
Contemplating Help-Seeking in Perinatal Psychological Distress—A Meta-Ethnography


Abstract
:
1. Introduction
1.1. Theoretical Perspective
1.2. Aim and Research Question
2. Materials and Methods
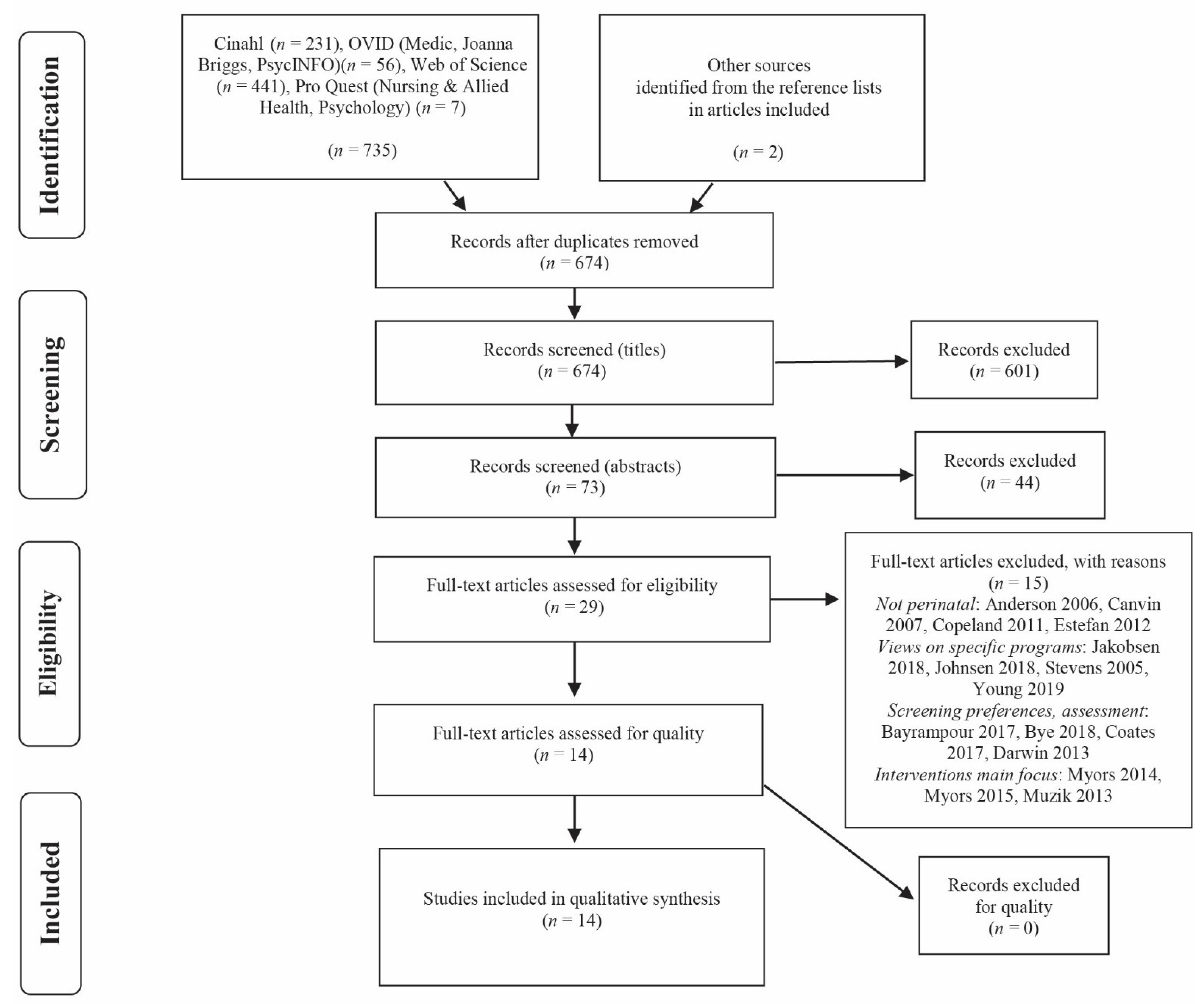
2.1. Search Strategy and Criteria
- mental disorders* OR help seeking behavior* AND mothers* OR maternal
- help-seeking behavior OR health care seeking behavior OR health behavior OR acceptability of health care OR patient acceptance of healthcare OR services utilization OR health care utilization OR health seeking OR health care seeking behavior OR perceived barriers OR barriers to OR facilitators to OR perceived access OR perceived barrier OR client participation OR client engagement OR client involvement
- mental disorders OR mental health disorder OR mental health or anxiety OR anxiety disorders OR depression OR depressive symptoms OR mental illness OR psychiatric and anxiety OR psychotic disorders
- pregnancy OR infant OR baby OR child OR perinatal time. Finally, we wanted to focus on qualitative studies, so we combined the previous searches with AND qualitative studies OR qualitative research OR phenomenology. We did not include alternate spellings such as ‘utilisation’ in addition to ‘utilization’.
