
Short-Term Effects of Balance Training with Stroboscopic Vision for Patients with Chronic Ankle Instability: A Single-Blinded Randomized Controlled Trial

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
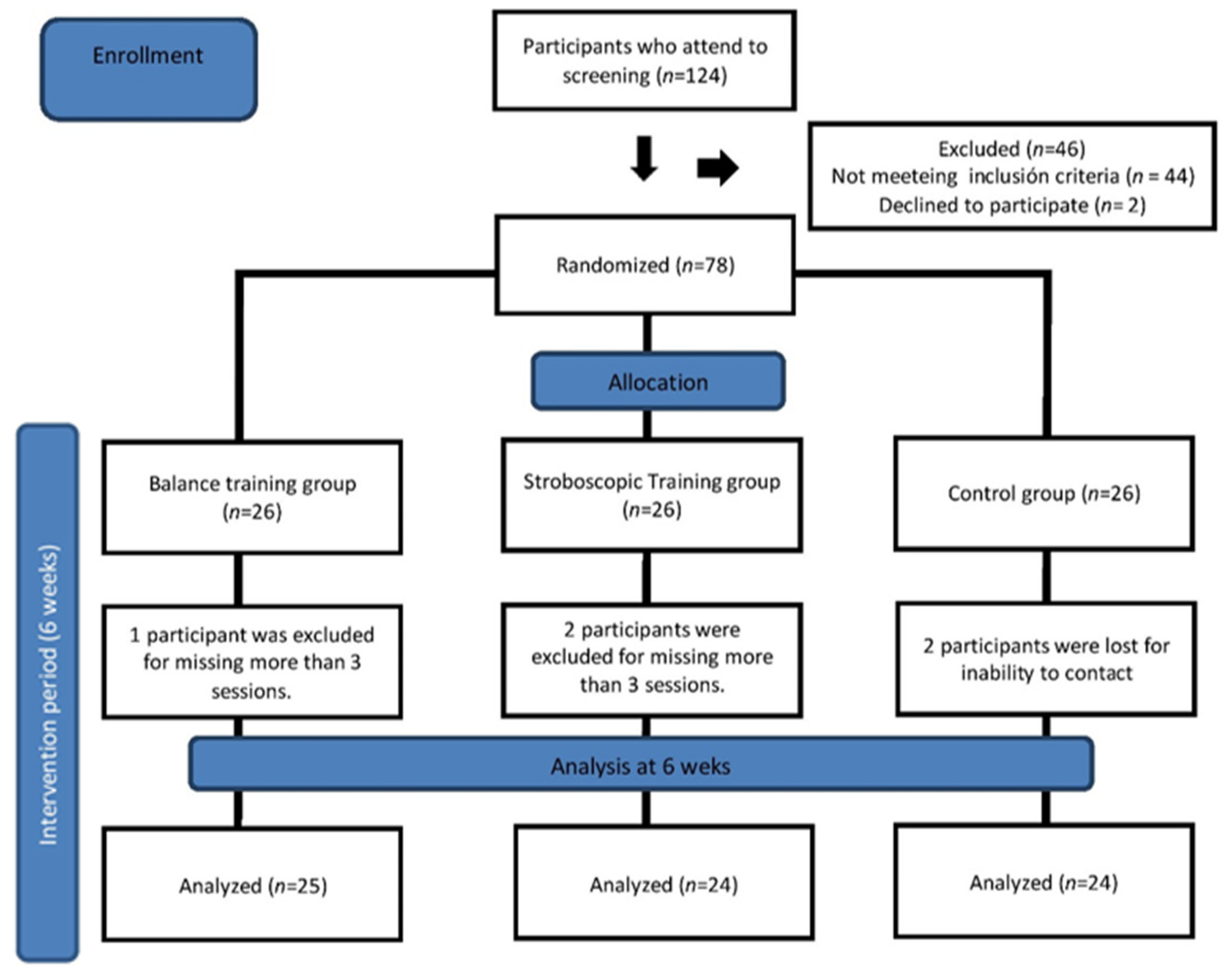
2.1. Participants and Randomization
2.2. Intervention
2.3. Balance Training (BT)
2.4. Balance Training and Stroboscopic Vision (BTSV)
2.5. Control Group
2.6. Outcome Measures
2.6.1. Primary Outcome Measures
2.6.2. Secondary Outcome Measures
2.7. Statistical Analyses
3. Results
4. Discussion
4.1. Patient-Reported Outcomes
4.2. Dynamic Balance
4.3. Dorsiflexion Range of Motion
4.4. Potential Neurophysiological Mechanisms
4.5. Clinical Implications
4.6. Study Limitations and Recommendations for Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fong, D.T.-P.; Hong, Y.; Chan, L.-K.; Yung, P.S.-H.; Chan, K.-M. A Systematic Review on Ankle Injury and Ankle Sprain in Sports. Sports Med. 2007, 37, 73–94. [Google Scholar] [CrossRef] [Green Version]
- Bridgman, S.A.; Clement, D.; Downing, A.; Walley, G.; Phair, I.; Maffulli, N. Population based epidemiology of ankle sprains attending accident and emergency units in the West Midlands of England, and a survey of UK practice for severe ankle sprains. Emerg. Med. J. 2003, 20, 508–510. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hertel, J. Functional Anatomy, Pathomechanics, and Pathophysiology of Lateral Ankle Instability. J. Athl. Train. 2002, 37, 364–375. [Google Scholar] [PubMed]
- Konradsen, L.; Bech, L.; Ehrenbjerg, M.; Nickelsen, T. Seven years follow-up after ankle inversion trauma. Scand. J. Med. Sci. Sports 2002, 12, 129–135. [Google Scholar] [CrossRef]
- Willems, T.; Witvrouw, E.; Verstuyft, J.; Vaes, P.; De Clercq, D. Proprioception and Muscle Strength in Subjects With a History of Ankle Sprains and Chronic Instability. J. Athl. Train. 2002, 37, 487–493. [Google Scholar]
- Docherty, C.L.; McLeod, T.C.V.; Shultz, S.J. Postural Control Deficits in Participants with Functional Ankle Instability as Measured by the Balance Error Scoring System. Clin. J. Sport Med. 2006, 16, 203–208. [Google Scholar] [CrossRef] [PubMed]
- Wright, C.J.; Linens, S.W.; Cain, M.S. A Randomized Controlled Trial Comparing Rehabilitation Efficacy in Chronic Ankle Instability. J. Sport Rehabil. 2017, 26, 238–249. [Google Scholar] [CrossRef]
- Smith, B.I.; Curtis, D.; Docherty, C.L. Effects of Hip Strengthening on Neuromuscular Control, Hip Strength, and Self-Reported Functional Deficits in Individuals With Chronic Ankle Instability. J. Sport Rehabil. 2018, 27, 364–370. [Google Scholar] [CrossRef]
- Cruz-Diaz, D.; Lomas-Vega, R.; Osuna-Pérez, M.C.; Contreras, F.H.; Martínez-Amat, A. Effects of 6 Weeks of Balance Training on Chronic Ankle Instability in Athletes: A Randomized Controlled Trial. Int. J. Sports Med. 2015, 36, 754–760. [Google Scholar] [CrossRef] [Green Version]
