
Mobile Phone Use and Cognitive Impairment among Elderly Chinese: A National Cross-Sectional Survey Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Sampling Method
2.3. Data Collection
2.4. Sociodemographic Characteristics, Lifestyle and Health-Related Variables
2.5. Mobile Phone Use
2.6. Cognitive Impairment
2.7. Statistical Analysis
3. Results
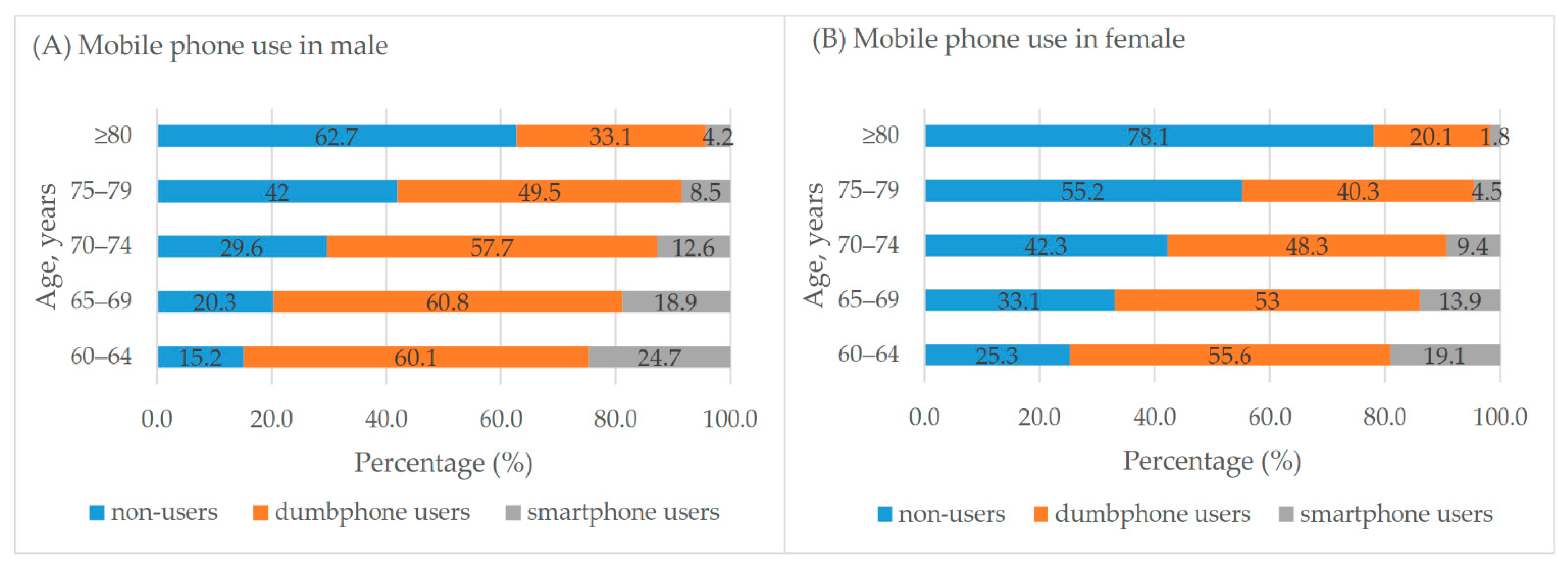
3.1. Mobile Phone Use
