
The Health Impacts of Hazardous Chemical Exposures among Child Labourers in Low- and Middle-Income Countries


Abstract
:1. Introduction
1.1. Rationale
1.2. Objectives
- Conduct studies carried out between t chemical exposures, adverse health consequences, and the industries which put child labourers most at risk;
- Describe exposure and health outcome measurement issues;
- Identify the public health implications of chemical exposure among child labourers.
2. Materials and Methods
2.1. Search Strategy
2.2. Selection Criteria
- Studies carried out before the 1999 ILO “Worst Forms of Child Labour Convention (No.182)” [1]
- Studies carried out in HIC, for example United States
- Studies without a non-worker comparison group which included participants aged 18 or below
2.3. Data Extraction and Analysis
2.3.1. Exposure and Health Outcome Measurement
2.3.2. Chemical Exposure Definitions and Measurement
2.3.3. Health Outcomes Definitions and Measurement
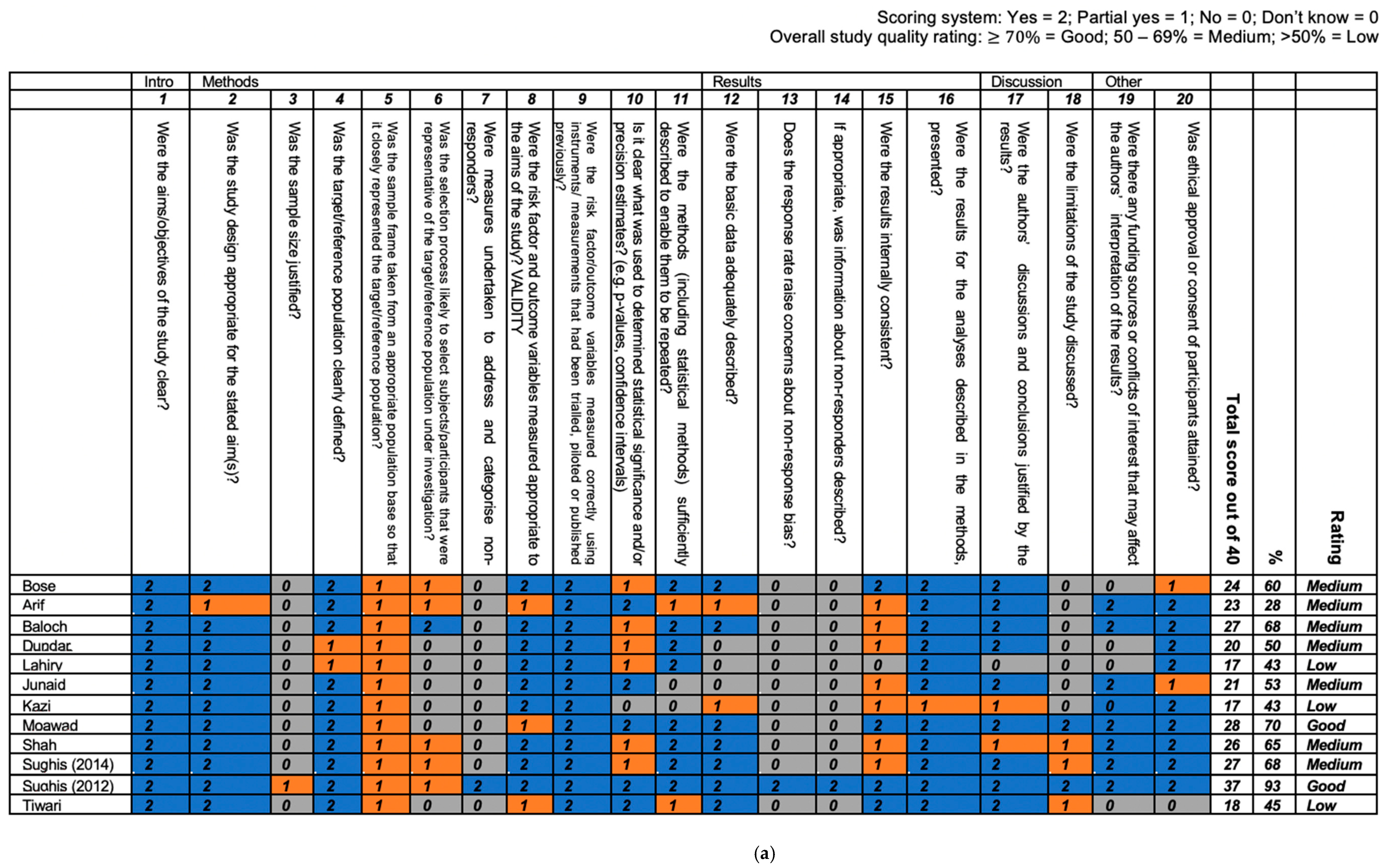
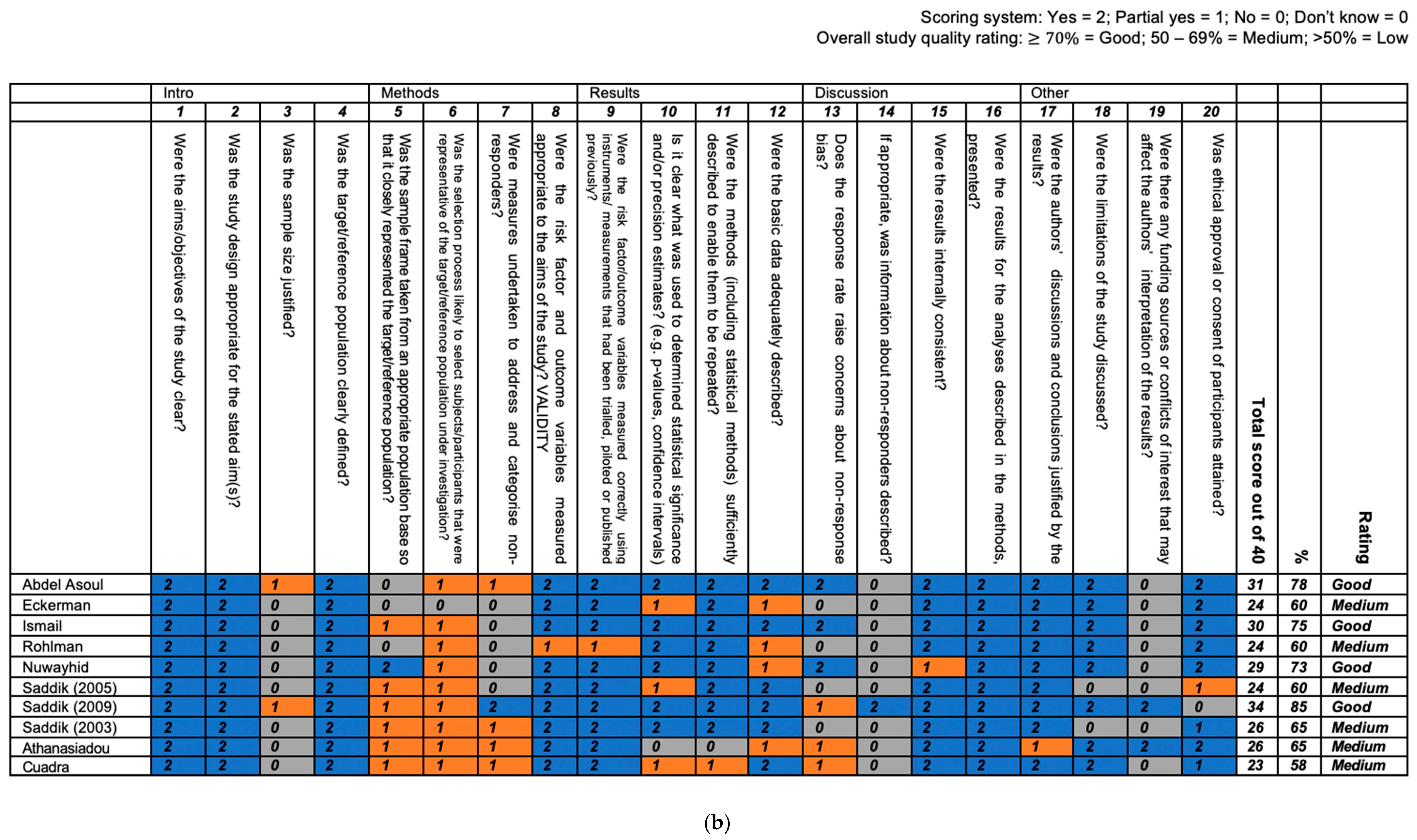
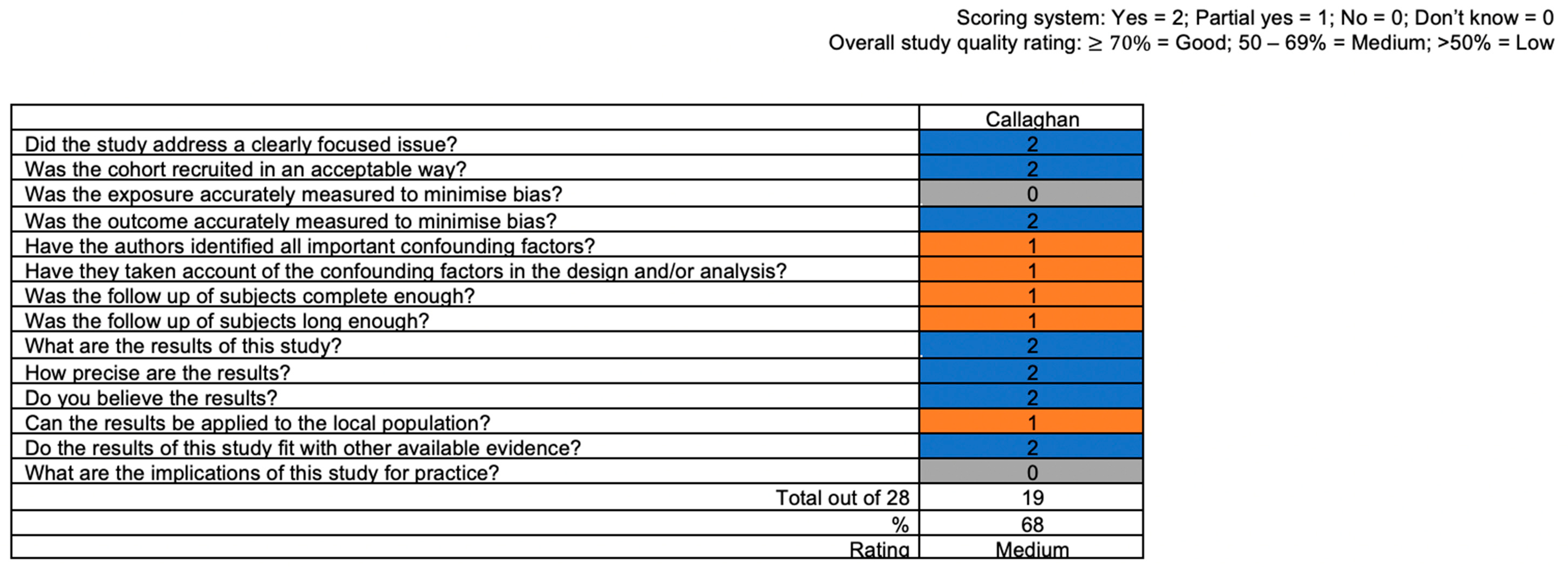
2.4. Quality Appraisal
3. Results
3.1. Characteristics of Included Studies
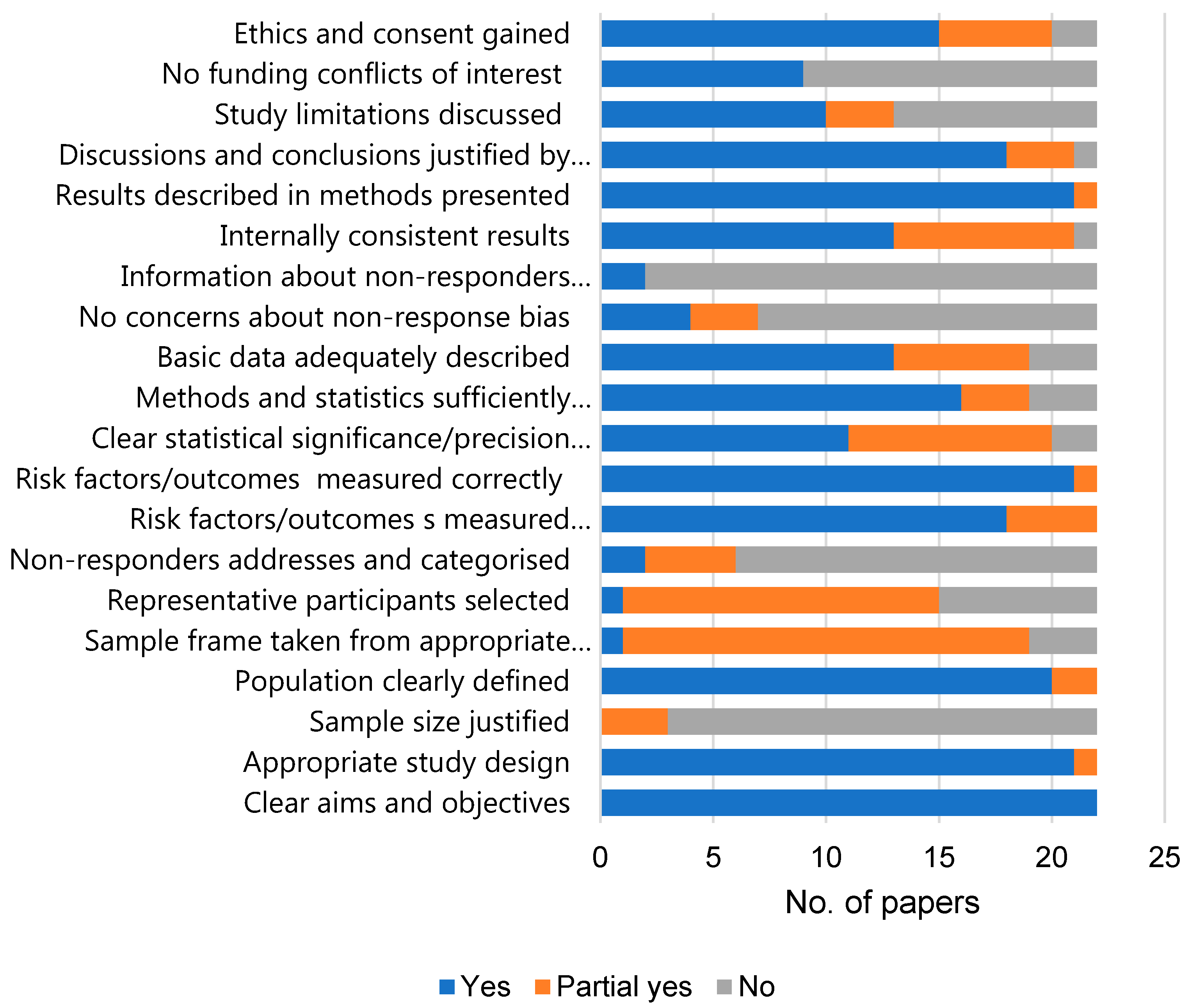
3.2. Quality Appraisal
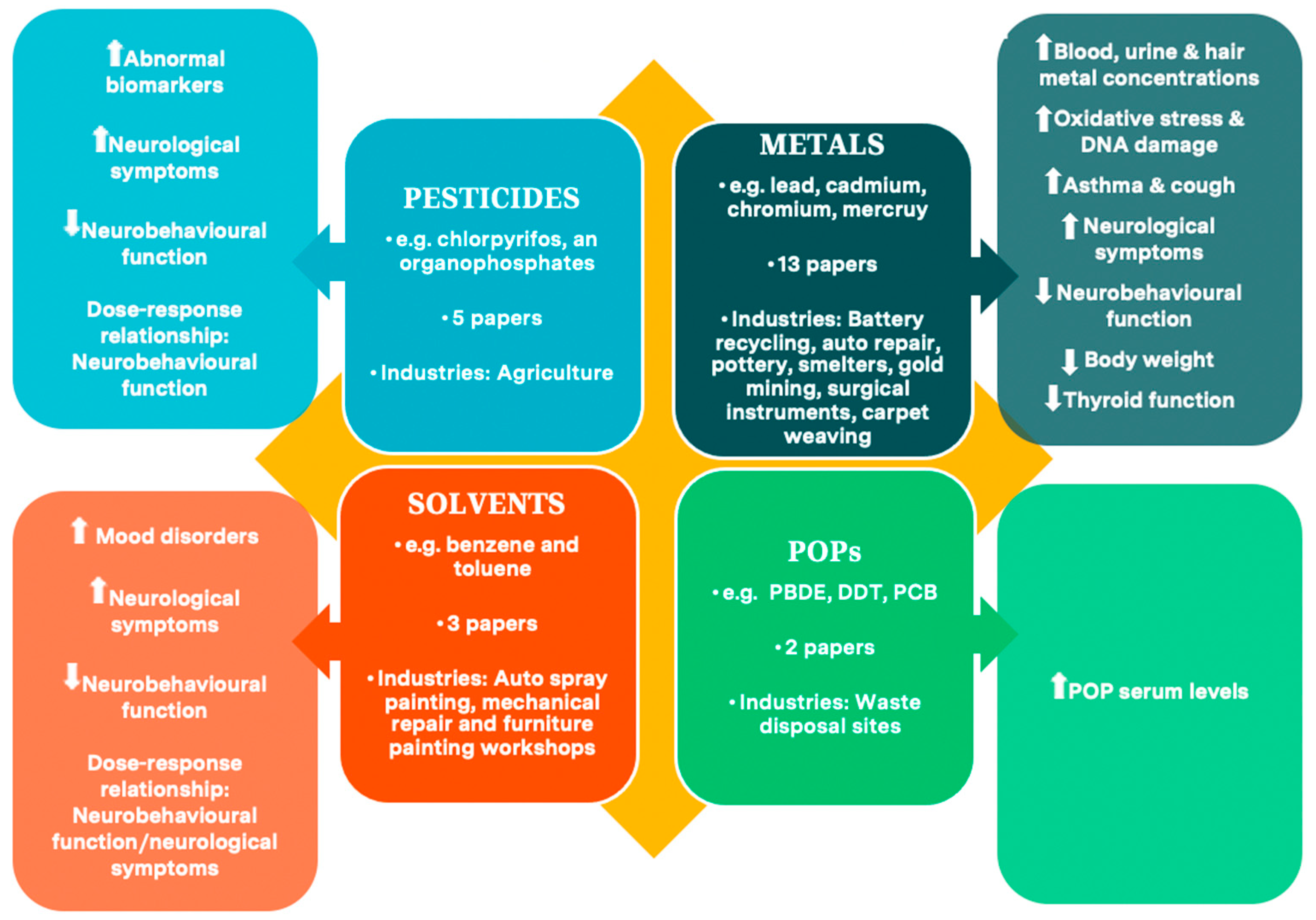
3.3. Evidence Synthesis of Health Outcomes by Chemical Type
3.3.1. Pesticides and Health Outcomes (n = 5)
3.3.2. Solvents and Health Outcomes (n = 3)
3.3.3. Metals and Health Outcomes (n = 13)
3.3.4. POPs and Health Outcomes (n = 2)
3.3.5. Health Outcomes Not Impacted by Chemicals
