
“Moving for My Baby!” Motivators and Perceived Barriers to Facilitate Readiness for Physical Activity during Pregnancy among Obese and Overweight Women of Urban Areas in Northern Taiwan


Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Participants
2.2. Focus Group Interviews
2.3. Data Analysis
3. Results
3.1. Demographics
3.2. Perceptions of and Readiness for Being Active
3.3. Motivations to Move for Unborn Babies
3.4. Multiple Barriers to Engage in PA
3.5. Preference of PA Advice from Obstetricians and Strategies for the Overweight and Obese
3.6. Peer Support during Focus Group
4. Discussion
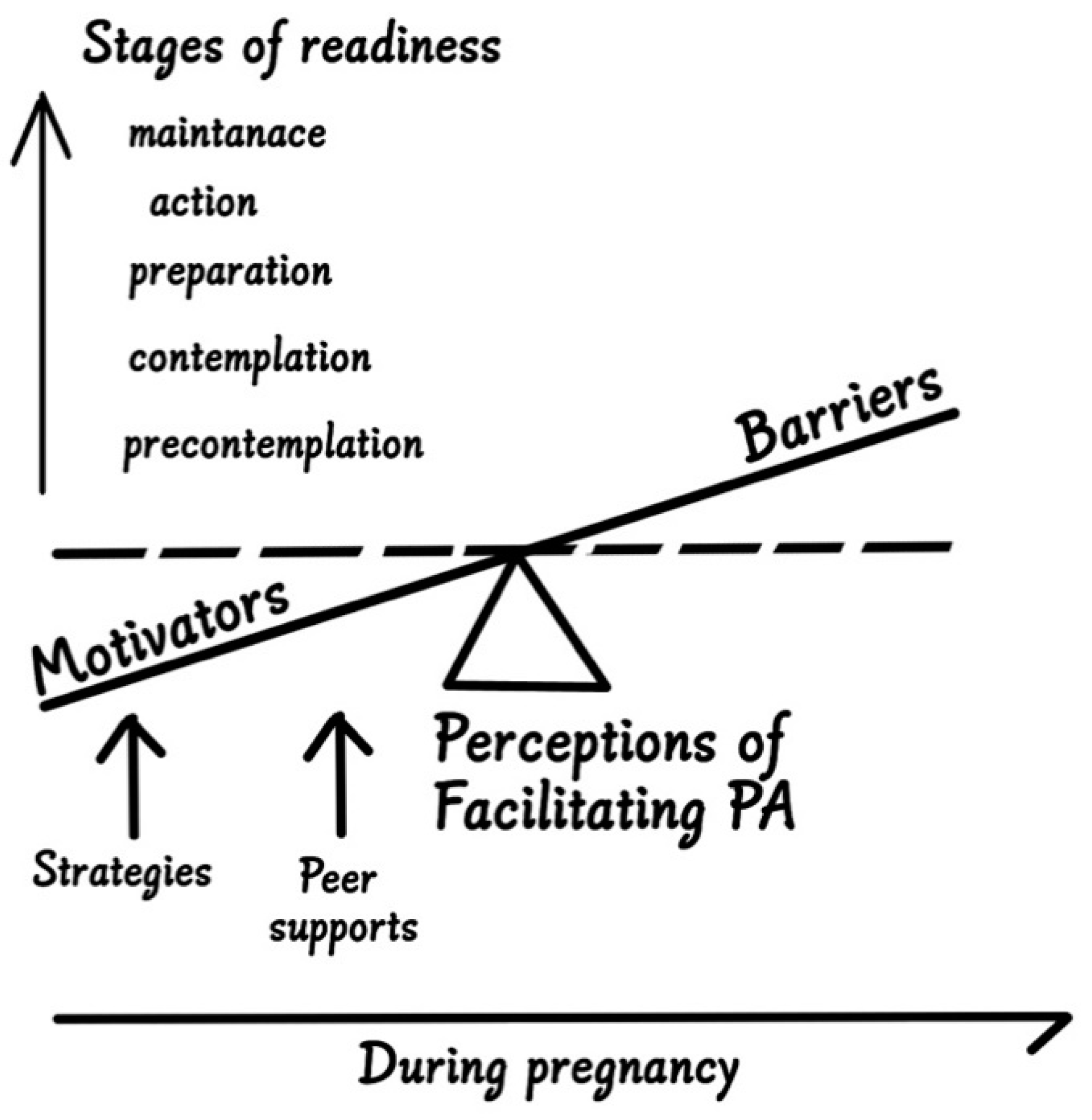
4.1. A Theoretical Basis of Perceptions and Readiness Stages for PA
4.2. Readiness for PA Engagement
4.3. Facilitating PA for Obese and Overweight Pregnant Women in Taiwan
4.3.1. Increase Motivations
4.3.2. Overcome Barriers
4.3.3. Strategies to Facilitate PA Readiness in Taiwan
4.4. Emotional Support during Focus Groups
4.5. Strengths and Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chan, H.-L.; Li, I.-F.; Tseng, L.-C.; Hsiung, Y. Exploring Behavioral Readiness and Program Strategies to Engage Older Community Residents in Advance Care Planning: A Pilot Mixed-Method Study in Taiwan. Int. J. Environ. Res. Public Health 2020, 17, 4285. [Google Scholar] [CrossRef]
- Flannery, C.; Fredrix, M.; Olander, E.K.; McAuliffe, F.M.; Byrne, M.; Kearney, P.M. Effectiveness of physical activity interventions for overweight and obesity during pregnancy: A systematic review of the content of behaviour change interventions. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 1–20. [Google Scholar] [CrossRef] [Green Version]
- Cedergren, M.I. Maternal morbid obesity and the risk of adverse pregnancy outcome. Obstet. Gynecol. 2004, 103, 219–224. [Google Scholar] [CrossRef] [PubMed]
- Lewandowska, M.; Więckowska, B.; Sajdak, S. Pre-Pregnancy Obesity, Excessive Gestational Weight Gain, and the Risk of Pregnancy-Induced Hypertension and Gestational Diabetes Mellitus. J. Clin. Med. 2020, 9, 1980. [Google Scholar] [CrossRef] [PubMed]
- Heslehurst, N.; Ells, L.J.; Simpson, H.; Batterham, A.; Wilkinson, J.; Summerbell, C.D. Trends in maternal obesity incidence rates, demographic predictors, and health inequalities in 36 821 women over a 15-year period. BJOG Int. J. Obstet. Gynaecol. 2007, 114, 187–194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ryan, D. Obesity in women: A life cycle of medical risk. Int. J. Obes. 2007, 31, S3–S7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sui, Z.; Dodd, J.M. Exercise in obese pregnant women: Positive impacts and current perceptions. Int. J. Women's Health 2013, 5, 389. [Google Scholar] [CrossRef] [Green Version]