- Ross, S.E.; Arnold, B.L.; Blackburn, J.T.; Brown, C.N.; Guskiewicz, K.M. Enhanced balance associated with coordination training with stochastic resonance stimulation in subjects with functional ankle instability: An experimental trial. J. Neuroeng. Rehabil. 2007, 4, 47. [Google Scholar] [CrossRef] [Green Version]
- McKeon, P.O.; Stein, A.J.; Ingersoll, C.D.; Hertel, J. Altered Plantar-Receptor Stimulation Impairs Postural Control in Those With Chronic Ankle Instability. J. Sport Rehabil. 2012, 21, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Powden, C.J.; Hoch, J.M.; Hoch, M.C. Rehabilitation and Improvement of Health-Related Quality-of-Life Detriments in Individuals With Chronic Ankle Instability: A Meta-Analysis. J. Athl. Train. 2017, 52, 753–765. [Google Scholar] [CrossRef]
- Mckeon, P.O.; Ingersoll, C.D.; Kerrigan, D.C.; Saliba, E.; Bennett, B.C.; Hertel, J. Balance Training Improves Function and Postural Control in Those with Chronic Ankle Instability. Med. Sci. Sports Exerc. 2008, 40, 1810–1819. [Google Scholar] [CrossRef] [PubMed]
- Powden, C.J.; Hoch, J.M.; Jamali, B.E.; Hoch, M.C. A 4-Week Multimodal Intervention for Individuals With Chronic Ankle Instability: Examination of Disease-Oriented and Patient-Oriented Outcomes. J. Athl. Train. 2019, 54, 384–396. [Google Scholar] [CrossRef] [Green Version]
- Song, K.; Burcal, C.; Hertel, J.; Wikstrom, E.A. Increased visual utilization in chronic ankle instability: A meta-analysis. Med. Sci. Sports Exerc. 2016, 48, 2046–2056. [Google Scholar] [CrossRef] [PubMed]
- Song, K.; Rhodes, E.; Wikstrom, E.A. Balance Training Does Not Alter Reliance on Visual Information during Static Stance in Those with Chronic Ankle Instability: A Systematic Review with Meta-Analysis. Sports Med. 2018, 48, 893–905. [Google Scholar] [CrossRef]
- Hertel, J. Sensorimotor Deficits with Ankle Sprains and Chronic Ankle Instability. Clin. Sports Med. 2008, 27, 353–370. [Google Scholar] [CrossRef]
- Kim, K.-M.; Kim, J.-S.; Grooms, D.R. Stroboscopic Vision to Induce Sensory Reweighting During Postural Control. J. Sport Rehabil. 2017, 26, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clark, J.F.; Ellis, J.K.; Bench, J.; Khoury, J.; Graman, P. High-Performance Vision Training Improves Batting Statistics for University of Cincinnati Baseball Players. PLoS ONE 2012, 7, e29109. [Google Scholar] [CrossRef] [Green Version]
- Chan, L.; Heinemann, A.W.; Roberts, J. Elevating the Quality of Disability and Rehabilitation Research: Mandatory Use of the Reporting Guidelines. Ann. Phys. Rehabil. Med. 2014, 57, 558–560. [Google Scholar] [CrossRef] [Green Version]
