
Pain Status and Its Association with Physical Activity, Psychological Stress, and Telework among Japanese Workers with Pain during the COVID-19 Pandemic

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
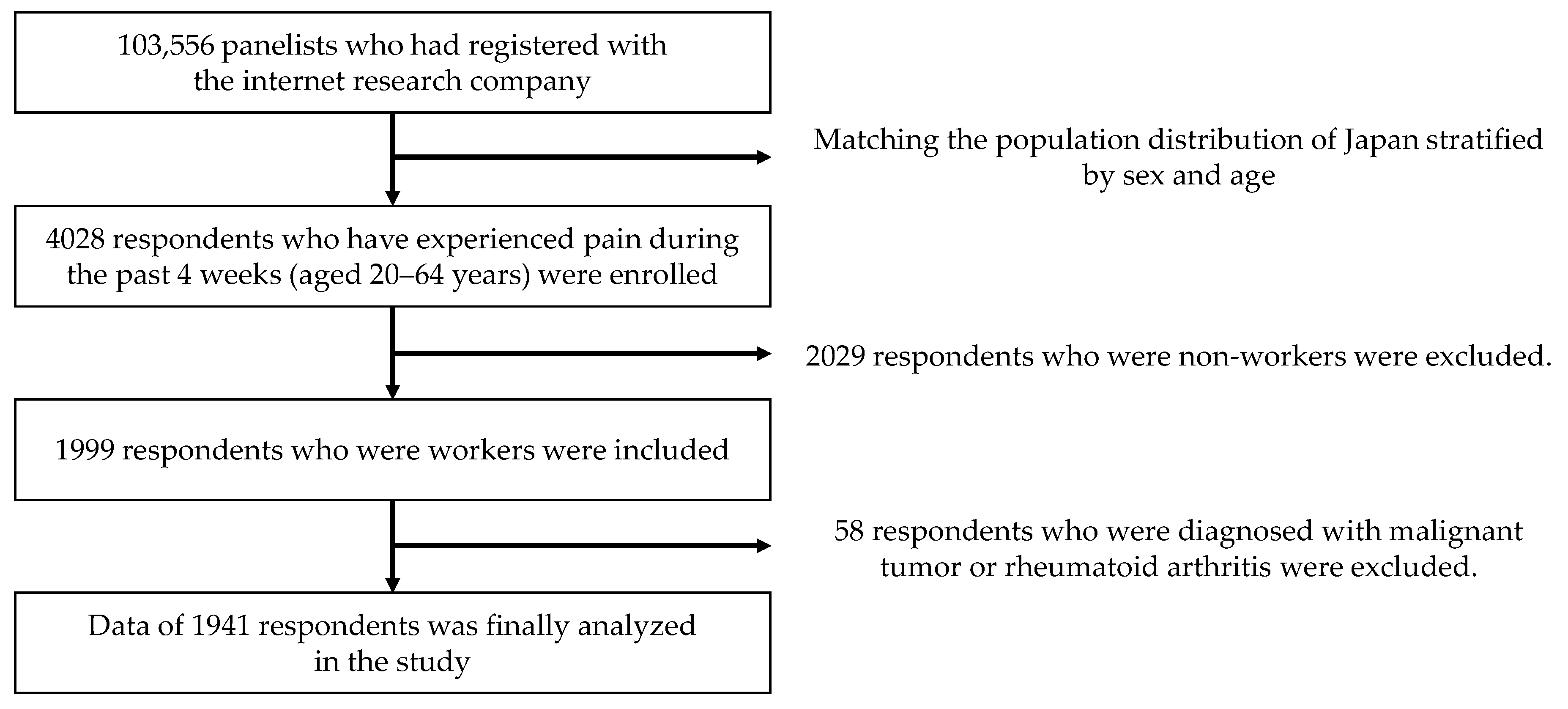
2.1. Study Population
2.2. Measurements
2.3. Statistical Analyses
3. Results
4. Discussion
4.1. Telework and Pain
4.2. Physical Activity and Pain
4.3. Psychological Stress and Pain
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sen-Crowe, B.; McKenney, M.; Elkbuli, A. Social distancing during the COVID-19 pandemic: Staying home save lives. Am. J. Emerg. Med. 2020, 38, 1519–1520. [Google Scholar] [CrossRef]
- Islam, N.; Sharp, S.J.; Chowell, G.; Shabnam, S.; Kawachi, I.; Lacey, B.; Massaro, J.M.; D’Agostino, R.B., Sr.; White, M. Physical distancing interventions and incidence of coronavirus disease 2019: Natural experiment in 149 countries. BMJ 2020, 370, m2743. [Google Scholar] [CrossRef]
- Prime Minister of Japan and His Cabinet. [COVID-19] Declaration of a State of Emergency in Response to the Novel Coronavirus Disease (16 April). Available online: https://japan.kantei.go.jp/ongoingtopics/_00020.html (accessed on 4 April 2021).