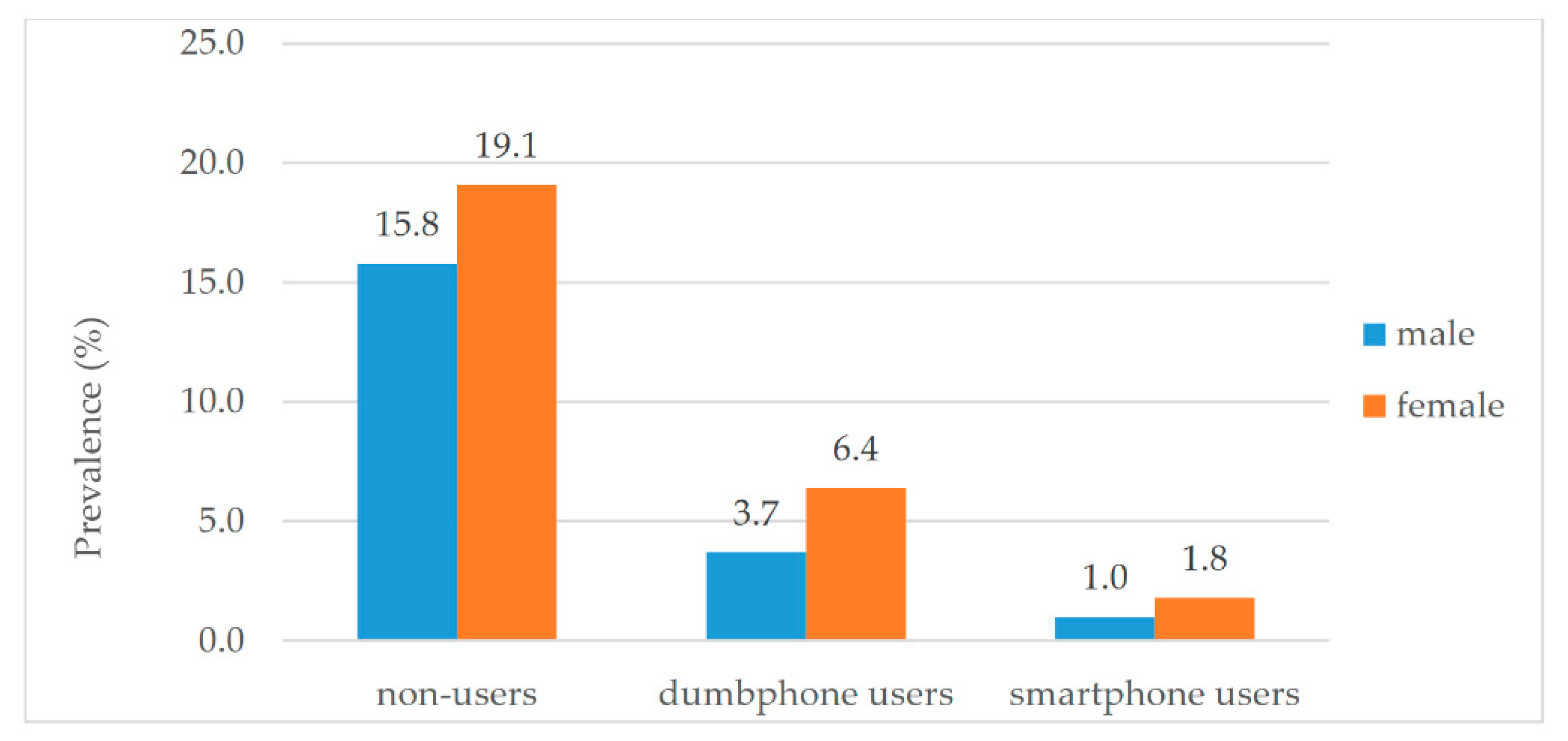
3.2. Mobile Phone Use and Cognitive Impairment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Ageing—Demographics: Percentage of Total Population Aged 60 Years or Over. Available online: https://www.who.int/data/maternal-newborn-child-adolescent-ageing/indicator-explorer-new/mca/percentage-of-total-population-aged-60-years-or-over (accessed on 10 April 2021).
