
Willingness to Be Vaccinated against COVID-19 in Spain before the Start of Vaccination: A Cross-Sectional Study

 ,
,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design, Population, and Sample
2.2. Data-Collection Tool
2.3. The Dependent Variable
2.4. Methods of Analysis
2.5. Ethical Considerations
3. Results
3.1. Population Description
3.2. Variables with Influence on the Decision
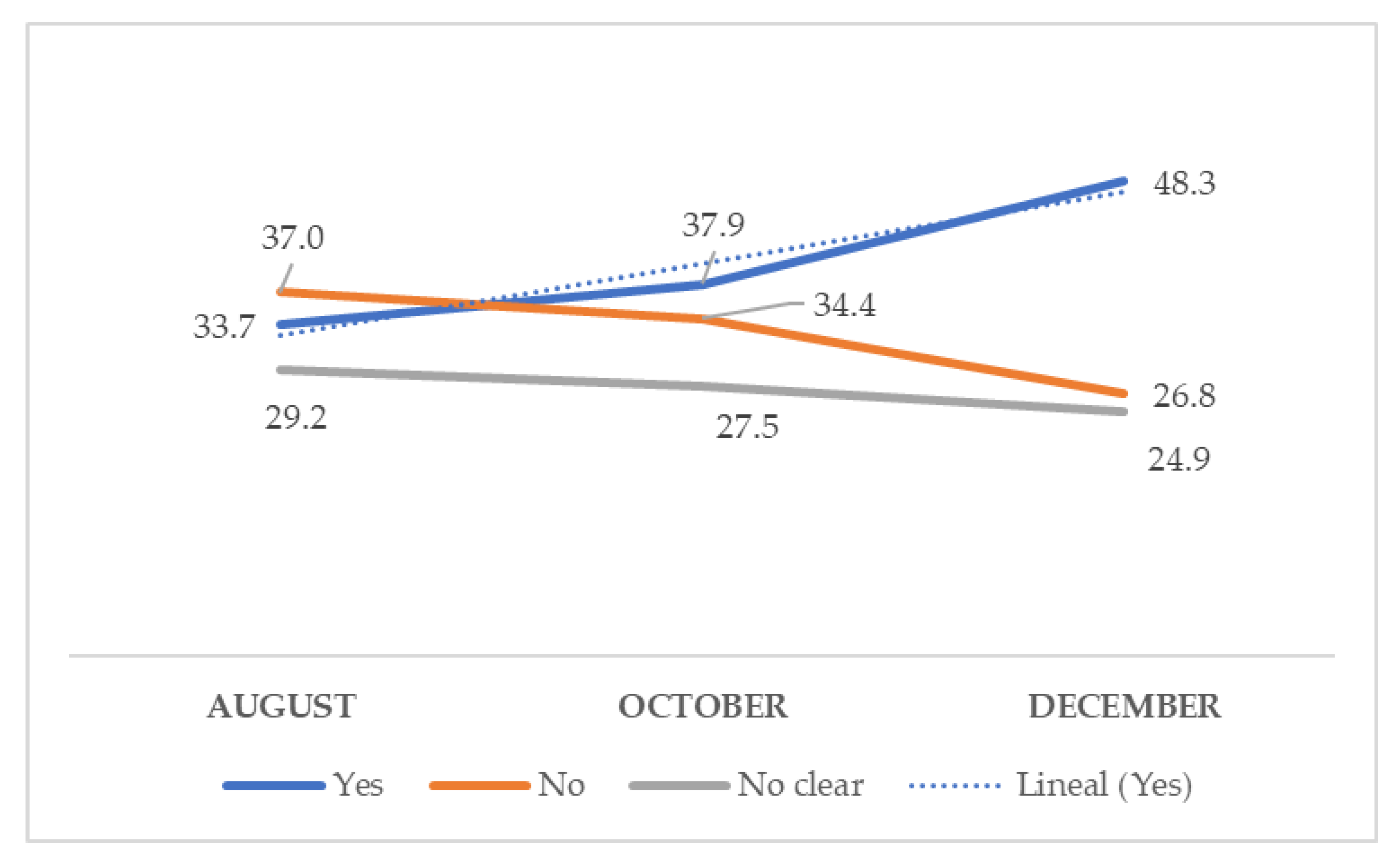
3.3. Acceptance, Rejection, or Hesitancy of the Vaccination through Time
3.4. Concerns and Sources of Information about the Vaccine
3.5. Multivariate Logistic Regression Analyses Showing Attitudes of the Participants as Factors Associated with Acceptance of a COVID-19 Vaccine in Spain
4. Discussion
4.1. Population: Vaccine Acceptance
4.2. Acceptance, Rejection or Vaccine Hesitancy through Time
4.3. Concerns and Sources of Vaccine-Related Information
4.4. A multivariate Logistic Regression Analysis Shows the Attitudes of the Participants as Factors Associated to COVID Vaccine Acceptance in Spain
4.5. Study Limitations
4.6. Practical Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Coronavirus: Worldometer. 2021. Available online: https://www.worldometers.info/coronavirus (accessed on 24 March 2021).
