
Short Dental Implants (≤8.5 mm) versus Standard Dental Implants (≥10 mm): A One-Year Post-Loading Prospective Observational Study

 , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Characteristics of Participants
2.2. Methodology
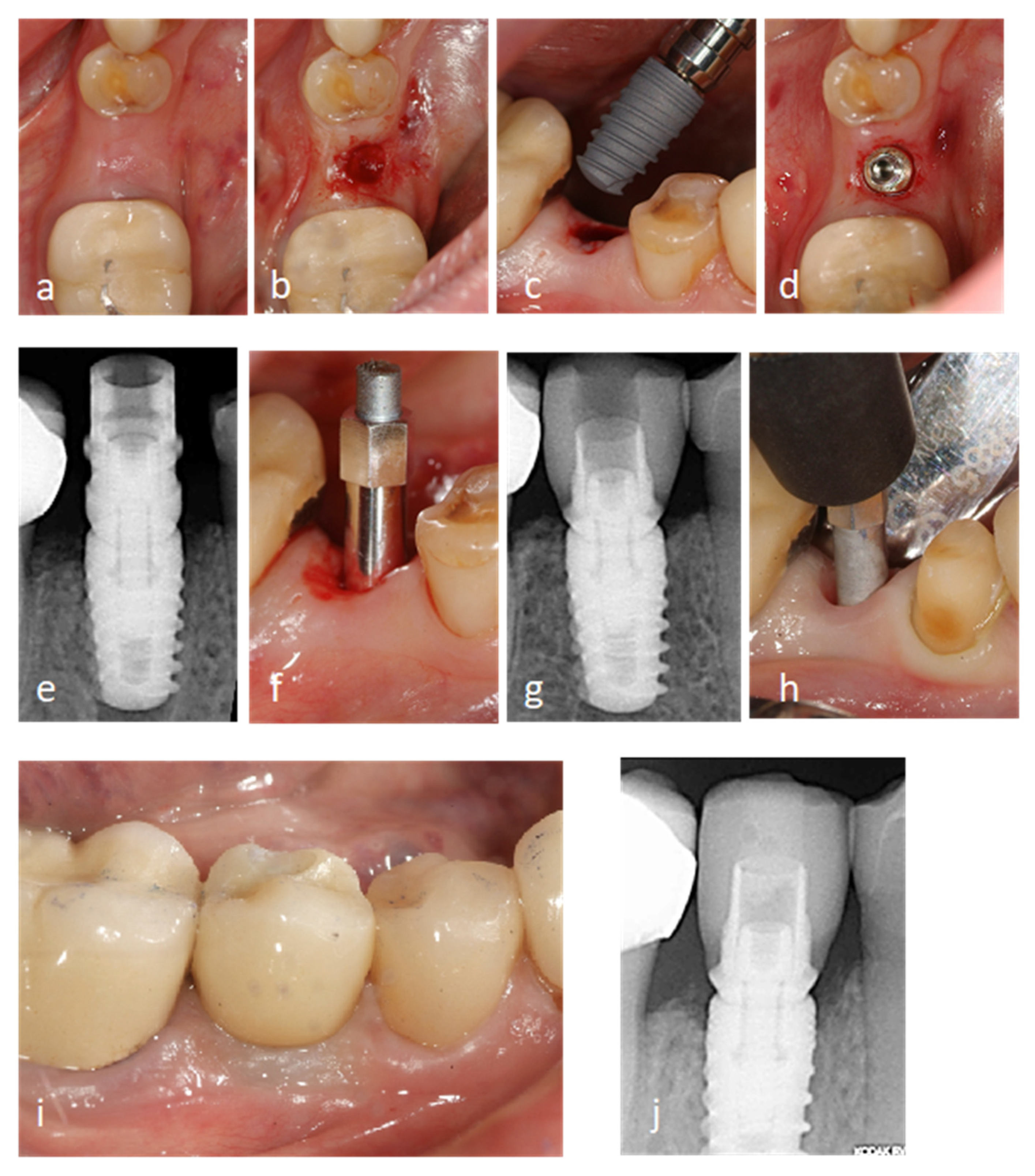
2.2.1. Surgical Procedure
2.2.2. Prosthetic Procedure
2.2.3. Clinical Examinations
2.2.4. Radiographic Measurements
2.2.5. Stability Assessment
2.3. Variables
2.4. Statistical Analysis
3. Results
3.1. Patient and Implant Characteristics
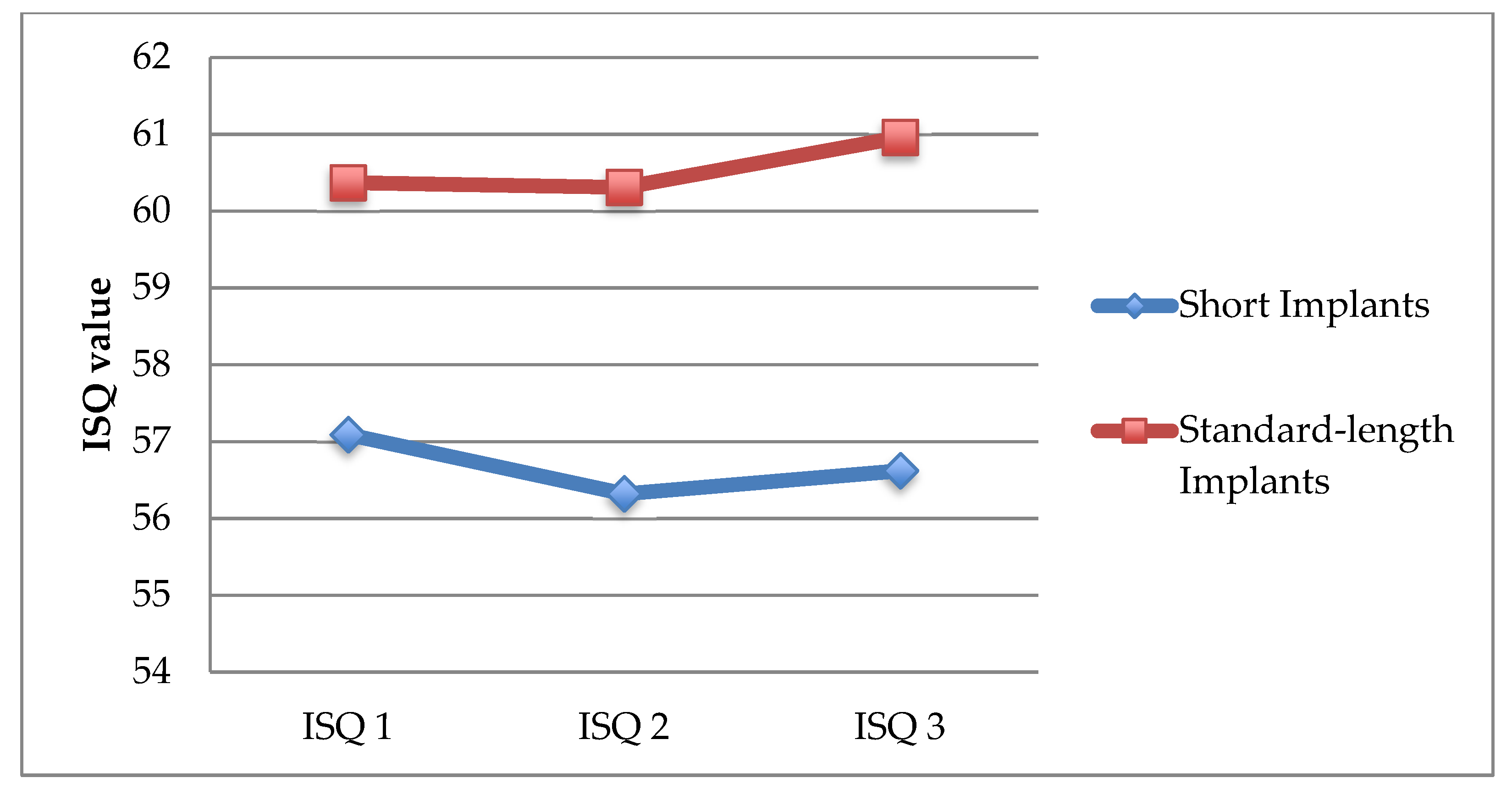
3.2. Assessment of Implant Stability (ISQ)
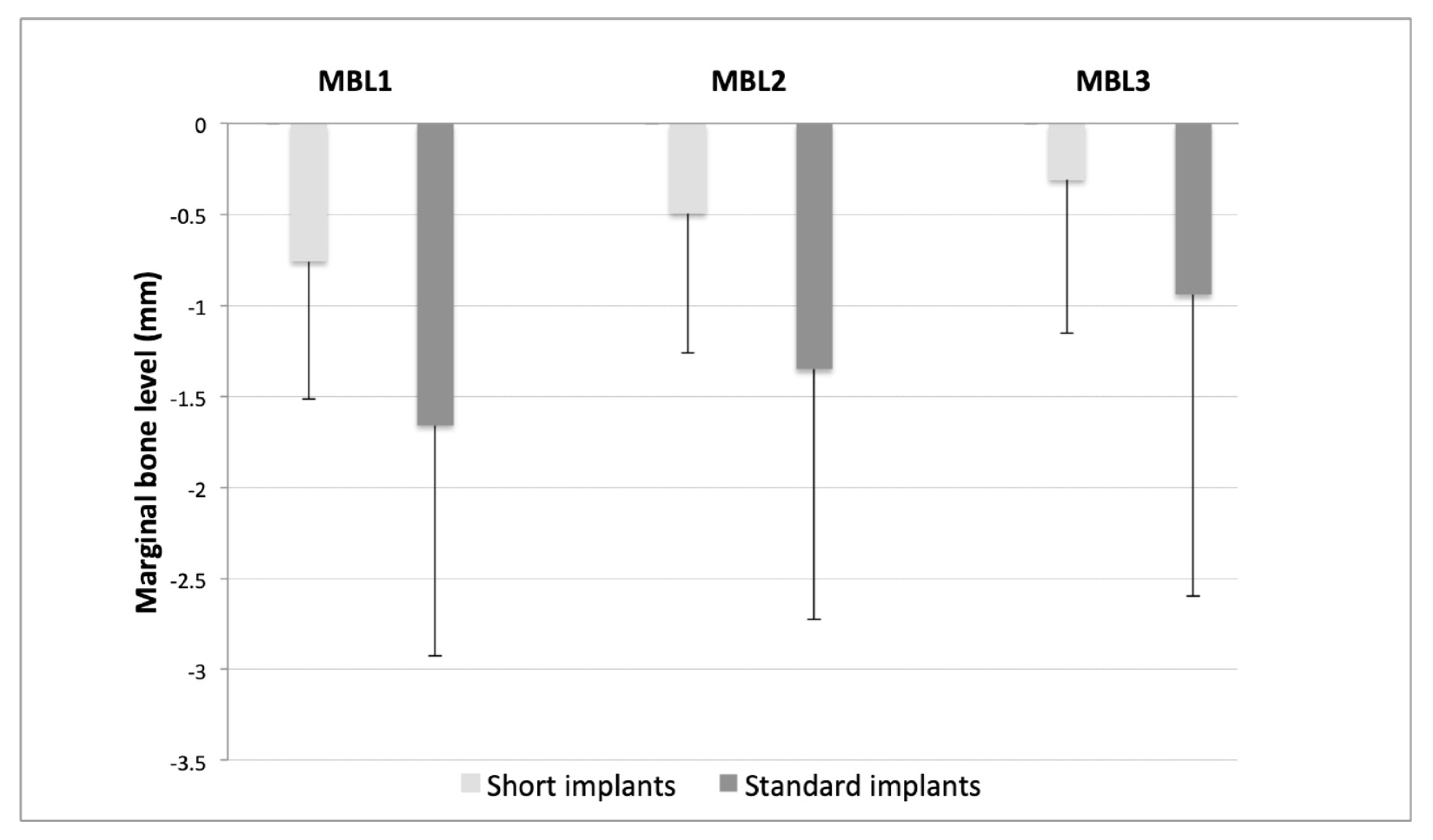
3.3. Assessment of Changes in Marginal Bone Level (MBL)
3.4. Correlation between Changes in ISQ and Marginal Bone Level (MBL) Changes According to Length, Diameter, Position, and Type of Prosthesis
3.5. Interaction between Factors (Sex and Age) with Type of Impant (Short and Standard) in ISQ and MBL Changes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Yan, Q.; Wu, X.; Su, M.; Hua, F.; Shi, B. Short implants (≤6 mm) versus longer implants with sinus floor elevation in atrophic posterior maxilla: A systematic review and meta-analysis. BMJ Open 2019, 9, e029826. [Google Scholar] [CrossRef] [PubMed]