4. Discussion
4.1. Key Findings
4.2. Public Health Implications
- Cancer/malignancy—work-related cancers are the largest cause of workplace mortality in adults and account for 32% of deaths [78]. High levels of chromium, lead, and cadmium were identified in biomatrix samples from the working children in this review. This is of particular concern, as the IARC (2012) has classified cadmium and chromium as carcinogenic to humans and lead as probably carcinogenic [79]. Indeed, chromium is a recognised carcinogen [80] and has been linked with lung cancer [81] and increasing blood lead level has been associated with increased trends for lung and brain cancer [82]. Many pesticides have also been classified by IARC as carcinogenic or probably carcinogenic to humans, with cancer excesses observed for numerous cancers, including prostate, leukaemia, thyroid, and testicular cancer [83].
- Other health outcomes—studies of adult populations have linked lead with kidney and brain damage [84] and cadmium with irreversible kidney and lung damage [85]. Chromium has been associated with immunosuppression [81]. Elevated mercury levels were found in the child labourers included in this review. This is significant when considering that mercury can produce harmful effects on numerous body systems, including the nervous, digestive, and immune systems, as well as the lungs and kidneys [86]. Elevated blood POPs, such as PCBs, have been identified as endocrine disrupting chemicals and have been implicated in numerous reproductive disorders [87].