2.2. Qualitative Appraisal of the Studies
2.3. The Interpretation and Synthesis Process
3. Results
3.1. Falling into Pieces
“Problems quickly generalised to all aspects of infant care: ‘once you failed at one thing, for example you thought you’d failed at your breastfeeding, you then decided you were going to fail at everything. So it kind of just circles off’.”[39]
“I was afraid to show my new baby any affection in front of my toddler for fear that she would think I didn’t love her anymore.”[42]
3.2. Trying so Hard
“I’d be told it was normal, that it was fine, that everybody felt that way, that it shouldn’t matter because I should just be happy that I have a healthy baby.”[48]
“I even went in at 3 months and I talked to a health nurse, and I just lied through my teeth because I thought, “What are they going to do if they find out I can’t be a good mom?”[40]
3.3. Having no Energy to Act
“When I was experiencing mental health issues, it was harder for me to get out, sort of on a schedule and be punctual.”[48]
3.4. Lacking Shared Experiences
“I still felt so alone as nobody in my close knit group of friends and family had ever had gone thought this and could not truly relate.”[42]
“I ask my husband for help, and he tries for maybe two days, then it’s right back to being unhelpful and uncaring.”[42]
“I don’t think I sought outside help because I didn’t know.”[43]
“The participant developed negative beliefs about the side effects of medications. Whether or not the information gained by participants through experience with family members or the media is accurate, it influenced their beliefs about postpartum depressive symptoms and possible treatments.”[46]
“There’s the fear of really telling the truth and I felt safer telling the midwife than I did telling my doctor the depth of how I was feeling because I was really scared and I was having pretty awful thoughts and even though I was seeing them both at the same time and they were both referring me, I didn’t really open up to my doctor and tell her the truth if you know what I mean?”[48]
3.5. Not Understanding One Has an Illness
“I just didn’t know what I wanted at the time and I didn’t know what I wanted to get out of it. I didn’t know what was going on.”[47]
3.6. Emerging Awareness
“It’s as though you have to figure it out for yourself first before you actually get the resources you need.”[48]
“The knowledge of mental health. I think it is probably the biggest thing, knowing, recognizing the signs and symptoms. Just knowing that I needed to seek help before it got worse.”[45]
3.7. Placing Hope in Oneself
“I had to do it all on my own, because nobody could do it well enough. I had a lot of anxiety. I didn’t want anybody holding him, I didn’t want anybody touching him. I didn’t want anybody in my house, because if I turned around and left him alone for a second, somebody would hurt my baby.”[40]
3.8. The Metaphor of a Seed
4. Discussion
4.1. Implications for Practice
4.2. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Saint Arnault, D. Defining and Theorizing About Culture. The evolution of the Cultural Determinants of Help-Seeking, Revised. Nurs. Res. 2018, 16, 161–168. [Google Scholar] [CrossRef] [PubMed]
- Ridner, S.H. Psychological distress: Concept analysis. J. Adv. Nurs. 2004, 45, 536–545. [Google Scholar] [CrossRef]
- Obrochta, C.A.; Chambers, C.; Bandoli, G. Psychological distress in pregnancy and postpartum. Women Birth 2020, 33, 583–591. [Google Scholar] [CrossRef] [PubMed]
