
Anticoagulation Control with Acenocoumarol or Warfarin in Non-Valvular Atrial Fibrillation in Primary Care (Fantas-TIC Study)

 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
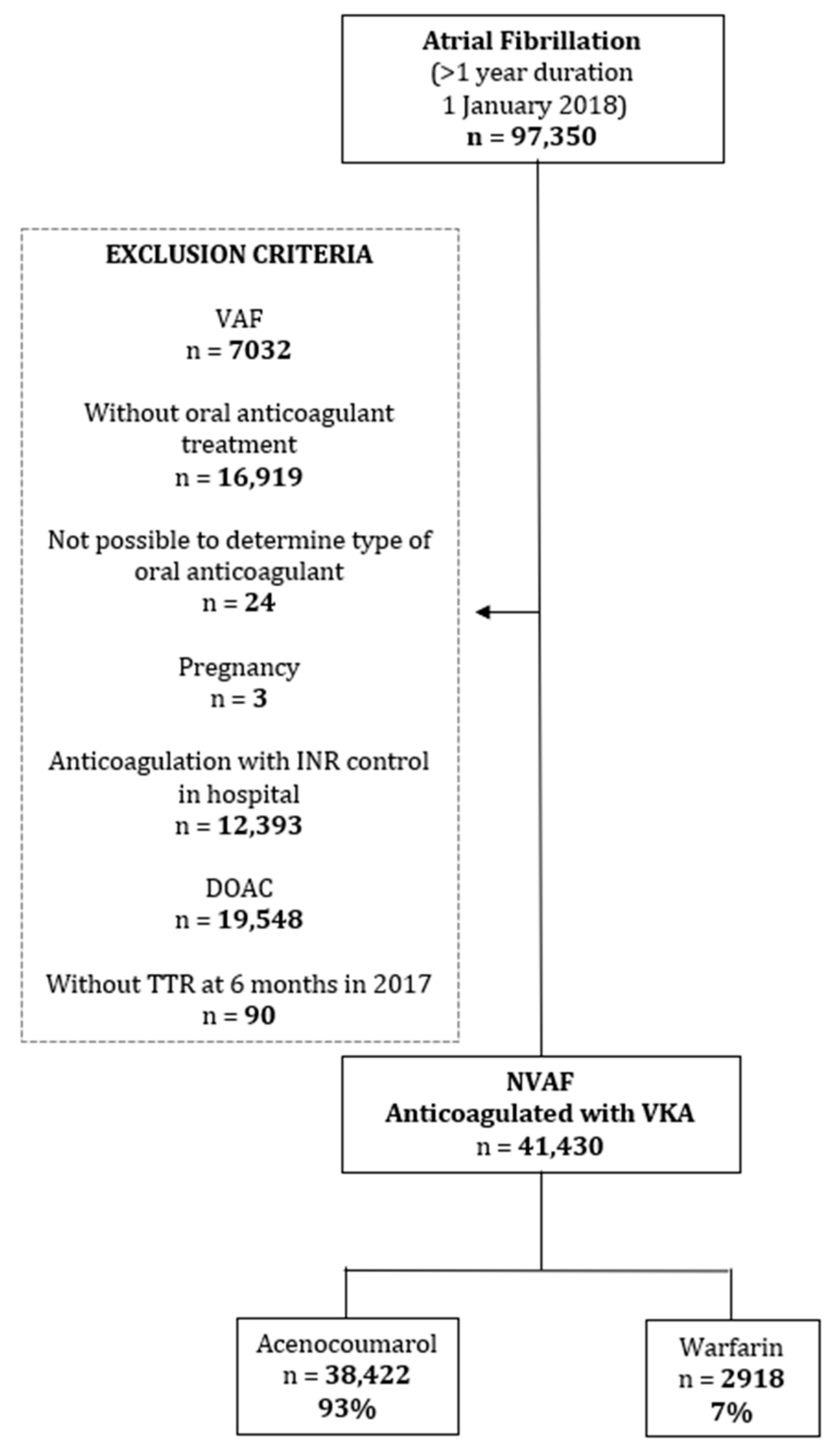
2.1. Design and Study Population
2.2. Inclusion and Exclusion Criteria
2.3. Study Variables
2.4. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Programa d’harmonització farmacoterapèutica, 2018. Pautes per a l’harmonització de l’ús d’anticoagulants orals per a la prevenció de l’ictus i l’embòlia sistèmica en pacients amb fibril·lació auricular. Servei Català de la Salut. Departament de Salut. Generalitat de Catalunya, 2018; pp. 1–76. Available online: https://catsalut.gencat.cat/web/.content/minisite/catsalut/proveidors_professionals/medicaments_farmacia/harmonitzacio/pautes/anticoagulants-orals-fibrilacio-auricular/pautes-harmonitzacio-anticoagulants-orals-en-fibrilacio-auricular.pdf (accessed on 14 December 2020).