4.3. A sizeable Burden of Disease in Later Life
4.4. Measurement Challenges in Exposure and Outcome Assessments
4.4.1. Validity and Reliability of Self-Report Questionnaires for Measuring Exposures Is Unclear
4.4.2. Single Biomarker Assessment Is Inadequate for Accurate Measurement
4.4.3. Workplace Chemical Exposure Is Impossible to Isolate from Wider Environmental Exposures
4.5. Limitations of This Review
4.6. Priority Research Recommendations
4.7. Priority Interventions/Practices
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AChE | Acetylcholinesterase |
| BARS | Behavioural Assessment and Research System |
| BChE | Butyrylcholinesterase |
| BEI | Biological Exposure Indices |
| CASP | Critical Appraisal Skills Program |
| CDC | Centers for Disease Control and Prevention |
| CL | Child labour |
| DALYS | Disability-adjusted life years |
| FEV | Forced expiratory volume |
| FT4 | Free thyroxine |
| FVC | Forced vital capacity |
| HIC | High income countries |
| IARC | International Agency for Research on Cancer |
| ILO | International labour Organisation |
| IPM | Integrated Pest Management |
| LMIC | Low- and middle-income countries |
| OEL | Occupational Exposure Limits |
| OSH | Occupational Safety and Health |
| PIPS | Performance and information processing systems test battery |
| PM | Particulate matter |
| POMS | Profile of Mood States |
| POPs | Persistent organic pollutants |
| PPE | Personal protective equipment |
| TCPy | 3,5,6-trichloro-2-pyridinol |
| WAIS | Wechsler Adult Intelligence Scale |
| WHO | World Health Organisation |
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Section/Topic | # | Checklist Item | Reported in Section |
|---|---|---|---|
| Title | |||
| Title | 1 | Identify the report as a systematic review, meta-analysis, or both. | Title |
| Abstract | |||
| Structured summary | 2 | Provide a structured summary including, as applicable: background; objectives; data sources; study eligibility criteria, participants, and interventions; study appraisal and synthesis methods; results; limitations; conclusions and implications of key findings; systematic review registration number. | Abstract |
| Introduction | |||
| Rationale | 3 | Describe the rationale for the review in the context of what is already known. | Background |
| Objectives | 4 | Provide an explicit statement of questions being addressed with reference to participants, interventions, comparisons, outcomes, and study design (PICOS). | Background-objectives |
| Methods | |||
| Protocol and registration | 5 | Indicate if a review protocol exists, if and where it can be accessed (e.g., Web address), and, if available, provide registration information including registration number. | Methods-search strategy |
| Eligibility criteria | 6 | Specify study characteristics (e.g., PICOS, length of follow-up) and report characteristics (e.g., years considered, language, publication status) used as criteria for eligibility, giving rationale. | Methods-eligibility criteria |
| Information sources | 7 | Describe all information sources (e.g., databases with dates of coverage, contact with study authors to identify additional studies) in the search and date last searched. | Methods-search strategy |
| Search | 8 | Present full electronic search strategy for at least one database, including any limits used, such that it could be repeated. | Table A2 and Table A3 |
| Study selection | 9 | State the process for selecting studies (i.e., screening, eligibility, included in systematic review, and, if applicable, included in the meta-analysis). | Methods-study selection |
| Data collection process | 10 | Describe method of data extraction from reports (e.g., piloted forms, independently, in duplicate) and any processes for obtaining and confirming data from investigators. | Methods-data extraction and analysis |
| Data items | 11 | List and define all variables for which data were sought (e.g., PICOS, funding sources) and any assumptions and simplifications made. | Methods-Exposure and health outcome measurements |
| Risk of bias in individual studies | 12 | Describe methods used for assessing risk of bias of individual studies (including specification of whether this was done at the study or outcome level), and how this information is to be used in any data synthesis. | Methods-quality appraisal |
| Summary measures | 13 | State the principal summary measures (e.g., risk ratio, difference in means). | Methods-data extraction and analysis |
| Synthesis of results | 14 | Describe the methods of handling data and combining results of studies, if done, including measures of consistency (e.g., I2) for each meta-analysis. | Methods-data extraction and analysis |
| Risk of bias across studies | 15 | Specify any assessment of risk of bias that may affect the cumulative evidence (e.g., publication bias, selective reporting within studies). | Methods-quality appraisal |
| Additional analyses | 16 | Describe methods of additional analyses (e.g., sensitivity or subgroup analyses, meta-regression), if done, indicating which were pre-specified. | n/a |
| Results | |||
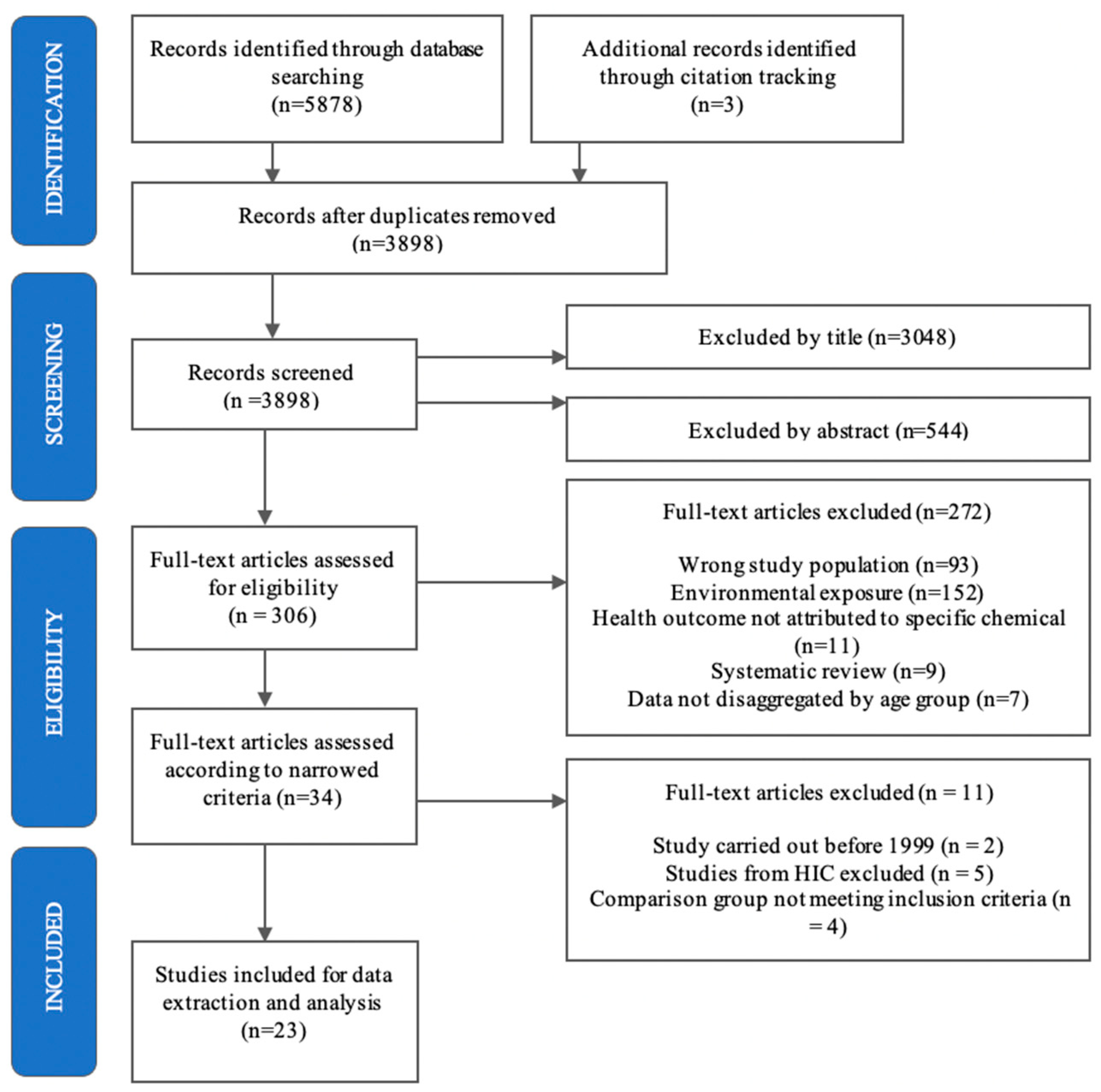
| Study selection | 17 | Give numbers of studies screened, assessed for eligibility, and included in the review, with reasons for exclusions at each stage, ideally with a flow diagram. | Results-study selection |
| Study characteristics | 18 | For each study, present characteristics for which data were extracted (e.g., study size, PICOS, follow-up period) and provide the citations. | Results-Table 4 |
| Risk of bias within studies | 19 | Present data on risk of bias of each study and, if available, any outcome level assessment (see item 12). | Results-quality appraisal |
| Results of individual studies | 20 | For all outcomes considered (benefits or harms), present, for each study: (a) simple summary data for each intervention group (b) effect estimates and confidence intervals, ideally with a forest plot. | Results |
| Synthesis of results | 21 | Present results of each meta-analysis done, including confidence intervals and measures of consistency. | n/a |
| Risk of bias across studies | 22 | Present results of any assessment of risk of bias across studies (see Item 15). | Results-quality appraisal |
| Additional analysis | 23 | Give results of additional analyses, if done (e.g., sensitivity or subgroup analyses, meta-regression [see Item 16]). | n/a |
| Discussion | |||
| Summary of evidence | 24 | Summarize the main findings including the strength of evidence for each main outcome; consider their relevance to key groups (e.g., healthcare providers, users, and policy makers). | Discussion |
| Limitations | 25 | Discuss limitations at study and outcome level (e.g., risk of bias), and at review-level (e.g., incomplete retrieval of identified research, reporting bias). | Discussion-limitations of this review |
| Conclusions | 26 | Provide a general interpretation of the results in the context of other evidence, and implications for future research. | Conclusion |
| Funding | |||
| Funding | 27 | Describe sources of funding for the systematic review and other support (e.g., supply of data); role of funders for the systematic review. | n/a |
| SEARCH 1: Child Labour Synonyms/Mesh Term and Chemical Synonyms/Mesh Terms | |
| CONCEPT A: Child Labour | |
