
An Evaluation of Two Systems for the Management of the Microbiological Quality of Water in Dental Unit Waterlines: Hygowater® and IGN Calbénium®


Abstract
:1. Introduction
2. Material and Methods
2.1. Dental Units and Disinfection Systems
2.2. Water Samples and Chlorine Follow-Up
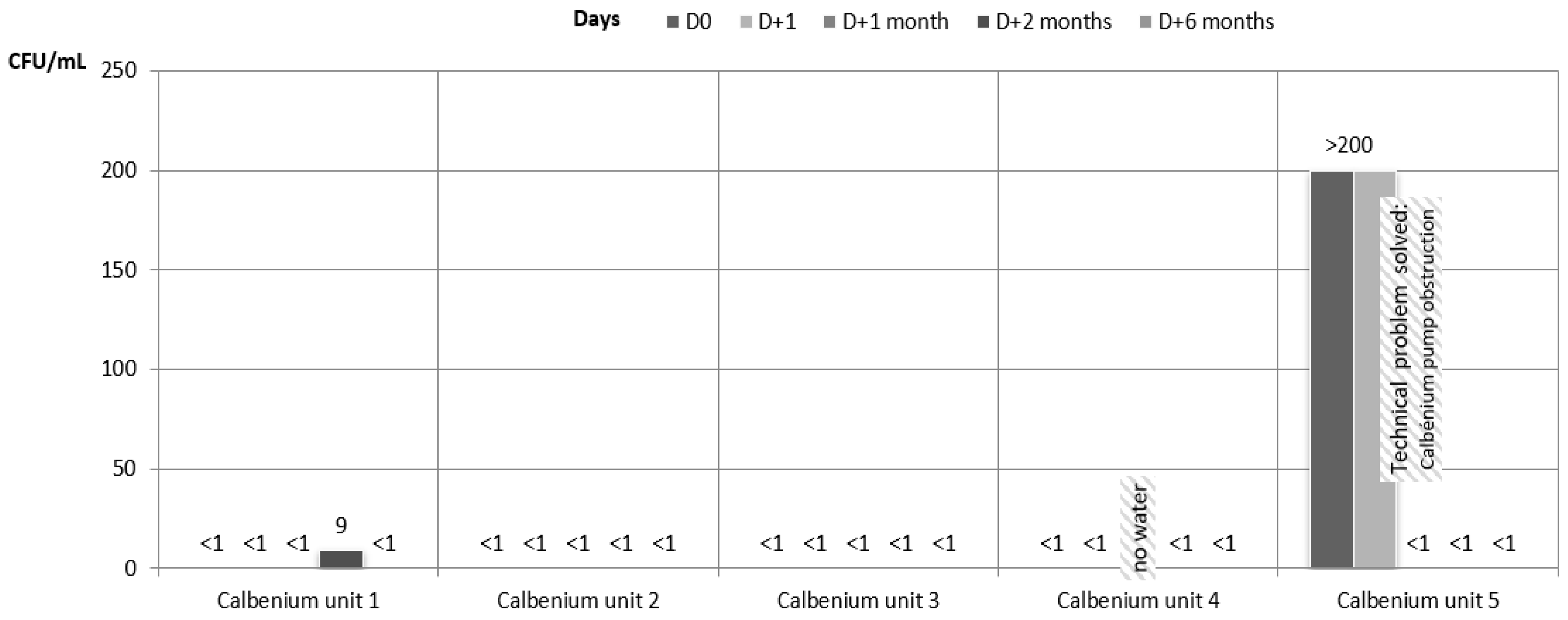
- D0, just before the installation of the Hygowater® system. At this moment, the 5 dental units which were then connected to the Hygowater® system did not benefit from any treatment. The 5 other dental units had already been connected to the IGN Calbenium® system for 1 year (1 unit), 4 years (2 units), or 5 years (2 units).
- D + 1, one day after the installation of the Hygowater® system.
- D + 14, only for the 5 units with the Hygowater® system.