- Daly, N.; Mitchell, C.; Farren, M.; Kennelly, M.M.; Hussey, J.; Turner, M.J. Maternal obesity and physical activity and exercise levels as pregnancy advances: An observational study. Ir. J. Med Sci. 2016, 185, 357–370. [Google Scholar] [CrossRef] [PubMed]
- Sui, Z.; Moran, L.J.; Dodd, J.M. Physical activity levels during pregnancy and gestational weight gain among women who are overweight or obese. Health Promot. J. Aust. Off. J. Aust. Assoc. Health Promot. Prof. 2013, 24, 206–213. [Google Scholar] [CrossRef]
- Sebastián Manzanares, G.; Ángel Santalla, H.; Irene Vico, Z.; López Criado, M.S.; Alicia Pineda, L.; José Luis Gallo, V. Abnormal maternal body mass index and obstetric and neonatal outcome. J. Matern. Fetal Neonatal Med. 2012, 25, 308–312. [Google Scholar] [CrossRef]
- Yu, Z.; Han, S.; Zhu, J.; Sun, X.; Ji, C.; Guo, X. Pre-pregnancy body mass index in relation to infant birth weight and offspring overweight/obesity: A systematic review and meta-analysis. PLoS ONE 2013, 8, e61627. [Google Scholar] [CrossRef] [Green Version]
- Lawlor, D.A.; Chaturvedi, N. Treatment and prevention of obesity—Are there critical periods for intervention? Int. J. Epidemiol. 2006, 35, 3–9. [Google Scholar] [CrossRef] [Green Version]
- Harnack, L.; Schmitz, K. The role of nutrition and physical activity in the obesity epidemic. In Obesity Prevention and Public Health; Crawford, D., Jeffery, R., Eds.; Oxford University Press: New York, NY, USA, 2005. [Google Scholar]
- Physical activity and exercise during pregnancy and the postpartum period. American College of Obstetricians and Gynecologists (ACOG) Committee Opinion No. 804. Obs. Gynecol. 2020, 135, e178–e188. [CrossRef] [Green Version]
- Flannery, C.; McHugh, S.; Anaba, A.E.; Clifford, E.; O’Riordan, M.; Kenny, L.C.; McAuliffe, F.M.; Kearney, P.M.; Byrne, M. Enablers and barriers to physical activity in overweight and obese pregnant women: An analysis informed by the theoretical domains framework and COM-B model. BMC Pregnancy Childbirth 2018, 18, 178. [Google Scholar] [CrossRef]
- Weir, Z.; Bush, J.; Robson, S.C.; McParlin, C.; Rankin, J.; Bell, R. Physical activity in pregnancy: A qualitative study of the beliefs of overweight and obese pregnant women. BMC Pregnancy Childbirth 2010, 10, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, K.M.; Campbell, C.G. Physical activity during pregnancy: Impact of applying different physical activity guidelines. J. Pregnancy 2013, 2013, 165617. [Google Scholar] [CrossRef]
- Health Promotion Administration. Maternal Health Instruction Booklet; Ministry of Health and Welfare: Taipei, Taiwan, 2021.