- Ministerio de Sanidad, Consumo y Bienestar Social—Profesionales—Estrategia de vacunación COVID-19 en España. 2020. Available online: https://www.mscbs.gob.es/profesionales/saludPublica/ccayes/alertasActual/nCov/vacunaCovid19.htm (accessed on 13 January 2021).
- González-Melado, F.J.; Di Pietro, M.L. The Vaccine Against COVID-19 and Institutional Trust. Enferm. Infecc. Microbiol. Clin. 2020. [Google Scholar] [CrossRef]
- Li, Q.; Tang, B.; Bragazzi, N.L.; Xiao, Y.; Wu, J. Modeling the Impact of Mass Influenza Vaccination and Public Health Interventions on COVID-19 Epidemics with Limited Detection Capability. Math. Biosci. 2020, 325, 108378. [Google Scholar] [CrossRef] [PubMed]
- Lane, S.; MacDonald, N.E.; Marti, M.; Dumolard, L. Vaccine Hesitancy around the Globe: Analysis of Three Years of WHO/UNICEF Joint Reporting Form Data-2015–2017. Vaccine 2018, 36, 3861–3867. [Google Scholar] [CrossRef] [PubMed]
- Schwarzinger, M.; Flicoteaux, R.; Cortarenoda, S.; Obadia, Y.; Moatti, J.-P. Low Acceptability of A/H1N1 Pandemic Vaccination in French Adult Population: Did Public Health Policy Fuel Public Dissonance? PLoS ONE 2010, 5, e10199. [Google Scholar] [CrossRef]
- Raude, J.; Caille-Brillet, A.-L.; Setbon, M. The 2009 Pandemic H1N1 Influenza Vaccination in France: Who Accepted to Receive the Vaccine and Why? PLoS Curr. 2010, 2, RRN1188. [Google Scholar] [CrossRef] [PubMed]
- Bone, A.; Guthmann, J.-P.; Nicolau, J.; Lévy-Bruhl, D. Population and Risk Group Uptake of H1N1 Influenza Vaccine in Mainland France 2009–2010: Results of a National Vaccination Campaign. Vaccine 2010, 28, 8157–8161. [Google Scholar] [CrossRef]
- French, J.; Deshpande, S.; Evans, W.; Obregon, R. Key Guidelines in Developing a Pre-Emptive COVID-19 Vaccination Uptake Promotion Strategy. Int. J. Environ. Res. Public Health 2020, 17, 5893. [Google Scholar] [CrossRef]
- Kennedy, J. Populist Politics and Vaccine Hesitancy in Western Europe: An Analysis of National-Level Data. Eur. J. Public Health 2019, 29, 512–516. [Google Scholar] [CrossRef]
- Lasco, G. Medical Populism and the COVID-19 Pandemic. Glob. Public Health 2020, 15, 1417–1429. [Google Scholar] [CrossRef]
- World Health Organization. The Guide to Tailoring Immunization Programs; World Health Organisation: Geneva, Switzerland, 2014. [Google Scholar]
- Rodríguez-Blanco, N.; Tuells, J.; Vila-Candel, R.; Nolasco, A. Adherence and Concordance of Influenza and Pertussis Vaccination Coverage in Pregnant Women in Spain. Int. J. Environ. Res. Public Health 2019, 16, 543. [Google Scholar] [CrossRef] [Green Version]
- Iserson, K.V. SARS-CoV-2 (COVID-19) Vaccine Development and Production: An Ethical Way Forward. Camb. Q. Healthc. Ethics 2021, 30, 59–68. [Google Scholar] [CrossRef] [PubMed]
- Aschwanden, C. Five Reasons Why COVID Herd Immunity is Probably Impossible. Nature 2021, 591, 520–522. [Google Scholar] [CrossRef] [PubMed]
