
Utilising a Behaviour Change Model to Improve Implementation of the Activate Injury Prevention Exercise Programme in Schoolboy Rugby Union


Abstract
:1. Introduction
2. Materials and Methods
2.1. Recruitment
2.2. Baseline Survey
2.3. Workshop
2.4. Post-Workshop Survey
2.5. Post-Season Survey
2.6. Analysis
3. Results
3.1. Workshop Attendance and Perceptions towards Injury Risk and Prevention
3.2. Workshop Attendance and Outcome Behaviour
3.3. Workshop Attendance and Post-Season HAPA Constructs
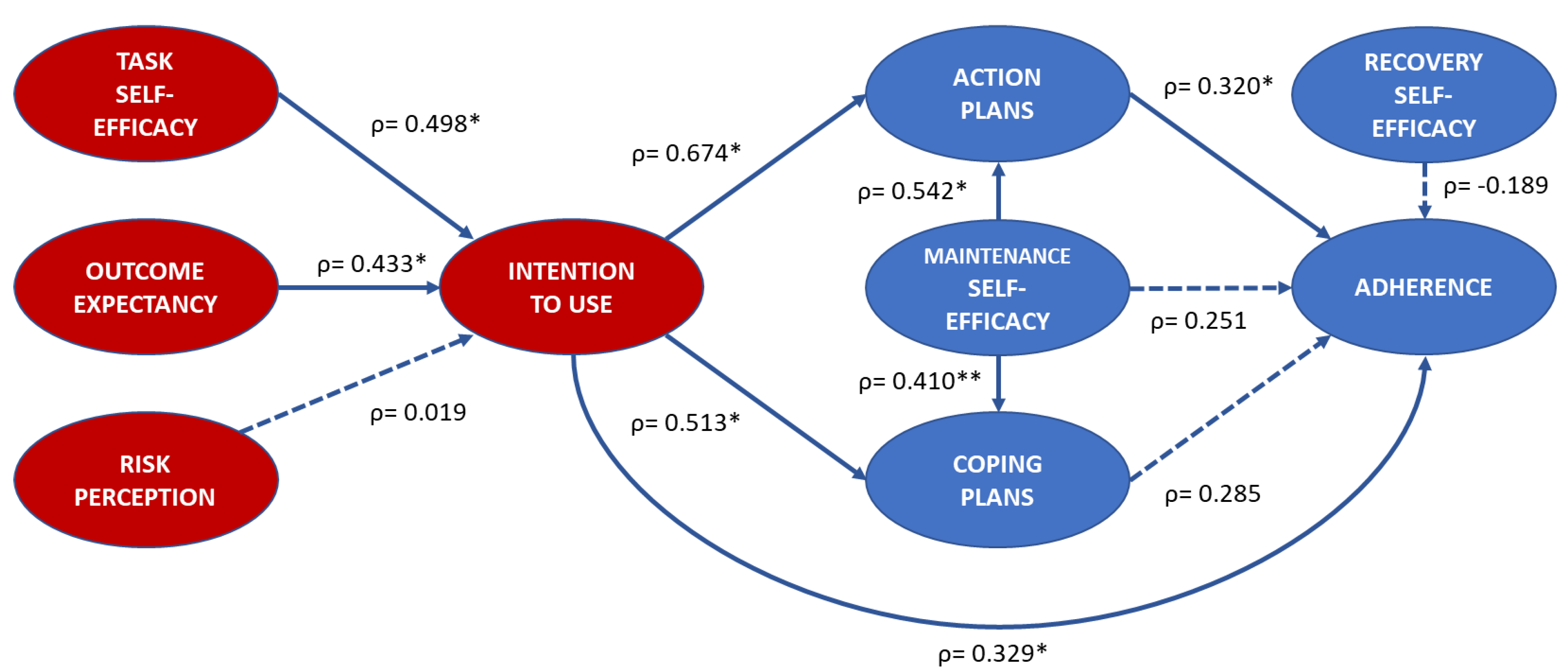
3.4. Exploratory Analysis of HAPA Constructs and Activate Adherence
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hislop, M.D.; Stokes, K.A.; Williams, S.; McKay, C.D.; England, M.; Kemp, S.P.; Trewartha, G. The efficacy of a movement control exercise programme to reduce injuries in youth rugby: A cluster randomised controlled trial. BMJ Open Sport Exerc. Med. 2016, 2, e000043. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hislop, M.D.; Stokes, K.A.; Williams, S.; McKay, C.D.; England, M.E.; Kemp, S.P.T.; Trewartha, G. Reducing musculoskeletal injury and concussion risk in schoolboy rugby players with a pre-activity movement control exercise programme: A cluster randomised controlled trial. Br. J. Sports Med. 2017, 51, 1140–1146. [Google Scholar] [CrossRef]
- Lindblom, H.; Walden, M.; Carlfjord, S.; Hagglund, M. Implementation of a neuromuscular training programme in female adolescent football: 3-year follow-up study after a randomised controlled trial. Br. J. Sports Med. 2014, 48, 1425–1430. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hanson, D.; Allegrante, D.E.; Sleet, D.A.; Finch, C. Research alone is not sufficient to prevent sports injury. Br. J. Sports Med. 2012, 48, 682–684. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andersson, S.H.; Bahr, R.; Olsen, M.J.; Myklebust, G. Attitudes, beliefs, and behavior toward shoulder injury prevention in elite handball: Fertile ground for implementation. Scand. J. Med. Sci. Sports 2019, 29, 1996–2009. [Google Scholar] [CrossRef]
- Finch, C.F. No longer lost in translation: The art and science of sports injury prevention implementation research. Br. J. Sports Med. 2011, 45, 1253–1257. [Google Scholar] [CrossRef] [Green Version]
- Finch, C. A new framework for research leading to sports injury prevention. J. Sci. Med. Sport 2006, 9, 3–9. [Google Scholar] [CrossRef]
- Verhagen, E.A.; van Stralen, M.M.; van Mechelen, W. Behaviour, the key factor for sports injury prevention. Sports Med. 2010, 40, 899–906. [Google Scholar] [CrossRef]
- Tee, J.C.; McLaren, S.J.; Jones, B. Sports Injury Prevention is Complex: We Need to Invest in Better Processes, Not Singular Solutions. Sports Med. 2020, 50, 689–702. [Google Scholar] [CrossRef]