- Atieh, M.; Zadeh, H.; Stanford, C.M.; Cooper, L.F. Survival of short dental implants for treatment of posterior partial edentulism: A systematic review. Int. J. Oral Maxillofac. Implant. 2012, 27, 1323–1331. [Google Scholar]
- Buser, D.; Mericske-Stern, R.; Bernard, J.P.P.; Behneke, A.; Behneke, N.; Hirt, H.P.; Belser, U.C.; Lang, N.P. Long-term evaluation of non-submerged ITI implants. Part 1: 8-year life table analysis of a prospective multi-center study with 2359 implants. Clin. Oral Implant. Res. 1997, 8, 161–172. [Google Scholar] [CrossRef]
- Telleman, G.; Raghoebar, G.M.; Vissink, A.; den Hartog, L.; Huddleston Slater, J.J.R.; Meijer, H.J.A. A systematic review of the prognosis of short (<10 mm) dental implants placed in the partially edentulous patient: Systematic review of short dental implants. J. Clin. Periodontol. 2011, 38, 667–676. [Google Scholar] [CrossRef] [PubMed]
- Ravidà, A.; Barootchi, S.; Askar, H.; Del Amo, F.S.-L.; Tavelli, L.; Wang, H.-L. Long-term effectiveness of extra-short (≤6 mm) dental implants: A systematic review. Int. J. Oral Maxillofac. Implant. 2019, 34, 68–84. Available online: http://quintpub.com/journals/omi/abstract.php?iss2_id=1584&article_id=19107 (accessed on 4 May 2021). [CrossRef]