- Kirchhof, P.; Benussi, S.; Kotecha, D.; Ahlsson, A.; Atar, D.; Casadei, B.; Castellá, M.; Diener, H.; Heidbuchel, H.; Hendriks, J.; et al. Guía ESC 2016 sobre el diagnóstico y tratamiento de la fibrilación auricular, desarrollada en colaboración con la EACTS. Rev. Esp. Cardiol. 2017, 70, e1–e84. [Google Scholar] [CrossRef] [Green Version]
- Coleman, C.I.; Briere, J.-B.; Fauchier, L.; Levy, P.; Bowrin, K.; Toumi, M.; Millier, A.; Taieb, V.; Wu, O. Meta-analysis of real-world evidence comparing non-vitamin K antagonist oral anticoagulants with vitamin K antagonists for the treatment of patients with non-valvular atrial fibrillation. J. Mark. Access Health Policy 2019, 7, 1574541. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2021, 42, 373–498. [Google Scholar] [CrossRef]
- Steffel, J.; Verhamme, P.; Potpara, T.S.; Albaladejo, P.; Antz, M.; Desteghe, L.; Haeusler, K.G.; Oldgren, J.; Reinecke, H.; Roldan-Schilling, V.; et al. The 2018 European Heart Rhythm Association Practical Guide on the use of non-Vitamin K antagonist oral anticoagulants in patients with atrial fibrillation. Eur. Heart J. 2018, 39, 1330–1393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- January, C.T.; Wann, L.S.; Calkins, H.; Chen, L.Y.; Cigarroa, J.E.; Cleveland, J.C.; Ellinor, P.T.; Ezekowitz, M.D.; Field, M.E.; Furie, K.L.; et al. 2019 AHA/ACC/HRS Focused Update of the 2014 AHA/ACC/HRS Guideline for the Management of Patients With Atrial Fibrillation: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart R. Circulation 2019, 140, e125–e151. [Google Scholar] [CrossRef]
- Ministerio de Sanidad. Servicios Sociales e Igualdad. Agencia Española de Medicamentos y Productos Sanitarios. Informe de Posicionamiento Terapéutico UT-ACOD/V5/211120162016 Criterios y recomendaciones generales para el uso de nuevos anticoagulantes orales (NACO) en la prevención del ictus y la embolia sistémica en pacientes con fibrilación auricular no valvular. Available online: https://www.aemps.gob.es/medicamentosUsoHumano/informesPublicos/docs/criterios-anticoagulantes-orales.pdf (accessed on 16 December 2020).
- Lin, P.J. Reviewing the reality: Why we need to change. Eur. Hear. J. Suppl. 2005, 7, 15–20. [Google Scholar] [CrossRef] [Green Version]
- Thijssen, H.H.W.; Drittij, M.J.; Vervoort, L.M.T.; De Vries-Hanje, J.C. Altered pharmacokinetics of R- and S-acenocoumarol in a subject heterozygous for CYP2C9*3. Clin. Pharmacol. Ther. 2001, 70, 292–298. [Google Scholar] [CrossRef] [PubMed]
- Kelly, J.G.; O’Malley, K. Clinical Pharmacokinetics of Oral Anticoagulants. Clin. Pharmacokinet. 1979, 4, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Ufer, M. Comparative pharmacokinetics of vitamin K antagonists warfarin, phenprocoumon and acenocoumarol. Clin. Pharmacokinet. 2005, 44, 1227–1246. [Google Scholar] [CrossRef]
- Barón Esquivias, G.; Escolar Albaladejo, G.; Zamorano, J.L.; Betegón Nicolás, L.; Canal Fontcuberta, C.; de Salas-Cansado, M.; Rubio-Rodríguez, D.; Rubio-Terrés, C. Cost-effectiveness Analysis Comparing Apixaban and Acenocoumarol in the Prevention of Stroke in Patients With Nonvalvular Atrial Fibrillation in Spain. Rev. Española Cardiol. (English Ed.) 2015, 68, 680–690. [Google Scholar] [CrossRef]
- González-Juanatey, J.R.; Álvarez-Sabin, J.; Lobos, J.M.; Martínez-Rubio, A.; Reverter, J.C.; Oyagüez, I.; González-Rojas, N.; Becerra, V. Cost-effectiveness of Dabigatran for Stroke Prevention in Non-valvular Atrial Fibrillation in Spain. Rev. Española Cardiol. (English Ed.) 2012, 65, 901–910. [Google Scholar] [CrossRef] [PubMed]
- Lekuona, I.; Anguita, M.; Zamorano, J.L.; Rodríguez, J.M.; Barja de Soroa, P.; Pérez-Alcántara, F. Would the Use of Edoxaban Be Cost-effective for the Prevention of Stroke and Systemic Embolism in Patients With Nonvalvular Atrial Fibrillation in Spain? Rev. Española Cardiol. (English Ed.) 2019, 72, 398–406. [Google Scholar] [CrossRef]
- FICHA TECNICA SINTROM 1 mg COMPRIMIDOS. Available online: https://cima.aemps.es/cima/dochtml/ft/58994/FichaTecnica_58994.html#7-titular-de-la-autorizaci%20-n-de-commercialization%20and%20therefore%20had%20a%20broader%20experience%20of%20use%20prior%20to%20warfarin (accessed on 21 April 2021).