- O’Brien, J.; Finch, C.F. A systematic review of core implementation components in team ball sport injury prevention trials. Inj. Prev. 2014, 20, 357–362. [Google Scholar] [CrossRef] [Green Version]
- Emery, C.A.; Hagel, B.; Morrongiello, B.A. Injury prevention in child and adolescent sport: Whose responsibility is it? Clin. J. Sport Med. 2006, 16, 514–521. [Google Scholar] [CrossRef] [PubMed]
- Barden, C.; Stokes, K.A.; McKay, C.D. Implementation of the Activate injury prevention exercise programme in English schoolboy rugby union. BMJ Open Sport Exerc. Med. 2021, 7, 1–10. [Google Scholar] [CrossRef]
- Steffen, K.; Meeuwisse, W.H.; Romiti, M.; Kang, J.; McKay, C.; Bizzini, M.; Dvorak, J.; Finch, C.; Myklebust, G.; Emery, C.A. Evaluation of how different implementation strategies of an injury prevention programme (FIFA 11+) impact team adherence and injury risk in Canadian female youth football players: A cluster-randomised trial. Br. J. Sports Med. 2013, 47, 480–487. [Google Scholar] [CrossRef] [PubMed]
- McKay, C.D.; Steffen, K.; Romiti, M.; Finch, C.F.; Emery, C.A. The effect of coach and player injury knowledge, attitudes and beliefs on adherence to the FIFA 11+ programme in female youth soccer. Br. J. Sports Med. 2014, 48, 1281–1286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gianotti, S.M.; Quarrie, K.L.; Hume, P.A. Evaluation of RugbySmart: A rugby union community injury prevention programme. J. Sci. Med. Sport 2009, 12, 371–375. [Google Scholar] [CrossRef] [PubMed]
- Brown, J.C.; Verhagen, E.; Knol, D.; Van Mechelen, W.; Lambert, M.I. The effectiveness of the nationwide BokSmart rugby injury prevention program on catastrophic injury rates. Scand. J. Med. Sci. Sports 2016, 26, 221–225. [Google Scholar] [CrossRef] [PubMed]
- Owoeye, O.B.A.; McKay, C.D.; Raisanen, A.M.; Hubkarao, T.; Palacios-Derflingher, L.; Emery, C.A. Psychosocial Factors and the Effects of a Structured Injury Prevention Workshop on Coaches’ Self-Efficacy to Implement the 11+ Exercise Program. Int. J. Exerc. Sci. 2020, 13, 1459–1475. [Google Scholar] [PubMed]
- Frank, B.; Register-Mihalik, J.; Padua, D. High levels of coach intent to integrate a ACL injury prevention program into training does not translate to effective implementation. J. Sci. Med. Sport 2015, 18, 400–406. [Google Scholar] [CrossRef] [PubMed]
- McGlashen, A.J.; Finch, C. The Extent to Which Behavioural and Social Sciences Theories and Models are Used in Sport Injury Prevention Research. Sports Med. 2010, 40, 841–858. [Google Scholar] [CrossRef]