| Synonyms | child* or adolescen* or teenage* or young or youth* or girl* or boy* or young human* adj8 work* or employ* or labo?r* or occupation* |
| MeSH terms | Child labor/ |
| CONCEPT B: Chemicals | |
| Synonyms | Chemical* or toxi* or acid* or poison* or cleaning agent* or clean* or metal*or heavy metal* or lead* or arsenic* or mercury* or cadmium* or chromium* or nickel* or manganese* or fluoride* or hydrofluoric* or hydrochloric* or chlor * or ammonia* or bleach* or pesticide* or fumigant* or fungicide* or rodenticide* or insecticide* or herbicide* or agrochemical* or agriculture* or carbamate* or organochloride* or organophosphate* or OPP or chlorpyrifos* or parathion-methyl* or aldicarb* or terbuphos* or phorate* or edifenphos* or methamidophos* or malathion* or metam sodium* or methyl bromide* or paraquat* or parathion* or pentachlorophenol* or warfarin* or methomyl* or inorganic* or organic* or solvent* or hexane* or benzene* or ethanol* or oil* or diesel* or petrol* or fuel* or paint thinner* or turpentine* or toluene* or nicotine* or tobacco* or carbon monoxide* or tetrachloroethylene* or persistent organic pollutant* or POP or chlorinated hydrocarbon* or polychlorinated biphenyl* or PCB or polybrominated diphenyl ether* or PBDE or dichlorodiphenyldichloroethylene* or DDE or dichlorodiphenyltrichloroethane* or DDT or phthalate* or bisphenol* or perfluorinated compound* or aldrin* |
| Mesh terms | Pesticides/ or Solvents/ or Metals, Heavy/ or Cadmium Poisoning/ or Organophosphate Poisoning/ or Heavy Metal Poisoning/ or Lead Poisoning/ or Manganese Poisoning/ or Mercury Poisoning/ or Poisoning/ |
| SEARCH 2: Child synonyms AND Occupational Exposure mesh terms AND Chemical synonyms | |
| CONCEPT C: Child | |
| Synonyms | child* or adolescen* or teenage* or young or youth* or girl* or boy* or young human* |
| CONCEPT D: Occupational exposure | |
| Mesh terms | Occupational Diseases/ or Occupational Exposure/ |
| CONCEPT B: Chemicals | |
| Synonyms | Chemical* or toxi* or acid* or poison* or cleaning agent* or clean* or metal*or heavy metal* or lead* or arsenic* or mercury* or cadmium* or chromium* or nickel* or manganese* or fluoride* or hydrofluoric* or hydrochloric* or chlori* or ammonia* or bleach* or pesticide* or fumigant* or fungicide* or rodenticide* or insecticide* or herbicide* or agrochemical* or agriculture* or carbamate* or organochloride* or organophosphate* or OPP or chlorpyrifos* or parathion-methyl* or aldicarb* or terbuphos* or phorate* or edifenphos* or methamidophos* or malathion* or metam sodium* or methyl bromide* or paraquat* or parathion* or pentachlorophenol* or warfarin* or methomyl* or inorganic* or organic* or solvent* or hexane* or benzene* or ethanol* or oil* or diesel* or petrol* or fuel* or paint thinner* or turpentine* or toluene* or nicotine* or tobacco* or carbon monoxide* or tetrachloroethylene* or persistent organic pollutant* or POP or chlorinated hydrocarbon* or polychlorinated biphenyl* or PCB or polybrominated diphenyl ether* or PBDE or dichlorodiphenyldichloroethylene* or DDE or dichlorodiphenyltrichloroethane* or DDT or phthalate* or bisphenol* or perfluorinated compound* or aldrin* |
| SEARCH 3: Child synonyms AND Occupational Exposure mesh terms AND Industry synonyms | |
| CONCEPT C: Child | |
| Synonyms | child* or adolescen* or teenage* or young or youth* or girl* or boy* or young human* |
| CONCEPT D: Occupational exposure | |
| Mesh terms | Occupational Diseases/ or Occupational Exposure/ |
| CONCEPT E: Industry | |
| Synonyms | Factory or Factories or Agricultur* or Mining or Mine or Street* or Workshop* or Industr* or Dump* or Scavenger* or Manufactur* |
| # | Search |
| 1 | ((child* or adolescen* or teenage* or young or youth* or girl* or boy* or young human*) adj8 (work* or employ* or labo?r* or occupation*)).m_titl. |
| 2 | exp Child Labor/ |
| 3 | 1 or 2 |
| 4 | (Chemical* or toxi * or acid* or poison* or cleaning agent* or clean* or metal* or heavy metal* or lead* or arsenic* or mercury* or cadmium* or chromium* or nickel* or manganese* or fluoride* or hydrofluoric* or hydrochloric* or chlori* or ammonia* or bleach* or pesticide* or fumigant* or fungicide* or rodenticide* or insecticide* or herbicide* or agrochemical* or agriculture* or carbamate* or organochloride* or organophosphate* or OPP or chlorpyrifos* or parathion-methyl* or aldicarb* or terbuphos* or phorate* or edifenphos* or methamidophos* or malathion* or metam sodium* or methyl bromide* or paraquat* or parathion* or pentachlorophenol* or warfarin* or methomyl* or inorganic* or organic* or solvent* or hexane* or benzene* or ethanol* or oil* or diesel* or petrol* or fuel* or paint thinner* or turpentine* or toluene* or nicotine* or tobacco* or carbon monoxide* or tetrachloroethylene* or persistent organic pollutant* or POP or chlorinated hydrocarbon* or polychlorinated biphenyl* or PCB or polybrominated diphenyl ether* or PBDE or dichlorodiphenyldichloroethylene* or DDE or dichlorodiphenyltrichloroethane* or DDT or phthalate* or bisphenol* or perfluorinated compound* or aldrin*).mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] |
| 5 | exp Pesticides/ or exp Solvents/ or exp Metals, Heavy/ Cadmium Poisoning/ or Organophosphate Poisoning/ or Heavy Metal Poisoning/ or Lead Poisoning/ or Manganese Poisoning/ or Mercury Poisoning/ or Poisoning/ |
| 6 | 4 or 5 |
| 7 | 3 and 6 (1071 records found) |
| 8 | (child* or adolescen* or teenage* or young or youth* or girl* or boy* or young human*).m_titl. |
| 9 | exp Occupational Diseases/ or exp Occupational Exposure/ |
| 10 | 4 and 8 and 9 (636 records found |
| 11 | (Factory or Factories or Agricultur* or Mining or Mine or Street* or Workshop* or Industr* or Dump* or Scavenger* or Manufactur).mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] |
| 12 | 8 and 9 and 11 (417 records found) |



References
- ILO. Convention C182—Worst Forms of Child Labour Convention, 1999 (No. 182). 2015. Available online: https://www.ilo.org/dyn/normlex/en/f?p=NORMLEXPUB:12100:0::NO::P12100_ILO_CODE:C182 (accessed on 6 August 2020).
- ILO. Global Estimates of Child Labour: Results and Trends, 2012–2016; ILO: Geneva, Switzerland, 2017; pp. 10–19. [Google Scholar]
- ILO. Children in Hazardous Work: What We Know, What We Need to Do; ILO: Geneva, Switzerland, 2011. [Google Scholar]
- Avis, W. Data on the Prevalence of the Worst Forms of Child Labour; K4D Helpdesk Report; Institute of Development Studies: Brighton, UK, 2017. [Google Scholar]
- Filip, I.; Radfar, A.; Asgharzadeh, S.A.A.; Quesada, F. Challenges and perspectives of child labor. Ind. Psychiatry J. 2018, 27, 17–20. [Google Scholar] [CrossRef]
- WHO. Protecting Children’s Health in a Changing Environment. Report of the 5th Ministerial Conference on Health and the Environment. 2010. Available online: http://www.euro.who.int/en/publications/abstracts/protecting-childrens-health-in-a-changing-environment.-report-of-the-fifth-ministerial-conference-on-environment-and-health (accessed on 6 August 2020).
- Sudhinaraset, M.; Blum, R.W. The unique developmental considerations of youth-related work injuries. Int. J. Occup. Environ. Health 2010, 16, 216–222. [Google Scholar] [CrossRef]
- Organisation for Economic Co-Operation and Development. The Costs and Benefits of Regulating Chemicals. 2018. Available online: http://www.oecd.org/environment/tools-evaluation/sacame.htm (accessed on 7 September 2020).