- Barrios, V.; Escobar, C.; Prieto, L.; Lobos, J.M.; Polo, J.; Vargas, D. Control of Anticoagulation with Warfarin or Acenocoumarol in Spain. Do They Differ? Rev. Esp. Cardiol. 2015, 68, 1181–1182. [Google Scholar] [CrossRef] [PubMed]
- Cancino, R.S.; Hylek, E.M.; Reisman, J.I.; Rose, A.J. Comparing patient-level and site-level anticoagulation control as predictors of adverse events. Thromb. Res. 2014, 133, 652–656. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, A.M.; Setakis, E.; Plumb, J.M.; Clemens, A.; van Staa, T.-P. Risks of stroke and mortality associated with suboptimal anticoagulation in atrial fibrillation patients. Thromb. Haemost. 2011, 106, 968–977. [Google Scholar] [CrossRef] [PubMed]
- Mearns, E.S.; White, C.M.; Kohn, C.G.; Hawthorne, J.; Song, J.S.; Meng, J.; Schein, J.R.; Raut, M.K.; Coleman, C.I. Quality of vitamin K antagonist control and outcomes in atrial fibrillation patients: A meta-analysis and meta-regression. Thromb. J. 2014, 12, 14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bolíbar, B.; Fina Avilés, F.; Morros, R.; Del Mar Garcia-Gil, M.; Hermosilla, E.; Ramos, R.; Rosell, M.; Rodríguez, J.; Medina, M.; Calero, S.; et al. Base de datos SIDIAP: La historia clínica informatizada de Atención Primaria como fuente de información para la investigación epidemiológica. Med. Clin. (Barc.) 2012, 138, 617–621. [Google Scholar] [CrossRef] [PubMed]
- Del Mar García-Gil, M.; Hermosilla, E.; Prieto-Alhambra, D.; Fina, F.; Rosell, M.; Ramos, R.; Rodriguez, J.; Williams, T.; Van Staa, T.; Bolíbar, B. Construction and validation of a scoring system for the selection of high-quality data in a Spanish population primary care database (SIDIAP). Inform. Prim. Care 2012, 19, 135–145. [Google Scholar] [CrossRef] [PubMed]
- WHOCC WHOCC—ATC/DDD Index. Available online: https://www.whocc.no/atc_ddd_index/ (accessed on 26 November 2020).
- World Health Organization (WHO); Classification of Diseases (ICD). Available online: https://www.who.int/classifications/classification-of-diseases (accessed on 26 November 2020).
- García-Sempere, A.; Hurtado, I.; Bejarano-Quisoboni, D.; Rodríguez-Bernal, C.; Santa-Ana, Y.; Peiró, S.; Sanfélix-Gimeno, G. Quality of INR control and switching to non-Vitamin K oral anticoagulants between women and men with atrial fibrillation treated with Vitamin K Antagonists in Spain. A population-based, real-world study. PLoS ONE 2019, 14, e0211681. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carmona-Torres, J.M.; Cobo-Cuenca, A.I.; Recio-Andrade, B.; Laredo-Aguilera, J.A.; Martins, M.M.; Rodríguez-Borrego, M.A. Prevalence and factors associated with polypharmacy in the older people: 2006–2014. J. Clin. Nurs. 2018, 27, 2942–2952. [Google Scholar] [CrossRef] [PubMed]