- Schwarzer, R. Health Action Process Approach (HAPA) as a Theoretical Framework to Understand Behavior Change. Actual. Psicol. 2016, 30, 119–130. [Google Scholar] [CrossRef]
- Schwarzer, R. Self-Efficacy and Health Behaviours; Open University Press: Berkshire, UK, 1995. [Google Scholar]
- Scholz, U.; Sniehotta, F.F.; Schwarzer, R. Predicting physical exercise in cardiac rehabilitation: The role of phase-specific self-efficacy beliefs. J. Sport Exerc. Psychol. 2005, 27, 135–151. [Google Scholar] [CrossRef]
- Renner, B.; Schwarzer, R. The motivation to eat a healthy diet: How intenders and nonintenders differ in terms of risk perception, outcome expectancies, self-efficacy and nutrition behavior. Pol. Psychol. Bull. 2005, 36, 7–15. [Google Scholar]
- Barg, C.J.; Latimer, A.E.; Pomery, E.A.; Rivers, S.E.; Rench, T.A.; Prapavessis, H.; Salovey, P. Examining predictors of physical activity among inactive middle-aged women: An application of the health action process approach. Psychol. Health 2012, 27, 829–845. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hislop, M.D. Injury Risk Factors and Prevention Strategies in Schoolboy Rugby Union. Ph.D. Thesis, University of Bath, Bath, UK, 2017. [Google Scholar]
- McKay, C.D.; Merrett, C.K.; Emery, C.A. Predictors of FIFA 11+ Implementation Intention in Female Adolescent Soccer: An Application of the Health Action Process Approach (HAPA) Model. Int. J. Environ. Res. Public Health 2016, 13, 657. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Brien, J.; Finch, C.F. Injury Prevention Exercise Programs for Professional Soccer: Understanding the Perceptions of the End-Users. Clin. J. Sport Med. 2017, 27, 1–9. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, J.; Finch, C.F. Injury prevention exercise programmes in professional youth soccer: Understanding the perceptions of programme deliverers. BMJ Open Sport Exerc. Med. 2016, 2, e000075. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Friedman, H.H.; Amoo, T. Rating the rating scales. J. Mark. Manag. 1999, 9, 114–123. [Google Scholar]
- Bandura, A. Self-Efficacy: The Exercise of Control; Worth Publishers: Broadway, UK, 1997. [Google Scholar]
- Attwood, M.J.; Roberts, S.P.; Trewartha, G.; England, M.E.; Stokes, K.A. Efficacy of a movement control injury prevention programme in adult men’s community rugby union: A cluster randomised controlled trial. Br. J. Sports Med. 2018, 52, 368–374. [Google Scholar] [CrossRef]
- Streiner, D.L. Starting at the beginning: An introduction to coefficient alpha and internal consistency. J. Pers. Assess. 2003, 80, 99–103. [Google Scholar] [CrossRef]
- Hopkins, W.G. New View of Statistics. Available online: http://www.sportsci.org/resource/stats/effectmag.html (accessed on 20 January 2021).