- World Health Organization. Principles for Evaluating Health Risks in Children Associated with Exposure to Chemicals; World Health Organization: Geneva, Switzerland, 2006. [Google Scholar]
- O’Donnell, O.; Van Doorslaer, E.; Rosati, F.C. Child Labour and Health: Evidence and Research Issues. SSRN Electron. J. 2002. [Google Scholar] [CrossRef] [Green Version]
- Roberts, J.R.; Karr, C.J. Council on Environmental Health Pesticide Exposure in Children. Pediatrics 2012, 130, e1765–e1788. [Google Scholar] [CrossRef] [Green Version]
- United Nations. Mining and Quarrying. In Industrial Commodity Statistics Yearbook 2010; United Nations Publications: New York, NY, USA, 2010; Volume 1, pp. 1–56. [Google Scholar] [CrossRef]
- Shah, F.; Kazi, T.G.; Afridi, H.I.; Naeemullah; Arain, S.S. Exposures of lead to adolescent workers in battery recycling workshops and surrounding communities. J. Expo. Sci. Environ. Epidemiol. 2012, 22, 649–653. [Google Scholar] [CrossRef] [Green Version]
- Lahiry, G.; Rahman, T.; Hasan, A.K.M.M.; Dutta, A.K.; Arif, M.; Howlader, Z.H. Assessment of Impact on Health of Children Working in the Garbage Dumping Site in Dhaka, Bangladesh. J. Trop. Pediatr. 2011, 57, 472–475. [Google Scholar] [CrossRef] [Green Version]
- Athanasiadou, M.; Cuadra, S.N.; Marsh, G.; Bergman, A.; Jakobsson, K. Polybrominated Diphenyl Ethers (PBDEs) and Bioaccumulative Hydroxylated PBDE Metabolites in Young Humans from Managua, Nicaragua. Environ. Health Perspect. 2008, 116, 400–408. [Google Scholar] [CrossRef] [Green Version]
- Tiwari, R.R.; Saha, A.; Sathwara, N.G.; Parikh, J.R. Blood chromium levels of children working in gem-polishing industries in India. Toxicol. Ind. Health 2011, 28, 170–173. [Google Scholar] [CrossRef]
- Grandjean, P.; Landrigan, P.J. Neurobehavioural effects of developmental toxicity. Lancet Neurol. 2014, 13, 330–338. [Google Scholar] [CrossRef] [Green Version]
- Kelishadi, R.; Poursafa, P.; Ataei, E. A systematic review on the effects of environmental exposure to some organohalogens and phthalates on early puberty. J. Res. Med Sci. 2015, 20, 613–618. [Google Scholar] [CrossRef]
- Pereira, R.; Ribeiro, R.; Gonçalves, F.J.M. Scalp hair analysis as a tool in assessing human exposure to heavy metals (S. Domingos mine, Portugal). Sci. Total Environ. 2004, 327, 81–92. [Google Scholar] [CrossRef] [Green Version]
- Lau, C.; Rogers, J.M. Embryonic and fetal programming of physiological disorders in adulthood. Birth Defects Res. Part C Embryo Today Rev. 2004, 72, 300–312. [Google Scholar] [CrossRef]
- Buralli, R.J.; Dultra, A.F.; Ribeiro, H. Respiratory and Allergic Effects in Children Exposed to Pesticides—A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 2740. [Google Scholar] [CrossRef]
- Blakley, B.; Brousseau, P.; Voccia, I.; Fournier, M. Immunotoxicity of pesticides: A review. Toxicol. Ind. Health 1999, 15, 119–132. [Google Scholar] [CrossRef]
- Landrigan, P.J.; Kimmel, C.A.; Correa, A.; Eskenazi, B. Children’s health and the environment: Public health issues and challenges for risk assessment. Environ. Health Perspect. 2004, 112, 257–265. [Google Scholar] [CrossRef]
- Fassa, A.G.; Facchini, L.A.; Dall’Agnol, M.M.; Christiani, D.C. Child Labor and Health: Problems and Perspectives. Int. J. Occup. Environ. Health 2000, 6, 55–62. [Google Scholar] [CrossRef]
- Estes, C.R.; Jackson, L.L.; Castillo, D.N. Occupational Injuries and Deaths among Younger Workers—United States, 1998–2007. Morb. Mortal. Wkly. Rep. 2010, 59, 449–455. [Google Scholar]
- Selevan, S.G.; Kimmel, C.A.; Mendola, P. Identifying Critical Windows of Exposure for Children’s Health. Environ. Health Perspect. 2000, 108, 451. [Google Scholar] [CrossRef]
- Sasmal, J.; Guillen, J. Poverty, Educational Failure and the Child-Labour Trap: The Indian Experience. Glob. Bus. Rev. 2015, 16, 270–280. [Google Scholar] [CrossRef]
- Muntaner, C.; Solar, O.; Vanroelen, C.; Martínez, J.M.; Vergara, M.; Santana, V.; Castedo, A.; Kim, I.-H.; Benach, J.; Network, E. Unemployment, Informal Work, Precarious Employment, Child Labor, Slavery, and Health Inequalities: Pathways and Mechanisms. Int. J. Health Serv. 2010, 40, 281–295. [Google Scholar] [CrossRef]
- Sámano-Ríos, M.L.; Ijaz, S.; Ruotsalainen, J.; Breslin, F.C.; Gummesson, K.; Verbeek, J. Occupational safety and health interventions to protect young workers from hazardous work—A scoping review. Saf. Sci. 2019, 113, 389–403. [Google Scholar] [CrossRef]
- Woolf, A.; Alpert, H.R.; Garg, A.; Lesko, S. Adolescent Occupational Toxic Exposures. Arch. Pediatr. Adolesc. Med. 2001, 155, 704–710. [Google Scholar] [CrossRef] [Green Version]
- Pega, F.; Chartres, N.; Guha, N.; Modenese, A.; Morgan, R.L.; Martínez-Silveira, M.S.; Loomis, D. The Effect of Occupational Exposure to Welding Fumes on Trachea, Bronchus and Lung Cancer: A Protocol for a Systematic Review and Meta-Analysis from the WHO/ILO Joint Estimates of the Work-Related Burden of Disease and Injury. Environ. Int. 2001, 145, 106089. [Google Scholar] [CrossRef]
- Hsiao, C.-Y.; Wu, H.-D.I.; Lai, J.-S.; Kuo, H.-W. A longitudinal study of the effects of long-term exposure to lead among lead battery factory workers in Taiwan (1989–1999). Sci. Total Environ. 2001, 279, 151–158. [Google Scholar] [CrossRef]
- International Occupational Safety and Health Information Centre. 2011. Chemical Exposure Limits. Available online: https://www.ilo.org/safework/info/publications/WCMS_151534 (accessed on 12 March 2016).
- Health and Safety Executive. EH4O/2005 Workplace Exposure Limits; Stationery Office: London, UK, 2020. [Google Scholar]
- Rothenberg, S.J. Blood Lead Levels in Children. Environ. Health Perspect. 2008, 116. [Google Scholar] [CrossRef]
- Kuimi, B.L.B.; Oppong-Nkrumah, O.; Kaufman, J.; Nazif-Munoz, J.I.; Nandi, A. Child labour and health: A systematic review. Int. J. Public Health 2018, 63, 663–672. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roggero, P.; Mangiaterra, V.; Bustreo, F.; Rosati, F. The Health Impact of Child Labor in Developing Countries: Evidence From Cross-Country Data. Am. J. Public Health 2007, 97, 271–275. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, A.; Abdalla, S.M.; Jafer, M.; Abdelgadir, J.; De Vries, N. Child labor and health: A systematic literature review of the impacts of child labor on child’s health in low- and middle-income countries. J. Public Health 2019, 41, 18–26. [Google Scholar] [CrossRef]
- Shendell, D.G.; Noomnual, S.; Chishti, S.; Allacci, M.S.; Madrigano, J. Exposures Resulting in Safety and Health Concerns for Child Laborers in Less Developed Countries. J. Environ. Public Health 2016, 3985498. [Google Scholar] [CrossRef] [Green Version]
- New World Bank Country Classifications by Income Level: 2020–2021. Available online: https://blogs.worldbank.org/opendata/new-world-bank-country-classifications-income-level-2020-2021 (accessed on 12 April 2021).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- OSHA. Occupational Chemical Database. Occupational Safety and Health Administration. 2019. Available online: https://www.osha.gov/chemicaldata/ (accessed on 25 July 2020).
- Lanphear, B.P. Biomarkers in paediatric research and practice. Arch. Dis. Child. 2005, 90, 594–600. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ohayo-Mitoko, G.J.; Kromhout, H.; Karumba, P.N.; Boleij, J.S. Identification of determinants of pesticide exposure among Kenyan agricultural workers using empirical modelling. Ann. Occup. Hyg. 1999, 43, 519–525. [Google Scholar] [CrossRef]
- Groopman, J.D.; Kensler, T.W. The light at the end of the tunnel for chemical-specific biomarkers: Daylight or headlight? Carcinogenesis 1999, 20, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Rushton, L. Retrospective exposure assessment in environmental epidemiology. Occup. Environ. Med. 2009, 66, 572–573. [Google Scholar] [CrossRef]
- Muñoz-Quezada, M.T.; Lucero, B.A.; Barr, D.B.; Steenland, K.; Levy, K.; Ryan, P.B.; Iglesias, V.; Alvarado, S.; Concha, C.; Rojas, E.; et al. Neurodevelopmental effects in children associated with exposure to organophosphate pesticides: A systematic review. Neurotoxicology 2013, 39, 158–168. [Google Scholar] [CrossRef] [Green Version]
- Moore, V. Spirometry: Step by step. Breathe 2012, 8, 232–240. [Google Scholar] [CrossRef] [Green Version]
- Koulouri, O.; Moran, C.; Halsall, D.; Chatterjee, K.; Gurnell, M. Pitfalls in the measurement and interpretation of thyroid function tests. Best Pract. Res. Clin. Endocrinol. Metab. 2013, 27, 745–762. [Google Scholar] [CrossRef] [Green Version]
- Cooke, M.S.; Evans, M.D.; Dizdaroglu, M.; Lunec, J. Oxidative DNA damage: Mechanisms, mutation, and disease. FASEB J. 2003, 17, 1195–1214. [Google Scholar] [CrossRef] [Green Version]
- Singh, N.P.; McCoy, M.T.; Tice, R.R.; Schneider, E.L. A simple technique for quantitation of low levels of DNA damage in individual cells. Exp. Cell Res. 1988, 175, 184–191. [Google Scholar] [CrossRef] [Green Version]
- Critical Appraisal Skills Programme. 2018. Home—CASP—Critical Appraisal Skills Programme. CASP Systematic Review Checklist. Available online: https://casp-uk.net/ (accessed on 25 July 2020).