- Lazarus, J.V.; Ratzan, S.C.; Palayew, A.; Gostin, L.O.; Larson, H.J.; Rabin, K.; Kimball, S.; El-Mohandes, A. A Global Survey of Potential Acceptance of a COVID-19 Vaccine. Nat. Med. 2020, 27, 225–228. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Jing, R.; Lai, X.; Zhang, H.; Lyu, Y.; Knoll, M.D.; Fang, H. Acceptance of COVID-19 Vaccination during the COVID-19 Pandemic in China. Vaccines 2020, 8, 482. [Google Scholar] [CrossRef] [PubMed]
- Salali, G.D.; Uysal, M.S. COVID-19 Vaccine Hesitancy is Associated with Beliefs on the Origin of the Novel Coronavirus in the UK and Turkey. Psychol. Med. 2020, 19, 1–3. [Google Scholar]
- Malik, A.A.; McFadden, S.M.; Elharake, J.; Omer, S.B. Determinants of COVID-19 Vaccine Acceptance in the US. E Clin. Med. 2020, 26, 100495. [Google Scholar]
- Eguia, H.; Vinciarelli, F.; Bosque-Prous, M.; Kristensen, T.; Saigí-Rubió, F. Spain’s Hesitation at the Gates of a COVID-19 Vaccine. Vaccines 2021, 9, 170. [Google Scholar] [CrossRef] [PubMed]
- Ministerio de Sanidad, Consumo y Bienestar Social. Gobierno de España. Available online: https://www.mscbs.gob.es/gabinetePrensa/notaPrensa/pdf/24.11241120144431769.pdf (accessed on 15 January 2021).
- Instituto Nacional de Estadística (INE). Available online: https://www.ine.es/dyngs/INEbase/es/operacion.htm?c=Estadistica_C&cid=1254736176951&menu=ultiDatos&idp=1254735572981 (accessed on 15 November 2020).
- Sample Size Calculator SurveyMonkey. Available online: https://es.surveymonkey.com/mp/sample-size-calculator (accessed on 15 November 2020).
- Larson, H.J.; Jarrett, C.; Eckersberger, E.; Smith, D.M.D.; Paterson, P. Understanding Vaccine Hesitancy around Vaccines and Vaccination from a Global Perspective: A Systematic Review of Published Literature, 2007–2012. Vaccine 2014, 32, 2150–2159. [Google Scholar] [CrossRef]
- Reiter, P.L.; Pennell, M.L.; Katz, M.L. Acceptability of a COVID-19 Vaccine Among Adults in the United States: How Many People would get Vaccinated? Vaccine 2020, 38, 6500–6507. [Google Scholar] [CrossRef]
- Glanville, D. Treatments and Vaccines for COVID-19: Authorised Medicines; European Medicines Agency: Amsterdam, The Netherlands. Available online: https://www.ema.europa.eu/en/human-regulatory/overview/public-health-threats/coronavirus-disease-covid-19/treatments-vaccines/treatments-vaccines-covid-19-authorised-medicines (accessed on 19 January 2021).
- World Health Organization. A Global Framework to Ensure Equitable and Fair Allocation of COVID-19 Products. WHO Member States Briefing. 2020. Available online: https://www.who.int/docs/default-source/coronaviruse/who-covid19-vaccine-allocation-final-working-version-9sept.pdf (accessed on 7 January 2021).
- Bell, B.P.; Romero, J.R.; Lee, G.M. Scientific and Ethical Principles Underlying Recommendations From the Advisory Committee on Immunization Practices for COVID-19 Vaccination Implementation. JAMA 2020, 324, 2025–2026. [Google Scholar] [CrossRef]
- NORC at The University of Chicago. Expectations for a COVID-19 Vaccine; The Associated Press and NORC: Chicago, IL, USA, 2020; Available online: https://apnorc.org/projects/expectations-for-a-covid-19-vaccine (accessed on 13 January 2021).