- Gschwind, L.; Rollason, V.; Lovis, C.; Boehlen, F.; Bonnabry, P.; Dayer, P.; Desmeules, J.A. Identification and weighting of the most critical “real-life” drug-drug interactions with acenocoumarol in a tertiary care hospital. Eur. J. Clin. Pharmacol. 2013, 69, 617–627. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teichert, M.; Eijgelsheim, M.; Rivadeneira, F.; Uitterlinden, A.G.; van Schaik, R.H.N.; Hofman, A.; De Smet, P.A.G.M.; van Gelder, T.; Visser, L.E.; Stricker, B.H.C. A genome-wide association study of acenocoumarol maintenance dosage. Hum. Mol. Genet. 2009, 18, 3758–3768. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Visser, L.E.; Van Vliet, M.; Van Schaik, R.H.N.; Kasbergen, A.A.H.; De Smet, P.A.G.M.; Vulto, A.G.; Hofman, A.; Van Duijn, C.M.; Stricker, B.H.C. The risk of overanticoagulation in patients with cytochrome P450 CYP2C9*2 or CYP2C9*3 alleles on acenocoumarol or phenprocoumon. Pharmacogenetics 2004, 14, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Barrios, V.; Escobar, C.; Prieto, L.; Osorio, G.; Polo, J.; Lobos, J.M.; Vargas, D.; García, N. Anticoagulation Control in Patients With Nonvalvular Atrial Fibrillation Attended at Primary Care Centers in Spain: The PAULA Study. Rev. Española Cardiol. (English Ed.) 2015, 68, 769–776. [Google Scholar] [CrossRef]
- Liang ADEF, H.-F.; Du, X.C.; Zhou, Y.-C.B.; Yang, X.-Y.B.; Xia BDF, S.-J.; Dong ADEF, J.-Z.; Lip, G.Y.; Ma, C.-S.; Squibb, M.; Ingelheim, B. Control of Anticoagulation Therapy in Patients with Atrial Fibrillation Treated with Warfarin: A Study from the Chinese Atrial Fibrillation Registry. Med. Sci. Monit. 2019, 25, 4691–4698. [Google Scholar] [CrossRef]
- Li, X.; Krumholz, H.M.; Yip, W.; Cheng, K.K.; De Maeseneer, J.; Meng, Q.; Mossialos, E.; Li, C.; Lu, J.; Su, M.; et al. Quality of primary health care in China: Challenges and recommendations. Lancet 2020, 395, 1802–1812. [Google Scholar] [CrossRef]
- Sánchez, M.A.; Martínez, V.B.; Fillat, Á.C. Quality of Vitamin K Antagonist Anticoagulation in Spain: Prevalence of Poor Control and Associated Factors on behalf of the CALIFA study researchers. Rev. Española Cardiol. (English Ed.) 2015. [Google Scholar] [CrossRef]
- Dharmarajan, L.; Dharmarajan, T.S. Prescribing warfarin appropriately to meet patient safety goals. Am. Health Drug Benefits 2008, 1, 26–32. [Google Scholar] [PubMed]
- Björck, F.; Kadhim, H.; Själander, A. Predictors for INR-control in a well-managed warfarin treatment setting. J. Thromb. Thrombolysis 2019, 47, 227–232. [Google Scholar] [CrossRef] [Green Version]