- Srinivasan, M.; Vazquez, L.; Rieder, P.; Moraguez, O.; Bernard, J.-P.; Belser, U.C. Survival rates of short (6 mm) micro-rough surface implants: A review of literature and meta-analysis. Clin. Oral Implant. Res. 2014, 25, 539–545. [Google Scholar] [CrossRef]
- Thoma, D.S.; Zeltner, M.; Hüsler, J.; Hämmerle, C.H.F.; Jung, R.E. EAO supplement working group 4—EAO CC 2015 short implants versus sinus lifting with longer implants to restore the posterior maxilla: A systematic review. Clin. Oral Implant. Res. 2015, 26, 154–169. [Google Scholar] [CrossRef]
- Anitua, E.; Piñas, L.; Orive, G. Retrospective study of short and extra-short implants placed in posterior regions: Influence of crown-to-implant ratio on marginal bone loss. Clin. Implant. Dent. Relat. Res. 2015, 17, 102–110. [Google Scholar] [CrossRef]
- Esposito, M.; Felice, P.; Worthington, H.V. Interventions for replacing missing teeth: Augmentation procedures of the maxillary sinus. Cochrane Database Syst. Rev. 2014, 5. [Google Scholar] [CrossRef] [Green Version]
- Weerapong, K.; Sirimongkolwattana, S.; Sastraruji, T.; Khongkhunthian, P. Comparative study of immediate loading on short dental implants and conventional dental implants in the posterior mandible: A randomized clinical trial. Int. J. Oral Maxillofac. Implant. 2019, 34, 141–149. [Google Scholar] [CrossRef]