- The COCONEL Group. A Future Vaccination Campaign against COVID-19 at Risk of Vaccine Hesitancy and Politicisation. Lancet Infect. Dis. 2020, 20, 769–770. [Google Scholar] [CrossRef]
- Neumann-Böhme, S.; Varghese, N.E.; Sabat, I.; Barros, P.P.; Brouwer, W.; van Exel, J.; Schreyögg, J.; Stargardt, T. Once we have it, will We use it? A European Survey on Willingness to be Vaccinated against COVID-19. Eur. J. Health Econ. 2020, 21, 977–982. [Google Scholar] [CrossRef]
- Al Ahdab, S. A Cross-Sectional Survey of Knowledge, Attitude and Practice (KAP) towards COVID-19 Pandemic among the Syrian Residents. BMC Public Health 2021, 21, 296. [Google Scholar] [CrossRef] [PubMed]
- Dodd, R.H.; Cvejic, E.; Bonner, C.; Pickles, K.; McCaffery, K.J.; Sydney Health Literacy Lab COVID-19 Group. Willingness to Vaccinate against COVID-19 in Australia. Lancet Infect. Dis. 2020, 21, 318–319. [Google Scholar] [CrossRef]
- Danchin, M.; Biezen, R.; Manski-Nankervis, J.A.; Kaufman, J.; Leask, J. Preparing the public for COVID-19 Vaccines: How can General Practitioners Build Vaccine Confidence and Optimise Uptake for Themselves and their Patients? Aust. J. Gen. Pract. 2020, 49, 625–629. [Google Scholar] [CrossRef] [PubMed]
- McAteer, J.; Yildirim, I.; Chahroudi, A. The VACCINES Act: Deciphering Vaccine Hesitancy in the Time of COVID-19. Clin. Infect. Dis. 2020, 71, 703–705. [Google Scholar] [CrossRef]
- Böhm, R.; Meier, N.W.; Groß, M.; Korn, L.; Betsch, C. The Willingness to Vaccinate Increases when Vaccination Protects others who have Low Responsibility for not being Vaccinated. J. Behav. Med. 2019, 42, 381–391. [Google Scholar] [CrossRef]
- Paul, E.; Steptoe, A.; Fancourt, D. Attitudes towards Vaccines and Intention to Vaccinate against COVID-19: Implications for Public Health Communications. Lancet Reg. Health—Eur. 2021, 1, 100012. [Google Scholar] [CrossRef]
- Kourlaba, G.; Kourkouni, E.; Maistreli, S.; Tsopela, C.G.; Molocha, N.M.; Triantafyllou, C.; Koniordou, M.; Kopsidas, I.; Chorianopoulou, E.; Maroudi-Manta, S.; et al. Willingness of Greek General Population to get a COVID-19 Vaccine. Glob. Health Res. Policy 2021, 6, 3. [Google Scholar] [CrossRef]
- Akarsu, B.; Canbay Özdemir, D.; Ayhan Baser, D.; Aksoy, H.; Fidancý, Ý.; Cankurtaran, M. While Studies on COVID-19 Vaccine is Ongoing, the Public’s Thoughts and Attitudes to the Future COVID-19 Vaccine. Int. J. Clin. Pract. 2020, 75, e13891. [Google Scholar]
- Prati, G. Intention to Receive a Vaccine Against SARS-CoV-2 in Italy and its Association with Trust, Worry and Beliefs about the Origin of the Virus. Health Educ. Res. 2020, 35, 505–511. [Google Scholar] [CrossRef] [PubMed]
- Nayar, R.K.; Nair, A.T.; Shaffi, M.; Swarnam, K.; Kumar, A.; Abraham, M.; Lordson, J.; Grace, C. Methods to Overcome Vaccine Hesitancy. Lancet Lond. Engl. 2019, 393, 1203–1204. [Google Scholar] [CrossRef] [Green Version]
- Ervasti, H.; Kouvo, A.; Venetoklis, T. Social and Institutional Trust in Times of Crisis: Greece, 2002–2011. Soc. Indic. Res. Int Interdiscip. J. Qual.—Life Meas. 2019, 141, 1207–1231. [Google Scholar] [CrossRef] [Green Version]