- Button, S.; Thornton, A.; Lee, S.; Shakespeare, J.; Ayers, S. Seeking help for perinatal psychological distress: A meta-synthesis of women’s experiences. Br. J. Gen. Pract. 2017, 67, E692–E699. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dennis, C.L.; Chung-Lee, L. Postpartum depression help-seeking barriers and maternal treatment preferences: A qualitative systematic review. Birth-Issues Perinat. Care 2006, 33, 323–331. [Google Scholar] [CrossRef] [PubMed]
- Myors, K.A.; Schmied, V.; Johnson, M.; Cleary, M. ‘My special time’: Australian women’s experiences of accessing a specialist perinatal and infant mental health service. Health Soc. Care Community 2014, 22, 268–277. [Google Scholar] [CrossRef] [PubMed]
- Liberto, T.L. Screening for Depression and Help-Seeking in Postpartum Women During Well-Baby Pediatric Visits: An Integrated Review. J. Pediatric Health Care 2012, 26, 109–117. [Google Scholar] [CrossRef] [PubMed]
- Hadfield, H.; Wittkowski, A. Women’s Experiences of Seeking and Receiving Psychological and Psychosocial Interventions for Postpartum Depression: A Systematic Review and Thematic Synthesis of the Qualitative Literature. J. Midwifery Womens Health 2017, 62, 723–736. [Google Scholar] [CrossRef] [PubMed]
- Glasheen, C.; Colpe, L.; Hoffman, V.; Warren, L.K. Prevalence of Serious Psychological Distress and Mental Health Treatment in a National Sample of Pregnant and Postpartum Women. Matern. Child Health J. 2015, 19, 204–216. [Google Scholar] [CrossRef]
- Bales, M.; Pambrun, E.; Melchior, M.; Glangeaud-Freudenthal, N.M.C.; Charles, M.A.; Verdoux, H.; Sutter-Dallay, A.-L. Prenatal psychological distress and access to mental health care in the ELFE cohort. Eur. Psychiatry 2015, 30. [Google Scholar] [CrossRef]
- Woody, C.A.; Ferrari, A.J.; Siskind, D.J.; Whiteford, H.A.; Harris, M.G. A systematic review and meta-regression of the prevalence and incidence of perinatal depression. J. Affect. Disord. 2017, 219, 86–92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wisner, K.L.; Sit, D.K.Y.; McShea, M.C.; Rizzo, D.M.; Zoretich, R.A.; Hughes, C.L.; Eng, H.F.; Luther, J.F.; Wisniewski, S.R.; Costantino, M.L.; et al. Onset Timing, Thoughts of Self-harm, and Diagnoses in Postpartum Women with Screen-Positive Depression Findings. JAMA Psychiatry 2013, 70, 490–498. [Google Scholar] [CrossRef] [PubMed]
- Chan, M.E. Antecedents of Instrumental Interpersonal Help-Seeking: An Integrative Review. Appl. Psychol. Int. Rev. Psychol. Appl. Rev. Int. 2013, 62, 571–596. [Google Scholar] [CrossRef]
- Rickwood, D.; Thomas, K. Conceptual measurement framework for help-seeking for mental health problems. Psychol. Res. Behav. Manag. 2012, 5, 173–183. [Google Scholar] [CrossRef] [Green Version]
- Cornally, N.; McCarthy, G. Help-seeking behaviour: A concept analysis. Int. J. Nurs. Pract. 2011, 17, 280–288. [Google Scholar] [CrossRef]
- Saunders, S.; Bowersox, N. The Process of Seeking Treatment for Mental Health Problems. Ment. Health Learn. Disabil. Res. Pract. 2007, 4, 99–123. [Google Scholar] [CrossRef] [Green Version]
- Jones, C.C.G.; Jomeen, J.; Hayter, M. The impact of peer support in the context of perinatal mental illness: A meta-ethnography. Midwifery 2014, 30, 491–498. [Google Scholar] [CrossRef]
- Smith, M.S.; Lawrence, V.; Sadler, E.; Easter, A. Barriers to accessing mental health services for women with perinatal mental illness: Systematic review and meta-synthesis of qualitative studies in the UK. BMJ Open 2019, 9, 1–9. [Google Scholar] [CrossRef]