- Uehara, P.N.; Matsubara, V.H.; Igai, F.; Sesma, N.; Mukai, M.; Araujo, M.G. Short dental implants (≤7 mm) versus longer implants in augmented bone area: A meta-analysis of randomized controlled trials. Open Dent. J. 2018, 12, 354–365. [Google Scholar] [CrossRef]
- Esposito, M.; Pellegrino, G.; Pistilli, R.; Felice, P. Rehabilitation of postrior atrophic edentulous jaws: Prostheses supported by 5 mm short implants or by longer implants in augmented bone? One-year results from a pilot randomised clinical trial. Eur. J. Oral Implant. 2011, 4, 21–30. [Google Scholar]
- Dias, F.D.N.; Pecorari, V.; Martins, C.; Del Fabbro, M.; Casati, M. Short implants versus bone augmentation in combination with standard-length implants in posterior atrophic partially edentulous mandibles: Systematic review and meta-analysis with the Bayesian approach. Int. J. Oral Maxillofac. Surg. 2019, 48, 90–96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Misch, C.E.; Steigenga, J.; Barboza, E.; Misch-Dietsh, F.; Cianciola, L.J.; Kazor, C. Short dental implants in posterior partial edentulism: A multicenter retrospective 6-year case series study. J. Periodontol. 2006, 77, 1340–1347. [Google Scholar] [CrossRef] [PubMed]