- Ward, J.K. Rethinking the Antivaccine Movement Concept: A Case Study of Public Criticism of the Swine Flu Vaccine’s Safety in France. Soc. Sci. Med. 2016, 159, 48–57. [Google Scholar] [CrossRef] [PubMed]
- Fontanet, A.; Cauchemez, S. COVID-19 Herd Immunity: Where are We? Nat. Rev. Immunol. 2020, 20, 583–584. [Google Scholar] [CrossRef] [PubMed]
- Hotez, P.J. COVID19 meets the Antivaccine Movement. Microbes Infect. 2020, 22, 162–164. [Google Scholar] [CrossRef] [PubMed]
- Yaqub, O.; Castle-Clarke, S.; Sevdalis, N.; Chataway, J. Attitudes to Vaccination: A Critical Review. Soc. Sci. Med. 2014, 112, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kata, A. A Postmodern Pandora’s Box: Anti-Vaccination Misinformation on the Internet. Vaccine 2010, 28, 1709–1716. [Google Scholar] [CrossRef]
- Sniehotta, F.F.; Scholz, U.; Schwarzer, R. Bridging the Intention-Behaviour Gap: Planning, Self-Efficacy, and Action Control in the Adoption and Maintenance of Physical Exercise. Psychol. Health 2005, 20, 143–160. [Google Scholar] [CrossRef]
- Preparing for the Vaccine. Nat. Biotechnol. 2020, 38, 1219. [CrossRef]
- Nayar, R.K.; Nair, A.T.; Shaffi, M.; Swarnam, K.; Kumar, A.; Abraham, M.; Lordson, J.; Grace, C. Looking beyond the Decade of Vaccines. Lancet 2018, 392, 2139. [Google Scholar]
- Sultana, J.; Mazzaglia, G.; Luxi, N.; Cancellieri, A.; Capuano, A.; Ferrajolo, C.; de Waure, C.; Ferlazzo, G.; Trifirò, G. Potential Effects of Vaccinations on the Prevention of COVID-19: Rationale, Clinical Evidence, Risks, and Public Health Considerations. Expert Rev. Vaccines 2020, 19, 919–936. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable (n) | Accept | Rejection | Hesitation | ||||
|---|---|---|---|---|---|---|---|
| n (%) | n (%) | OR (95% CI) | p-Value | n (%) | OR (95% CI) | p-Value | |
| Gender (2494) | |||||||
| Male (R) | 396 (55.9) | 164 (23.2) | 1 | <0.001 | 148 (23.9) | 1 | 0.001 |
| Female | 809 (45.3) | 506 (28.3) | 1.51 (1.22–1.87) | 471 (26.4) | 1.55 (1.25–1.94) | ||
| Civil status (2494) | |||||||
| Couple (R) | 802 (51.5) | 388 (24.9) | 1 | 0.001 | 366 (23.5) | 1 | 0.02 |
| Single | 316 (43.9) | 217 (30.1) | 1.42 (1.15–1.75) | 0.043 | 187 (26.0) | 1.30 (1.04–1.61) | 0.011 |
| Divorced | 88 (41.5) | 61 (28.8) | 1.43 (1.01–2.03) | 63 (29.7) | 1.57 (1.11–2.22) | ||
| Age group (2412) | |||||||
| 18–29 (R) | 289 (45.5) | 182 (28.7) | 1 | 1 | 164 (25.8) | 1 | 1 |
| 30–39 | 206 (44.9) | 134 (29.2) | 1.03 (0.78–1.38) | 0.824 | 119 (25.9) | 1.02(0.76–1.37) | 0.906 |
| 40–49 | 368 (49.5) | 200 (30.7) | 0.86 (0.67–1.11) | 0.254 | 176 (23.7) | 0.84 (0.65–1.10) | 0.202 |
| 50–59 | 178 (47.7) | 99 (15.2) | 0.88 (0.65–1.20) | 0.429 | 96 (25.7) | 0.95 (0.67–1.30) | 0.750 |
| >60 | 119 (59.2) | 36 (17.9) | 0.48 (0.32–0.73) | 0.001 | 46 (7.7) | 0.68 (0.46–1.00) | 0.054 |
| Employment (2461) | |||||||
| Worker (R) | 909 (50.2) | 486 (26.8) | 1 | 1 | 416 (23.0) | 1 | 1 |
