
Direct and Inverse Correlates of Post-Traumatic Stress Disorder among School-Age Autistic Boys

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Measures
2.3. Procedure
2.4. Statistical Analyses
3. Results
3.1. Sample Data
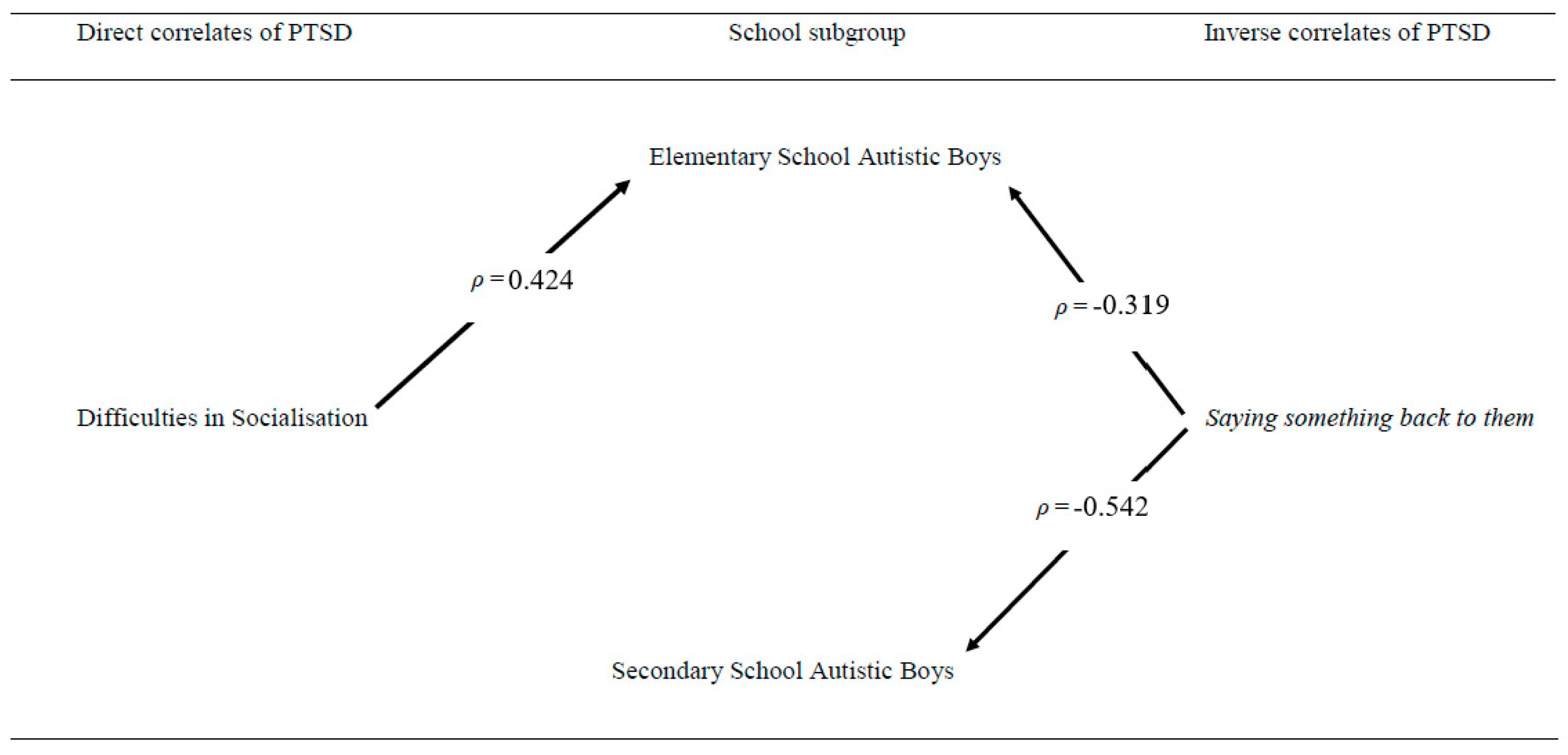
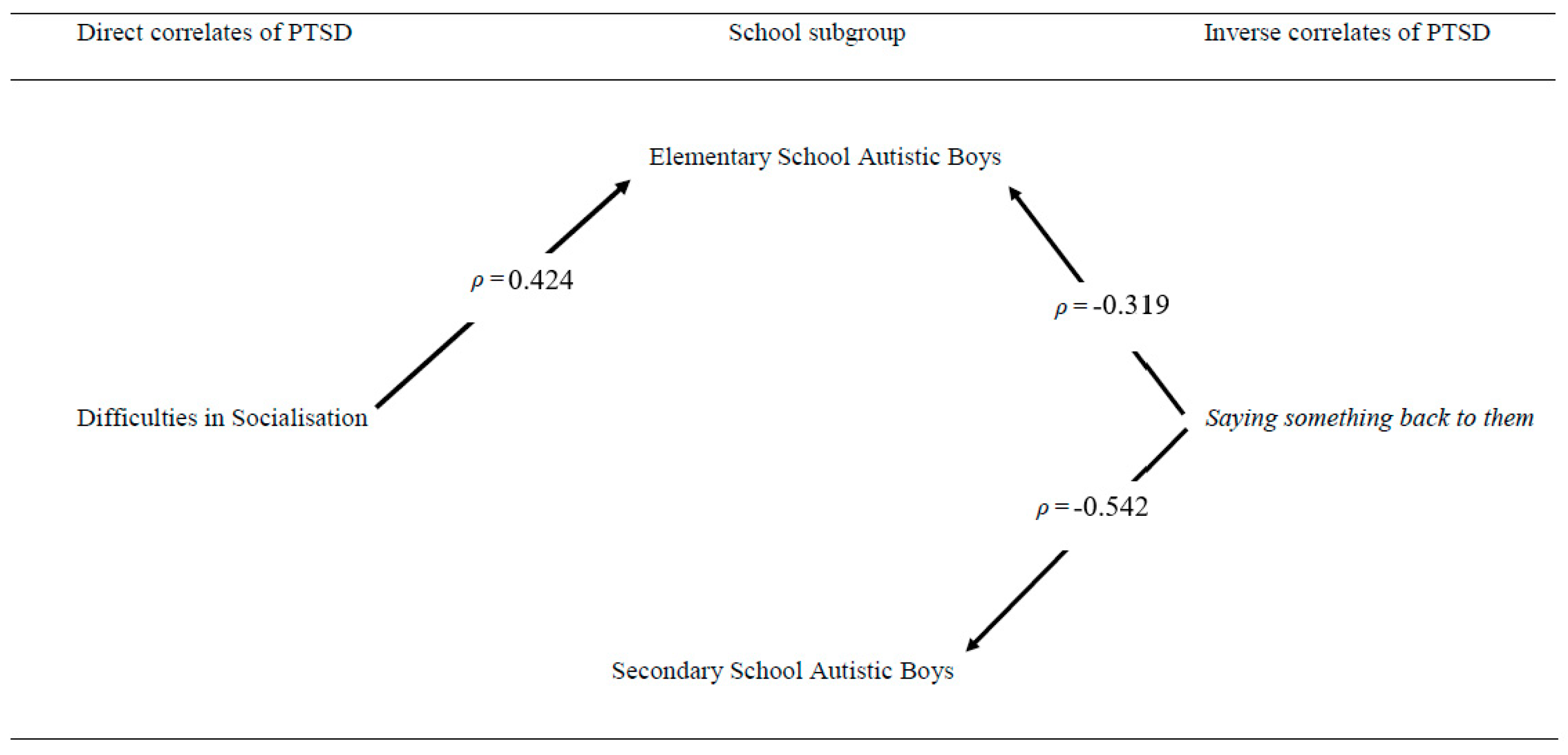
3.2. Elementary vs. Secondary School Boys
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dai, W.; Liu, A.; Kaminga, A.; Deng, J.; Lai, Z.; Wen, S. Prevalence of Posttraumatic Stress Disorder among Children and Adolescents following Road Traffic Accidents: A Meta-Analysis. Can. J. Psychiatry 2018, 63, 798–808. [Google Scholar] [CrossRef] [Green Version]
- Marthoenis, M.; Ilyas, A.; Sofyan, H.; Schouler-Ocak, M. Prevalence, comorbidity and predictors of post-traumatic stress disorder, depression, and anxiety in adolescents following an earthquake. Asian J. Pharm. 2019, 43, 154–159. [Google Scholar] [CrossRef]
- Sharpley, C.; Bitsika, V.; Andronicos, N.; Agnew, L. Prevalence, Structure and Correlates of Anxiety-Depression in boys with an Autism Spectrum Disorder. Res. Dev. Disabil. 2016, 49–50, 302–311. [Google Scholar]
- White, S.W.; Oswald, D.; Ollendick, T.; Scahill, L. Anxiety in children and adolescents with autism spectrum disorders. Clin. Psychol. Rev. 2009, 29, 216–229. [Google Scholar] [CrossRef] [Green Version]
- DeFilippis, M. Depression in Children and Adolescents with Autism Spectrum Disorder. Children 2018, 5, 112. [Google Scholar] [CrossRef] [Green Version]
- Mehtar, M.; Mukaddes, N. Posttraumatic Stress Disorder in individuals with diagnosis of Autistic Spectrum Disorders. Res. Autism Spectr. Disord. 2011, 5, 539–546. [Google Scholar] [CrossRef]
- Kenny, L.; Hattersley, C.; Molins, B.; Buckley, C.; Povey, C.; Pellicano, E. Which terms should be used to describe autism? Perspectives from the UK autism community. Autism 2016, 20, 442–462. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Pub: Washington, DC, USA, 2013. [Google Scholar]