- U.S. Department of Health and Human Services. Physical Activity Guidelines for Americans, 2nd ed.; U.S. Department of Health and Human Services: Washington, DC, USA, 2018.
- Harrison, A.L.; Taylor, N.F.; Shields, N.; Frawley, H.C. Attitudes, barriers and enablers to physical activity in pregnant women: A systematic review. J. Physiother. 2018, 64, 24–32. [Google Scholar] [CrossRef] [PubMed]
- Su, M.; Chang, M.; Sun, J. The Perceptions and Experience of Women with Gestational Diabetes Mellitus in Taiwan: A Phenomenological Study; Research Square: Taipei, Taiwan, 2021. [Google Scholar] [CrossRef]
- Evenson, K.R.; Savitz, D.A.; Huston, S.L. Leisure-time physical activity among pregnant women in the US. Paediatr. Perinat. Epidemiol. 2004, 18, 400–407. [Google Scholar] [CrossRef]
- O'Keeffe, L.M.; Dahly, D.L.; Murphy, M.; Greene, R.A.; Harrington, J.M.; Corcoran, P.; Kearney, P.M. Positive lifestyle changes around the time of pregnancy: A cross-sectional study. BMJ Open 2016, 6, e010233. [Google Scholar] [CrossRef] [Green Version]
- Evenson, K.R.; Mottola, M.F.; Owe, K.M.; Rousham, E.K.; Brown, W.J. Summary of international guidelines for physical activity following pregnancy. Obstet. Gynecol. Surv. 2014, 69, 407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prochaska, J.O.; DiClemente, C.C. Stages and processes of self-change of smoking: Toward an integrative model of change. J. Consult. Clin. Psychol. 1983, 51, 390–395. [Google Scholar] [CrossRef]
- Prochaska, J.O.; Velicer, W.D.; DiClemente, C.C. Measuring processes of change: Applications to the cessation of smoking. J. Consult. Clin. Psychol. 1988, 56, 520–528. [Google Scholar] [CrossRef]
- Nyumba, T.; Wilson, K.; Derrick, C.J.; Mukherjee, N. The use of focus group discussion methodology: Insights from two decades of application in conservation. Methods. Ecol. Evol. 2018, 9, 20–32. [Google Scholar] [CrossRef] [Green Version]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health. Care. 2007, 19, 349–357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Constantinou, C.S.; Georgiou, M.; Perdikogianni, M. A comparative method for themes saturation (CoMeTS) in qualitative interviews. Qual. Res. 2017, 17, 571–588. [Google Scholar] [CrossRef]
- Thompson, E.L.; Vamos, C.A.; Daley, E.M. Physical activity during pregnancy and the role of theory in promoting positive behavior change: A systematic review. J. Sport Health Sci. 2017, 6, 198–206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, C.; Jancey, J.; Howat, P.; Dhaliwal, S.; Burns, S.; McManus, A.; Hills, A.P.; Anderson, A.S. Utility of stages of change construct in the planning of physical activity interventions among playgroup mothers. BMC Res. Notes 2013, 6, 300. [Google Scholar] [CrossRef] [Green Version]
- Hogan, C.L.; Catalino, L.I.; Mata, J.; Fredrickson, B.L. Beyond emotional benefits: Physical activity and sedentary behaviour affect psychosocial resources through emotions. Psychol. Health 2015, 30, 354–369. [Google Scholar] [CrossRef]
- Watson, E.D.; Oddie, B.; Constantinou, D. Exercise during pregnancy: Knowledge and beliefs of medical practitioners in South Africa: A survey study. BMC Pregnancy Childbirth 2015, 15, 245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Renault, K.M.; Nørgaard, K.; Nilas, L.; Carlsen, E.M.; Cortes, D.; Pryds, O.; Secher, N.J. The Treatment of Obese Pregnant Women (TOP) study: A randomized controlled trial of the effect of physical activity intervention assessed by pedometer with or without dietary intervention in obese pregnant women. Am. J. Obstet. Gynecol. 2014, 210, 134.e1–134.e9. [Google Scholar] [CrossRef]
- Donofry, S.D.; Germeroth, L.J.; Conlon, R.P.K.; Venditti, E.M.; Levine, M.D. Correlates of Physical Activity Engagement among Pregnant Women with Overweight and Obesity. Women's Health Issues 2020, 30, 393–400. [Google Scholar] [CrossRef] [PubMed]