- Downes, M.J.; Brennan, M.L.; Williams, H.C.; Dean, R.S. Development of a critical appraisal tool to assess the quality of cross-sectional studies (AXIS). BMJ Open 2016, 6, e011458. [Google Scholar] [CrossRef] [Green Version]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef] [PubMed]
- Callahan, C.L.; Al-Batanony, M.; Ismail, A.A.; Abdel-Rasoul, G.; Hendy, O.; Olson, J.R.; Rohlman, D.S.; Bonner, M.R. Chlorpyrifos Exposure and Respiratory Health among Adolescent Agricultural Workers. Int. J. Environ. Res. Public Health 2014, 11, 13117–13129. [Google Scholar] [CrossRef] [PubMed]
- Ismail, A.A.; Bonner, M.R.; Hendy, O.; Rasoul, G.A.; Wang, K.; Olson, J.R.; Rohlman, D.S. Comparison of neurological health outcomes between two adolescent cohorts exposed to pesticides in Egypt. PLoS ONE 2017, 12, e0172696. [Google Scholar] [CrossRef]
- Kazi, T.G.; Shah, F.; Afridi, H.I.; Naeemullah. Occupational and Environmental Lead Exposure to Adolescent Workers in Battery Recycling Workshops. Toxicol. Ind. Health 2015, 31, 1288–1295. [Google Scholar] [CrossRef] [PubMed]
- Baloch, S.; Kazi, T.G.; Baig, J.A.; Afridi, H.I.; Arain, M.B. Occupational exposure of lead and cadmium on adolescent and adult workers of battery recycling and welding workshops: Adverse impact on health. Sci. Total Environ. 2020, 720, 137549. [Google Scholar] [CrossRef]
- Sughis, M.; Nawrot, T.S.; Haufroid, V.; Nemery, B. Adverse Health Effects of Child Labor: High Exposure to Chromium and Oxidative DNA Damage in Children Manufacturing Surgical Instruments. Environ. Health Perspect. 2012, 120, 1469–1474. [Google Scholar] [CrossRef]
- Abdel Rasoul, G.M.; Abou Salem, M.E.; Mechael, A.A.; Hendy, O.M.; Rohlman, D.S.; Ismail, A.A. Effects of Occupational Pesticide Exposure on Children Applying Pesticides. Neurotoxicology 2008, 29, 833–838. [Google Scholar] [CrossRef]
- Hariton, E.; Locascio, J.J. Randomised controlled trials—the gold standard for effectiveness research. BJOG Int. J. Obstet. Gynaecol. 2018, 125, 1716. [Google Scholar] [CrossRef] [Green Version]
- Eckerman, D.A.; Gimenes, L.S.; De Souza, R.C.; Galvão, P.R.L.; Sarcinelli, P.N.; Chrisman, J.R. Age related effects of pesticide exposure on neurobehavioral performance of adolescent farm workers in Brazil. Neurotoxicol. Teratol. 2007, 29, 164–175. [Google Scholar] [CrossRef]
- Rohlman, D.S.; Ismail, A.A.; Abdel-Rasoul, G.; Lasarev, M.; Hendy, O.; Olson, J.R. Characterizing exposures and neurobehavioral performance in Egyptian adolescent pesticide applicators. Metab. Brain Dis. 2014, 29, 845–855. [Google Scholar] [CrossRef] [Green Version]
- Saddik, B.; Williamson, A.; Black, D.; Nuwayhid, I. Neurobehavioral Impairment in Children Occupationally Exposed to Mixed Organic Solvents. Neurotoxicology 2009, 30, 1166–1171. [Google Scholar] [CrossRef] [PubMed]
- Saddik, B.; Nuwayhid, I.; Williamson, A.; Black, D. Evidence of Neurotoxicity in Working Children in Lebanon. Neurotoxicology 2003, 24, 733–739. [Google Scholar] [CrossRef]
- Saddik, B.; Williamson, A.; Nuwayhid, I.; Black, D. The Effects of Solvent Exposure on Memory and Motor Dexterity in Working Children. Public Health Rep. 2005, 120, 657–663. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nuwayhid, I.A.; Usta, J.; Makarem, M.; Khudr, A.; El-Zein, A. Health of children working in small urban industrial shops. Occup. Environ. Med. 2005, 62, 86–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moawad, E.M.I.; Badawy, N.M.; Manawill, M. Environmental and Occupational Lead Exposure Among Children in Cairo, Egypt. Medicine 2016, 95, e2976. [Google Scholar] [CrossRef] [PubMed]
- Arif, M.; Islam, M.T.; Shekhar, H.U. Lead induced oxidative DNA damage in battery-recycling child workers from Bangladesh. Toxicol. Ind. Health 2018, 34, 213–218. [Google Scholar] [CrossRef]
- Dundar, B.; Öktem, F.; Arslan, M.K.; Delibas, N.; Baykal, B.; Arslan, Ç.; Gultepe, M.; Ilhan, I.E. The effect of long-term low-dose lead exposure on thyroid function in adolescents. Environ. Res. 2006, 101, 140–145. [Google Scholar] [CrossRef]
- Bose-O’Reilly, S.; Lettmeier, B.; Gothe, R.M.; Beinhoff, C.; Siebert, U.; Drasch, G. Mercury as a serious health hazard for children in gold mining areas. Environ. Res. 2008, 107, 89–97. [Google Scholar] [CrossRef]
- Junaid, M.; Malik, R.N.; Pei, D.-S. Health hazards of child labor in the leather products and surgical instrument manufacturing industries of Sialkot, Pakistan. Environ. Pollut. 2017, 226, 198–211. [Google Scholar] [CrossRef]
- Sughis, M.; Nawrot, T.S.; Riaz, A.; Ikram-Dar, U.; Mahmood, A.; Haufroid, V.; Nemery, B. Metal exposure in schoolchildren and working children. A urinary biomonitoring study from Lahore, Pakistan. Int. J. Hyg. Environ. Health 2014, 217, 669–677. [Google Scholar] [CrossRef]
- Cuadra, S.N.; Linderholm, L.; Athanasiadou, M.; Jakobsson, K. Persistent Organochlorine Pollutants in Children Working at a Waste-Disposal Site and in Young Females with High Fish Consumption in Managua, Nicaragua. AMBIO 2006, 35, 109–116. [Google Scholar] [CrossRef]
- American Conference of Governmental Industrial Hygienists. TLVs and BEIs: Based on the Documentation of the Threshold Limit Values for Chemical Substances and Physical Agents & Biological Exposure Indices; ACGIH: Cincinnati, OH, USA, 2006. [Google Scholar]
- Gottesfeld, P.; Pokhrel, A.K. Review: Lead Exposure in Battery Manufacturing and Recycling in Developing Countries and Among Children in Nearby Communities. J. Occup. Environ. Hyg. 2011, 8, 520–532. [Google Scholar] [CrossRef] [PubMed]
- Rees, N.; Fuller, R. The Toxic Truth: Children’ s Exposure to Lead Pollution Undermines a Generation of Future Potential; UNICEF: New York, NY, USA, 2020; pp. 1–90. [Google Scholar]
- ILO. Work-Related Fatalities Reach 2 Million Annually. 2002. Available online: https://www.ilo.org/global/about-the-ilo/newsroom/news/WCMS_007789/lang--en/index.htm (accessed on 23 September 2020).
- International Agency for Research on Cancer. Arsenic, Metals, Fibres and Dusts: A Review of Human Carcinogens—Part C; WHO: Geneva, Switzerland, 2021. [Google Scholar]
- Proctor, D.M.; Otani, J.M.; Finley, B.L.; Paustenbach, D.J.; Bland, J.A.; Speizer, N.; Sargent, E.V. Is hexavalent chromium carcinogenic via ingestion? A weight-of-evidence review. J. Toxicol. Environ. Health Part A 2002, 65, 701–746. [Google Scholar] [CrossRef]
- Shrivastava, R.; Upreti, R.; Seth, P.; Chaturvedi, U. Effects of chromium on the immune system. FEMS Immunol. Med. Microbiol. 2002, 34, 1–7. [Google Scholar] [CrossRef]
- Steenland, K.; Barry, V.; Anttila, A.; Sallmen, M.; Mueller, W.; Ritchie, P.; McElvenny, D.M.; Straif, K. Cancer incidence among workers with blood lead measurements in two countries. Occup. Environ. Med. 2019, 76, 603–610. [Google Scholar] [CrossRef]
- Lerro, C.C.; Koutros, S.; Andreotti, G.; Sandler, D.P.; Lynch, C.F.; Louis, L.M.; Blair, A.; Parks, C.G.; Shrestha, S.; Lubin, J.H.; et al. Cancer incidence in the Agricultural Health Study after 20 years of follow-up. Cancer Causes Control 2019, 30, 311–322. [Google Scholar] [CrossRef]
- WHO. Lead Poisoning and Health. 2019. Available online: https://www.who.int/news-room/fact-sheets/detail/lead-poisoning-and-health (accessed on 13 September 2020).
- WHO. Exposure to Cadmium: A Major Public Health Concern. Preventing Disease Through Healthy Environments, 3–6. 2010. Available online: http://www.who.int/ipcs/features/cadmium.pdf (accessed on 13 September 2020).
- Bernhoft, R.A. Mercury Toxicity and Treatment: A Review of the Literature. J. Environ. Public Health 2011, 2012, 460508. [Google Scholar] [CrossRef]
- Trasande, L.; Zoeller, R.T.; Hass, U.; Kortenkamp, A.; Grandjean, P.; Myers, J.P.; DiGangi, J.; Hunt, P.M.; Rüdel, R.; Sathyanarayana, S.; et al. Burden of disease and costs of exposure to endocrine disrupting chemicals in the European Union: An updated analysis. Andrology 2016, 4, 565–572. [Google Scholar] [CrossRef] [Green Version]
- Sturrock, S.; Hodes, M. Child labour in low- and middle-income countries and its consequences for mental health: A systematic literature review of epidemiologic studies. Eur. Child Adolesc. Psychiatry 2016, 25, 1273–1286. [Google Scholar] [CrossRef]
- Campion, J. Public Mental Health: Evidence, Practice and Commissioning; Royal Society for Public Health: London, UK, 2019. [Google Scholar]
- London, L.; Beseler, C.; Bouchard, M.F.; Bellinger, D.C.; Colosio, C.; Grandjean, P.; Harari, R.; Kootbodien, T.; Kromhout, H.; Little, F.; et al. Neurobehavioral and neurodevelopmental effects of pesticide exposures. Neurotoxicology 2012, 33, 887–896. [Google Scholar] [CrossRef] [Green Version]
- Pandey, A.K.; Bajpayee, M.; Parmar, D.; Kumar, R.; Rastogi, S.K.; Mathur, N.; Thorning, P.; De Matas, M.; Shao, Q.; Anderson, D.; et al. Multipronged evaluation of genotoxicity in Indian petrol-pump workers. Environ. Mol. Mutagen. 2008, 49, 695–707. [Google Scholar] [CrossRef]
- Liu, Q.; Cao, J.; Li, K.Q.; Miao, X.H.; Li, G.; Fan, F.Y.; Zhao, Y.C. Chromosomal aberrations and DNA damage in human populations exposed to the processing of electronics waste. Environ. Sci. Pollut. Res. 2008, 16, 329–338. [Google Scholar] [CrossRef] [PubMed]
- Harrison, D.; Griendling, K.K.; Landmesser, U.; Hornig, B.; Drexler, H. Role of oxidative stress in atherosclerosis. Am. J. Cardiol. 2003, 91, 7–11. [Google Scholar] [CrossRef]
- Finkel, T.; Holbrook, N.J. Oxidants, oxidative stress and the biology of ageing. Nature 2000, 408, 239–247. [Google Scholar] [CrossRef]
- Parks, C.G.; D’Aloisio, A.A.; Sandler, D.P. Childhood Residential and Agricultural Pesticide Exposures in Relation to Adult-Onset Rheumatoid Arthritis in Women. Am. J. Epidemiol. 2018, 187, 214–223. [Google Scholar] [CrossRef] [Green Version]
- Grosse, S.D.; Matte, T.D.; Schwartz, J.; Jackson, R.J. Economic gains resulting from the reduction in children’s exposure to lead in the United States. Environ. Health Perspect. 2002, 110, 563–569. [Google Scholar] [CrossRef] [Green Version]
- Bharadwaj, P.; Lakdawala, L.K.; Li, N. Perverse Consequences of Well Intentioned Regulation: Evidence from India’s Child Labor Ban. J. Eur. Econ. Assoc. 2019, 18, 1158–1195. [Google Scholar] [CrossRef] [Green Version]
- The Consequences of Banning Child Labor. Available online: https://blogs.worldbank.org/developmenttalk/consequences-banning-child-labor (accessed on 2 December 2020).