- Anitua, E.; Orive, G.; Aguirre, J.J.; Andía, I. Five-year clinical evaluation of short dental implants placed in posterior areas: A retrospective study. J. Periodontol. 2008, 79, 42–48. [Google Scholar] [CrossRef] [PubMed]
- Lemos, C.A.A.; Ferro-Alves, M.L.; Okamoto, R.; Mendonça, M.R.; Pellizzer, E.P. Short dental implants versus standard dental implants placed in the posterior jaws: A systematic review and meta-analysis. J. Dent. 2016, 47, 8–17. [Google Scholar] [CrossRef] [Green Version]
- Anitua, E.; Alkhraisat, M.H. 15-year follow-up of short dental implants placed in the partially edentulous patient: Mandible vs maxilla. Ann. Anat. Anat. Anz. 2019, 222, 88–93. [Google Scholar] [CrossRef] [PubMed]
- Subirà-Pifarré, C.; Masuet-Aumatell, C.; Alonso, C.R.; Madrid, R.M.; Galletti, C. Assessment of dental implants with modified calcium-phosphate surface in a multicenter, prospective, non-interventional study: Results up to 50 months of follow-up. J. Funct. Biomater. 2019, 10, 5. [Google Scholar] [CrossRef] [Green Version]
- O’Leary, T.J.; Drake, R.B.; Naylor, J.E. The plaque control record. J. Periodontol. 1972, 43, 38. [Google Scholar] [CrossRef]
- Raviv, E.; Turcotte, A.; Harel-Raviv, M. Short dental implants in reduced alveolar bone height. Quintessence Int. 2010, 41, 575–579. Available online: http://www.quintpub.com/userhome/qi/qi_41_7_Raviv_8.pdf (accessed on 4 May 2021).