- García-Fernández, A.; Esteve-Pastor, M.A.; Roldán-Rabadán, I.; Muñiz, J.; Ruiz Ortiz, M.; Cequier, Á.; Bertomeu-Martínez, V.; Badimón, L.; Otero, D.; Anguita, M.; et al. Relationship of adverse events to quality of anticoagulation control in atrial fibrillation patients with diabetes: Real-world data from the FANTASIIA Registry. Ann. Med. 2020, 52, 300–309. [Google Scholar] [CrossRef]
- Dalmau Llorca, M.R.; Gonçalves, A.Q.; Forcadell Drago, E.; Fernández-Sáez, J.; Hernández Rojas, Z.; Pepió Vilaubí, J.M.; Rodríguez Cumplido, D.; Morral Parente, R.M.; Aguilar Martín, C. A new clinical decision support tool for improving the adequacy of anticoagulant therapy and reducing the incidence of stroke in nonvalvular atrial fibrillation. Medicine (United States) 2018, 97, e9578. [Google Scholar] [CrossRef] [PubMed]
- Rosa Dalmau Llorca, M.; Martín, C.A.; Carrasco-Querol, N.; Rojas, Z.H.; Drago, E.F.; Cumplido, D.R.; Vilaubí, J.M.P.; Blanco, E.C.; Gonçalves, A.Q.; Fernández-Sáez, J. Oral anticoagulant adequacy in non-valvular atrial fibrillation in primary care: A cross-sectional study using real-world data (fantas-tic study). Int. J. Environ. Res. Public Health 2021, 18, 2244. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Total | 41,340 |
|---|---|
| Sex | |
| Female | 20,241 (49.0) |
| Male | 21,099 (51.0) |
| Age in Years. mean (SD) | 78.4 (9.0) |
| Type of AVK | |
| Acenocoumarol | 38,422 (92.9) |
| Warfarin | 2918 (7.1) |
| Oral Anticoagulation Prescription in Primary Care | 33,185 (80.3) |
| Cardiovascular History | |
| Peripheral Arteriopathy | 2698 (6.5) |
| Ischaemic Heart Disease | 7494 (18.1) |
| Aortic Atheromatosis | 399 (1.0) |
| Ischaemic Stroke or Transient Ischaemic Attack | 6421 (15.5) |
| Intracranial Haemorrhage | 363 (0.9) |
| Morbidity | |
| Diabetes Mellitus | 13,552 (32.8) |
| Arterial Hypertension | 33,284 (80.5) |
| Heart Failure | 10,806 (26.1) |
| Renal Insufficiency | 12,303 (29.8) |
| Bleeding Risk History | |
| Alcohol | 1721 (4.2) |
| Intracranial Aneurysm | 27 (0.1) |
| Portal Hypertension | 80 (0.2) |
| Liver Failure | 263 (0.6) |
| Hereditary Telangiectasia | 2 (0.0) |
| Active Aortic Aneurysm and Dissection | 612 (1.5) |
| Intestinal Angiodysplasia | 92 (0.2) |
| Haemorrhages Other Than Gastrointestinal and Intracranial | 567 (1.4) |
| Gastrointestinal Bleeding | 3272 (7.9) |
| Scores | |
| CHA2DS2VASc | |
| 0 | 404 (1.0) |
| 1 | 2104 (5.1) |
| 2 | 7246 (17.5) |
| 3 | 14,656 (35.5) |
| ≥4 | 16,930 (41.0) |
| HAS-BLED | |
| 0 | 953 (2.3) |
| 1 | 14,548 (35.2) |
| 2 | 15,075 (36.5) |