- Gribble, P.A.; Delahunt, E.; Bleakley, C.M.; Caulfield, B.; Docherty, C.L.; Fong, D.T.-P.; Fourchet, F.; Hertel, J.; Hiller, C.E.; Kaminski, T.W.; et al. Selection Criteria for Patients With Chronic Ankle Instability in Controlled Research: A Position Statement of the International Ankle Consortium. J. Athl. Train. 2014, 49, 121–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bennell, K.; Talbot, R.; Wajswelner, H. Intra-rater and inter-rater reliability of a weight-bearing lunge measure of ankle dorsifl exion. Aust. J. Physiother. 1998, 44, 175–180. [Google Scholar] [CrossRef] [Green Version]
- Hoch, M.C.; Staton, G.S.; McKeon, J.M.M.; Mattacola, C.G.; McKeon, P.O. Dorsiflexion and dynamic postural control deficits are present in those with chronic ankle instability. J. Sci. Med. Sport 2012, 15, 574–579. [Google Scholar] [CrossRef] [PubMed]
- Hertel, J.; Braham, R.A.; Hale, S.A.; Olmsted-Kramer, L.C. Simplifying the Star Excursion Balance Test: Analyses of Subjects With and Without Chronic Ankle Instability. J. Orthop. Sports Phys. Ther. 2006, 36, 131–137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gribble, P.A.; Hertel, J. Considerations for normoralizing measures of the Star Excursion Balance Test. Meas. Phys. Ed. Exer. Sci. 2003, 7, 89–100. [Google Scholar] [CrossRef]
- Robinson, R.H.; Gribble, P.A. Support for a Reduction in the Number of Trials Needed for the Star Excursion Balance Test. Arch. Phys. Med. Rehabil. 2008, 89, 364–370. [Google Scholar] [CrossRef] [PubMed]
- Hiller, C.E.; Refshauge, K.M.; Bundy, A.C.; Herbert, R.D.; Kilbreath, S.L. The Cumberland Ankle Instability Tool: A Report of Validity and Reliability Testing. Arch. Phys. Med. Rehabil. 2006, 87, 1235–1241. [Google Scholar] [CrossRef]
- Cruz-Díaz, D.; Hita-Contreras, F.; Lomas-Vega, R.; Osuna-Pérez, M.C.; Martínez-Amat, A. Cross-cultural adaptation and validation of the Spanish version of the Cumberland Ankle Instability Tool (CAIT): An instrument to assess unilateral chronic ankle instability. Clin. Rheumatol. 2013, 32, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Wright, C.J.; Linens, S.W.; Cain, M.S. Establishing the Minimal Clinical Important Difference and Minimal Detectable Change for the Cumberland Ankle Instability Tool. Arch. Phys. Med. Rehabil. 2017, 98, 1806–1811. [Google Scholar] [CrossRef] [PubMed]
- Martin, R.L.; Irrgang, J.J.; Burdett, R.G.; Conti, S.F.; Van Swearingen, J.M. Evidence of Validity for the Foot and Ankle Ability Measure (FAAM). Foot Ankle Int. 2005, 26, 968–983. [Google Scholar] [CrossRef] [PubMed]
- Carcia, C.R.; Martin, R.L.; Drouin, J.M. Validity of the Foot and Ankle Ability Measure in Athletes With Chronic Ankle Instability. J. Athl. Train. 2008, 43, 179–183. [Google Scholar] [CrossRef] [Green Version]
- Maher, C.G.; Sherrington, C.; Herbert, R.D.; Moseley, A.M.; Elkins, M. ElkinsReliability of the PEDro scale for rating quality of randomized controlled trials. Phys. Ther. 2003, 83, 713–721. [Google Scholar] [CrossRef] [Green Version]