- Genkinger, J.M.; Jehn, M.L.; Sapun, M.; Mabry, I.; Young, D.R. Does weight status influence perceptions of physical activity barriers among African-American women? Ethn. Dis. 2006, 16, 78. [Google Scholar] [PubMed]
- Sui, Z.; Turnbull, D.; Dodd, J. Overweight and obese women’s perceptions about making healthy change during pregnancy: A mixed method study. Matern. Child Health J. 2013, 17, 1879–1887. [Google Scholar] [CrossRef] [PubMed]
- Bisson, M.; Alméras, N.; Dufresne, S.S.; Robitaille, J.; Rhéaume, C.; Bujold, E.; Frenette, J.; Tremblay, A.; Marc, I. A 12-week exercise program for pregnant women with obesity to improve physical activity levels: An open randomised preliminary study. PLoS ONE 2015, 10, e0137742. [Google Scholar] [CrossRef]
- Miller, W.R. Motivational interviewing: Research, practice, and puzzles. Addict. Behav. 1996, 21, 835–842. [Google Scholar] [CrossRef]
- Hoare, E.; Milton, K.; Foster, C.; Allender, S. The associations between sedentary behaviour and mental health among adolescents: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 1–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- King, J.; Jebeile, H.; Garnett, S.; Baur, L.; Paxton, S.; Gow, M. Physical activity based pediatric obesity treatment, depression, self-esteem and body image: A systematic review with meta-analysis. Ment. Health Phys. Act. 2020, 19, 100342. [Google Scholar] [CrossRef]
- Rodriguez-Ayllon, M.; Cadenas-Sánchez, C.; Estévez-López, F.; Muñoz, N.E.; Mora-Gonzalez, J.; Migueles, J.H.; Molina-García, P.; Henriksson, H.; Mena-Molina, A.; Martínez-Vizcaíno, V. Role of physical activity and sedentary behavior in the mental health of preschoolers, children and adolescents: A systematic review and meta-analysis. Sports Med. 2019, 49, 1383–1410. [Google Scholar] [CrossRef] [PubMed]
- Weissgerber, T.L.; Wolfe, L.A.; Davies, G.A.; Mottola, M.F. Exercise in the prevention and treatment of maternal–fetal disease: A review of the literature. Appl. Physiol. Nutr. Metab. 2006, 31, 661–674. [Google Scholar] [CrossRef] [PubMed]
- Kołomańska, D.; Zarawski, M.; Mazur-Bialy, A. Physical activity and depressive disorders in pregnant women—A systematic review. Medicina 2019, 55, 212. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| 1. How do you manage your weight gain/loss before and during your pregnancy? |
| 2. Have you had successful experience to manage your weight by increasing physical activity? |
| 3. When you hear people say, “increase your physical activity” or “be more active in your leisure time,” what comes to your mind? What is your impression when people talk about the connection between weight and physical activity? |
| 4. What have your obstetrician suggested regarding physical activity, if any? |
| 5. How much do you intend to change your current lifestyle? Are you willing to start increasing physical activity? Why and why not? |
| 6. Do you think it is necessary now to adopt a more active lifestyle? Say, increase PA in your leisure time? |
| 7. Do you want to know more about how to increase physical activity? |
| 8. Are you engaged in any physical activity routine? Official or unofficial? How? |
| 9. Say if you plan to be more active on a regular basis, what would be the possible hurdle? |
| 10. If you have increased your physical activity during pregnancy, do you plan to continue doing so? |
| 11. Do you need to get someone’s approval or assistance in order to achieve your physical activity plan? Who would that be? |
| 12. What would be considered appropriate advice for an obstetrician or a nurse to tell his/her patient to increase physical activity, what is your suggestion? |
| 13. How do you prefer to be motivated or assisted to increase physical activity after you deliver your baby? |
| n | % | |
|---|---|---|
| Pre-pregnancy BMI | ||
| Overweight (≥25) | 7 | 53.9 |
| Obese (≥30) | 6 | 46.1 |
| Parity | ||
| nulliparous | 9 | 69.2 |
| multiparous | 4 | 30.8 |