- Blair, S.L. Children’s participation in household labor: Child socialization versus the need for household labor. J. Youth Adolesc. 1992, 21, 241–258. [Google Scholar] [CrossRef]
- O’Kane, C.; Barros, O.; Meslaoui, N. It’s Time to Talk!—Children’s Views on Children’s Work; Save the Children: London, UK; Kindernothilfe: Vienna, Austria; Terre des Hommes: Geneva, Switzerland, 2017. [Google Scholar]
- Woodhead, M. Combatting Child Labour. Childhood 1999, 6, 27–49. [Google Scholar] [CrossRef]
- Kassouf, A.L.; McKee, M.; Mossialos, E. Early entrance to the job market and its effect on adult health: Evidence from Brazil. Health Policy Plan. 2001, 16, 21–28. [Google Scholar] [CrossRef] [Green Version]
- Dammert, A.C.; De Hoop, J.; Mvukiyehe, E.; Rosati, F.C. Effects of public policy on child labor: Current knowledge, gaps, and implications for program design. World Dev. 2018, 110, 104–123. [Google Scholar] [CrossRef] [Green Version]
- Home. Available online: http://www.mymeproject.org/ (accessed on 2 December 2020).
- Schmidt, L.; Garratt, A.; Fitzpatrick, R. Instruments for Mental Health: A Review Report from the Patient-reported Health Instruments Group to the Department of Health; Patient-Reported Health Instruments Group: London, UK, September 2000. [Google Scholar]
- Rebok, G.; Riley, A.; Forrest, C.; Starfield, B.; Green, B.; Robertson, J.; Tambor, E. Elementary school-aged children’s reports of their health: A cognitive interviewing study. Qual. Life Res. 2001, 10, 59–70. [Google Scholar] [CrossRef] [PubMed]
- Eckerman, D.A.; Coelho, C.; Gimenes, L.S.; Huber, E.R.; Rohlman, D.S.; Anger, W.K. Behavioral Observation Used to Estimate Pesticide Exposure for Farm Workers in Brazil. Psychol. Neurosci. 2009, 2, 43. [Google Scholar] [CrossRef] [Green Version]
- Macfarlane, E.; Glass, D.; Fritschi, L. Is farm-related job title an adequate surrogate for pesticide exposure in occupational cancer epidemiology? Occup. Environ. Med. 2009, 66, 497–501. [Google Scholar] [CrossRef] [PubMed]
- CDC. 2009. Fourth National Report on Human Exposure to Environmental Chemicals. Available online: https://www.cdc.gov/exposurereport/pdf/fourthreport.pdf (accessed on 13 September 2020).
- Barbosa, F.; Tanus-Santos, J.E.; Gerlach, R.F.; Parsons, P.J. A Critical Review of Biomarkers Used for Monitoring Human Exposure to Lead: Advantages, Limitations, and Future Needs. Environ. Health Perspect. 2005, 113, 1669–1674. [Google Scholar] [CrossRef] [Green Version]
- Gil, F.; Hernández, A.F.; Márquez, C.; Femia, P.; Olmedo, P.; López-Guarnido, O.; Pla, A. Biomonitorization of cadmium, chromium, manganese, nickel and lead in whole blood, urine, axillary hair and saliva in an occupationally exposed population. Sci. Total Environ. 2011, 409, 1172–1180. [Google Scholar] [CrossRef]
- Esteban, M.; Castaño, A. Non-invasive matrices in human biomonitoring: A review. Environ. Int. 2009, 35, 438–449. [Google Scholar] [CrossRef]
- Gamlin, J.; Romo, P.D.; Hesketh, T. Exposure of young children working on Mexican tobacco plantations to organophosphorous and carbamic pesticides, indicated by cholinesterase depression. Child Care Health Dev. 2007, 33, 246–248. [Google Scholar] [CrossRef] [PubMed]
- Rohlman, D.S.; Lasarev, M.R.; Anger, W.K.; Scherer, J.; Stupfel, J.; McCauley, L. Neurobehavioral Performance of Adult and Adolescent Agricultural Workers. Neurotoxicology 2007, 28, 374–380. [Google Scholar] [CrossRef]
- Mitro, S.D.; Johnson, T.; Zota, A.R. Cumulative Chemical Exposures During Pregnancy and Early Development. Curr. Environ. Health Rep. 2015, 2, 367–378. [Google Scholar] [CrossRef] [Green Version]
- Hanvold, T.N.; Kines, P.; Nykänen, M.; Thomée, S.; Holte, K.A.; Vuori, J.; Wærsted, M.; Veiersted, K.B. Occupational Safety and Health Among Young Workers in the Nordic Countries: A Systematic Literature Review. Saf. Health Work 2019, 10, 3–20. [Google Scholar] [CrossRef]
- Haz-Map—Hazardous Chemicals and Occupational Diseases Information. Available online: https://haz-map.com/ (accessed on 28 September 2020).
- CISDOC Database. Available online: https://www.ilo.org/dyn/cisdoc2/cismain.home?p_lang=en (accessed on 28 September 2020).
- Pega, F.; Norris, S.L.; Backes, C.; Bero, L.A.; Descatha, A.; Gagliardi, D.; Godderis, L.; Loney, T.; Modenese, A.; Morgan, R.L.; et al. RoB-SPEO: A tool for assessing risk of bias in studies estimating the prevalence of exposure to occupational risk factors from the WHO/ILO Joint Estimates of the Work-related Burden of Disease and Injury. Environ. Int. 2020, 135, 105039. [Google Scholar] [CrossRef]
- Calvert, G.M.; Mehler, L.N.; Rosales, R.; Baum, L.; Thomsen, C.; Male, D.; Shafey, O.; Das, R.; Lackovic, M.; Arvizu, E. Acute Pesticide-Related Illnesses Among Working Youths, 1988–1999. Am. J. Public Health 2003, 93, 605–610. [Google Scholar] [CrossRef]
- Corriols, M.; Aragón, A. Child labor and acute pesticide poisoning in Nicaragua: Failure to comply with children’s rights. Int. J. Occup. Environ. Health 2010, 16, 193–200. [Google Scholar] [CrossRef]
- Rogan, W.J.; Ware, J.H. Exposure to Lead in Children—How Low Is Low Enough? N. Engl. J. Med. 2003, 348, 1515–1516. [Google Scholar] [CrossRef] [PubMed] [Green Version]




| Types of Chemicals | Examples of Chemicals Commonly Used by Child Labourers | Types of Industries Using These Chemicals | Specific Tasks Conducted by Child Labourers |
|---|---|---|---|
| Pesticides | Organochlorides e.g., dichlorodiphenyltrichloroethane (DDT) and chlorinated alicyclics Organophosphates e.g., chlorpyrifos, parathion Carbamate insecticides e.g., aldicarb, carbofuran | Agriculture, plantations, other rural sectors | Handling, mixing, spraying pesticides |
| Heavy metals | Lead, mercury, chromium, cadmium | Mining and quarrying, construction, service sector and street work, manufacturing, textiles, leather, footwear | Mining tasks (e.g., crushing and amalgamating, sieving, washing, and sorting), vehicle repair, trash recycling, shoe-shining, making textiles, tanning leather, ceramics |
| Solvents | Isopropanol, benzene, toluene, xylene, and solvent mixtures, such as white spirits. | Food and drink, construction, printing, plastics, rubber, textiles, leather, footwear, manufacturing, dry cleaning | Making textiles, tanning leather, painting, printing, plastic product works, pressing clothes, cleaning |
| POPs * | DDT, polychlorinated biphenyl (PCB), polybrominated diphenyl ethers (PBDE) | Agriculture, vehicle repair, plastics, construction, electronics | Pesticide use, painting, rubbish recycling, waste incineration |
| Topic | Inclusion | Exclusion |
|---|---|---|
| Participants: Age | Participants are ≤18 years | Participants are >18 years old. Studies include those who are 18 years and under, however without disaggregated data for this age group |
| Participants: Workers | Participants are child labours, as defined by the study authors | Studies which do not involve work (e.g., those which are limited to environmental exposures only) |
| Interventions/exposures | A clearly defined chemical exposure | No specific chemical exposure |
| Comparisons | No criteria defined | No criteria defined |
| Outcomes | Health outcome directly related to occupational chemical exposure Acute or long-term outcome | Outcome not disaggregated according to exposure type |
| Study design | Qualitative studies Quantitative studies (intervention/case control/cohort/cross-sectional) | Grey literature |
| Language | English language only | Non-English language |
| Author-Defined Exposure | Exposure Measurement |
| Child labour in the presence of chemicals | Sector where chemicals are used (usually based on questionnaire. Sometimes sector is used as a blanket category of chemical exposure by researchers before the study) |
| Current work status/work history | Self-report questionnaire to determine number of hours at workplace where chemicals are used and number of years in sector |
| Scientific measurement using specialised equipment | Biomarkers of exposure (e.g., chemical concentrations or metabolite levels) Environmental assessment to measure workplace exposure to chemical levels (e.g., environmental air, water, soil, or food samples) * |
| Health Outcome Types | Examples |
| DNA damage | Oxidative stress and DNA damage |
| Biomarkers of effect | Toxin and metabolite levels (measured in blood, urine, hair, and saliva) |
| Organ e.g., lung, heart, liver, skin, kidneys | Cancer, diabetes, asthma, kidney disease, dermatitis |
| Body system e.g., Cardiovascular, endocrine, respiratory, neurological, reproductive, immune | Cardiovascular disease, neurotoxic symptoms, neurobehavioural deficits, hypothyroidism, hypertension, pulmonary function |
| Mental health | Mood disorders e.g., anxiety, depression |
| Non-specific symptoms | Wheezing, nail discolouration, fatigue |
| Author Country (Year) | Chemical | Industry | Participant Age | Participant Gender | Author-Defined Sample Description | Author-Defined Exposure Measurement | Author-Defined Health Outcomes | Paper Quality |
|---|---|---|---|---|---|---|---|---|