- Gauthier, S.; Reisberg, B.; Zaudig, M.; Petersen, R.C.; Ritchie, K.; Broich, K.; Belleville, S.; Brodaty, H.; Bennett, D.; Chertkow, H.; et al. Mild cognitive impairment. Lancet 2006, 367, 1262–1270. [Google Scholar] [CrossRef]
- Xue, J.; Li, J.R.; Liang, J.M.; Chen, S.L. The prevalence of mild cognitive impairment in china: A systematic review. Aging Dis. 2018, 9, 706–715. [Google Scholar] [CrossRef] [Green Version]
- Jia, L.; Du, Y.; Chu, L.; Zhang, Z.; Li, F.; Lyu, D.; Li, Y.; Li, Y.; Zhu, M.; Jiao, H.; et al. Prevalence, risk factors, and management of dementia and mild cognitive impairment in adults aged 60 years or older in china: A cross-sectional study. Lancet Public Health 2020, 5, e661–e671. [Google Scholar] [CrossRef]
- Mitchell, A.J.; Shiri-Feshki, M. Rate of progression of mild cognitive impairment to dementia—Meta-analysis of 41 robust inception cohort studies. Acta Psychiatr. Scand. 2009, 119, 252–265. [Google Scholar] [CrossRef]
- Petersen, R.C.; Roberts, R.O.; Knopman, D.S.; Boeve, B.F.; Geda, Y.E.; Ivnik, R.J.; Smith, G.E.; Jack, C.R. Mild cognitive impairment ten years later. Arch. Neurol. 2009, 66, 1447–1455. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Q.; Wu, Y.; Han, T.; Liu, E. Changes in cognitive function and risk factors for cognitive impairment of the elderly in china: 2005–2014. Int. J. Environ. Res. Public Health 2019, 16, 2847. [Google Scholar] [CrossRef] [Green Version]
- Livingston, G.; Huntley, J.; Sommerlad, A.; Ames, D.; Ballard, C.; Banerjee, S.; Brayne, C.; Burns, A.; Cohen-Mansfield, J.; Cooper, C.; et al. Dementia prevention, intervention, and care: 2020 report of the lancet commission. Lancet 2020, 396, 413–446. [Google Scholar] [CrossRef]
- China Internet Network Information Center. The 43rd Statistical Report on Internet Development in China. Available online: http://www.cac.gov.cn/2019-02/28/c_1124175677.htm (accessed on 20 April 2021).
- Yuan, M.Q.; Chen, J.; Zhou, Z.; Yin, J.H.; Wu, J.L.; Luo, M.L.; Wang, L.X.; Fang, Y. Joint associations of smartphone use and gender on multidimensional cognitive health among community-dwelling older adults: A cross-sectional study. BMC Geriatr. 2019, 19, 140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, L.; Jing, X.C.; Lv, S.J.; Liang, J.H.; Tian, L.; Li, H.L.; Puts, M.; Xu, Y. Mobile device use and the cognitive function and depressive symptoms of older adults living in residential care homes. BMC Geriatr. 2020, 20, 41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sugita, A.; Ling, L.; Tsuji, T.; Kondo, K.; Kawachi, I. Cultural engagement and incidence of cognitive impairment: A six-year longitudinal follow-up of the japan gerontological evaluation study (jages). J. Epidemiol. 2020, JE20190337. [Google Scholar] [CrossRef] [PubMed]
- Damant, J.; Knapp, M.; Freddolino, P.; Lombard, D. Effects of digital engagement on the quality of life of older people. Health Soc. Care Community 2017, 25, 1679–1703. [Google Scholar] [CrossRef] [Green Version]
- Liao, S.; Zhou, Y.; Liu, Y.; Wang, R. Variety, frequency, and type of internet use and its association with risk of depression in middle- and older-aged Chinese: A cross-sectional study. J. Affect. Disord. 2020, 273, 280–290. [Google Scholar] [CrossRef] [PubMed]
- Brown, E.L.; Ruggiano, N.; Li, J.J.; Clarke, P.J.; Kay, E.S.; Hristidis, V. Smartphone-based health technologies for dementia care: Opportunities, challenges, and current practices. J. Appl. Gerontol. 2019, 38, 73–91. [Google Scholar] [CrossRef]