- Jung, R.E.; Al-Nawas, B.; Araujo, M.; Ortiz, G.A.; Barter, S.; Brodala, N.; Chappuis, V.; Chen, B.; De Souza, A.; Almeida, R.F.; et al. Group 1 ITI consensus report: The influence of implant length and design and medications on clinical and patient-reported outcomes. Clin. Oral Implant. Res. 2018, 29, 69–77. [Google Scholar] [CrossRef] [Green Version]
- Thoma, D.S.; Haas, R.; Sporniak-Tutak, K.; Garcia, A.; Taylor, T.D.; Hämmerle, C.H.F. Randomized controlled multicentre study comparing short dental implants (6 mm) versus longer dental implants (11–15 mm) in combination with sinus floor elevation procedures: 5-Year data. J. Clin. Periodontol. 2018, 45, 1465–1474. [Google Scholar] [CrossRef]
- Da Rosa de Souza, P.T.; Albini Martini, M.B.; Azevedo-Alanis, L.R. Do short implants have similar survival rates compared to standard implants in posterior single crown? A systematic review and meta-analysis. Implant. Dent. Relat. Res. 2018, 20, 890–901. [Google Scholar] [CrossRef]
- Balevi, B. In selected sites, short, rough-surfaced dental implants are as successful as long dental implants. J. Am. Dent. Assoc. 2013, 144, 195–196. [Google Scholar] [CrossRef] [PubMed]
- Queiroz, T.P.; Aguiar, S.C.; Margonar, R.; Faloni, A.P.D.S.; Gruber, R.; Luvizuto, E.R. Clinical study on survival rate of short implants placed in the posterior mandibular region: Resonance frequency analysis. Clin. Oral Implant. Res. 2015, 26, 1036–1042. [Google Scholar] [CrossRef] [PubMed]
- Albrektsson, T.; Wennerberg, A. Oral implant surfaces: Part 1–review focusing on topographic and chemical properties of different surfaces and in vivo responses to them. Int. J. Prosthodont. 2004, 17, 536–543. [Google Scholar] [PubMed]
- Wennerberg, A.; Albrektsson, T. Suggested guidelines for the topographic evaluation of implant surfaces. Int. J. Oral Maxillofac. Implant. 2000, 15, 331–344. [Google Scholar]
- Hagi, D.; DePorter, D.A.; Pilliar, R.M.; Arenovich, T. A targeted review of study outcomes with short (≤7 mm) endosseous dental implants placed in partially edentulous patients. J. Periodontol. 2004, 75, 798–804. [Google Scholar] [CrossRef]
- Griffin, T.J.; Cheung, W.S. The use of short, wide implants in posterior areas with reduced bone height: A retrospective investigation. J. Prosthet. Dent. 2004, 92, 139. [Google Scholar] [CrossRef]
- Gentile, M.A.; Chuang, S.-K.; Dodson, T.B. Survival estimates and risk factors for failure with 6 x 5.7-mm implants. Int. J. Oral Maxillofac. Implant. 2005, 20, 930–937. [Google Scholar]
- Albrektsson, T.; Jansson, T.; Lekholm, U. Osseointegrated dental implants. Dent. Clin. N. Am. 1986, 30, 151–174. [Google Scholar]
- Buser, D.; Weber, H.P.; Brägger, U.; Balsiger, C. Tissue integration of one-stage implants: Three-year results of a prospective longitudinal study with hollow cylinder and hollow screw implants. Quint. Int. 1994, 25, 679–686. [Google Scholar]
- Feng, S.-W.; Lin, C.-T.; Chang, W.-J.; Lee, S.-Y.; Cheng, C.-H.; Huang, H.-M. Influence of simulated bone quality and cortical bone thickness on implant stability detection using resonance frequency and damping factor analysis. Int. J. Oral Maxillofac. Implant. 2014, 29, 105–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bischof, M.; Nedir, R.; Szmukler-Moncler, S.; Bernard, J.-P.; Samson, J. Implant stability measurement of delayed and immediately loaded implants during healing. A clinical resonance-frequency analysis study with sandblasted-and-etched ITI implants. Clin. Oral Implant. Res. 2004, 15, 529–539. [Google Scholar] [CrossRef] [PubMed]
- Nedir, R.; Bischof, M.; Szmukler-Moncler, S.; Bernard, J.-P.; Samson, J. Predicting osseointegration by means of implant primary stability. A resonance-frequency analysis study with delayed and immediately loaded ITI SLA implants. Clin. Oral Implant. Res. 2004, 15, 520–528. [Google Scholar] [CrossRef]
- Schincaglia, G.P.; Marzola, R.; Scapoli, C.; Scotti, R. Immediate loading of dental implants supporting fixed partial dentures in the posterior mandible: A randomized controlled split-mouth study—Machined versus titanium oxide implant surface. Int. J. Oral Maxillofac. Implant. 2007, 22, 35–46. [Google Scholar]
- Zix, J.; Kessler-Liechti, G.; Mericske-Stern, R. Stability measurements of 1-stage implants in the maxilla by means of resonance frequency analysis: A pilot study. Int. J. Oral Maxillofac. Implant. 2005, 20, 747–752. [Google Scholar]
- Ostman, P.-O.; Hellman, M.; Wendelhag, I.; Sennerby, L. Resonance frequency analysis measurements of implants at placement surgery. Int. J. Prosthodont. 2006, 19. Available online: https://pubmed.ncbi.nlm.nih.gov/16479765/ (accessed on 4 May 2021).