- Stewart, W.F.; Ricci, J.A.; Chee, E.; Morganstein, D.; Lipton, R. Lost productive time and cost due to common pain conditions in the US workforce. JAMA 2003, 290, 2443–2454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rice, A.S.C.; Smith, B.H.; Blyth, F.M. Pain and the global burden of disease. Pain 2016, 157, 791–796. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoshimoto, T.; Oka, H.; Fujii, T.; Nagata, T.; Matsudaira, K. The Economic Burden of Lost Productivity due to Presenteeism Caused by Health Conditions Among Workers in Japan. J. Occup. Environ. Med. 2020, 62, 883–888. [Google Scholar] [CrossRef] [PubMed]
- Clauw, D.J.; Hauser, W.; Cohen, S.P.; Fitzcharles, M.A. Considering the potential for an increase in chronic pain after the COVID-19 pandemic. Pain 2020, 161, 1694–1697. [Google Scholar] [CrossRef]
- Hruschak, V.; Flowers, K.M.; Azizoddin, D.R.; Jamison, R.N.; Edwards, R.R.; Schreiber, K.L. Cross-sectional study of psychosocial and pain-related variables among patients with chronic pain during a time of social distancing imposed by the coronavirus disease 2019 pandemic. Pain 2021, 162, 619–629. [Google Scholar] [CrossRef]
- Sagat, P.; Bartik, P.; Prieto Gonzalez, P.; Tohanean, D.I.; Knjaz, D. Impact of COVID-19Quarantine on Low Back Pain Intensity, Prevalence, and Associated Risk Factors among Adult Citizens Residing in Riyadh (Saudi Arabia): A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2020, 17, 7302. [Google Scholar] [CrossRef]
- Nieto, R.; Pardo, R.; Sora, B.; Feliu-Soler, A.; Luciano, J.V. Impact of COVID-19 Lockdown Measures on Spanish People with Chronic Pain: An Online Study Survey. J. Clin. Med. 2020, 9, 3558. [Google Scholar] [CrossRef]
- Mustajab, D.; Bauw, A.; Rasyid, A.; Irawan, A.; Akbar, M.; Hamid, M.A. Working From Home Phenomenon As an Effort to Prevent COVID-19 Attacks and Its Impacts on Work Productivity. TIJAB 2020, 4, 13. [Google Scholar] [CrossRef]
- Moretti, A.; Menna, F.; Aulicino, M.; Paoletta, M.; Liguori, S.; Iolascon, G. Characterization of Home Working Population during COVID-19 Emergency: A Cross-Sectional Analysis. Int. J. Environ. Res. Public Health 2020, 17, 6284. [Google Scholar] [CrossRef] [PubMed]
- Tison, G.H.; Avram, R.; Kuhar, P.; Abreau, S.; Marcus, G.M.; Pletcher, M.J.; Olgin, J.E. Worldwide Effect of COVID-19 on Physical Activity: A Descriptive Study. Ann. Intern. Med. 2020, 173, 767–770. [Google Scholar] [CrossRef] [PubMed]
- Fuzeki, E.; Groneberg, D.A.; Banzer, W. Physical activity during COVID-19 induced lockdown: Recommendations. J. Occup. Med. Toxicol. 2020, 15, 25. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, T.; Uchiumi, C.; Suzuki, N.; Yoshimoto, J.; Murillo-Rodriguez, E. The Psychological Impact of ‘Mild Lockdown’ in Japan during the COVID-19 Pandemic: A Nationwide Survey under a Declared State of Emergency. Int. J. Environ. Res. Public Health 2020, 17, 9382. [Google Scholar] [CrossRef]
- Giorgi, G.; Lecca, L.I.; Alessio, F.; Finstad, G.L.; Bondanini, G.; Lulli, L.G.; Arcangeli, G.; Mucci, N. COVID-19-Related Mental Health Effects in the Workplace: A Narrative Review. Int. J. Environ. Res. Public Health 2020, 17, 7857. [Google Scholar] [CrossRef]
- Alzahrani, H.; Mackey, M.; Stamatakis, E.; Zadro, J.R.; Shirley, D. The association between physical activity and low back pain: A systematic review and meta-analysis of observational studies. Sci. Rep. 2019, 9, 8244. [Google Scholar] [CrossRef]
- Landmark, T.; Romundstad, P.R.; Borchgrevink, P.C.; Kaasa, S.; Dale, O. Longitudinal associations between exercise and pain in the general population—The HUNT pain study. PLoS ONE 2013, 8, e65279. [Google Scholar] [CrossRef] [Green Version]
- Crofford, L.J. Psychological aspects of chronic musculoskeletal pain. Best Pract. Res. Clin. Rheumatol. 2015, 29, 147–155. [Google Scholar] [CrossRef] [Green Version]
- Statistics of Japan. Population Estimates (Survey Date 2018). Available online: https://www.e-stat.go.jp/en/stat-search/files?page=1&layout=datalist&toukei=00200524&tstat=000000090001&cycle=7&year=20180&month=0&tclass1=000001011679&tclass2val=0 (accessed on 7 May 2021).