- Guo, Y.; Yang, F.; Hu, F.; Li, W.; Ruggiano, N.; Lee, H.Y. Existing mobile phone apps for self-care management of people with alzheimer disease and related dementias: Systematic analysis. JMIR Aging 2020, 3, e15290. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neal, D.; van den Berg, F.; Planting, C.; Ettema, T.; Dijkstra, K.; Finnema, E.; Droes, R.M. Can use of digital technologies by people with dementia improve self-management and social participation? A systematic review of effect studies. J. Clin. Med. 2021, 10, 604. [Google Scholar] [CrossRef]
- Qi, S.; Zhang, H.; Guo, H.; Wu, J.; Wang, Z. Undetected dementia in community-dwelling older people—6 provincial-level administrative divisions, China, 2015–2016. China CDC Wkly. 2020, 2, 731–735. [Google Scholar] [CrossRef]
- Zhou, B.F. Cooperative Meta-Analysis Group of the Working Group on Obesity in China. Predictive values of body mass index and waist circumference for risk factors of certain related diseases in Chinese adults--study on optimal cut-off points of body mass index and waist circumference in chinese adults. Biomed. Environ. Sci. 2002, 15, 83–96. [Google Scholar] [PubMed]
- Li, T.; Wang, H.; Yang, Y.; Galvin, J.E.; Morris, J.C.; Yu, X. The reliability and validity of Chinese version of ad8. Zhonghua Nei Ke Za Zhi 2012, 51, 777–780. [Google Scholar]
- Chen, H.H.; Sun, F.J.; Yeh, T.L.; Liu, H.E.; Huang, H.L.; Kuo, B.I.T.; Huang, H.Y. The diagnostic accuracy of the ascertain dementia 8 questionnaire for detecting cognitive impairment in primary care in the community, clinics and hospitals: A systematic review and meta-analysis. Fam. Pract. 2018, 35, 239–246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, M.Y.; Katzman, R.; Salmon, D.; Jin, H.; Cai, G.J.; Wang, Z.Y.; Qu, G.Y.; Grant, I.; Yu, E.; Levy, P.; et al. The prevalence of dementia and alzheimer’s disease in shanghai, china: Impact of age, gender, and education. Ann. Neurol. 1990, 27, 428–437. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. Mini-mental state. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Dormann, C.F.; Elith, J.; Bacher, S.; Buchmann, C.; Carl, G.; Carre, G.; Marquez, J.R.G.; Gruber, B.; Lafourcade, B.; Leitao, P.J.; et al. Collinearity: A review of methods to deal with it and a simulation study evaluating their performance. Ecography 2013, 36, 27–46. [Google Scholar] [CrossRef]
- Baumgart, M.; Snyder, H.M.; Carrillo, M.C.; Fazio, S.; Kim, H.; Johns, H. Summary of the evidence on modifiable risk factors for cognitive decline and dementia: A population-based perspective. Alzheimers Dement. 2015, 11, 718–726. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brandt, A.; Jensen, M.P.; Soberg, M.S.; Andersen, S.D.; Sund, T. Information and communication technology-based assistive technology to compensate for impaired cognition in everyday life: A systematic review. Disabil. Rehabil. Assist. Technol. 2020, 15, 810–824. [Google Scholar] [CrossRef] [PubMed]
- Kurniawan, S. Older people and mobile phones: A multi-method investigation. Int. J. Hum. Comput. Stud. 2008, 66, 889–901. [Google Scholar] [CrossRef]
- Hedman, A.; Nygard, L.; Almkvist, O.; Kottorp, A. Amount and type of everyday technology use over time in older adults with cognitive impairment. Scand. J. Occup. Ther. 2015, 22, 196–206. [Google Scholar] [CrossRef]
- World Health Organization. Electromagnetic Fields and Public Health: Mobile Phones. Available online: https://www.who.int/news-room/fact-sheets/detail/electromagnetic-fields-and-public-health-mobile-phones (accessed on 10 May 2021).