- Huwiler, M.A.; Pjetursson, B.E.; Bosshardt, D.D.; Salvi, G.E.; Lang, N.P. Resonance frequency analysis in relation to jawbone characteristics and during early healing of implant installation. Clin. Oral Implant. Res. 2007, 18, 275–280. [Google Scholar] [CrossRef]
- Albrektsson, T.; Buser, D.; Sennerby, L. Crestal bone loss and oral implants. Clin. Implant. Dent. Relat. Res. 2012, 14, 783–791. [Google Scholar] [CrossRef] [PubMed]
- Nunes, M.; Almeida, R.F.; Felino, A.C.; Malo, P.; de Araújo Nobre, M. The influence of crown-to-implant ratio on short implant marginal bone loss. Int. J. Oral Maxillofac. Implant. 2016, 31, 1156–1163. [Google Scholar] [CrossRef] [PubMed]
- Benlidayi, M.E.; Ucar, Y.; Tatli, U.; Ekren, O.; Evlice, B.; Kisa, H.I.; Baksi, U. Short implants versus standard implants: Midterm outcomes of a clinical study. Implant. Dent. 2018, 27, 95–100. [Google Scholar] [CrossRef] [PubMed]
- Zadeh, H.H.; Guljé, F.; Palmer, P.J.; Abrahamsson, I.; Chen, S.; Mahallati, R.; Stanford, C.M. Marginal bone level and survival of short and standard-length implants after 3 years: An open multi-center randomized controlled clinical trial. Clin. Oral Implant. Res. 2018, 29, 894–906. [Google Scholar] [CrossRef]
- Wang, T.-M.; Leu, L.-J.; Wang, J.; Lin, L.-D. Effects of prosthesis materials and prosthesis splinting on peri-implant bone stress around implants in poor-quality bone: A numeric analysis. Int. J. Oral Maxillofac. Implant. 2002, 17, 231–237. [Google Scholar]
- Blanes, R.J. To what extent does the crown-implant ratio affect the survival and complications of implant-supported reconstructions? A systematic review. Clin. Oral Implant. Res. 2009, 20, 67–72. [Google Scholar] [CrossRef]
- Monje, A.; Suarez, F.; Galindo-Moreno, P.; García-Nogales, A.; Fu, J.-H.; Wang, H.-L. A systematic review on marginal bone loss around short dental implants (<10 mm) for implant-supported fixed prostheses. Clin. Oral. Impl. Res. 2014, 25, 1119–1124. [Google Scholar] [CrossRef] [Green Version]
- Chrcanovic, B.R.; Albrektsson, T.; Wennerberg, A. Platform switch and dental implants: A meta-analysis. J. Dent. 2015, 43, 629–646. [Google Scholar] [CrossRef]
- Bergkvist, G.; Koh, K.-J.; Sahlholm, S.; Klintström, E.; Lindh, C. Bone density at implant sites and its relationship to assessment of bone quality and treatment outcome. Int. J. Oral Maxillofac. Implant. 2010, 25, 321–328. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Short Implants Group (n = 33 pt and n = 47 ix) | Standard Implants Group (n = 41 pt and n = 52 ix) | p-Value |
|---|---|---|---|
| Patients (n = 74) | |||
| Age: mean ± SD | 51.76 ± 9.46 | 44.68 ± 10.94 | 0.008 (t-test) |