- D + 1 month, D + 2 months, and D + 6 months for every dental unit.
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Costa, D.; Girardot, M.; Bertaud, J.; Verdon, J.; Imbert, C. Efficacy of dental unit waterlines disinfectants on a plymicrobial biofilm. Water Res. 2016, 91, 38–44. [Google Scholar] [CrossRef]
- Barbeau, J.; Buhler, T. Biofilms augment the number of free-living amoebae in dental unit waterlines. Res. Microbiol. 2001, 152, 753–760. [Google Scholar] [CrossRef]
- Arvand, M.; Hack, A. Microbial contamination of dental unit waterlines in dental practices in Hesse, Germany: A cross-sectional study. Eur. J. Microbiol. Immunol. 2013, 3, 49–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Offner, D.; Fioretti, F.; Musset, A.M. Contamination of dental unit waterlines: Assessment of three continuous water disinfection systems. BDJ Open 2016, 2, 16007. [Google Scholar] [CrossRef] [PubMed]
- Walker, J.T.; Marsh, P.D. Microbial biofilm formation in DUWS and their control using disinfectants. J. Dent. 2017, 35, 721–730. [Google Scholar] [CrossRef] [PubMed]
- Baudet, A.; Lizon, J.; Martrette, J.M.; Camelot, F.; Florentin, A.; Clément, C. Dental unit waterlines: A survey of practices in eastern France. Int. J. Environ. Res. Public Health 2019, 16, 4242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pasquarella, C.; Veronesi, L.; Napoli, C.; Castiglia, P.; Liguori, G.; Rizzetto, R.; Torre, I.; Righi, E.; Farruggia, P.; Tesauro, M.; et al. Microbial environmental contamination in Italian dental clinics: A multicenter study yielding recommendations for standardized sampling methods and threshold values. Sci. Total Environ. 2012, 420, 289–299. [Google Scholar] [CrossRef] [PubMed]
- Rogers, J.; Dowsett, A.B.; Dennis, P.J.; Lee, J.V.; Keevil, C.W. Influence of plumbing materials on biofilm formation and growth of Legionella pneumophilia in potable water systems. Appl. Environ. Microbiol. 1994, 60, 1842–1851. [Google Scholar] [CrossRef] [Green Version]
- Coleman, D.C.; O’Donnell, M.J.; Shore, A.C.; Russell, R.J. Biofilm problems in dental unit water systems and its practical control. J. Appl. Microbiol. 2008, 106, 1424–1437. [Google Scholar] [CrossRef]
- Farah, R.F.I. Effect of cooling water temperature on the temperature changes in pulp chamber and at handpiece head during high-speed tooth preparation. Restor. Dent. Endod. 2018, 44, e3. [Google Scholar] [CrossRef]
- Sinjari, B.; D’Addazio, G.; Bozzi, M.; Santilli, M.; Traini, T.; Murmura, G.; Caputi, S. SEM Analysis of Enamel Abrasion after Air Polishing Treatment with Erythritol, Glycine and Sodium Bicarbonate. Coatings 2019, 9, 549. [Google Scholar] [CrossRef] [Green Version]
- Smith, G.; Smith, A. Microbial contamination of used dental handpieces. Am. J. Infect. Control 2014, 42, 1019–1021. [Google Scholar] [CrossRef] [PubMed]
- Offner, D.; Brisset, L.; Musset, A.M. Evaluation of the mechanical cleaning efficacy of dental handpieces. J. Hosp. Infect. 2019, 103, e73–e80. [Google Scholar] [CrossRef] [PubMed]
- Petti, S.; Moroni, C.; Messano, G.A.; Polimeni, A. Detection of oral streptococci in dental unit water lines after therapy with air turbine handpiece: Biological flui retractation more frequent than expected. Future Microbiol. 2013, 8, 413–421. [Google Scholar] [CrossRef] [PubMed]