- Kim, K.-J.; Heo, M. Effects of virtual reality programs on balance in functional ankle instability. J. Phys. Ther. Sci. 2015, 27, 3097–3101. [Google Scholar] [CrossRef] [PubMed]
- Wright, C.J.; Arnold, B.L.; Ross, S.E.; Linens, S.W. Recalibration and Validation of the Cumberland Ankle Instability Tool Cutoff Score for Individuals With Chronic Ankle Instability. Arch. Phys. Med. Rehabil. 2014, 95, 1853–1859. [Google Scholar] [CrossRef] [PubMed]
- McGuine, T.A.; Greene, J.J.; Best, T.; Leverson, G. Balance As a Predictor of Ankle Injuries in High School Basketball Players. Clin. J. Sport Med. 2000, 10, 239–244. [Google Scholar] [CrossRef]
- Hoch, M.C.; Andreatta, R.D.; Mullineaux, D.R.; English, R.A.; McKeon, J.M.M.; Mattacola, C.G.; McKeon, P.O. Two-week joint mobilization intervention improves self-reported function, range of motion, and dynamic balance in those with chronic ankle instability. J. Orthop. Res. 2012, 30, 1798–1804. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schaefer, J.L.; Sandrey, M.A. Effects of a 4-week dynamic-balance-training program supplemented with Graston instrument-assisted soft-tissue mobilization for chronic ankle instability. J. Sport Rehabil. 2012, 21, 313–326. [Google Scholar] [CrossRef]
- Hilgendorf, J.R.; Vela, L.I.; Gobert, D.V.; Harter, R.A. Influence of Vestibular–Ocular Reflex Training on Postural Stability, Dynamic Visual Acuity, and Gaze Stabilization in Patients With Chronic Ankle Instability. Athl. Train. Sports Health Care 2012, 4, 220–229. [Google Scholar] [CrossRef]
- Ardakani, M.K.; Wikstrom, E.A.; Minoonejad, H.; Rajabi, R.; Sharifnezhad, A. Hop-Stabilization Training and Landing Biomechanics in Athletes With Chronic Ankle Instability: A Randomized Controlled Trial. J. Athl. Train. 2019, 54, 1296–1303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shih, Y.-F.; Yu, H.-T.; Chen, W.-Y.; Liao, K.-K.; Lin, H.-C.; Yang, Y.-R. The effect of additional joint mobilization on neuromuscular performance in individuals with functional ankle instability. Phys. Ther. Sport 2018, 30, 22–28. [Google Scholar] [CrossRef]
- Gabriner, M.L.; Houston, M.N.; Kirby, J.L.; Hoch, M.C. Contributing factors to Star Excursion Balance Test performance in individuals with chronic ankle instability. Gait Posture 2015, 41, 912–916. [Google Scholar] [CrossRef] [PubMed]
- Terada, M.; Harkey, M.S.; Wells, A.M.; Pietrosimone, B.G.; Gribble, P.A. The influence of ankle dorsiflexion and self-reported patient outcomes on dynamic postural control in participants with chronic ankle instability. Gait Posture 2014, 40, 193–197. [Google Scholar] [CrossRef]
- Hall, E.A.; Chomistek, A.K.; Kingma, J.J.; Docherty, C.L. Balance- and Strength-Training Protocols to Improve Chronic Ankle Instability Deficits, Part II: Assessing Patient-Reported Outcome Measures. J. Athl. Train. 2018, 53, 578–583. [Google Scholar] [CrossRef] [PubMed]