- Donaldson, A.; Callaghan, A.; Bizzini, M.; Jowett, A.; Keyzer, P.; Nicholson, M. Awareness and use of the 11+injury prevention program among coaches of adolescent female football teams. Int. J. Sports Sci. Coach. 2018, 13, 929–938. [Google Scholar] [CrossRef]
- Wilke, J.; Niederer, D.; Vogt, L.; Banzer, W. Is the message getting through? Awareness and use of the 11+ injury prevention programme in amateur level football clubs. PLoS ONE 2018, 13, e0195998. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Norcross, M.F.; Johnson, S.T.; Bovbjerg, V.E.; Koester, M.C.; Hoffman, M.A. Factors influencing high school coaches’ adoption of injury prevention programs. J. Sci. Med. Sport 2016, 19, 299–304. [Google Scholar] [CrossRef] [PubMed]
- Donaldson, A.; Finch, C. Planning for implementation and translation: Seek first to understand the end-users’ perspectives. Br. J. Sports Med. 2012, 46. [Google Scholar] [CrossRef] [PubMed]
- Hind, K.; Konerth, N.; Entwistle, I.; Theadom, A.; Lewis, G.; King, D.; Chazot, P.; Hume, P. Cumulative Sport-Related Injuries and Longer Term Impact in Retired Male Elite- and Amateur-Level Rugby Code Athletes and Non-contact Athletes: A Retrospective Study. Sports Med. 2020, 50, 2051–2061. [Google Scholar] [CrossRef] [PubMed]
- Davies, M.A.M.; Judge, A.D.; Delmestri, A.; Kemp, S.P.T.; Stokes, K.A.; Arden, N.K.; Newton, J.L. Health amongst former rugby union players: A cross-sectional study of morbidity and health-related quality of life. Sci. Rep. 2017, 7, 11786. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, S.; Trewartha, G.; Kemp, S.P.; Brooks, J.H.; Fuller, C.W.; Taylor, A.E.; Cross, M.J.; Stokes, K.A. Time loss injuries compromise team success in Elite Rugby Union: A 7-year prospective study. Br. J. Sports Med. 2016, 50, 651–656. [Google Scholar] [CrossRef] [Green Version]
- Finch, C.F.; Donaldson, A. A sports setting matrix for understanding the implementation context for community sport. Br. J. Sports Med. 2010, 44, 973–978. [Google Scholar] [CrossRef] [PubMed]
- Steib, S.; Rahlf, A.L.; Pfeifer, K.; Zech, A. Dose-Response Relationship of Neuromuscular Training for Injury Prevention in Youth Athletes: A Meta-Analysis. Front. Physiol. 2017, 8, 920. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glanz, K.; Rimer, B.K.; Viswanath, K. Health Behaviour and Health Education. Theory, Research and Practice, 4th ed.; Jossey-Bass: San Francisco, CA, USA, 2008. [Google Scholar]
- Sewry, N.; Verhagen, E.; Lambert, M.; van Mechelen, W.; Brown, J. Players’ and coaches’ knowledge and awareness of the BokSmart Safe Six injury prevention programme: An ecological cross-sectional questionnaire study. BMJ Open 2017, 7, e018575. [Google Scholar] [CrossRef] [Green Version]
- Brown, J.C.; Gardner-Lubbe, S.; Lambert, M.I.; Van Mechelen, W.; Verhagen, E. The BokSmart intervention programme is associated with improvements in injury prevention behaviours of rugby union players: An ecological cross-sectional study. Inj. Prev. 2015, 21, 173–178. [Google Scholar] [CrossRef]
- Brown, J.; Gardner-Lubbe, S.; Lambert, M.; Van Mechelen, W.; Verhagen, E. Coach-directed education is associated with injury-prevention behaviour in players: An ecological cross-sectional study. Br. J. Sports Med. 2016, 52, 989–993. [Google Scholar] [CrossRef]
- Rugby Australia. Smart Rugby Policy. Available online: https://australia.rugby/-/media/rugbyau/documents/rugbyausmartrugbypolicy.pdf?la=en&hash=3CD78348D711193C5135DA24DA2FFC71#:~:text=It%20is%20a%20minimum%20requirement,are%20no%20exceptions%20to%20this (accessed on 25 February 2021).