| 3 | 7754 (18.8) |
| ≥4 | 3010 (7.3) |
| eGFR mL/min/1.73 m2 | 61.2 (18.9) |
| Patients Treated Outside Primary Care Centre | |
| Treated at Home | 4892 (11.8) |
| Treated in an Institution | 1636 (4.0) |
| Acenocoumarol | Warfarin | ||||||
|---|---|---|---|---|---|---|---|
| Total | TTR < 65% | % | Total | TTR < 65% | % | a p | |
| Total | 38,422 | 14,944 | 38.9 | 2918 | 1121 | 38.4 | 0.610 |
| Sex | |||||||
| Female | 18,808 | 7626 | 40.5 | 1433 | 587 | 41.0 | 0.757 |
| Male | 19,614 | 7318 | 37.3 | 1485 | 534 | 36.0 | 0.299 |
| Age (years) | |||||||
| <60 | 862 | 370 | 42.9 | 72 | 27 | 37.5 | 0.371 |
| 60–69 | 4281 | 1610 | 37.6 | 397 | 145 | 36.5 | 0.670 |
| 70–79 | 12,558 | 4691 | 37.4 | 1085 | 390 | 35.9 | 0.357 |
| ≥80 | 20,721 | 8273 | 39.9 | 1364 | 559 | 41.0 | 0.440 |
| Oral Anticoagulant Prescription in Primary Care | |||||||
| Yes | 30,938 | 11,964 | 38.7 | 2247 | 866 | 38.5 | 0.902 |
| No | 7484 | 2980 | 39.8 | 671 | 255 | 38.0 | 0.357 |
| Cardiovascular History | |||||||
| Peripheral Arteriopathy | 2492 | 1088 | 43.7 | 206 | 89 | 43.2 | 0.899 |
| No | 35,930 | 13,856 | 38.6 | 2712 | 1032 | 38.1 | 0.598 |
| Ischaemic Heart Disease | 6951 | 2855 | 41.1 | 543 | 222 | 40.9 | 0.931 |
| No | 31,471 | 12,089 | 38.4 | 2375 | 899 | 37.9 | 0.588 |
| Aortic Atheromatosis | 354 | 139 | 39.3 | 45 | 16 | 35.6 | 0.631 |
| No | 38,068 | 14,805 | 38.9 | 2873 | 1105 | 38.5 | 0.649 |
| Ischaemic Stroke or TIA | 5810 | 2351 | 40.5 | 611 | 252 | 41.2 | 0.709 |
| No | 32,612 | 12,593 | 38.6 | 2307 | 869 | 37.7 | 0.367 |
| Intracranial Haemorrhage | 334 | 156 | 46.7 | 29 | 16 | 55.2 | 0.381 |
| No | 38,088 | 14,788 | 38.8 | 2889 | 1105 | 38.2 | 0.539 |
| Morbidity | |||||||
| Diabetes mellitus | 12,549 | 5293 | 42.2 | 1003 | 406 | 40.5 | 0.294 |
| No | 25,873 | 9651 | 37.3 | 1915 | 715 | 37.3 | 0.975 |
| Arterial Hypertension | 30,947 | 12,047 | 38.9 | 2337 | 913 | 39.1 | 0.894 |
| No | 7475 | 2897 | 38.8 | 581 | 208 | 35.8 | 0.159 |
| Heart Failure | 9947 | 4320 | 43.4 | 859 | 363 | 42.3 | 0.506 |
| No | 28,475 | 10,624 | 37.3 | 2059 | 758 | 36.8 | 0.653 |
| Renal Insufficiency | 11,346 | 4752 | 41.9 | 957 | 417 | 43.6 | 0.309 |
| No | 27,076 | 10,192 | 37.6 | 1961 | 704 | 35.9 | 0.124 |
| Bleeding Risk History | |||||||
| Alcohol | 1564 | 711 | 45.5 | 157 | 71 | 45.2 | 0.955 |
| No | 36,858 | 14,233 | 38.6 | 2761 | 1050 | 38.0 | 0.542 |
| Intracranial Aneurysm | 26 | 12 | 46.2 | 1 | 1 | 100.0 | 0.290 |
| No | 38,396 | 14,932 | 38.9 | 2917 | 1120 | 38.4 | 0.598 |
| Portal Hypertension | 72 | 27 | 37.5 | 8 | 4 | 50.0 | 0.491 |
| No | 38,350 | 14,917 | 38.9 | 2910 | 1117 | 38.4 | 0.585 |