| Unemployed | 30 (39.5) | 20 (26.3) | 1.25 (0.70–2.22) | 0.453 | 26 (34.2) | 1.89 (1.11–3.24) | 0.020 |
| Retired | 71 (55.5) | 20 (15.6) | 0.53 (0.32–0.88) | 0.013 | 37 (28.9) | 1.14 (0.75–1.72) | 0.539 |
| Student | 186 (41.7) | 131 (29.4) | 1.32 (1.03–1.69) | 0.03 | 129 (28.9) | 1.51 (1.18–1.95) | 0.001 |
| Type of work (1811) | |||||||
| Health (R) | 363 (52.0) | 179 (25.6) | 1 | 1 | 156 (22.3) | 1 | 1 |
| Humanities | 130 (508) | 71 (27.7) | 1.11 (0.79–1.56) | 0.556 | 55 (51.5) | 0.98 (0.68–1.42) | 0.933 |
| Social | 161 (45.9) | 106 (30.2) | 1.34 (0.99–1.81) | 0.062 | 84 (23.9) | 1.20 (0.88–1.68) | 0.240 |
| Services | 197 (49.0) | 104 (25.9) | 1.07 (0.80–1.44) | 0.653 | 101 (25.1) | 1.19 (0.88–1.62) | 0.256 |
| Others | 58 (55.8) | 26 (25.0) | 0.91 (0.55–1.49) | 0.706 | 20 (19.2) | 0.80 (0.47–1.38) | 0.426 |
| Level of study (2483) | |||||||
| University (R) | 761 (51.7) | 374 (25.4) | 1 | 1 | 336 (22.8) | 1 | 1 |
| Vocational training | 135 (38.2) | 130 (36.8) | 1.96 (1.50–2.57) | <0.001 | 88 (24.9) | 1.48 (1.10–2.00) | 0.010 |
| A-level degree | 156 (43.6) | 94 (26.3) | 1.23 (0.92–0.162) | 0.160 | 108 (30.2) | 1.57 (1.19–2.01) | 0.001 |
| High school | 147 (48.8) | 65 (21.6) | 0.90 (0.66–1.23) | 0.514 | 89 (29.6) | 1.37 (1.02–1.84) | 0.035 |
| Economic status (2487) | |||||||
| Medium (R) | 802 (50.9) | 383 (24.3) | 1 | 1 | 392 (24.9) | 1 | 1 |
| Low | 28 (38.9) | 29 (40.3) | 2.17 (1.27–3.70) | 0.004 | 15 (20.8) | 1.10 (0.58–2.01) | 0.78 |
| Low/Medium | 211 (44.4) | 137 (28.8) | 1.36 (1.06–1.74) | 0.015 | 127 (26.7) | 1.23 (0.96–1.58) | 0.10 |
| Medium/High | 159 (44.9) | 112 (31.6) | 1.47 (1.12–1.93) | 0.005 | 83 (23.4) | 1.07 (0.80–1.43) | 0.66 |
| High | 5 (55.6) | 4 (44.4) | 1.68 (0.45–6.27) | 0.444 | 0 (0) | - | |
| Religion (2456) | |||||||
| Christian (R) | 651 (46.8) | 371 (26.7) | 1 | 1 | 369 (26.5) | 1 | 1 |
| None | 533 (51.0) | 276 (26.4) | 0.91 (0.75–1.10) | 0.331 | 237 (22.7) | 0.78 (0.64–0.96) | 0.017 |
| Others | 6 (31.6) | 6 (31.6) | 1.76 (0.56–5.48) | 0.333 | 7 (36.8) | 2.058 (0.69–6.17) | 0.198 |
| Political inclination (2303) | |||||||
| Right (R) | 232 (39.4) | 202 (34.3) | 1 | 1 | 155 (26.3) | 1 | 1 |
| Center | 389 (47.3) | 210 (25.5) | 0.62 (0.48–0.80) | <0.001 | 224 (27.2) | 0.86 (0.66–1.12) | 0.265 |
| Left | 534 (59.9) | 171 (19.2) | 0.37 (0.29–0.48) | <0.001 | 186 (20.9) | 0.52 (0.40–0.68) | 0.001 |
| What Do You Think May be the Main Problem(s) that Leads to Doubts against Becoming Vaccinated with Covid-19 when the Vaccine Becomes Available? | |
| Misinformation about the side effects that the vaccine may have | 1757 (70.9) |
| How quickly its creation has taken place | 1293 (52.2) |
| The variety of information from different media | 693 (28.0) |
| That there are social agents of recognized prestige who doubt the vaccine | 627 (25.3) |
| Lack of consensus among political leaders in developing vaccination policies | 377 (15.2) |
| There is no factor that raises doubts | 35 (1.4) |