| Gender: n (%) | 0.776 (χ2) | ||
| Male | 15 (45.46) | 20 (48.79) | |
| Female | 18 (54.54) | 21 (51.21) | |
| Implants (n = 99) | |||
| Maxilla/Mandible: n (%) | 0.849 (χ2) | ||
| Maxilla | 28 (59.57) | 33 (63.46) | |
| Mandible | 19 (40.43) | 19 (36.54) | |
| Anterior/Posterior: n (%) | <0.001 (χ2) | ||
| Anterior | 3 (6.39) | 24 (46.16) | |
| Posterior | 44 (93.61) | 28 (53.84) | |
| Diameter: n (%) | 0.001 (χ2) | ||
| 3.5 mm2 | 0 (0.00) | 13 (25.00) | |
| 4.0 mm2 | 19 (40.42) | 24 (46.16) | |
| 4.5 mm2 | 13 (22.67) | 6 (11.53) | |
| 5.0 mm2 | 15 (31.91) | 9 (17.31) | |
| Type of restoration: n (%) | 0.036 (χ2) | ||
| Single crowns | 19 (40.42) | 32 (61.53) | |
| Fixed partial prosthesis | 28 (59.58) | 20 (38.47) |
| Time of Follow-Up | Short Implants (n = 47) Mean ± SD | Standard Implants (n = 52) Mean ± SD | p-Value |
|---|---|---|---|
| Δ ISQ2-ISQ1 | −0.745 ± 2.192 | −0.057 ± 2.796 | =0.316 (MW) |
| Δ ISQ3-ISQ2 | 0.298 ± 1.876 | 0.654 ± 1.781 | =0.336 (MW) |
| p-value | =0.014 (Friedman + Tukey) | =0.043 (Friedman + Tukey) |
| Time of Follow-Up | Short Implants (n = 47) Mean ± SD | Standard Implants (n = 52) Mean ± SD | p-Value |
|---|---|---|---|
| Δ MBL2-MBL1 | −0.263 ± 0.244 | −0.305 ± 0.272 | =0.324 (MW) |
| Δ MBL3-MBL2 | −0.184 ± 0.191 | −0.412 ± 0.588 | =0.004 (MW) |
| p-value | =0.009 (Friedman + Tukey) | =0.889 (Friedman + Tukey) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pardo-Zamora, G.; Ortiz-Ruíz, A.J.; Camacho-Alonso, F.; Martínez-Marco, J.F.; Molina-González, J.M.; Piqué-Clusella, N.; Vicente-Hernández, A. Short Dental Implants (≤8.5 mm) versus Standard Dental Implants (≥10 mm): A One-Year Post-Loading Prospective Observational Study. Int. J. Environ. Res. Public Health 2021, 18, 5683. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115683
Pardo-Zamora G, Ortiz-Ruíz AJ, Camacho-Alonso F, Martínez-Marco JF, Molina-González JM, Piqué-Clusella N, Vicente-Hernández A. Short Dental Implants (≤8.5 mm) versus Standard Dental Implants (≥10 mm): A One-Year Post-Loading Prospective Observational Study. International Journal of Environmental Research and Public Health. 2021; 18(11):5683. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115683
Chicago/Turabian StylePardo-Zamora, Guillermo, Antonio José Ortiz-Ruíz, Fabio Camacho-Alonso, José Francisco Martínez-Marco, Juan Manuel Molina-González, Núria Piqué-Clusella, and Ascensión Vicente-Hernández. 2021. "Short Dental Implants (≤8.5 mm) versus Standard Dental Implants (≥10 mm): A One-Year Post-Loading Prospective Observational Study" International Journal of Environmental Research and Public Health 18, no. 11: 5683. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115683