- Zemouri, C.; de Soet, H.; Crielaard, W.; Laheij, A. A scoping review on bio-aerosols in healthcare and the dental environment. PLoS ONE 2017, 12, 0178007. [Google Scholar] [CrossRef]
- Offner, D.; Fernandez de Grado, G.; Strub, M.; Belotti, L.; Deboscker, S.; Musset, A.M. Mobile Dental Delivery System: An Effective Protocol for Hygiene and Disinfection. Int. J. Environ. Res. Public Health 2020, 17, 1603. [Google Scholar] [CrossRef] [Green Version]
- Ricci, M.L.; Fontana, S.; Pinci, F.; Fiumana, E.; Pedna, M.F.; Farolfi, P.; Sabattini, M.A.B.; Scaturro, M. Pneumonia associated with a dental unit waterline. Lancet 2012, 379, 684. [Google Scholar] [CrossRef]
- Schönning, C.; Jernberg, C.; Klingenberg, D.; Andersson, S.; Pääjärvi, A.; Alm, E.; Tano, E.; Lytsy, B. Legionellosis acquired through a dental unit: A case study. J. Hosp. Infect. 2017, 96, 89–92. [Google Scholar] [CrossRef]
- Hatzenbuehler, L.A.; Tobin-D’Angelo, M.; Drenzek, C.; Peralta, G.; Cranmer, L.C.; Anderson, E.J.; Milla, S.S.; Abramowicz, S.; Yi, J.; Hilinski, J.; et al. Pediatric dental clinic-associated outbreak of mycobacterium abscessus infection. J. Pediatric Infect. Dis. Soc. 2017, 6, e116–e122. [Google Scholar] [CrossRef]
- Baudet, A.; Lizon, J.; Martrette, J.M.; Camelot, F.; Florentin, A.; Clément, C. Efficacy of BRS® and Alpron®/Bilpron® disinfectants for dental unit waterlines: A six-year study. Int. J. Environ. Res. Public Health 2020, 17, 2634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chate, R.A.C. An audit improves the quality of water within the dental unit waterlines of general dental practices across the East of England. Br. Dent. J. 2010, 209, E11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schel, A.J.; Marsh, P.D.; Bradshaw, D.J.; Finney, M.; Fulford, M.R.; Frandsen, E.; Østergaard, E.; Ten Cate, J.M.; Moorer, W.R.; Mavridou, A.; et al. Comparison of the efficacies of disinfectants to control microbial contamination in dental unit water systems in general dental practices across the European Union. Appl. Environ. Microbiol. 2006, 72, 1380–1387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zemouri, C.; de Soet, J.J.; Volgenant, C.M.C.; Crielaard, W.; Laheij, A.M.G.A. Heterogeneity in the efficacy of dental chemical disinfectants on water-derived biofilms in vitro. Biofouling 2020, 36, 587–596. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.J.; McHugh, S.; Aitken, I.; Hood, J. Evaluation of the efficacy of Alpron disinfectant for dental unit water lines. Br. Dent. J. 2002, 193, 593–596. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Munive-Degregori, A.; Mayta-Tovalino, F.; Gallo, W.; Luza, S.; Mauricio, F.; Ilizarbe, S.; Munive-Méndez, A. Evaluation of hydrogen peroxide and cetylpyrimidium chloride as bacterial decontaminants of dental unit water lines at a private Peruvian dental school. J. Int. Soc. Prevent. Community Dent. 2020, 10, 731–735. [Google Scholar]
- European Council. Council directive 98/83/EC of 3 November 1998 on the quality of water intended for human consumption. Off. J. Eur. Commun. 1998, L330, 32–54. [Google Scholar]
- Ministère de la Santé, D.G.S. Guide de Prévention des Infections Liées Aux Soins en Chirurgie Dentaire et en Stomatologie. 2006. Available online: http://social-sante.gouv.fr/IMG/pdf/Guide_de_prevention_des_infections_liees_aux_soins_en_chirurgie_dentaire_et_en_stomatologie.pdf (accessed on 15 March 2021).