- Ministry of Internal Affairs and Communications. Japanese Standard Industrial Classification. Available online: https://www.soumu.go.jp/toukei_toukatsu/index/seido/sangyo/H25index.htm(accessed on 4 April 2021).
- Asundi, K.; Odell, D.; Luce, A.; Dennerlein, J.T. Notebook computer use on a desk, lap and lap support: Effects on posture, performance and comfort. Ergonomics 2010, 53, 74–82. [Google Scholar] [CrossRef] [PubMed]
- Yu, Z.; James, C.; Edwards, S.; Snodgrass, S.J. Differences in posture kinematics between using a tablet, a laptop, and a desktop computer in sitting and in standing. Work 2018, 61, 257–266. [Google Scholar] [CrossRef] [Green Version]
- Lis, A.M.; Black, K.M.; Korn, H.; Nordin, M. Association between sitting and occupational LBP. Eur. Spine J. 2007, 16, 283–298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xie, Y.; Szeto, G.; Dai, J. Prevalence and risk factors associated with musculoskeletal complaints among users of mobile handheld devices: A systematic review. Appl. Ergon. 2017, 59, 132–142. [Google Scholar] [CrossRef] [PubMed]
- Yassierli, Y.; Juraida, A. Effects of Netbook and Tablet Usage Postures on the Development of Fatigue, Discomfort and Pain. J. Eng. Technol. Sci. 2016, 48, 243–253. [Google Scholar] [CrossRef] [Green Version]
- Bouziri, H.; Smith, D.R.M.; Descatha, A.; Dab, W.; Jean, K. Working from home in the time of COVID-19: How to best preserve occupational health? Occup. Environ. Med. 2020, 77, 509–510. [Google Scholar] [CrossRef]
- Vlaeyen, J.W.; Kole-Snijders, A.M.; Rotteveel, A.M.; Ruesink, R.; Heuts, P.H. The role of fear of movement/(re)injury in pain disability. J. Occup. Rehabil. 1995, 5, 235–252. [Google Scholar] [CrossRef]
- Moreira-Silva, I.; Teixeira, P.M.; Santos, R.; Abreu, S.; Moreira, C.; Mota, J. The Effects of Workplace Physical Activity Programs on Musculoskeletal Pain: A Systematic Review and Meta-Analysis. Workplace Health Saf. 2016, 64, 210–222. [Google Scholar] [CrossRef] [Green Version]
- Fukushima, N.; Machida, M.; Kikuchi, H.; Amagasa, S.; Hayashi, T.; Odagiri, Y.; Takamiya, T.; Inoue, S. Associations of working from home with occupational physical activity and sedentary behavior under the COVID-19 pandemic. J. Occup. Health 2021, 63, e12212. [Google Scholar] [CrossRef]
- Rogers, A.H.; Garey, L.; Zvolensky, M.J. COVID-19 psychological factors associated with pain status, pain intensity, and pain-related interference. Cogn. Behav. Ther. 2021, 1–13. [Google Scholar] [CrossRef]
- Rhodes, S.D.; Bowie, D.A.; Hergenrather, K.C. Collecting behavioural data using the world wide web: Considerations for researchers. J. Epidemiol. Community Health 2003, 57, 68–73. [Google Scholar] [CrossRef]
- Lacasse, A.; Page, M.G.; Dassieu, L.; Sourial, N.; Janelle-Montcalm, A.; Dorais, M.; Nguena Nguefack, H.L.; Godbout-Parent, M.; Hudspith, M.; Moor, G.; et al. Impact of the COVID-19 pandemic on the pharmacological, physical, and psychological treatments of pain: Findings from the Chronic Pain & COVID-19 Pan-Canadian Study. Pain Rep. 2021, 6, e891. [Google Scholar]



{kind=link}
{kind=link}
| All | Pain | |||
|---|---|---|---|---|
| Augmented | Not Augmented | p-Value | ||
| (N = 1941) | (n = 282) | (n = 1659) | ||
| Sex, n (%) | ||||
| Men | 1368 (70.5) | 182 (64.5) | 1186 (71.5) | 0.018 |
| Women | 573 (29.5) | 100 (35.5) | 473 (28.5) | |
| Age, years | 43 (33, 52) | 40 (30, 48) | 43 (33, 52) | <0.001 |
| BMI, kg/m2 | 22.1 (19.9, 24.7) | 21.6 (19.7, 24.4) | 22.2 (20.0, 24.7) | 0.143 |