- Sperlich, M.; Seng, J.S.; Li, Y.; Taylor, J.; Bradbury-Jones, C. Integrating Trauma-Informed Care Into Maternity Care Practice: Conceptual and Practical Issues. J. Midwifery Womens Health 2017, 62, 661–672. [Google Scholar] [CrossRef]
- Wang, P.S.; Angermeyer, M.; Borges, G.; Bruffaerts, R.; Chiu, W.T.; de Girolamo, G.; Fayyad, J.; Gureje, O.; Haro, J.M.; Huang, Y.; et al. Delay and failure in treatment seeking after first onset of mental disorders in the World Health Organization’s World Mental Health Survey Initiative. World Psychiatry 2007, 6, 177–185. [Google Scholar]
- Sareen, J.; Jagdeo, A.; Cox, B.J.; Clara, I.; ten Have, M.; Belik, S.L.; de Graaf, R.; Stein, M.B. Perceived barriers to mental health service utilization in the United States, Ontario, and the Netherlands. Psychiatr. Serv. 2007, 58, 357–364. [Google Scholar] [CrossRef]
- van Beljouw, I.; Verhaak, P.; Prins, M.; Cuijpers, P.; Penninx, B.; Bensing, J. Reasons and Determinants for Not Receiving Treatment for Common Mental Disorders. Psychiatr. Serv. 2010, 61, 250–257. [Google Scholar] [CrossRef]
- Fonagy, P.; Steele, M.; Steele, H.; Moran, G.S.; Higgitt, A.C. The Capacity for Understanding Mental States—The Reflective Self in Parent and Child and its Significance for Security of Attachment. Infant Ment. Health J. 1991, 12, 201–218. [Google Scholar] [CrossRef]
- Berthelot, N.; Ensink, K.; Bernazzani, O.; Normandin, L.; Luyten, P.; Fonagy, P. Intergenerational Transmission of Attachment in Abused and Neglected Mothers: The Role of Trauma-Specific Reflective Functionin. Infant Ment. Health J. 2015, 36, 200–212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rouhi, M.; Stirling, C.; Ayton, J.; Crisp, E.P. Women’s help-seeking behaviours within the first twelve months after childbirth: A systematic qualitative meta-aggregation review. Midwifery 2019, 72, 39–49. [Google Scholar] [CrossRef]
- Bayrampour, H.; McNeil, D.A.; Benzies, K.; Salmon, C.; Gelb, K.; Tough, S. A qualitative inquiry on pregnant women’s preferences for mental health screening. BMC Pregnancy Childbirth 2017, 17, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jarrett, P.M. Pregnant women’s experience of depression care. J. Ment. Health Train. 2016, 11, 33–47. [Google Scholar] [CrossRef]
- Dahlberg, K.; Dahlberg, H.; Nyström, M. Reflective Lifeworld Research, 2nd ed.; Studentlitteratur: Malmö, Sweden, 2008. [Google Scholar]
- Rauhala, L. Ihmiskäsitys ihmistyössä; Gaudeamus: Jyväskylä, Finland, 1983. [Google Scholar]
- Noblit, G.; Hare, R. Meta-Ethnography; Sage Publications Inc.: London, UK, 1988. [Google Scholar]
- France, E.F.; Cunningham, M.; Ring, N.; Uny, I.; Duncan, E.A.S.; Jepson, R.G.; Maxwell, M.; Roberts, R.J.; Turley, R.L.; Booth, A.; et al. Improving reporting of meta-ethnography: The eMERGe reporting guidance. Bmc Med Res. Methodol. 2019, 19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sandelowski, M.; Barroso, J. Handbook for Synthesizing Qualitative Research; Springer Publishing Company: New York, NY, USA, 2007. [Google Scholar]
- Bondas, T.; Hall, E. Challenges in approaching metasynthesis research. Qual. Health Res. 2007, 17, 113–121. [Google Scholar] [CrossRef] [PubMed]
- Bondas, T.; Hall, E. A decade of metasynthesis research in health sciences: A meta-method study. Int. J. Qual. Stud. Health Wellbeing 2007, 2, 101–113. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4. [Google Scholar] [CrossRef] [Green Version]
- Critical Appraisal Skills Programme. CASP (Qualitative) Checklist 2018. Available online: https://casp-uk.net/casp-tools-checklists/ (accessed on 20 January 2020).