- Association Dentaire Française (ADF). Grille Technique D’évaluation Pour la Prévention des Infections Associées aux Soins. 2006. Available online: https://adf.asso.fr/articles/grille-technique-d-evaluation-pour-la-prevention-des-infections (accessed on 18 May 2021).
- ISO 6222. Water Quality—Enumeration of Culturable Micro-Organisms—Colony Count by Inoculation in a Nutrient Agar Culture Medium; International Standard Organization: Geneva, Switzerland, 1999. [Google Scholar]
- ISO 9308-1. Water Quality—Enumeration of Escherichia Coli and Coliform Bacteria—Part 1: Membrane Filtration Method for Waters with Low Bacterial Background Flora; International Standard Organization: Geneva, Switzerland, 2014. [Google Scholar]
- ISO 16266. Water Quality—Detection and Enumeration of Pseudomonas Aeruginosa—Method by Membrane Filtration; International Standard Organization: Geneva, Switzerland, 2006. [Google Scholar]
- Statement on Dental Unit Waterlines. American Dental Association. 20 March 2019. Available online: https://www.ada.org/en/member-center/oral-health-topics/dental-unit-waterlines (accessed on 15 March 2021).
- Bednarsh, H.S.; Eklund, K.J.; Mills, S. Denta Unit Waterlines: Check Your Dental Unit Water IQ. 1997. Available online: https://www.osap.org/page/Issues_DUWL_7XXXX/Dental-Unit-Waterlines.htm (accessed on 15 March 2021).
- Vandini, A.; Temmerman, R.; Frabetti, A.; Caselli, E.; Antonioli, P.; Balboni, P.G.; Platano, D.; Branchini, A.; Mazzacane, S. Hard surface biocontrol in hospitals using microbial-based cleaning products. PLoS ONE 2014, 9, e108598. [Google Scholar] [CrossRef] [Green Version]
- Al-Marzooq, F.; Al Bayat, S.; Sayyar, F.; Ishaq, H.; Nasralla, H.; Koutaich, R.; Al Kawas, S. Can probiotic cleaning solutions replace chemical disinfectants in dental clinics? Eur. J. Dent. 2018, 12, 532–539. [Google Scholar] [CrossRef]
