |
| Fast food (chain) | Large | 8 | 11 | 3 |
| Restaurant | Large | 22 | 18 | 28 |
| Take out | Large | 13 | 6 | 22 |
| Food kiosk | Small | 40 | 46 | 32 |
| Street vendor | Very small | 14 | 16 | 12 |
| Food place and Characteristics | Nairobi and Kisumu | Nairobi | Kisumu |
|---|---|---|---|
| Food retail outlets: | n = 362 | n = 143 | n = 219 |
| Low income neighborhood | 35 | 54 | 23 |
| Medium-income neighborhood | 50 | 18 | 70 |
| High income neighborhood | 15 | 27 | 7 |
| Having multiple cashpoints | 12 | 13 | 11 |
| Prepared food sources: | n = 144 | n = 84 | n = 60 |
| Low income neighborhood | 40 | 57 | 14 |
| Medium-income neighborhood | 29 | 20 | 43 |
| High income neighborhood | 31 | 23 | 43 |
| Having multiple cashpoints | 6 | 3 | 11 |
| Variety of healthy cooking methods: | |||
| 0 | 37 | 27 | 51 |
| 1–2 | 62 | 73 | 47 |
| 3–5 | 1 | 0 | 2 |
| Variety of healthy sides: | |||
| 0 | 33 | 31 | 37 |
| 1–2 | 62 | 65 | 58 |
| 3–5 | 3 | 1 | 5 |
| Unknown | 2 | 3 | 0 |
| Food Group | Food Retail Outlets | Prepared Food Sources | ||||
|---|---|---|---|---|---|---|
| Nairobi & Kisumu, n = 362 | Nairobi, n = 143 | Kisumu, n = 219 | Nairobi and Kisumu, n = 138 | Nairobi, n = 81 | Kisumu, n = 57 | |
| Healthy foods: | ||||||
| Vegetables | 54 | 67 | 45 **** | 74 | 73 | 77 |
| Fruits | 39 | 37 | 41 | 40 | 37 | 45 |
| Legumes, nuts & seeds | 41 | 57 | 31 **** | 48 | 42 | 55 |
| Meat | 7 | 15 | 1 **** | 35 | 32 | 39 |
| Fish | 16 | 27 | 8 **** | 43 | 38 | 50 |
| Poultry | 42 | 69 | 24 **** | 64 | 64 | 63 |
| Grains | 37 | 50 | 28 *** | 59 | 60 | 57 |
| Dairy | 5 | 4 | 6 | 52 | 54 | 50 |
| Non-dairy drinks | 29 | 48 | 17 **** | 70 | 73 | 66 |
| Oils and fats | 27 | 44 | 16 **** | |||
| Condiments | 24 | 36 | 16 **** | |||
| Unhealthy foods: | ||||||
| Vegetables | 23 | 40 | 13 **** | 54 | 48 | 63 |
| Fruits | 4 | 6 | 0 ** | |||
| Legumes, nuts & seeds | ||||||
| Meat | 8 | 10 | 6 | 69 | 72 | 66 |
| Fish | 2 | 0 | 4 * | |||
| Poultry | 15 | 7 | 25 ** | |||
| Grains | 41 | 59 | 29 **** | 79 | 79 | 79 |
| Dairy | 25 | 38 | 16 **** | 14 | 9 | 21 * |
| Non-dairy drinks | 28 | 44 | 17 **** | 47 | 46 | 48 |
| Oils and fats | 4 | 1 | 6 * | |||
| Condiments | 27 | 43 | 16 **** | |||
| Size of Food Place | Examples | Low SES Schools, n = 82 | Medium SES Schools, n = 34 | High SES Schools, n = 10 |
|---|---|---|---|---|
| Very small | Open-air market stands, temporary stands and street vendors | 30 | 29 | 40 |
| Small | Small shops, kiosks and butcheries | 47 | 53 | 30 |
| Medium and large | Supermarkets, minimarts, and fast food places and restaurants | 22 | 12 | 0 |
| School canteens and lunch programs | 1 | 6 | 30 |
| Food Availability Score and Independent Variables | Bivariate Models, n = 499 | Multivariate Models, n = 499 | ||
|---|---|---|---|---|
| PR | CI | PR | CI | |
| Healthy Food Availability Score (HFAS) | ||||
| Nairobi (ref = Kisumu) | 2.21 | (1.73, 2.84) | ||
| Retail outlet (ref = prepared food source) | 0.87 | (0.68, 1.12) | ||
| Having multiple cashpoints (ref= having one cashpoint) | 2.44 | (1.98, 3.00) | 1.95 | (1.54, 2.48) |
| Small-sized food places (ref = very small) | 5.06 | (3.32, 7.74) | 1.11 | (0.88, 1.41) |
| Medium or large-sized food places (ref = very small) | 7.06 | (4.65, 10.7) | 1.67 | (1.35, 2.07) |
| Medium income neighborhood (ref = low income neighborhood) | 0.60 | (0.45, 0.81) | 0.84 | (0.60, 1.18) |
| High income neighborhood (ref = low income neighborhood) | 1.47 | (1.15, 1.89) | 1.42 | (1.11, 1.81) |
| Unhealthy Food Availability Score (UFAS) | ||||
| Nairobi (ref = Kisumu) | 2.14 | (1.63, 2.82) | ||
| Retail outlet (ref = prepared food source) | 0.87 | (0.66, 1.15) | ||
| Having multiple cashpoints (ref = having one cashpoint) | 3.24 | (2.64, 3.98) | 2.32 | (1.85, 2.90) |
| Small-sized food places (ref = very small) | 18.8 | (7.75, 45.4) | 1.17 | (0.95, 1.40) |
| Medium or large-sized food places (ref = very small) | 34.6 | (14.5, 83.0) | 17.6 | (7.25, 42.8) |
| Medium income neighborhood (ref = low income neighborhood) | 0.69 | (0.49, 0.97) | 0.96 | (0.65, 1.42) |
| High income neighborhood (ref = low income neighborhood) | 1.87 | (1.41, 2.47) | 1.81 | (1.38, 2.38) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gewa, C.A.; Onyango, A.C.; Opiyo, R.O.; Cheskin, L.; Gittelsohn, J. Food Environment in and around Primary School Children’s Schools and Neighborhoods in Two Urban Settings in Kenya. Int. J. Environ. Res. Public Health 2021, 18, 5136. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18105136
Gewa CA, Onyango AC, Opiyo RO, Cheskin L, Gittelsohn J. Food Environment in and around Primary School Children’s Schools and Neighborhoods in Two Urban Settings in Kenya. International Journal of Environmental Research and Public Health. 2021; 18(10):5136. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18105136
Chicago/Turabian StyleGewa, Constance Awuor, Agatha Christine Onyango, Rose Okoyo Opiyo, Lawrence Cheskin, and Joel Gittelsohn. 2021. "Food Environment in and around Primary School Children’s Schools and Neighborhoods in Two Urban Settings in Kenya" International Journal of Environmental Research and Public Health 18, no. 10: 5136. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18105136