- McCarthy, M.; McMahon, C. Acceptance and experience of treatment for postnatal depression in a community mental health setting. Health Care Women Int. 2008, 29, 618–637. [Google Scholar] [CrossRef] [PubMed]
- Raymond, N.C.; Pratt, R.J.; Godecker, A.; Harrison, P.A.; Kim, H.; Kuendig, J.; O’Brien, J.M. Addressing perinatal depression in a group of underserved urban women: A focus group study. BMC Pregnancy Childbirth 2014, 14, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bilszta, J.; Ericksen, J.; Buist, A.; Milgrom, J. Women’s experience of postnatal depression—Beliefs and attitudes as barriers to care. Aust. J. Adv. Nurs. 2010, 27, 44–54. [Google Scholar]
- Letourneau, N.; Duffett-Leger, L.; Stewart, M.; Hegadoren, K.; Dennis, C.-L.; Rinaldi, C.M.; Stoppard, J. Canadian Mothers ‘ Perceived Support Needs During Postpartum Depression. Jognn-J. Obstet. Gynecol. Neonatal Nurs. 2007, 36, 441–449. [Google Scholar] [CrossRef]
- Foulkes, M. Enablers and Barriers to Seeking Help for a Postpartum Mood Disorder. Jognn-J. Obstet. Gynecol. Neonatal Nurs. 2011, 40, 450–457. [Google Scholar] [CrossRef] [Green Version]
- Thomas, L.J.; Scharp, K.M.; Paxman, C.G. Stories of Postpartum Depression: Exploring Health Constructs and Help-Seeking in Mothers’ Talk. Women Health 2014, 53, 373–387. [Google Scholar] [CrossRef]
- Holopainen, D. The Experience of Seeking Help for Postnatal Depression. Aust. J. Adv. Nurs. 2002, 19, 39–44. [Google Scholar]
- Sword, W.; Busser, D.; Ganann, R.; McMillan, T.; Swinton, M. Women’s care-seeking experiences after referral for postpartum depression. Qual. Health Res. 2008, 18, 1161–1173. [Google Scholar] [CrossRef]
- Byatt, N.; Cox, L.; Moore Simas, T.A.; Kini, N.; Biebel, K.; Sankaran, P.; Swartz, H.A.; Weinreb, L. How Obstetric Settings Can Help Address Gaps in Psychiatric Care for Pregnant and Postpartum Women with Bipolar Disorder. Arch. Women’s Ment. Health 2018, 21, 543–551. [Google Scholar] [CrossRef]
- Guy, S.; Sterling, B.S.; Walker, L.O.; Harrison, T.C. Mental Health Literacy and Postpartum Depression: A Qualitative Description of Views of Lower Income Women. Arch. Psychiatr. Nurs. 2014, 28, 256–262. [Google Scholar] [CrossRef] [PubMed]
- Bell, L.; Feeley, N.; Hayton, B.; Zelkowitz, P.; Tait, M.; Desindes, S. Barriers and Facilitators to the Use of Mental Health Services by Women With Elevated Symptoms of Depression and Their Partners. Issues Ment. Health Nurs. 2016, 37, 651–659. [Google Scholar] [CrossRef] [PubMed]
- Viveiros, C.J.; Darling, E.K. Barriers and facilitators of accessing perinatal mental health services: The perspectives of women receiving continuity of care midwifery. Midwifery 2018, 65, 8–15. [Google Scholar] [CrossRef] [PubMed]
- Jesse, D.; Dolbier, C.; Blanchard, A. Barriers to seeking help and treatment suggestions for prenatal depressive symptoms: Focus groups with rural low-income women. Issues Ment. Health Nurs. 2008, 29, 3–19. [Google Scholar] [CrossRef] [PubMed]
- Vaillant, G.E. Positive mental health: Is there a cross-cultural definition? World Psychiatry 2012, 11, 93–99. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
{kind=link}
| Criteria Headings | Reporting Criteria | Page | |
|---|---|---|---|
| Phase 1 Selecting meta-ethnography and starting | 1. Rationale and context for the meta-ethnography | Describe the gap in research or knowledge to be filled by the meta-ethnography, and the wider context of the meta-ethnography | 1–3 |
| 2. Aim(s) of the meta-ethnography | Describe the meta-ethnography aim(s) | 3–4 | |
| 3. Focus of the meta-ethnography | Describe the meta-ethnography review question(s) (or objectives) | 3 | |
| 4. Rationale for using meta-ethnography | Explain why meta-ethnography was considered the most appropriate qualitative synthesis methodology | 3-4 | |
| Phase 2 Deciding what is relevant | 5. Search strategy | Describe the rationale for the literature search strategy | 5–7 |
| 6. Search processes | Describe how the literature searching was carried out and by whom | 6-7 | |
| 7. Selecting primary studies | Describe the process of study screening and selection, and who was involved | 6–7 | |
| 8. Outcome of study selection | Describe the results of study searches and screening | 6 | |
| Phase 3 Reading included studies | 9. Reading and data extraction approach | Describe the reading and data extraction method and processes | 15 |
| 10. Presenting characteristics of included studies | Describe characteristics of the included studies | 8–14, 15-16 | |
| Phase 4 Determining how studies are related | 11. Process for determining how studies are related | Describe the methods and processes for determining how the included studies are related:
| 15 |
| 12. Outcome of relating studies | Describe how studies relate to each other | 15 | |
| Phase 5 Translating studies into one another | 13. Process of translating studies | Describe the methods of translation:
| 15 |
| 14. Outcome of translation | Describe the interpretive findings of the translation | 15–22 | |
| Phase 6 Synthesizing translations | 15. Synthesis process | Describe the methods used to develop overarching concepts (“synthesized translations”) Describe how potential alternative interpretations or explanations were considered in the synthesis | 15–20 |
| 16. Outcome of synthesis process | Describe the new theory, conceptual framework, model, configuration, or interpretation of data developed from the synthesis | 21–22 | |
| Phase 7 Expressing the synthesis | 17. Summary of findings | Summarize the main interpretive findings of the translation and synthesis and compare them to existing literature | 22–23 |
| 18. Strengths, and limitations | Reflect on and describe the strengths and limitations of the synthesis:
| 23–24 | |
| 19. Recommendations and conclusions | Describe the implications of the synthesis | 22–24 | |
| Author(s), Year, Country | Aim/Objective | Participants | Psychological Distress and Inclusion | Setting | Data Collection, Method | Results | CASP Qualitative Evaluation |
|---|---|---|---|---|---|---|---|
| Bell, Feeley, Hayon, Zelkowitz, Tait et al. (2016) Canada | To explore perceived barriers and facilitators to the use of mental health services experienced by women and their partners. | 30 women, 32.5 years (average) | Postnatal depression, inclusion EPDS * 12 | Two hospitals providing tertiary care and mental health services | Interviews with couples Content analysis | Five principal barriers and facilitators: accessibility and proximity, appropriateness and fit, stigma, encouraged to seek help, and personal characteristics. | 20 |
| Bilszta, Ericksen, Buist and Milgrom (2010) Australia | To explore barriers to care by asking women who are experiencing postnatal depression (PND) and who have accessed treatment and support services; how they recognized and acknowledged their depression; how being depressed affected their ability to actively seek help; what sort of help they wanted and why and how the attitudes of health professionals, friends and family, and the general community influenced the type of treatment sought. | 37 women, 34 years (mean) | Postnatal depression, EPDS * 14 median, most participated in structured treatment program | Hospital outpatient postnatal depression programs, community based mutual support programs | Focus groups Interpretative phenomenology (Smith) | Findings suggest the lived experience of PND and associated attitudes and beliefs result in significant barriers to accessing help. Eight theme clusters were identified: expectations of motherhood; not coping and fear of failure; stigma and denial; poor mental health awareness and access; interpersonal support; baby management; help-seeking and treatment experiences and relationship with health professionals. | 13 |
| Byatt, Cox, Moore, Simas, Kini et al. (2018) United States | To elucidate in a sample: (1) the challenges associated with under-recognition of bipolar disorder in obstetric settings; (2) what barriers they face when trying to access psychiatric care; and (3) their perspectives regarding how obstetric practices can facilitate the identification of bipolar disorder in this population and connect women with mental health care. | 25 women, age 18–55 years | Bipolar disorder, inclusion EDPS * 10 and DSM-IV criteria for bipolar disorder I, II | Five obstetrics practices, tertiary care center | Mixed. Qualitative study interviews Qualitative study modified grounded theory with phenomenological emphasis | Participants want their obstetric practices to proactively screen for, discuss, and help them obtain mental health treatment. Most were unaware of their diagnosis. Self-blame, stigma, fear, and lack of support prevent women from seeking help. | 15 |
| Foulkes (2011) Canada | To explore the barriers and enablers identified by women experiencing a postpartum mood disorder (PPMD) that preclude and facilitate their help-seeking behaviors. | 10 women, age 32.5 (mean) | PPMD, inclusion with no preexisting psychiatric illness and a diagnosis of postpartum mood disorder | Well-baby clinics and a parent resource center | Interviews Grounded theory (Strauss and Corbin) | The core category of ‘‘having postpartum’’ captured the essence of women’s experiences in seeking help for a PPMD. Women identified four main stressors that contributed to their development of a PPMD, two barrier categories, and an enabler category that influenced their help-seeking behaviors. Through navigation of formal and informal help, women were able to begin to reclaim the mothering instincts they had lost to mental illness. | 19 |