- Garland, R. The Mid-Point on a Rating Scale: Is it Desirable. Mark. Bull. 1991, 2, 66–70. [Google Scholar]
- Choi, B.C.; Pak, A.W. A catalog of biases in questionnaires. Prev. Chronic Dis. 2005, 2, A13. [Google Scholar] [PubMed]
- Tavakol, M.; Dennick, R. Making sense of Cronbach’s alpha. Int. J. Med. Educ. 2011, 2, 53–55. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Information/Question | Response | Workshop Attendance | |
|---|---|---|---|
| No n (%) | Yes n (%) | ||
| School type | Independent (private) | 26 (74%) | 36 (88%) |
| State (government funded) | 9 (26%) | 5 (12%) | |
| Age of participant | Mean Age (SD) | 36.8 (±10.8) | 38.6 (±10.3) |
| What is your role? | Director of Sport/Rugby | 5 (14%) | 2 (5%) |
| Head Coach | 15 (43%) | 13 (32%) | |
| Assistant Coach | 7 (20%) | 19 (46%) | |
| Team manager | 3 (9%) | 5 (12%) | |
| Strength and conditioner | 2 (6%) | 0 (0%) | |
| Medical practitioner | 3 (9%) | 2 (5%) | |
| If coaching, what age groups do you coach? | |||
| Under-12/13 | 2 (7%) | 2 (6%) | |
| Under-14/15 | 5 (19%) | 11 (32%) | |
| Under-16 | 2 (7%) | 3 (9%) | |
| Under-17/18/19 | 8 (30%) | 11 (32%) | |
| Various | 10 (37%) | 7 (21%) | |
| If coaching, how many years coaching experience do you have? | |||
| Less than 2 years | 3 (11%) | 3 (9%) | |
| 2–3 years | 1 (4%) | 4 (12%) | |
| 4–5 years | 3 (11%) | 3 (9%) | |
| 6+ years | 20 (74%) | 24 (70%) | |
| What is the highest coaching qualification you hold? | |||
| RFU Level 1 | 2 (7%) | 8 (23%) | |
| RFU Level 2 | 11 (41%) | 12 (35%) | |
| RFU Level 3 | 7 (26%) | 7 (21%) | |
| RFU Level 4 | 3 (11%) | 1 (3%) | |
| None | 3 (11%) | 5 (15%) | |
| Unknown | 1 (4%) | 1 (3%) | |
| Have you ever used a specific programme to reduce injury risk amongst your players? | |||
| No | 22 (63%) | 24 (59%) | |
| Yes | 13 (37%) | 17 (41%) | |
| Construct | Questions | Workshop Attendance | Z Score | Cronbach’s Alpha (α) | |
|---|---|---|---|---|---|
| No | Yes | ||||
| Outcome Expectancy | 2 | 0.32 (0.27–0.37) | 0.27 (0.24–0.30) | −1.49 | 0.585 |
| Task Self-efficacy | 2 | 0.31 (0.27–0.35) | 0.22 (0.19–0.24) | −3.46 * | 0.625 |
| Intention | 1 | 0.47 (0.40–0.54) | 0.29 (0.24–0.34) | −4.33 * | - |
| Action Planning | 2 | 0.49 (0.44–0.55) | 0.39 (0.34–0.43) | −2.61 | 0.716 |
| Coping Plans | 2 | 0.53 (0.48–0.58) | 0.42 (0.37–0.47) | −3.21 | 0.810 |
| Maintenance Self-efficacy | 3 | 0.48 (0.42–0.54) | 0.39 (0.34–0.43) | −2.28 | 0.733 |
| Recovery Self-efficacy | 1 | 0.44 (0.37–0.50) | 0.36 (0.32–0.40) | −1.75 | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barden, C.; Stokes, K.A.; McKay, C.D. Utilising a Behaviour Change Model to Improve Implementation of the Activate Injury Prevention Exercise Programme in Schoolboy Rugby Union. Int. J. Environ. Res. Public Health 2021, 18, 5681. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115681
Barden C, Stokes KA, McKay CD. Utilising a Behaviour Change Model to Improve Implementation of the Activate Injury Prevention Exercise Programme in Schoolboy Rugby Union. International Journal of Environmental Research and Public Health. 2021; 18(11):5681. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115681
Chicago/Turabian StyleBarden, Craig, Keith A. Stokes, and Carly D. McKay. 2021. "Utilising a Behaviour Change Model to Improve Implementation of the Activate Injury Prevention Exercise Programme in Schoolboy Rugby Union" International Journal of Environmental Research and Public Health 18, no. 11: 5681. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115681