- Hall, E.A.; Chomistek, A.K.; Kingma, J.J.; Docherty, C.L. Balance- and Strength-Training Protocols to Improve Chronic Ankle Instability Deficits, Part I: Assessing Clinical Outcome Measures. J. Athl. Train. 2018, 53, 568–577. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vallandingham, R.A.; Gaven, S.L.; Powden, C.J. Changes in Dorsiflexion and Dynamic Postural Control After Mobilizations in Individuals With Chronic Ankle Instability: A Systematic Review and Meta-Analysis. J. Athl. Train. 2019, 54, 403–417. [Google Scholar] [CrossRef] [Green Version]
- Wilkins, L.; Appelbaum, L.G. An early review of stroboscopic visual training: Insights, challenges and accomplishments to guide future studies. Int. Rev. Sport Exerc. Psychol. 2020, 13, 65–80. [Google Scholar] [CrossRef]
- Appelbaum, L.G.; Erickson, G. Sports vision training: A review of the state-of-the-art in digital training techniques. Int. Rev. Sport Exerc. Psychol. 2018, 11, 160–189. [Google Scholar] [CrossRef]
- Mitroff, S.R.; Friesen, P.; Bennett, D.; Yoo, H.; Reichow, A.W. Enhancing Ice Hockey Skills Through Stroboscopic Visual Training: A Pilot Study. Athl. Train. Sports Health Care 2013, 5, 261–264. [Google Scholar] [CrossRef] [Green Version]
- Wilkins, L.; Gray, R. Effects of Stroboscopic Visual Training on Visual Attention, Motion Perception, and Catching Performance. Percept. Mot. Ski. 2015, 121, 57–79. [Google Scholar] [CrossRef] [PubMed]
- Wilkins, L.; Nelson, C.; Tweddle, S. Stroboscopic Visual Training: A Pilot Study with Three Elite Youth Football Goalkeepers. J. Cogn. Enhanc. 2017, 2, 3–11. [Google Scholar] [CrossRef] [Green Version]
- Hülsdünker, T.; Rentz, C.; Ruhnow, D.; Käsbauer, H.; Strüder, H.K.; Mierau, A. The Effect of 4-Week Stroboscopic Training on Visual Function and Sport-Specific Visuomotor Performance in Top-Level Badminton Players. Int. J. Sports Physiol. Perform. 2019, 14, 343–350. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.-T.; Meng, L.-F.; Chang, C.-J.; Lai, P.-L.; Lung, C.-W.; Chern, J.-S. Effect of Postural Control Demands on Early Visual Evoked Potentials during a Subjective Visual Vertical Perception Task in Adolescents with Idiopathic Scoliosis. Front. Hum. Neurosci. 2017, 11, 326. [Google Scholar] [CrossRef] [PubMed]
- Grooms, D.; Appelbaum, G.; Onate, J. Neuroplasticity Following Anterior Cruciate Ligament Injury: A Framework for Visual-Motor Training Approaches in Rehabilitation. J. Orthop. Sports Phys. Ther. 2015, 45, 381–393. [Google Scholar] [CrossRef]
- Taube, W.; Gollhofer, A.; Lauber, B. Training-, muscle- and task-specific up- and downregulation of cortical inhibitory processes. Eur. J. Neurosci. 2020, 51, 1428–1440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beck, S.; Taube, W.; Gruber, M.; Amtage, F.; Gollhofer, A.; Schubert, M. Task-specific changes in motor evoked potentials of lower limb muscles after different training interventions. Brain Res. 2007, 1179, 51–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levy, A.R.; Polman, R.C.J.; Clough, P.J. Adherence to sport injury rehabilitation programs: An integrated psycho-social approach. Scand. J. Med. Sci. Sports 2008, 18, 798–809. [Google Scholar] [CrossRef] [PubMed]