| Guy, Sterling, Walker and Harrison (2014) United States | To use Jorm’s (2000) framework to understand mental health literacy in one sample of lower income women to share participants’ knowledge and beliefs about recognizing postpartum depressive symptoms and seeking help for these symptoms. | 25 women, 24.3 years (mean) | Postnatal depression, inclusion CES-D ** over 16 | Prenatal care through Medicaid | Focus groups Deductive analysis based on mental health literacy conceptual categories (Jorm), qualitative thematic analysis | Women recognized behavioral changes indicating mental distress, but fears prevented them from seeking help, and some resorted to risky behaviors. | 18 |
| Holopainen (2002) Australia | To explore women’s experiences of support and treatment for postnatal depression. | 7 women, age 24–43 years | Postnatal depression, inclusion current or recent perinatal depression | Postnatal support group in community health services, sexual assault center | Interviews Phenomenology (Creswell) | Women did not know where to seek help and were unaware of perinatal depression. Women were ambivalent of the use of medication. Women had ambivalent personal beliefs of being weak. Women wanted to be understood. Programs did not involve the family. | 20 |
| Jarrett (2015) United Kingdom | To explore women’s perspective of care from GPs and midwives, when they experience symptoms of depression during pregnancy. | 22 women, age not known | Prenatal depression, inclusion self-reported symptoms of depression | Internet discussion group for mental health during pregnancy | Online questions in two discussion forums Qualitative descriptive design (Neergaard), thematic analysis (Braun and Clarke) | Themes were identified from the data including women’s disclosure of symptoms to GP’s and midwives; lack of knowledge of perinatal mental health among health providers; attitudes of staff and systemic issues as barriers to good care; anti-depressant therapy and care that women found helpful. | 19 |
| Jesse, Dolbier, and Blanchard (2008) United States | To identify: (1) potential barriers to sharing depressive symptoms with health care providers, (2) suggestions about how health care providers can best help women with depressive symptoms overcome barriers to seeking care, and (3) feedback regarding prenatal interventions that might be helpful for low-income women with depressive symptoms or depression in pregnancy. | 21 women, all over 18 years | Prenatal depressive disorders, inclusion if assessed with high psychosocial risk in pregnancy | Prenatal clinic | Focus groups and two individual interviews Content analysis | Participants identified themes regarding barriers to seeking help. These were: (1) lack of trust, (2) judgment/stigma, (3) dissatisfaction with the health care system, and (4) not wanting help. Themes identified regarding overcoming barriers were: (1) facilitating trust and (2) offering support and help. | 17 |
| Letourneau, Duffett-Leger, Stewart, Hegadoren, Dennis et al. (2007) Canada | To assess the support needs, support resources, barriers to support, and preferences for support intervention for women with postpartum depression. | 52 women, 31.3 years (mean) | Postnatal depression, inclusion depressive symptoms within past 2 years, 12 weeks of delivery, for longer than 2 weeks | Settings within integrated mental health services and postpartum follow-up | Interviews, group interviews Thematic content analysis | For most mothers, one-on-one support was preferred when postpartum depression is recognized. Group support should be available once the mothers start to feel better and are able to comfortably interact with other mothers in a group format. | 15 |
| McCarthy and McMahon (2008) New Zealand | To investigate the acceptance and experience of treatment for postnatal depression. | 15 women, age 27–41 years | Postnatal depression, inclusion diagnosis of postnatal depression and in treatment since 3–12 months, with antidepressant medication | Community mental health setting | Interviews Grounded theory, “analytic induction method” (Glaser and Strauss) | The majority of women interviewed had reached “crisis point” before they sought and received treatment. The stigma attached to an inability to cope and being a “bad mother” emerged as the main barrier to seeking help earlier. In addition, women were unable to differentiate between “normal” levels of postpartum distress and depressive symptoms that might require intervention. Talking about their distress and experiences, both with health professionals and other mothers, was regarded as of primary importance in the recovery process. | 16 |