- Barth, A.; Ponocny, I.; Gnambs, T.; Winker, R. No effects of short-term exposure to mobile phone electromagnetic fields on human cognitive performance: A meta-analysis. Bioelectromagnetics 2012, 33, 159–165. [Google Scholar] [CrossRef]
- Ng, T.P.; Lim, M.L.; Niti, M.; Collinson, S. Long-term digital mobile phone use and cognitive decline in the elderly. Bioelectromagnetics 2012, 33, 176–185. [Google Scholar] [CrossRef]
- Fan, J.; Tao, W.; Li, X.; Li, H.; Zhang, J.; Wei, D.; Chen, Y.; Zhang, Z. The contribution of genetic factors to cognitive impairment and dementia: Apolipoprotein e gene, gene interactions, and polygenic risk. Int. J. Mol. Sci. 2019, 20, 1177. [Google Scholar] [CrossRef] [Green Version]
- Winblad, B.; Palmer, K.; Kivipelto, M.; Jelic, V.; Fratiglioni, L.; Wahlund, L.O.; Nordberg, A.; Backman, L.; Albert, M.; Almkvist, O.; et al. Mild cognitive impairment--beyond controversies, towards a consensus: Report of the international working group on mild cognitive impairment. J. Intern. Med. 2004, 256, 240–246. [Google Scholar] [CrossRef]
- Etgen, T.; Sander, D.; Bickel, H.; Sander, K.; Forstl, H. Vitamin d deficiency, cognitive impairment and dementia: A systematic review and meta-analysis. Dement. Geriatr. Cogn. Disord. 2012, 33, 297–305. [Google Scholar] [CrossRef] [PubMed]
- Moore, E.M.; Ames, D.; Mander, A.G.; Carne, R.P.; Brodaty, H.; Woodward, M.C.; Boundy, K.; Ellis, K.A.; Bush, A.I.; Faux, N.G. Among vitamin b12 deficient older people, high folate levels are associated with worse cognitive function: Combined data from three cohorts. J. Alzheimers Dis. 2014, 39, 661–668. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | n (%) 1 | Mobile Phone Use | |||
|---|---|---|---|---|---|
| None n (%) 1 | Dumbphone n (%) 1 | Smartphone n (%) 1 | p Values | ||
| Sex | |||||
| Male | 10,651 (49.0) | 2919 (27.4) | 5936 (55.7) | 1796 (16.9) | <0.001 |
| Female | 11,081 (51.0) | 4591 (41.4) | 5182 (46.8) | 1309 (11.8) | |
| Age groups, years | |||||
| 60–64 | 7179 (33.0) | 1449 (20.2) | 4155 (57.9) | 1575 (21.9) | <0.001 |
| 65–69 | 5031 (23.2) | 1340 (26.6) | 2864 (56.9) | 828 (16.5) | |
| 70–74 | 4035 (18.6) | 1452 (36.0) | 2139 (53.0) | 445 (11.0) | |
| 75–79 | 2919 (13.4) | 1429 (49.0) | 1304 (44.6) | 186 (6.4) | |
| ≥80 | 2568 (11.8) | 1840 (71.6) | 657 (25.6) | 72 (2.8) | |
| Living area | |||||
| Urban | 9580 (44.1) | 2617 (27.4) | 4669 (48.7) | 2294 (23.9) | <0.001 |
| Rural | 12,152 (55.9) | 4892 (40.3) | 6448 (53.0) | 811(6.7) | |
| Marital status | |||||
| Widowed | 4780 (22.0) | 2307 (48.2) | 2154 (45.1) | 320 (6.7) | <0.001 |
| Non-widowed | 16,952 (78.0) | 5202 (30.7) | 8964 (52.9) | 2785 (16.4) | |
| Education, years | |||||
| 0 | 8808 (40.5) | 4481 (50.8) | 4005 (45.5) | 322 (3.7) | <0.001 |
| 1–6 | 6898 (31.8) | 1971 (28.6) | 4118 (59.7) | 809 (11.7) | |
| ≥7 | 6026 (27.7) | 1057 (17.6) | 2994 (49.6) | 1974 (32.8) | |
| Occupation | |||||
| Non-manual 2 | 3425 (15.8) | 676 (19.7) | 1662 (48.5) | 1087 (31.8) | <0.001 |
| Worker | 4439 (20.4) | 1057 (23.8) | 2280 (51.4) | 1102 (24.8) | |
| Farmer | 13,868 (63.8) | 5777 (41.7) | 7176 (51.7) | 916 (6.6) | |
| Residing status | |||||
| Living alone | 2465 (11.3) | 1021 (41.4) | 1248 (50.7) | 196 (7.9) | <0.001 |