| Marital status, n (%) | ||||
| Married | 962 (49.6) | 135 (47.9) | 827 (49.8) | 0.677 |
| Unmarried | 850 (43.8) | 130 (46.1) | 720 (43.4) | |
| Divorced or widowed | 129 (6.7) | 17 (6.0) | 112 (6.8) | |
| Education level, n (%) | ||||
| No college | 813 (41.9) | 107 (37.9) | 706 (42.6) | 0.147 |
| College | 1128 (58.1) | 175 (62.1) | 953 (57.4) | |
| Employment type, n (%) | ||||
| Regular | 1167 (60.1) | 181 (64.2) | 986 (59.4) | 0.132 |
| Non-regular | 774 (39.9) | 101 (35.8) | 673 (40.6) | |
| Industry type, n (%) | ||||
| Primary industry | 21 (1.1) | 5 (1.8) | 16 (1.0) | 0.444 |
| Secondary industry | 463 (23.9) | 64 (22.7) | 399 (24.1) | |
| Tertiary industry | 1328 (68.4) | 191 (67.7) | 1137 (68.5) | |
| Others | 129 (6.6) | 22 (7.8) | 107 (6.4) | |
| Conditions during COVID-19 pandemic | ||||
| Physical activity, n (%) | ||||
| Decreased | 916 (47.2) | 208 (73.8) | 708 (42.7) | <0.001 |
| Not decreased | 1025 (52.8) | 74 (26.2) | 951 (57.3) | |
| Psychological stress, n (%) | ||||
| Increased | 908 (46.8) | 179 (63.5) | 729 (43.9) | <0.001 |
| Not increased | 1033 (53.2) | 103 (36.5) | 930 (56.1) | |
| Teleworking, n (%) | ||||
| Started/increased | 521 (26.8) | 120 (42.6) | 401 (24.2) | <0.001 |
| Not started/increased | 1420 (73.2) | 162 (57.4) | 1258 (75.8) | |
| Pain Augmented | Crude | Adjusted * | ||||
|---|---|---|---|---|---|---|
| n (%) | OR | 95%CI | OR | 95%CI | ||
| Telework | Started/increased | 120 (23.0) | 2.32 | 1.79–3.02 | 2.27 | 1.68–3.06 |
| Not started/increased | 162 (11.4) | 1.00 | 1.00 | |||
| Physical activity | Decreased | 208 (22.7) | 3.78 | 2.85–5.01 | 3.18 | 2.38–4.27 |
| Not decreased | 74 (7.2) | 1.00 | 1.00 | |||
| Psychological stress | Increased | 179 (19.7) | 2.22 | 1.71–2.88 | 2.16 | 1.64–2.84 |
| Not increased | 103 (10.0) | 1.00 | 1.00 | |||
| Pain Augmented | Crude | Adjusted * | ||||
|---|---|---|---|---|---|---|
| N | n (%) | OR | 95%CI | OR | 95%CI | |
| Telework (+) and PA decreased (+) | 326 | 93 (28.5) | 6.65 | 4.55–9.72 | 7.45 | 4.97–11.18 |
| Telework (−) and PA decreased (+) | 590 | 115 (19.5) | 4.03 | 2.82–5.77 | 3.74 | 2.60–5.38 |
| Telework (+) and PA decreased (−) | 195 | 27 (13.8) | 2.68 | 1.62–4.42 | 3.18 | 1.88–5.36 |
| Telework (−) and PA decreased (−) | 830 | 47 (5.7) | 1.00 | 1.00 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoshimoto, T.; Fujii, T.; Oka, H.; Kasahara, S.; Kawamata, K.; Matsudaira, K. Pain Status and Its Association with Physical Activity, Psychological Stress, and Telework among Japanese Workers with Pain during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 5595. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115595
Yoshimoto T, Fujii T, Oka H, Kasahara S, Kawamata K, Matsudaira K. Pain Status and Its Association with Physical Activity, Psychological Stress, and Telework among Japanese Workers with Pain during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2021; 18(11):5595. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115595
Chicago/Turabian StyleYoshimoto, Takahiko, Tomoko Fujii, Hiroyuki Oka, Satoshi Kasahara, Kayo Kawamata, and Ko Matsudaira. 2021. "Pain Status and Its Association with Physical Activity, Psychological Stress, and Telework among Japanese Workers with Pain during the COVID-19 Pandemic" International Journal of Environmental Research and Public Health 18, no. 11: 5595. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115595