| From what sources do you collect information regarding the Covid-19 vaccine? | |
| Written or digital press | 1226 (49.5) |
| Television or radio | 949 (38.3) |
| Social media | 638 (25.8) |
| Official pages of health-related organizations and associations and medical bibliographic bases | 499 (20.1) |
| Google-type search engines | 458 (18.5) |
| No | 9 (0.4) |
| Which of the following social agents do you trust the most? | |
| Health | 2295 (91.8) |
| Spiritual leaders | 35 (1.4) |
| Journalists | 11 (0.4) |
| Political | 10 (0.4) |
| Other | 15 (0.6) |
| None at all | 99 (4.0) |
| Not clear | 14 (0.6) |
| No answer provided | 22 (0.9) |
| If the social agent you have selected recommends that you get the COVID-19 vaccine when it is ready, will you do it? | |
| Yes | 1555 (62.5) |
| No | 329 (13.2) |
| Not clear | 606 (24.3) |
| Variable (n) | Accept | Rejection | Hesitation | ||||
|---|---|---|---|---|---|---|---|
| n (%) | n (%) | OR (95% CI) | p-Value | n (%) | OR (95% CI) | p-Value | |
| In the case that you have children, will you receive the COVID-19 vaccine when it becomes available? (2324) | |||||||
| No (R) | 44 (6.1) | 580 (79.8) | 1 | 103 (14.2) | 1 | ||
| Yes | 846 (96.1) | 11 (1.2) | 0.001 (0.001–0.02) | <0.001 | 24 (2.7) | 0.01 (0.01–0.02) | <0.001 |
| Not clear | 220 (30.7) | 49 (6.8) | 0.02 (0.01–0.03) | <0.001 | 447 (62.4) | 0.87 (0.49–1.23) | 0.475 |
| Do you usually receive the vaccine against the flu? (2495) | |||||||
| No (R) | 529 (38.1) | 501 (36.1) | 1 | 359 (25.8) | 1 | ||
| Yes | 501 (63.2) | 115 (14.5) | 0.24 (0.19–0.31) | <0.001 | 177 (22.3) | 0.52 (0.42–0.65) | <0.001 |
| Occasionally | 172 (55.0) | 60 (19.2) | 0.37 (0.27–0.51) | <0.001 | 81 (25.9) | 0.70 (0.52–0.93) | 0.016 |
| Do you believe that, without vaccines, the population would suffer more diseases, such as measles, chickenpox, etc.? (2499) | |||||||
| No (R) | 26 (22.6) | 77 (67.0) | 1 | 12 (10.4) | 1 | ||
| Yes | 1158 (51.5) | 530 (23.6) | 0.16 (0.10–0.24) | <0.001 | 562 (25.0) | 1.05 (0.53–2.10) | 0.887 |
| Not clear | 19 (14.2) | 70 (52.2) | 1.24 (0.63–2.44) | 0.526 | 45 (33.6) | 5.13 (2.15–12.2) | <0.001 |
| Do you believe that vaccines can cause more diseases that they intend to prevent? (2500) | |||||||
| No (R) | 906 (58.9) | 307 (20.0) | 1 | 325 (21.1) | 1 | ||
| Yes | 113 (26.3) | 202 (47.1) | 5.28 (4.05–6.87) | <0.001 | 114 (26.6) | 2.81 (2.11–3.76) | <0.001 |
| Not clear | 186 (34.9) | 168 (31.5) | 2.67 (2.09–3.41) | <0.001 | 179 (33.6) | 2.68 (2.11–3.42) | <0.001 |
| In the case that you have children, do they have the vaccination calendar up to date? (2389) | |||||||
| No (R) | 6 (20.0) | 20 (66.7) | 1 | 4 (13.3) | 1 | ||
| Yes | 702 (49.9) | 361 (25.5) | 0.15 (0.06–0.39) | <0.001 | 354 (25.0) | 0.76 (0.21–2.70) | 0.667 |
| Not clear | 2 (18.2) | 3 (27.3) | 0.45 (0.06–3.35) | 0.436 | 6 (54.5) | 4.5 (0.59–34.6) | 0.148 |
| Not children | 442 (47.5) | 264 (28.4) | 0.18 (0.71–0.45) | <0.001 | 225 (24.2) | 0.76 (0.21–2.73) | 0.678 |
| Variable | Accept | Rejection | Hesitation | ||||