- Smith, T.Q.; Mitroff, S.R. Stroboscopic Training Enhances Anticipatory Timing. Int. J. Exerc. Sci. 2012, 5, 344–353. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Balance Training (n = 25) | Stroboscopic Vision (n = 24) | Control (n = 24) | p-Value | |
|---|---|---|---|---|---|
| Age (years) | 29.76 ± 10.009 | 27.38 ± 7.383 | 29.67 ± 9.407 | 0.755 | |
| Height (cm) | 167.48 ± 22.946 | 170.63 ± 8.791 | 170.50 ± 9.758 | 0.963 | |
| Mass (kg) | 73.22 ± 21.122 | 71.94 ± 9.891 | 69.38 ± 9.188 | 0.374 | |
| Gender | Male | 12/48% | 17/70.83% | 13/54.17% | 0.249 |
| Female | 13/52% | 7/29.17% | 11/45.83% | ||
| Occupational status | 0.724 | ||||
| Full-Time worker | 18/72% | 16/66.6% | 19/79.16% | ||
| Part-time worker | 2/8% | 1/4.16% | 2/8.33% | ||
| unemployed | 5/20% | 7/29.16% | 3/12.5% | ||
| Education | 0.912 | ||||
| Primary | 4/16% | 5/20.83% | 4/16.6% | ||
| Secondary | 8/32% | 10/41.26% | 11/45.83% | ||
| University | 13/52% | 9/37.5% | 9/37.5% | ||
| Affected ankle | Left | 12/48% | 9/37.5% | 11/45.83% | 0.738 |
| Right | 13/52% | 15/62.5% | 13/54.17% | ||
| DFROM | 8.348 ± 2.854 | 6.733 ± 2.886 | 8.821 ± 0.8876 | 0.317 | |
| SEBT-Ant | 78.016 ± 3.519 | 77.337 ± 4.748 | 74.929 ± 2.8403 | 0.124 | |
| SEBT-PM | 85.524 ± 4.350 | 83.238 ± 5.045 | 83.208 ± 4.4112 | 0.271 | |
| SEBT-PL | 84.252 ± 4.823 | 81.871 ± 6.884 | 80.946 ± 4.7340 | 0.089 | |
| CAIT | 15.28 ± 4.650 | 15.13 ± 4.803 | 15.29 ± 5.645 | 0.934 | |
| FAAM-ADL | 79.60 ± 6.278 | 74.04 ± 8.175 | 72.50 ± 9.325 | 0.067 | |
| FAAM-Sport | 69.60 ± 6.278 | 69.17 ± 6.197 | 67.29 ± 6.252 | 0.232 |
| Progression 1 | Progression 2 | Progression 3 | |
|---|---|---|---|
| Crossed arms, single-limb stance on the floor (60”) | Crossed arms, single-limb stance on a mat (30”) | Crossed arms, single-limb stance on a mat (60”) | Crossed arms, single-limb stance on a dynair (30”) |
| Throwing/catching a ball. single-limb on the floor (10 repetitions) | Throwing/catching a ball. Single-limb on a mat (10 repetitions) | Throwing/catching a ball. Single-limb on a dynair (10 repetitions) | Throwing/catching a ball. Single-limb on a bosu (10 repetitions) |
| Single leg deadlift with open arms (10 repetitions) | Single leg deadlift with hands at the hip (10 repetitions) | Single leg deadlift with a lightweight (10 repetitions) | Single leg deadlift reaching 3 points (10 repetitions) |
| Lateral hop to stabilization hands at the hip (10 repetitions) | Lateral hop to stabilization with hands at the hip (10 repetitions) (30 cm) | Lateral hop to stabilization with hands at the hip (10 repetitions) (45 cm) | Lateral hop to stabilization with hands at the hip (10 repetitions) (1 m) |