- Tierney, S.; Burns, J.; Kilbey, E. Looking behind the mask: Social coping strategies of girls on the autistic spectrum. Res. Autism Spectr. Disord. 2016, 23, 73–83. [Google Scholar] [CrossRef] [Green Version]
- Winston, F.; Kassam-Adams, N.; Garcia-Espana, F.; Ittenbach, R.; Cnaan, A. Screening for risk of persistent posttraumatic stress in injured children and their parents. Jama 2003, 290, 643–649. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chou, W.-J.; Wang, P.-W.; Hsiao, R.; Hu, H.-F.; Yen, C.-F. Role of School Bullying Involvement in Depression, Anxiety, Suicidality, and Low Self-Esteem Among Adolescents with High-Functioning Autism Spectrum Disorder. Front. Psychiatry 2020, 11, 9. [Google Scholar] [CrossRef]
- Bitsika, V.; Heyne, D.; Sharpley, C. Is Bullying Associated with Emerging School Refusal in Autistic Boys? J. Autism Dev. Disord. 2021, 51, 1081–1092. [Google Scholar] [CrossRef] [PubMed]
- Maïano, C.; Normand, C.; Salvas, M.-C.; Moullec, G.; Aimé, A. Prevalence of School Bullying Among Youth with Autism Spectrum Disorders: A Systematic Review and Meta-Analysis. Autism Res. 2016, 9, 601–615. [Google Scholar] [CrossRef]
- Humphrey, N.; Hebron, J. Bullying of children and adolescents with autism spectrum conditions: A ‘state of the field’ review. Int. J. Incl. Educ. 2015, 19, 845–862. [Google Scholar] [CrossRef]
- Haruvi-Lamdan, N.; Horesh, D.; Golan, O. PTSD and autism spectrum disorder: Co-morbidity, gaps in research, and potential shared mechanisms. Psychol. Trauma 2018, 10, 290–299. [Google Scholar] [CrossRef] [PubMed]
- Hull, L.; Petrides, K.; Allison, C.; Smith, P.; Baron-Cohen, S.; Lai, M.; Mandy, W. “Putting on my best normal”: Social camouflaging in adults with autism spectrum conditions. J. Autism Dev. Disord. 2017, 47, 2519–2534. [Google Scholar] [CrossRef]
- Gadow, K.; Sprafkin, J. Child and Adolescent Symptom Inventory 4R: Screening and Norms Manual; Checkmate Plus: Stony Brook, NY, USA, 2010. [Google Scholar]
- Gadow, K.; Devincent, C.; Pomeroy, J.; Azizian, A. Comparison of DSM-IV symptoms in elementary school-age children with PDD versus clinic and community samples. Autism 2005, 9, 392–415. [Google Scholar] [CrossRef] [PubMed]