|---|---|---|---|---|---|---|---|
| n (%) | n (%) | OR (95% CI) | p-Value | n (%) | OR (95% CI) | p-Value | |
| Cancer | |||||||
| No | 1189 (48.8) | 651 (26.7) | 0.46 (0.14–1.50) | 0.196 | 594 (24.4) | 0.21 (0.07–0.59) | 0.003 |
| Yes (R) | 5 (21.7) | 6 (26.1) | 1 | 12 (52.2) | 1 | ||
| Respiratory disease | |||||||
| No | 1121 (47.8) | 627 (26.7) | 0.46 (0.14–1.5) | 0.456 | 597 (25.5) | 4.35 (2.15–8.80) | 0.001 |
| Yes (R) | 73 (65.2) | 30 (26.8) | 1 | 9 (8.0) | 1 | ||
| Diabetes | |||||||
| No | 1156 (48.3) | 643 (26.9) | 1.51 (0.81–2.80) | 0.193 | 591 (24.8) | 1.62 (0.84–3.14) | 0.146 |
| Yes (R) | 38 (59.4) | 14 (21.9) | 1 | 12 (18.8) | 1 | ||
| Cardiac disease | |||||||
| No | 1170 (48.5) | 647 (26.8) | 1.33 (0.63–2.79) | 0.456 | 593 (24.6) | 0.94 (0.47–1.85) | 0.936 |
| Yes (R) | 24 (51.1) | 10 (21.3) | 1 | 13 (27.7) | 1 | ||
| Liver disease | |||||||
| No | 1187 (48.5) | 655 (26.8) | 1.93 (0.40–9.32) | 0.413 | 606 (24.8) | - | - |
| Yes (R) | 7 (77.8) | 2 (22.2) | 1 | 0 (0.0) | 1 | ||
| Renal disease | |||||||
| No | 1190 (48.7) | 654 26.8) | 0.73 (0.16–3.28) | 0.685 | 600 (24.5) | 0.34 (0.09–1.20) | 0.092 |
| Yes (R) | 4 (30.8) | 3 (23.1) | 1 | 6 (46.2) | 1 | ||
| Hypercholesterolemia | |||||||
| No | 1122 (48.1) | 629 (26.9) | 1.44 (0.92–2.26) | 0.109 | 584 (25.0) | 1.70 (1.05–2.78) | 0.032 |
| Yes (R) | 72 (59.0) | 28 (23.0) | 1 | 22 (18.0) | 1 | ||
| Immunodepression | |||||||
| No | 1162 (48.3) | 651 (27.0) | 2.99 (1.24–7.18) | 0.014 | 595 (24.7) | 1.49 (0.75–2.98) | 0.259 |
| Yes (R) | 32 (65.3) | 6 (12.2) | 1 | 11 (22.4) | 1 | ||
| Overweightness | |||||||
| No | 995 (47.3) | 583 (27.7) | 1.58 (1.18–2.10) | 0.002 | 524 (24.9) | 1.28 (0.97–1.69) | 0.084 |
| Yes (R) | 199 (56.1) | 74 (20.8) | 1 | 82 (23.1) | 1 | ||
| Hypertension | |||||||
| No | 1081 (48.0) | 619 (27.5) | 1.70 (1.16–2.49) | 0.006 | 553 (24.5) | 1.09 (0.78–1.54) | 0.619 |
| Yes (R) | 113 (55.4) | 38 (18.6) | 1 | 53 (26.0) | 1 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodríguez-Blanco, N.; Montero-Navarro, S.; Botella-Rico, J.M.; Felipe-Gómez, A.J.; Sánchez-Más, J.; Tuells, J. Willingness to Be Vaccinated against COVID-19 in Spain before the Start of Vaccination: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 5272. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18105272
Rodríguez-Blanco N, Montero-Navarro S, Botella-Rico JM, Felipe-Gómez AJ, Sánchez-Más J, Tuells J. Willingness to Be Vaccinated against COVID-19 in Spain before the Start of Vaccination: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2021; 18(10):5272. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18105272
Chicago/Turabian StyleRodríguez-Blanco, Noelia, Sergio Montero-Navarro, José M. Botella-Rico, Antonio J. Felipe-Gómez, Jesús Sánchez-Más, and José Tuells. 2021. "Willingness to Be Vaccinated against COVID-19 in Spain before the Start of Vaccination: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 18, no. 10: 5272. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18105272