| Ismail et al. Egypt (2017) [56] | Pesticides: Chlorpyrifos | Agriculture: Cotton | 12–18 years | M | Pesticide applicators 2005 (n = 41); 2009 (n = 21) Non-applicators 2005 (n = 38); 2009 (n = 20) | SRQ: Current work status/work history/non-work chemical exposures | Neurobehavioural tests-BARS/WAIS-R Neurological symptoms Plasma BChE | Good |
| Abdel Rasoul et al. Egypt (2008) [60] | Pesticides: Chlorpyrifos | Agriculture: Cotton | 2 groups: 9–15 years 16–18 years | M | 9–15 years Pesticide applicators (n = 30) Non-applicators (n = 30) 16–18 years Pesticide applicators (n = 20) Non-applicators (n = 20) | SRQ: Current work status/work history BIO: Plasma AChE | Neurobehavioural tests-WAIS Neurological symptoms | Good |
| Eckerman et al. Brazil (2007) [62] | Pesticides: Unspecified OP | Agriculture: Green vegetables | 10–18 years | M/F | Farmworker schoolchildren (n = 38) Urban schoolchildren (n = 28) | SRQ: Current work status/work history ENV: Non-work chemical exposures-Exposure index | Neurobehavioural tests-BARS | Medium |
| Callahan et al. Egypt * (2014) [55] | Pesticides: Chlorpyrifos | Agriculture: Cotton | 12–19 years ** | M | Pesticide applicators (n = 38) Non-applicators (n = 24) | SRQ: Current work status/ non-work chemical exposures) BIO: Urinary TCPy | Self-reported wheeze Lung function | Medium |
| Rohlman et al. Egypt (2014) [63] | Pesticides: Chlorpyrifos | Agriculture: Cotton | 12–18 years | M/F | Pesticide applicators (n = 21) Non applicators (n = 20) | SRQ: Current work status/work history BIO: Urinary TCPy. Plasma AChE/BChE | Neurobehavioural tests-BARS/WAIS | Medium |
| Saddik at al Lebanon (2009) [64] *** | Solvents | Auto spray painting, mechanical repair and furniture painting workshops | 10–17 years | M | Solvent-exposed workers (n = 100) Non-exposed workers (n = 100) Non-working, non-exposed schoolchildren (n = 100) | SRQ: Current work status/work history ENV: Ambient air levels of six solvents | Neurobehavioural tests-PIPS/non-computerised tests Mood-POMS | Good |
| Saddik at al Lebanon (2003) [65] *** | Solvents | Auto spray painting, mechanical repair, furniture painting workshops | 10–17 years | M | Solvent-exposed workers (n = 100) Non-exposed workers (n = 100) Non-working, non-exposed schoolchildren (n = 100) | SRQ: Current work status/work history | Neurological symptoms Neurobehavioural tests-PIPS | Medium |
| Saddik at al Lebanon (2005) [66] *** | Solvents | Auto spray painting, mechanical repair and furniture painting workshops | 10–17 years | M | Solvent-exposed workers (n = 100) Non-exposed workers (n = 100) Non-working, non-exposed schoolchildren (n = 100) | SRQ: Current work status/work history | Neurological symptoms Neurobehavioural tests-non computerised tests Mood-POMS | Medium |
| Nuwayhid et al. Lebanon (2005) [67] | Metals: Lead | Carpentry, mechanics, metal works | 10–17 years | M | Workers (n = 78) Non-workers (n = 60) | SRQ: Work history | Mental health Physical exam Blood lead Haemoglobin/ferritin | Good |
| Moawad et al. Egypt (2015) [68] | Metals: Lead | Auto repair, car batteries, smelters, radiators, pottery workshops, garbage collection | 6–18 years | M/F | Non-workers with moderate living standard (n = 100) Non-workers in slums (n = 100) Schoolchildren (suburban n = 70; urban n = 30) Workshop group (n = 100) | SRQ: CL status ENV: Water, dust, soil ***** | Blood lead Haemoglobin | Good |
| Sughis et al. Pakistan (2012) [59] | Metals: Various | Surgical instrument manufacture | 10–14 years | M | Exposed workers (n = 104) Schoolchildren (n = 75) | BIO: Urine chromium and nickel concentrations | Respiratory symptoms Lung function-spirometry Blood pressure Oxidative DNA damage | Good |
| Arif et al. Bangladesh (2018) [69] | Metals: Lead | Battery recycling | 10–14 years | M | Exposed workers (n = 30) Non-exposed workers | SRQ: Current work status/work history BIO: Minimum blood lead concentration | Oxidative stress DNA damage-Comet assay Growth retardation | Medium |
| Shah et al. Pakistan (2012) [13] | Metals: Lead | Battery recycling | 12–15 years | M | Exposed workers (n = 118) Exposed non-workers (n = 89) Non-exposed (n = 95) | SRQ: Current work status/work history | Blood lead | Medium |
| Dundar et al. Turkey (2005) [70] | Metals: Lead | Auto repair | 15–17 years | M | Exposed workers (n = 42) Non-exposed (n = 55) | SRQ: Work history | Blood lead concentration Thyroid function-TSH/ FT4/FT3 Thyroid volume-ultrasound | Medium |
| Baloch et al. Pakistan (2020) [58] | Metals: Lead, Cadmium | Battery recycling, welding | 12–18 years | M | 12–18 years Battery workers (n = 95) Welding workers (n = 60) Non-exposed (n = 100) 20–45 years Battery workers (n = 100) Welding workers (n = 120) Non-exposed (n = 145) | SRQ: Current work status/work history ENV: Water, soil ***** | Blood/hair lead/cadmium Haemoglobin | Medium |
| Bose-O’Reilly et al. Indonesia/ Zimbabwe (2008) [71] | Metals: Mercury | Gold mining | 9–17 years | M/F | Exposed workers (n = 80) Children living in exposed areas (n = 80) Non-exposed (n = 50) | SRQ: Current work status/work history | Blood/urine/hair mercury Medical symptoms Neurobehavioural tests | Medium |
| Junaid et al. Pakistan (2017) [72] | Metals: Various | Leather and surgical instrument manufacturing | 8–18 years | M/F | Exposed workers (n = 60) Unexposed (n = 15) | SRQ: Current work status/work history ENV: Equation to measure exposure from inhalation, ingestion and dermal contact | Blood/urine/saliva/hair various metals | Medium |
| Sughis et al. Pakistan (2014) [73] | Metals: Various | Carpet weaving, brick industry | 8–12 years | M/F | Carpet weaving workers (n = 80) Brick industry workers (n = 80) School: high air pollution area (n = 100) School: lower air pollution area (n = 79) | SRQ: Current work status/work history ENV: Water and particulate matter | Urine various metals | Medium |
| Kazi et al. Pakistan (2015) [57] | Metals: Lead | Battery recycling | 12–15 years | M | Exposed workers (n = 118) Exposed non-workers (n = 85) Non-exposed (n = 90) | SRQ: Work history | Hair lead | Low |
| Tiwari et al. India (2012) [16] | Metals: Chromium | Gem polishing | <14 years | M/F | Gem polishing workers (n = 24) Non-workers (n = 23) | SRQ: Current work status/work history | Blood chromium | Low |
| Lahiry et al. Bangladesh (2011) [14] | Metals: Various | Waste disposal | 8–15 years | M/F | Waste disposal workers (n = 20) Non-workers (n = 15) | SRQ: CL status | Oxidative stress DNA damage-Comet assay Liver function tests | Low |
| Cuadra et al. Nicaragua (2006) [74] **** | POPs: Various | Waste disposal | 11–15 years | M/F | Workers living onsite (n = 11) Workers living nearby (n = 23) Non-workers living nearby (n = 16) Non-workers living nearby/not eating lake fish (n = 16) Non-workers living remotely/not eating lake fish (n = 11) | SRQ: Current work status/work history/diet | Serum POP POP metabolites | Medium |
| Athanasiadou et al. Nicaragua (2008) [15] **** | POPs: PBDE | Waste disposal | 11–15 years | M/F | Workers living onsite (n = 19) Workers living nearby (n = 44) Non-workers living nearby (n = 31) Non-workers living nearby/not eating lake fish (n = 18) Non-workers living remotely/not eating lake fish (n = 19) | SRQ: Current work status/work history/diet | Serum PBDE PBDE metabolites | Medium |
| Category | Key Areas |
|---|---|
| Health outcomes | No studies looked at acute poisoning cases for example, despite a high incidence of work-related poisoning cases in children, both in the developed [120] and developing world [121]. Neurobehavioural deficits due to lead exposure. Long-term health outcomes e.g., chronic conditions in adulthood and diseases with long latencies, such as cancers. |
| Chemical types | Ammonia and chlorine-based bleaches, for example used by child labourers working in domestic cleaning roles. Further pesticide studies are needed due to the high proportion of child labourers working in agriculture. |
| Industries | Transport and construction were identified as being particularly hazardous to child labourers [10]. No studies were found looking at chemical exposures in these areas. |
| Countries | Few or no studies were found from China, Africa, Latin America. An expanded database search is recommended for these areas, looking at non-English language papers. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scott, N.B.; Pocock, N.S. The Health Impacts of Hazardous Chemical Exposures among Child Labourers in Low- and Middle-Income Countries. Int. J. Environ. Res. Public Health 2021, 18, 5496. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18105496
Scott NB, Pocock NS. The Health Impacts of Hazardous Chemical Exposures among Child Labourers in Low- and Middle-Income Countries. International Journal of Environmental Research and Public Health. 2021; 18(10):5496. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18105496
Chicago/Turabian StyleScott, Natasha B., and Nicola S. Pocock. 2021. "The Health Impacts of Hazardous Chemical Exposures among Child Labourers in Low- and Middle-Income Countries" International Journal of Environmental Research and Public Health 18, no. 10: 5496. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18105496