| Living with family | 19,267 (88.7) | 6489 (33.7) | 9870 (51.2) | 2909 (15.1) | |
| Total | 21,732 (100.0) | 7510 (34.5) | 11,118 (51.2) | 3105 (14.3) | |
| Models | Variables | Reference Groups | OR/AOR (95% CI) |
|---|---|---|---|
| Crude | Dumbphone users | No mobile phone use | 0.24 (0.22, 0.27) *** |
| Smartphone users | 0.06 (0.04, 0.10) *** | ||
| Adjusted for demographics | Dumbphone users | No mobile phone use | 0.37 (0.33, 0.42) *** |
| Smartphone users | 0.14 (0.10, 0.22) *** | ||
| Full model | Dumbphone users | No mobile phone use | 0.39 (0.35, 0.45) *** |
| Smartphone users | 0.16 (0.11, 0.25) *** | ||
| Sex (female) | Sex (male) | 1.24 (1.05, 1.46) * | |
| Aged 65–69 years | Aged 60–64 years | 1.11 (0.92, 1.35) | |
| Aged 70–74 years | 1.37 (1.13, 1.67) ** | ||
| Aged 75–79 years | 2.00 (1.63, 2.43) *** | ||
| Aged ≥ 80 years | 3.43 (2.80, 4.20) *** | ||
| Living in rural area | Living in urban area | 1.03 (0.89, 1.19) | |
| Non-widowed | Widowed | 0.80 (0.69, 0.92) ** | |
| Education: 1–6 years | Education: 0 year | 0.77 (0.67, 0.89) *** | |
| Education: ≥7 years | 1.00 (0.79, 1.24) | ||
| Worker | Non-manual worker | 0.91 (0.70, 1.18) | |
| Farmer | 1.62 (1.24, 2.12) *** | ||
| Current smoker | Non-smoker | 0.98 (0.81, 1.19) | |
| Former smoker | 1.08 (0.87, 1.19) | ||
| Alcohol drinking | No alcohol drinking | 1.02 (0.88, 1.19) | |
| Regular tea drinking | No regular tea drinking | 0.91 (0.78, 1.06) * | |
| Regular exercise | No regular exercise | 0.83 (0.72, 0.95) ** | |
| Living with family | Living alone | 1.15 (0.96, 1.37) | |
| Socialize with neighbors occasionally | Almost never | 0.58 (0.44, 0.77) *** | |
| Socialize with neighbors daily | 0.51 (0.45, 0.59) *** | ||
| Read newspapers occasionally | Almost never | 0.70 (0.56, 0.88) ** | |
| Read newspapers daily | 0.62 (0.46, 0.84) *** | ||
| BMI < 18.5 | 18.5 ≤ BMI < 24.0 | 1.08 (0.91, 1.30) | |
| 24.0 ≤ BMI < 28.0 | 1.03 (0.90, 1.17) | ||
| BMI ≥ 28.0 | 1.07 (0.88, 1.31) | ||
| Hypertension | No hypertension | 1.04 (0.93, 1.17) | |
| CHD | No CHD | 0.99 (0.81, 1.20) | |
| Diabetes | No diabetes | 1.00 (0.87, 1.16) | |
| Stroke | No stroke | 2.56 (2.08, 3.14) *** | |
| Hearing loss | No hearing loss | 1.61 (1.28, 2.01) *** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Qi, S.; Sun, Y.; Yin, P.; Zhang, H.; Wang, Z. Mobile Phone Use and Cognitive Impairment among Elderly Chinese: A National Cross-Sectional Survey Study. Int. J. Environ. Res. Public Health 2021, 18, 5695. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115695
Qi S, Sun Y, Yin P, Zhang H, Wang Z. Mobile Phone Use and Cognitive Impairment among Elderly Chinese: A National Cross-Sectional Survey Study. International Journal of Environmental Research and Public Health. 2021; 18(11):5695. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115695
Chicago/Turabian StyleQi, Shige, Yuying Sun, Peng Yin, Han Zhang, and Zhihui Wang. 2021. "Mobile Phone Use and Cognitive Impairment among Elderly Chinese: A National Cross-Sectional Survey Study" International Journal of Environmental Research and Public Health 18, no. 11: 5695. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115695