- Patini, R.; Cattani, P.; Marchetti, S.; Isola, G.; Quaranta, G.; Gallenzi, P. Evaluation of predation capability of periodontopathognes bacteria by Bdellovibrio bacteriovorus HD100. An in vitro study. Materials 2019, 12, 2008. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Microorganisms Sought | Volume Analyzed | Maximum Storage Duration Before Analysis Recommended (h) | Maximum Storage Duration Before Analysis Accepted (h) | Storage Temperature (°C) Before Analysis | Samples’ Seeding Conditions | Standards |
|---|---|---|---|---|---|---|
| viable aerobic MO at 22 °C | 1 mL | 8 | 12 | 5 ± 3 | 72 h at 22 °C on agar PCA by inclusion | ISO 6222 [29] |
| viable aerobic MO at 37 °C | 1 mL | 8 | 12 | 5 ± 3 | 48 h at 36 °C on agar PCA by inclusion | ISO 6222 [29] |
| Coliform bacteria and E. coli | 100 mL | 8 | 18 | 5 ± 3 | 24 h at 36 °C on agar TTC by membrane filtration, 2nd inspection after 48 h | ISO 9308-1 [30] |
| Pseudomonas aeruginosa | 100 mL | 8 | 12 | 5 ± 3 or ambient (≤25) | 48 h at 36 °C on cetrimide agar by membrane filtration | ISO 16266 [31] |
| D0 | D + 14 | D + 1 Month | D + 2 Months | D + 6 Months | |
|---|---|---|---|---|---|
| Hygowater unit 1 | Acidovorax temperans Sphingomonas sp. | Sphingomonas sp. Chryseobacterium sp. | Cupriavidus metallidurans | - | Blastomonas sp. Methylobacterium sp. |
| Hygowater unit 2 | Acidovorax temperans Sphingomonas sp. | - | - | - | - |
| Hygowater unit 3 | Acidovorax temperans Novosphingobium sp. Blastomonas sp. Sphingomonas sp. | Sphingomonas sp. | Blastomonas sp. Cupriavidus metallidurans | - | Methylobacterium sp. |