- Weisbrot, D.; Gadow, K.; DeVincent, C.; Pomeroy, J. The presentation of anxiety in children with Pervasive Developmental Disorders. J. Child. Adolesc. Psychopharmacol. 2005, 15, 477–496. [Google Scholar] [CrossRef]
- Gadow, K.; Sprafkin, J. The Symptom Inventories: An Annotated Bibliography; Checkmate Plus: Stony Brook, NY, USA, 2015. [Google Scholar]
- Sainato, D.; Goldstein, H.; Strain, P. Effects of self-evaluation on preschool children’s use of social interaction strategies with their classmates with autism. J. Appl. Behav. Anal. 1992, 25, 127–141. [Google Scholar] [CrossRef] [Green Version]
- Capps, L.; Sigman, M.; Yirmiya, N. Self-competence and emotional understanding in high-functioning children with autism. Dev. Psychopathol. 1995, 7, 137–149. [Google Scholar] [CrossRef]
- Bauminger, N.; Kasari, C. Loneliness and friendship in high-functioning children with autism. Child. Dev. 2000, 71, 447–456. [Google Scholar] [CrossRef]
- Kuusikko, S.; Pollock-Wurman, R.; Jussila, K.; Carter, A.; Mattila, M.-L.; Ebeling, H.; Pauls, D.L.; Moilanen, I. Social anxiety in high-functioning children and adolescents with Autism and Asperger Syndrome. J. Autism Dev. Disord. 2008, 38, 1697–1709. [Google Scholar] [CrossRef] [PubMed]
- Vickerstaff, S.; Heriot, S.; Wong, M.L.; Lopes, A.; Dossetor, D. Intellectual ability, self-perceived social competence, and depressive symptomatology in children with high-functioning autistic spectrum disorders. J. Autism Dev. Disord. 2007, 37, 1647–1664. [Google Scholar] [CrossRef] [PubMed]
- Lecavalier, L.; Gadow, K.; DeVincent, C.; Edwards, M. Validation of DSM-IV Model of psychiatric syndromes in children with Autism Spectrum Disorders. J. Autism Dev. Disord. 2009, 39, 278–289. [Google Scholar] [CrossRef] [PubMed]
- Bitsika, V.; Sharpley, C.; Sweeney, J.; McFarlane, J. HPA and SAM axis responses as correlates of self- vs parental ratings of anxiety in boys with an Autistic Disorder. Physiol. Behav. 2014, 127, 1–7. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power for the Behavioural Sciences; Psychology Press: Hillsdale, NJ, USA, 2004. [Google Scholar]