| Back and forward hop to stabilization with hands at the hip (10 repetitions) | Back and forward hop to stabilization with hands at the hip (10 repetitions) (30 cm) | Back and forward hop to stabilization with hands at the hip (10 repetitions) (45 cm) | Back and forward hop to stabilization with hands at the hip (10 repetitions) (1 m) |
| Randomized hop to stabilization in 4 directions (10 repetitions) | Increasing the speed during the performance (physiotherapist randomly indicates the direction). | ||
| Circuit was repeated two times with 30” of rest between exercises and 2′ of rest between each circuit. | |||
| Within-Group Change Scores | Between-Group Differences in Change Scores | |||||||
|---|---|---|---|---|---|---|---|---|
| Variable | Baseline Mean ± SD | End of Treatment Mean ± SD | Mean (95% CI) | p-Value | d-Cohen | Mean (95% CI) | p-Value | d-Cohen |
| DFROM | ||||||||
| Games–Howell | Kruskal–Wallis → p = 0.000 | |||||||
| BT | 8.348 ± 2.854 | 10.016 ± 2.637 | −1.6680 (−2.1876, −1.1484) | 0.000 | 0.607 | BT-BTSV: −0.302 (−1.3995, 0.793) | 0.781 | BT-BTSV: 0.192 |
| BTSV | 6.733 ± 2.886 | 8.704 ± 2.927 | −1.9708 (−2.7444, −1.1973) | 0.000 | 0.678 | BT-CG: 1.681 (1.046, 2.314) | 0.000 | BT-CG: 1.869 |
| CG | 8.821 ± 0.887 | 8.808 ± 0.876 | 0.0125 (−0.0625, 0.0875) | 0.734 | 0.014 | BTSV-CG: 1.983 (1.043, 2.923) | 0.000 | BTSV-CG: 1.523 |
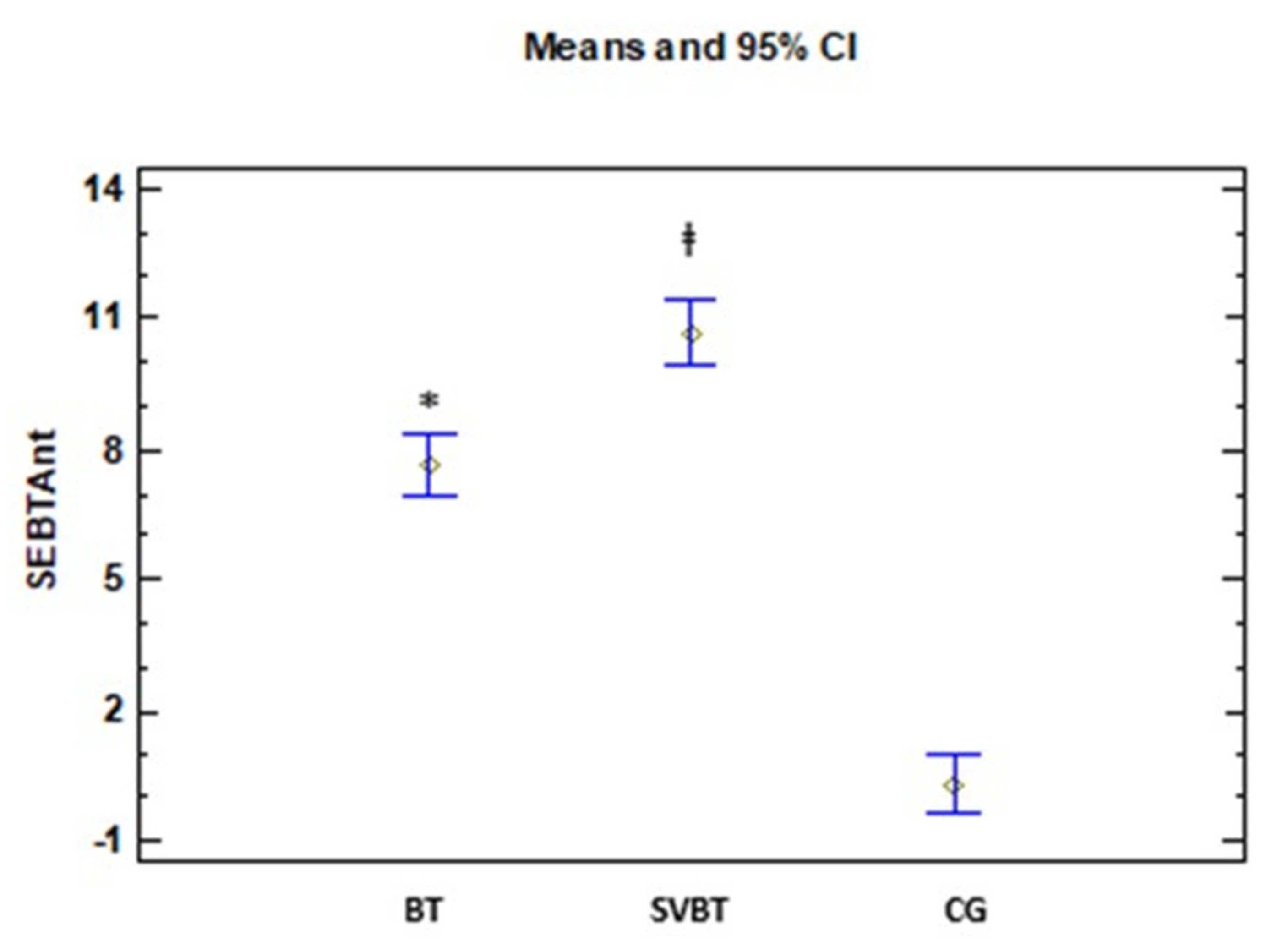
| SEBT-Ant | ||||||||
| Games–Howell | Kruskal–Wallis → p = 0.000 | |||||||
| BT | 78.016± 3.519 | 85.668± 3.481 | −7.6520 (−8.0262, −7.2778) | 0.000 | 2.185 | BT-BTSV: −3.039 (−4.801, −1.278) | 0.001 | BT-BTSV: 1.235 |
| BTSV | 77.337 ± 4.748 | 88.029 ± 3.979 | −10.6917 (−12.1100, −9.2734) | 0.000 | 2.440 | BT-CG: 7.335 (6.683, 7.987) | 0.000 | BT-CG: 7.787 |
| CG | 74.929 ± 2.840 | 75.246 ± 2.822 | −0.3167 (−0.7288, 0.0955) | 0.126 | 0.112 | BTSV-CG: 10.375 (8.604, 12.145) | 0.000 | BTSV-CG: 4.194 |
| SEBT-PM | ||||||||
| Games–Howell | Kruskal–Wallis → p = 0.000 | |||||||
| BT | 85.524 ± 4.350 | 92.228 ± 3.570 | −6.7040 (−8.0703, −5.3377) | 0.000 | 1.684 | BT-BTSV: −2.533 (−6.245, 1.178) | 0.230 | BT-BTSV: 0.481 |
| BTSV | 83.238 ± 5.045 | 92.475 ± 4.965 | −9.2375 (−12.0535, −6.4215) | 0.000 | 1.845 | BT-CG: 6.199 (3.738, 8.661) | 0.000 | BT-CG: 1.746 |
| CG | 83.208 ± 4.411 | 83.713 ± 6.131 | −0.5042 (−2.0985, 1.0901) | 0.519 | 0.094 | BTSV-CG: 8.733 (4.911, 12.555) | 0.000 | BTSV-CG: 1.611 |
| SEBT-PL | ||||||||
| Games–Howell | Kruskal–Wallis → p = 0.000 | |||||||
| BT | 84.252 ± 4.823 | 90.708 ± 4.460 | −6.4560 (−8.4358, −4.4762) | 0.000 | 1.389 | BT-BTSV: −1.960(−5.708, 1.787) | 0.420 | BT-BTSV: 0.363 |
| BTSV | 81.871 ± 6.884 | 90.288 ± 2.958 | −8.4167 (−10.9235, −5.9099) | 0.000 | 1.588 | BT-CG: 5.514 (2.886, 8.142) | 0.000 | BT-CG: 1.457 |