| Hygowater unit 4 | Acidovorax temperans Blastomonas sp. Sphingomonas sp. | Sphingomonas sp. Cupriavidus metallidurans | Blastomonas sp. Methylobacterium sp. | Blastomonas sp. | Sphingomonas sp. Methylobacterium sp. |
| Hygowater unit 5 | Blastomonas sp. Sphingomonas sp. | Blastomonas sp. Sphingomonas sp. Chryseobacterium sp. | - | - | Chryseobacterium sp. Sphingomonas sp. Cupriavidus sp. |
| Calbenium unit 2 | - | - | - | - | Methylobacterium sp. |
| Calbenium unit 5 | Stenotrophomonas maltophilia | - | - | - | - |
| Weeks | Hygowater Unit 1 | Hygowater Unit 2 | Hygowater Unit 3 | Hygowater Unit 4 | Hygowater Unit 5 |
|---|---|---|---|---|---|
| 0 | 0.8 | 0.8 | 0.8 | 0.8 | 0.8 |
| 1 | 0.3 | no water | 0.4 | 0.3 | 0.6 |
| 2 | 0.8 | 0.4 | 0.6 | 0.4 | 0.8 |
| 3 | 0.8 | 0.4 | 1 | 0.6 | 0.8 |
| 4 | 0.8 | 0.4 | 0.8 | 0.8 | 0.6 |
| 5 | 0.6 | 0.4 | 0.6 | 0.4 | 0.8 |
| 6 | 0.8 | 0.4 | no water | 0.4 | 0.6 |
| 7 | 0.8 | 0.4 | 0.8 | 0.4 | 0.6 |
| 8 | 1 | 0.4 | 0.6 | 0.4 | 0.8 |
| 9 | 0.8 | 0.4 | 0.6 | 0.4 | 0.6 |
| 10 | 0.8 | 0.4 | 0.6 | 0.4 | 0.6 |
| 11 | 0.8 | 0.4 | 0.4 | 0.4 | 0.6 |
| 12 | ND | ND | ND | ND | ND |
| 13 | ND | ND | ND | ND | ND |
| 14 | 1 | 0.6 | 0.8 | 0.6 | 0.4 |
| 15 | 0.8 | 0.4 | 0.6 | 0.4 | 0.6 |
| 16 | 1 | 0.4 | 0.4 | 0.6 | 0.6 |
| 17 | 1 | 0.4 | 0.4 | 0.4 | 0.6 |
| 18 | 0.8 | 0.4 | 0.4 | 0.4 | 0.8 |
| 19 | 1 | 0.6 | 0.4 | 0.8 | 0.8 |
| 20 | 0.8 | 0.4 | 0.8 | 0.4 | 0.8 |
| 21 | 0.8 | 0.6 | 0.4 | 0.4 | 0.8 |
| 22 | 0.8 | 0.4 | 0.8 | 0.6 | 0.8 |
| 23 | 0.4 | 0.6 | 0.4 | 0.6 | 1 |
| 24 | 0.6 | 0.6 | 0.4 | 0.8 | 0.8 |
| 25 | 0.6 | 0.4 | 0.4 | 0.8 | 0.8 |
| Unit 1 | Unit 2 | Unit 3 | Unit 4 | Unit 5 | Mean Value | p-Value (Versus D0 in Hygowater System) | p-Value (Versus IGN Calbenium System) | ||
|---|---|---|---|---|---|---|---|---|---|
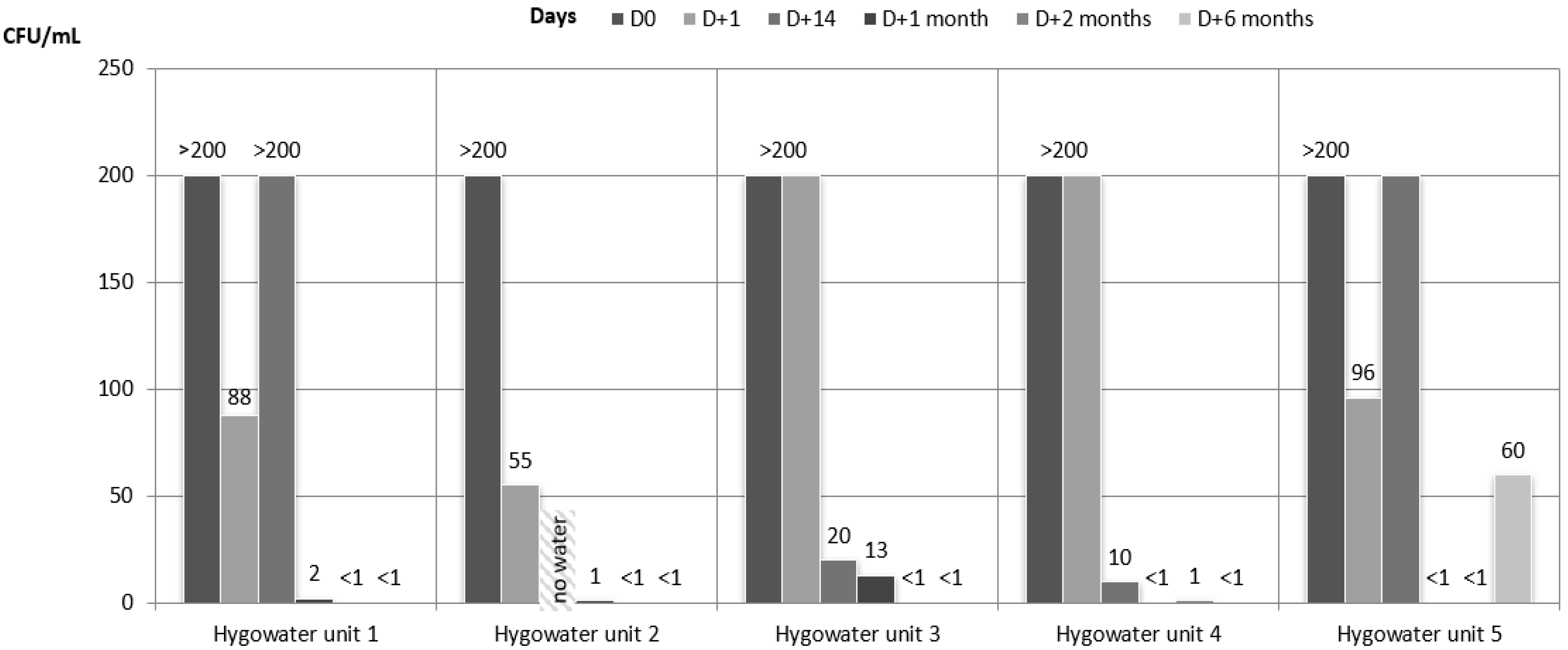