| Employment | ||
| Yes | 4 | 30.8 |
| No | 9 | 69.2 |
| Married | ||
| Yes | 11 | 84.6 |
| No | 2 | 15.4 |
| Education level | ||
| College or university | 13 | 100 |
| Smartphone possession | ||
| Yes | 13 | 100 |
| Online search for pregnant information | ||
| Yes | 13 | 100 |
| Experience of using pregnant-related APPs | ||
| Yes | 7 | 53.9 |
| No | 6 | 46.1 |
| Being suggested to manage gestational weight gain | ||
| Yes | 13 | 100 |
| Being suggested to increase physical activity | ||
| Yes | 13 | 100 |
| I. Perceptions of Physical Activity Engagement | |
| Theme 1 | Physical activity perceived as a cliché when being suggested by obstetricians |
| Theme 2 | Physical activity triggers negative experience about unsuccessful weight management |
| Theme 3 | Engaging in higher levels of physical activity evokes negative emotions (representing an impossible task) |
| II. Motivation and Readiness to Adopt an Active Lifestyle | |
| Theme 4 | All obese and overweight pregnant women are believers of PA’s beneficial effects |
| Lower levels of motivation to change are associated with lower levels of self-esteem and self-efficacy | |
| Higher levels of motivation to change are associated with fetus health, child-bearing responsibilities, and significant others’ expectations | |
| Theme 5 | A tongue never gets things done and preparation usually takes a long time |
| Information is needed to prepare for pregnancy-appropriate physical activities | |
| Theme 6 | Higher levels of readiness are associated with successful weight management experience |
| III. Barriers to Engage in Higher Levels of Physical Activity | |
| Theme 7 | Particular cultural beliefs limit pregnant women’s physical activity |
| Theme 8 | Fear of birth-related complications limits pregnant women’s physical activity |
| Theme 9 | Low peer support (to work out together) and limited support from significant others |
| External conditions perceived inappropriate for physical activities | |
| Competing family and/or work priorities | |
| IV. Preference of Facilitation Strategies | |
| Theme 10 | Empathetic communication from the health care providers |
| Theme 11 | A “fetus-centered” approach to motivate mothers and facilitate physical activity |
| “Patient-centered” counseling to overcome barriers by tailoring each individual’s needs | |
| V. Peer Support During Focus Groups | |
| Theme 12 | Support for being an expectant mother |
| Theme 13 | Support for low self-esteem: empathizing similar body image and unsuccessful weight management (being lazy and ugly) |
| Theme 14 | Support for low self-efficacy: empathizing similar feelings of frustration regarding multiple barriers to initiate an active lifestyle |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsiung, Y.; Lee, C.-F.; Chi, L.-K.; Huang, J.-P. “Moving for My Baby!” Motivators and Perceived Barriers to Facilitate Readiness for Physical Activity during Pregnancy among Obese and Overweight Women of Urban Areas in Northern Taiwan. Int. J. Environ. Res. Public Health 2021, 18, 5275. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18105275
Hsiung Y, Lee C-F, Chi L-K, Huang J-P. “Moving for My Baby!” Motivators and Perceived Barriers to Facilitate Readiness for Physical Activity during Pregnancy among Obese and Overweight Women of Urban Areas in Northern Taiwan. International Journal of Environmental Research and Public Health. 2021; 18(10):5275. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18105275
Chicago/Turabian StyleHsiung, Yvonne, Ching-Fang Lee, Li-Kang Chi, and Jian-Pei Huang. 2021. "“Moving for My Baby!” Motivators and Perceived Barriers to Facilitate Readiness for Physical Activity during Pregnancy among Obese and Overweight Women of Urban Areas in Northern Taiwan" International Journal of Environmental Research and Public Health 18, no. 10: 5275. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18105275