- Rumball, F. A Systematic Review of the Assessment and Treatment of Posttraumatic Stress Disorder in Individuals with Autism Spectrum Disorders. Rev. J. Autism. Dev. Disord. 2019, 6, 294–324. [Google Scholar] [CrossRef] [Green Version]
- Bejerot, S.; Mortberg, E. Do autistic traits play a role in the bullying of Obsessive-Compulsive Disorder and Social Phobia sufferers? Psychopathology 2009, 42, 170–176. [Google Scholar] [CrossRef]
- Kerns, C.; Berkowitz, S.; Moskowitz, L.; Drahota, A.; Lerner, M.; Newschaffer, C. Screening and treatment of trauma-related symptoms in youth with autism spectrum disorder among community providers in the United States. Autism 2020, 24, 515–525. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Strategy | Spearman Correlation with CASI-4R PTSD Score | p |
|---|---|---|
| Ignore them | 0.007 | 0.961 |
| Smile and act OK | 0.054 | 0.686 |
| Say something back to them | −0.370 | 0.004 |
| Be physically aggressive | −0.145 | 0.278 |
| Chase them away | −0.239 | 0.071 |
| Walk away from them | −0.111 | 0.405 |
| Avoid them | −0.041 | 0.759 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bitsika, V.; Sharpley, C.F. Direct and Inverse Correlates of Post-Traumatic Stress Disorder among School-Age Autistic Boys. Int. J. Environ. Res. Public Health 2021, 18, 5285. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18105285
Bitsika V, Sharpley CF. Direct and Inverse Correlates of Post-Traumatic Stress Disorder among School-Age Autistic Boys. International Journal of Environmental Research and Public Health. 2021; 18(10):5285. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18105285
Chicago/Turabian StyleBitsika, Vicki, and Christopher F. Sharpley. 2021. "Direct and Inverse Correlates of Post-Traumatic Stress Disorder among School-Age Autistic Boys" International Journal of Environmental Research and Public Health 18, no. 10: 5285. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18105285