| HPC 22 °C | D0 | >200 | >200 | >200 | >200 | >200 | >200 | *** | |
| D + 1 | 88 | 55 | 200 | 200 | 96 | 127.8 | NS | * | |
| D + 14 | 200 | N/A | 20 | 10 | 200 | 107.5 | NS | N/A | |
| D + 1 month | 2 | 1 | 13 | <1 | <1 | 3.2 | *** | NS | |
| D + 2 months | <1 | <1 | <1 | 1 | <1 | 0.2 | *** | NS | |
| D + 6 months | <1 | <1 | <1 | <1 | 60 | 12 | *** | NS | |
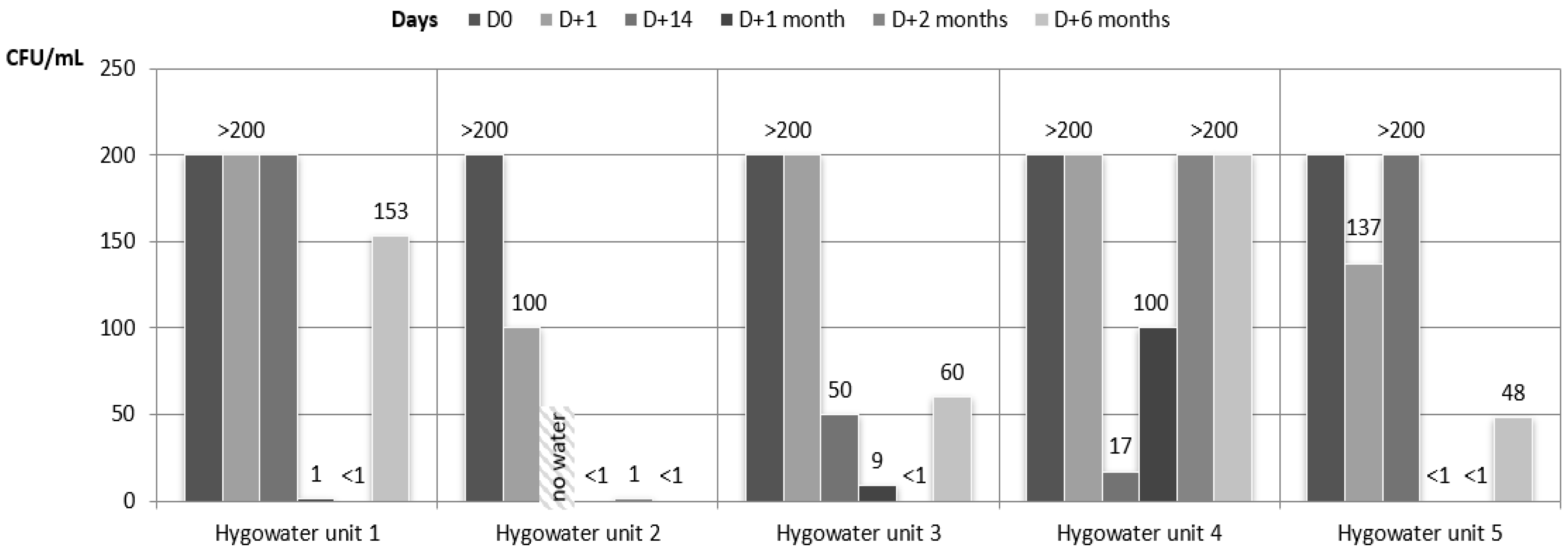
| HPC 37 °C | D0 | >200 | >200 | >200 | >200 | >200 | >200 | *** | |
| D + 1 | 200 | 100 | 200 | 200 | 137 | 167.4 | NS | ** | |
| D + 14 | 200 | N/A | 50 | 17 | 200 | 116.7 | NS | N/A | |
| D + 1 month | 1 | <1 | 9 | 100 | <1 | 22 | *** | NS | |
| D + 2 months | <1 | 1 | <1 | 200 | <1 | 40.2 | * | NS | |
| D + 6 months | 153 | <1 | 60 | 200 | 48 | 92.2 | * | NS | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Offner, D.; Musset, A.-M. An Evaluation of Two Systems for the Management of the Microbiological Quality of Water in Dental Unit Waterlines: Hygowater® and IGN Calbénium®. Int. J. Environ. Res. Public Health 2021, 18, 5477. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18105477
Offner D, Musset A-M. An Evaluation of Two Systems for the Management of the Microbiological Quality of Water in Dental Unit Waterlines: Hygowater® and IGN Calbénium®. International Journal of Environmental Research and Public Health. 2021; 18(10):5477. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18105477
Chicago/Turabian StyleOffner, Damien, and Anne-Marie Musset. 2021. "An Evaluation of Two Systems for the Management of the Microbiological Quality of Water in Dental Unit Waterlines: Hygowater® and IGN Calbénium®" International Journal of Environmental Research and Public Health 18, no. 10: 5477. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18105477