| Liver Failure | 242 | 116 | 47.9 | 21 | 11 | 52.4 | 0.696 |
| No | 38,180 | 14,828 | 38.8 | 2897 | 1110 | 38.3 | 0.579 |
| Hereditary Telangiectasia | 1 | 0 | 0.0 | 1 | 1 | 100.0 | 0.157 |
| No | 38,421 | 14,944 | 38.9 | 2917 | 1120 | 38.4 | 0.593 |
| Active Aortic Aneurysm and Dissection | 558 | 207 | 37.1 | 54 | 27 | 50.0 | 0.062 |
| No | 37,864 | 14,737 | 38.9 | 2864 | 1094 | 38.2 | 0.444 |
| Intestinal Angiodysplasia | 85 | 40 | 47.1 | 7 | 4 | 57.1 | 0.608 |
| No | 38,337 | 14,904 | 38.9 | 2911 | 1117 | 38.4 | 0.590 |
| Haemorrhages Other Than Gastrointestinal and Intracranial | 523 | 194 | 37.1 | 44 | 16 | 36.4 | 0.923 |
| No | 37,899 | 14,750 | 38.9 | 2874 | 1105 | 38.4 | 0.617 |
| Gastrointestinal Bleeding | 3028 | 1252 | 41.3 | 244 | 101 | 41.4 | 0.989 |
| No | 35,394 | 13,692 | 38.7 | 2674 | 1020 | 38.1 | 0.581 |
| Scores | |||||||
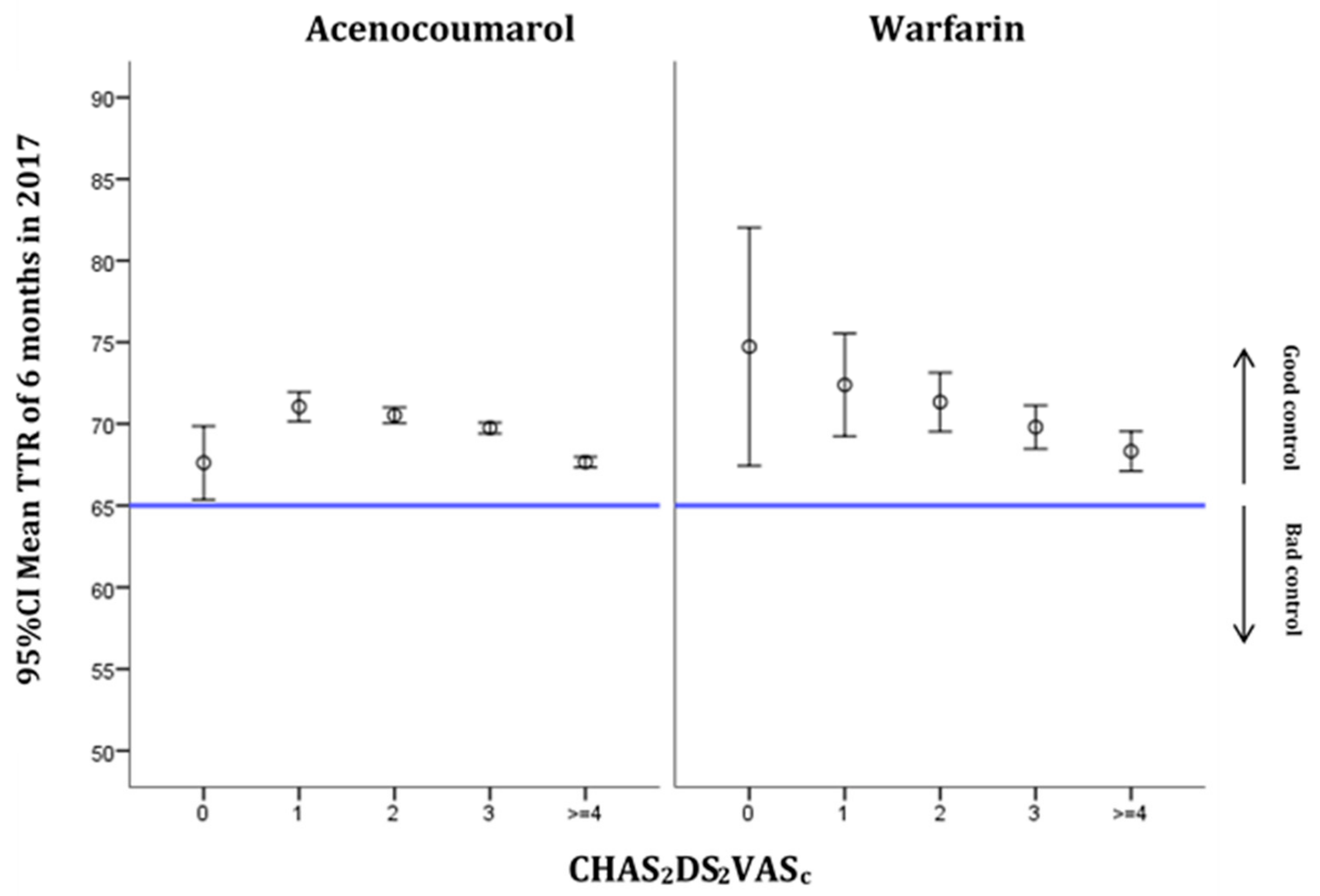
| CHA2DS2VASc | |||||||
| 0 | 366 | 137 | 37.4 | 38 | 13 | 34.2 | 0.696 |
| 1 | 1939 | 683 | 35.2 | 165 | 54 | 32.7 | 0.519 |
| 2 | 6722 | 2402 | 35.7 | 524 | 170 | 32.4 | 0.129 |
| 3 | 13,698 | 5148 | 37.6 | 958 | 382 | 39.9 | 0.157 |
| ≥4 | 15,697 | 6574 | 41.9 | 1233 | 502 | 40.7 | 0.424 |
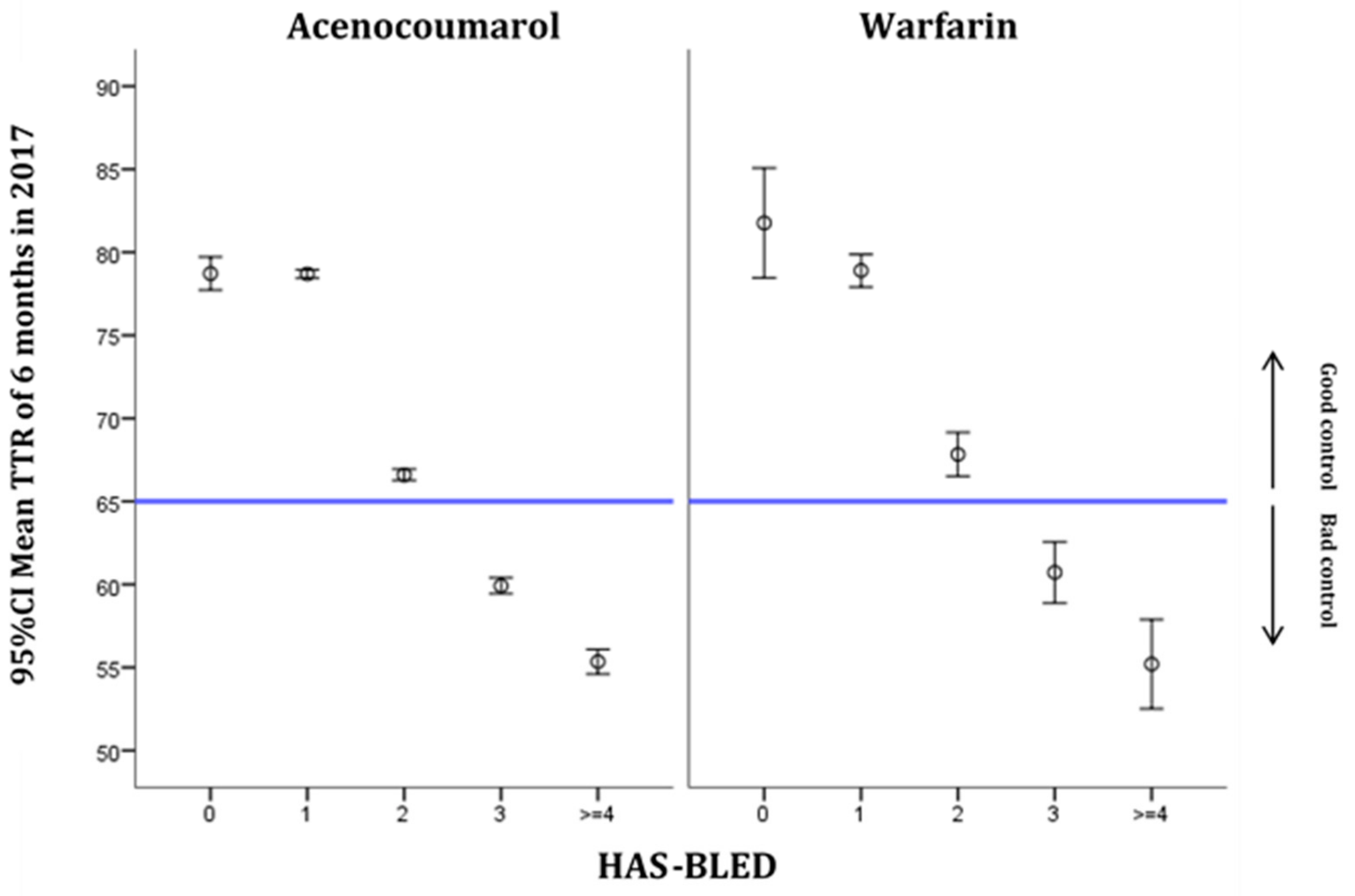
| HAS-BLED | |||||||
| 0 | 872 | 168 | 19.3 | 81 | 11 | 13.6 | 0.210 |
| 1 | 13,530 | 2387 | 17.6 | 1018 | 190 | 18.7 | 0.410 |
| 2 | 14,065 | 6285 | 44.7 | 1010 | 443 | 43.9 | 0.611 |
| 3 | 7180 | 4210 | 58.6 | 574 | 320 | 55.7 | 0.177 |
| ≥4 | 2775 | 1894 | 68.3 | 235 | 157 | 66.8 | 0.648 |
| eGFR mL/min/1.73 m2 | |||||||
| < 15 | 270 | 172 | 63.7 | 41 | 23 | 56.1 | 0.348 |
| 15–29 | 1678 | 825 | 49.2 | 164 | 84 | 51.2 | 0.616 |
| 30–49 | 7570 | 3292 | 43.5 | 639 | 274 | 42.9 | 0.766 |
| ≥ 50 | 25,887 | 9537 | 36.8 | 1926 | 679 | 35.3 | 0.164 |
| Lost | 3017 | 1118 | 37.1 | 148 | 61 | 41.2 | 0.307 |
| Patients Treated Outside Primary Care Centre | |||||||
| Treated at Home | 4504 | 2149 | 47.7 | 388 | 184 | 47.4 | 0.912 |
| No | 33,918 | 12,795 | 37.7 | 2530 | 937 | 37.0 | 0.491 |
| Treated in an Institution | 1546 | 756 | 48.9 | 90 | 48 | 53.3 | 0.414 |
| No | 36,876 | 14,188 | 38.5 | 2828 | 1073 | 37.9 | 0.575 |
| ORadj | 95% CI | p | |
|---|---|---|---|
| Type of anticoagulant | |||
| Acenocoumarol | 1 | ||
| Warfarin | 0.96 | 0.88–1.03 | 0.268 |
| Sex | |||
| Female | 1 | ||
| Male | 0.87 | 0.83–0.91 | <0.001 |
| Age (years) | |||
| <60 | 1 | ||
| 60–69 | 0.82 | 0.71–0.95 | 0.010 |
| 70–79 | 0.78 | 0.68–0.90 | <0.001 |
| ≥80 | 0.82 | 0.72–0.94 | 0.004 |
| Oral Anticoagulant Prescription in Primary Care | 0.95 | 0.90–1.00 | 0.036 |
| Cardiovascular History | |||