| Raymond, Pratt, Godecker, Harrisin, Kim et al. (2014) United States | To explore the following research objectives: What perceived needs do women describe they have in relation to their mental health through the perinatal period? What help do women describe current seeking in relation to addressing mental health concerns during the perinatal period? What support do women describe wanting for addressing mental health concerns during the perinatal period? | 37 women, 27.5 years (average) | Perinatal mental health needs, inclusion if receiving prenatal or postnatal care | Three healthcare clinics in disadvantaged parts of urban areas | Focus groups Thematic analysis, social constructivist version of grounded theory (Charmaz) | Thirteen themes emerged which were described in relation to mental health needs, help currently accessed and the type of support wanted. The themes included the various mental health needs including dealing with changing moods, depression, feelings of isolation, worrying and a sense of being burdened. Women described using a limited range of supports and help. Participants expressed a preference for mental health support that was empowerment focused in its orientation, including peer support. Women also described the compounding effect that social and economic stresses had on their mental health. | 19 |
| Sword, Busser, Ganann, McMillan and Swinton (2008) Canada | To explore care seeking among women after public health nurse referral for probable postpartum depression, including responses to being referred, specific factors that hindered or facilitated care seeking, experiences seeking care, and responses to interventions offered. | 18 women, 29.4 years (mean) | Postnatal depression, inclusion EPDS * 12 | Public health setting with early prevention | Interviews Socioecological framework of health services, conventional content analysis (Hsieh) | Women’s normalizing of symptoms, limited understanding of postpartum depression, waiting for symptom improvement, discomfort discussing mental health concerns, and fears deterred care seeking; symptom awareness and not feeling like oneself were facilitating influences. Family and friends sometimes hindered care seeking because they, too, normalized symptoms or had limited understanding of postpartum depression. Care seeking was facilitated when women encouraged a health professional visit or expressed worry and concern. | 18 |
| Thomas, Scharp and Paxman (2014) United States | What IM ***-derived constructs permeate mothers’ talk about the postpartum depression experience? | 30 women, age not known | Postnatal depression, inclusion if writing represents a woman’s 1st person account of her experiences | Online discussion group on postpartum depression | Anonymous online stories IM ***, inductive open coding; closed-coding procedure (Strauss and Corbin) | Five constructs (i.e., social norms; severity; barriers to help-seeking; facilitators to, and cues to action for, help-seeking; and self-efficacy) were prevalent. | 18 |
| Viveiros and Darling (2018) Canada | To explore access to PMH care services from a midwifery perspective: What do recipients of midwifery care perceive to be the factors that prevent or facilitate access to mental health care for women who experience depression, anxiety, and other mental health concerns in the perinatal period? | 16 women, all over 18 years | Perinatal mental health, inclusion if self-identification of mental health concerns | Midwifery care | Interviews, focus groups Deductive thematic analysis (Braun and Clarke) based on Levesque’s et al. framework on access to health care | Five salient themes emerged from the data: cultural values, knowledge, relationships, flexibility, and system gaps. Barriers and facilitators to accessing perinatal mental health services are grouped under each theme. Stigma and fear, broken referral pathways, distant service location, lack of number/capacity of specialized services, baby-centeredness, discharge from midwifery care at six weeks postpartum, and cost were barriers to accessing care. Information and midwives’ knowledge/experience were context-specific factors that could hinder or facilitate access. Continuity, community, and advocacy were facilitators to accessing care. | 19 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sorsa, M.A.; Kylmä, J.; Bondas, T.E. Contemplating Help-Seeking in Perinatal Psychological Distress—A Meta-Ethnography. Int. J. Environ. Res. Public Health 2021, 18, 5226. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18105226
Sorsa MA, Kylmä J, Bondas TE. Contemplating Help-Seeking in Perinatal Psychological Distress—A Meta-Ethnography. International Journal of Environmental Research and Public Health. 2021; 18(10):5226. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18105226
Chicago/Turabian StyleSorsa, Minna Anneli, Jari Kylmä, and Terese Elisabet Bondas. 2021. "Contemplating Help-Seeking in Perinatal Psychological Distress—A Meta-Ethnography" International Journal of Environmental Research and Public Health 18, no. 10: 5226. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18105226