| CG | 80.946 ± 4.734 | 81.888 ± 4.238 | −0.9417 (−1.9420, 0.0587) | 0.064 | 0.209 | BTSV-CG: 7.475 (4.259, 10.690) | 0.000 | BTSV-CG: 1.653 |
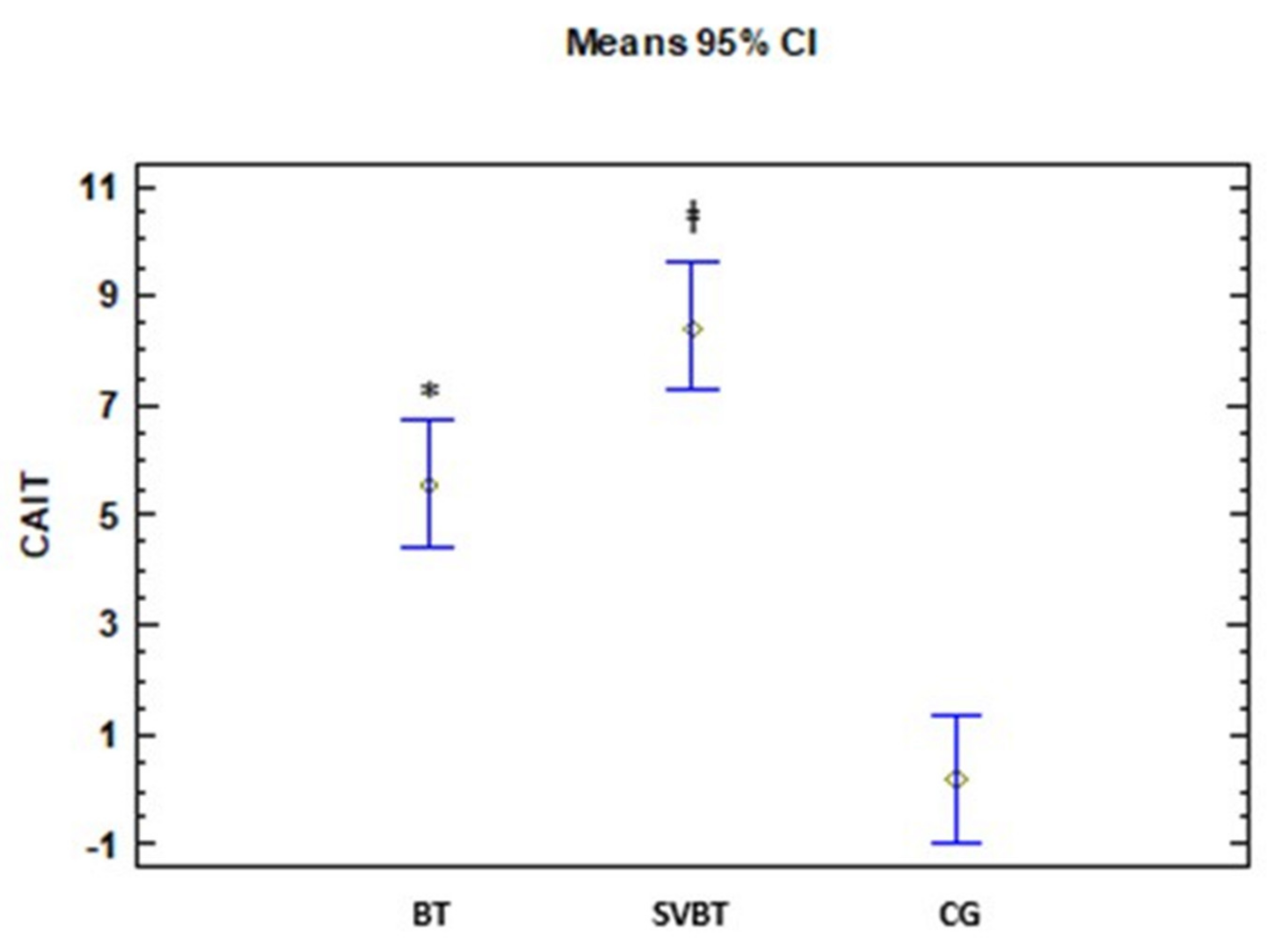
| CAIT | ||||||||
| Games–Howell | Kruskal–Wallis → p = 0.000 | |||||||
| BT | 15.282 ± 4.650 | 20.840 ± 4.696 | −5.560 (−6.898, −4.222) | 0.000 | 1.189 | BT-BTSV: −2.856 (−5.629, −0.084) | 0.042 | BT-BTSV: 0.718 |
| BTSV | 15.137 ± 4.803 | 23.541 ± 2.843 | −8.417 (−10.357, −6.476) | 0.000 | 2.130 | BT-CG: 5.351 (3.557, 7.146) | 0.000 | BT-CG: 2.069 |
| CG | 15.290 ± 5.645 | 15.503 ± 4.987 | −0.208 (−0.923, 0.507) | 0.553 | 0.039 | BTSV-CG: 8.208 (5.739, 10.676) | 0.000 | BTSV-CG: 2.370 |
| FAAM-ADL | ||||||||
| Games–Howell | Kruskal–Wallis → p = 0.000 | |||||||
| BT | 79.602 ± 6.278 | 86.800 ± 8.021 | −7.200 (−9.935, −4.465) | 0.000 | 0.999 | BT-BTSV: −4.383 (−9.826, 1.059) | 0.136 | BT-BTSV: 0.560 |
| BTSV | 74.044 ± 8.175 | 85.630 ± 5.578 | −11.583 (−15.323, −7.844) | 0.000 | 1.656 | BT-CG: 6.783 (3.087, 10.479) | 0.000 | BT-CG: 1.273 |
| CG | 72.500 ± 9.325 | 72.920 ± 9.315 | −0.417 (−1.931, 1.098) | 0.575 | 0.045 | BTSV-CG: 11.166 (6.361, 15.971) | 0.000 | BTSV-CG: 1.652 |
| FAAM-sport | ||||||||
| Games–Howell | Kruskal–Wallis → p = 0.000 | |||||||
| BT | 69.602 ± 6.278 | 86.000 ± 6.124 | −16.400 (−18.508, −14.292) | 0.000 | 2.644 | BT-BTSV: −1.5166(−6.468, 3.434) | 0.737 | BT-BTSV: 0.214 |
| BTSV | 69.174 ± 6.197 | 87.080 ± 7.506 | −17.917 (−21.543, −14.291) | 0.000 | 2.602 | BT-CG: 15.983 (12.933, 19.033) | 0.000 | BT-CG: 3.622 |
| CG | 67.290 ± 6.252 | 67.710 ± 6.252 | −0.417 (−1.931, 1.098) | 0.575 | 0.067 | BTSV-CG: 17.500 (12.823, 22.176) | 0.000 | BTSV-CG: 2.659 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, K.-M.; Estudillo-Martínez, M.D.; Castellote-Caballero, Y.; Estepa-Gallego, A.; Cruz-Díaz, D. Short-Term Effects of Balance Training with Stroboscopic Vision for Patients with Chronic Ankle Instability: A Single-Blinded Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2021, 18, 5364. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18105364
Kim K-M, Estudillo-Martínez MD, Castellote-Caballero Y, Estepa-Gallego A, Cruz-Díaz D. Short-Term Effects of Balance Training with Stroboscopic Vision for Patients with Chronic Ankle Instability: A Single-Blinded Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2021; 18(10):5364. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18105364
Chicago/Turabian StyleKim, Kyung-Min, María D. Estudillo-Martínez, Yolanda Castellote-Caballero, Alejandro Estepa-Gallego, and David Cruz-Díaz. 2021. "Short-Term Effects of Balance Training with Stroboscopic Vision for Patients with Chronic Ankle Instability: A Single-Blinded Randomized Controlled Trial" International Journal of Environmental Research and Public Health 18, no. 10: 5364. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18105364