| Peripheral Arteriopathy | 1.17 | 1.08–1.27 | <0.001 |
| Ischaemic Heart Disease | 1.08 | 1.02–1.13 | 0.006 |
| Aortic Atheromatosis | 0.96 | 0.79–1.18 | 0.723 |
| Ischaemic Stroke or Transient Ischaemic Attack | 1.04 | 0.98–1.10 | 0.213 |
| Intracranial Haemorrhage | 1.35 | 1.10–1.67 | 0.004 |
| Morbidity | |||
| Diabetes Mellitus | 1.19 | 1.14–1.24 | <0.001 |
| Arterial Hypertension | 0.95 | 0.90–1.00 | 0.034 |
| Heart Failure | 1.18 | 1.12–1.23 | <0.001 |
| Renal Insufficiency | 1.13 | 1.08–1.18 | <0.001 |
| Bleeding Risk History | |||
| Alcohol | 1.38 | 1.25–1.53 | <0.001 |
| Intracranial Aneurysm | 1.36 | 0.63–2.91 | 0.436 |
| Portal Hypertension | 0.81 | 0.51–1.29 | 0.372 |
| Liver Failure | 1.37 | 1.07–1.77 | 0.014 |
| Hereditary Telangiectasia | 1.61 | 0.10–25.91 | 0.736 |
| Active Aortic Aneurysm and Dissection | 1.04 | 0.88–1.23 | 0.673 |
| Intestinal Angiodysplasia | 1.39 | 0.92–2.11 | 0.116 |
| Haemorrhages Other Than Gastrointestinal and Intracranial | 0.89 | 0.75–1.06 | 0.202 |
| Gastrointestinal Bleeding | 1.11 | 1.03–1.20 | 0.005 |
| Patients Treated Outside Primary Care Centre | |||
| Treated at Home | 1.33 | 1.25–1.42 | <0.001 |
| Treated in an Institution | 1.35 | 1.22–1.50 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dalmau Llorca, M.R.; Aguilar Martín, C.; Carrasco-Querol, N.; Hernández Rojas, Z.; Forcadell Drago, E.; Rodríguez Cumplido, D.; Castro Blanco, E.; Gonçalves, A.Q.; Fernández-Sáez, J. Anticoagulation Control with Acenocoumarol or Warfarin in Non-Valvular Atrial Fibrillation in Primary Care (Fantas-TIC Study). Int. J. Environ. Res. Public Health 2021, 18, 5700. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115700
Dalmau Llorca MR, Aguilar Martín C, Carrasco-Querol N, Hernández Rojas Z, Forcadell Drago E, Rodríguez Cumplido D, Castro Blanco E, Gonçalves AQ, Fernández-Sáez J. Anticoagulation Control with Acenocoumarol or Warfarin in Non-Valvular Atrial Fibrillation in Primary Care (Fantas-TIC Study). International Journal of Environmental Research and Public Health. 2021; 18(11):5700. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115700
Chicago/Turabian StyleDalmau Llorca, M. Rosa, Carina Aguilar Martín, Noèlia Carrasco-Querol, Zojaina Hernández Rojas, Emma Forcadell Drago, Dolores Rodríguez Cumplido, Elisabet Castro Blanco, Alessandra Queiroga Gonçalves, and José Fernández-Sáez. 2021. "Anticoagulation Control with Acenocoumarol or Warfarin in Non-Valvular Atrial Fibrillation in Primary Care (Fantas-TIC Study)" International Journal of Environmental Research and Public Health 18, no. 11: 5700. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115700