
Healthcare Utilization in Different Stages among Patients with Dementia: A Nationwide Population-Based Study


Abstract
:1. Introduction
2. Materials and Methods
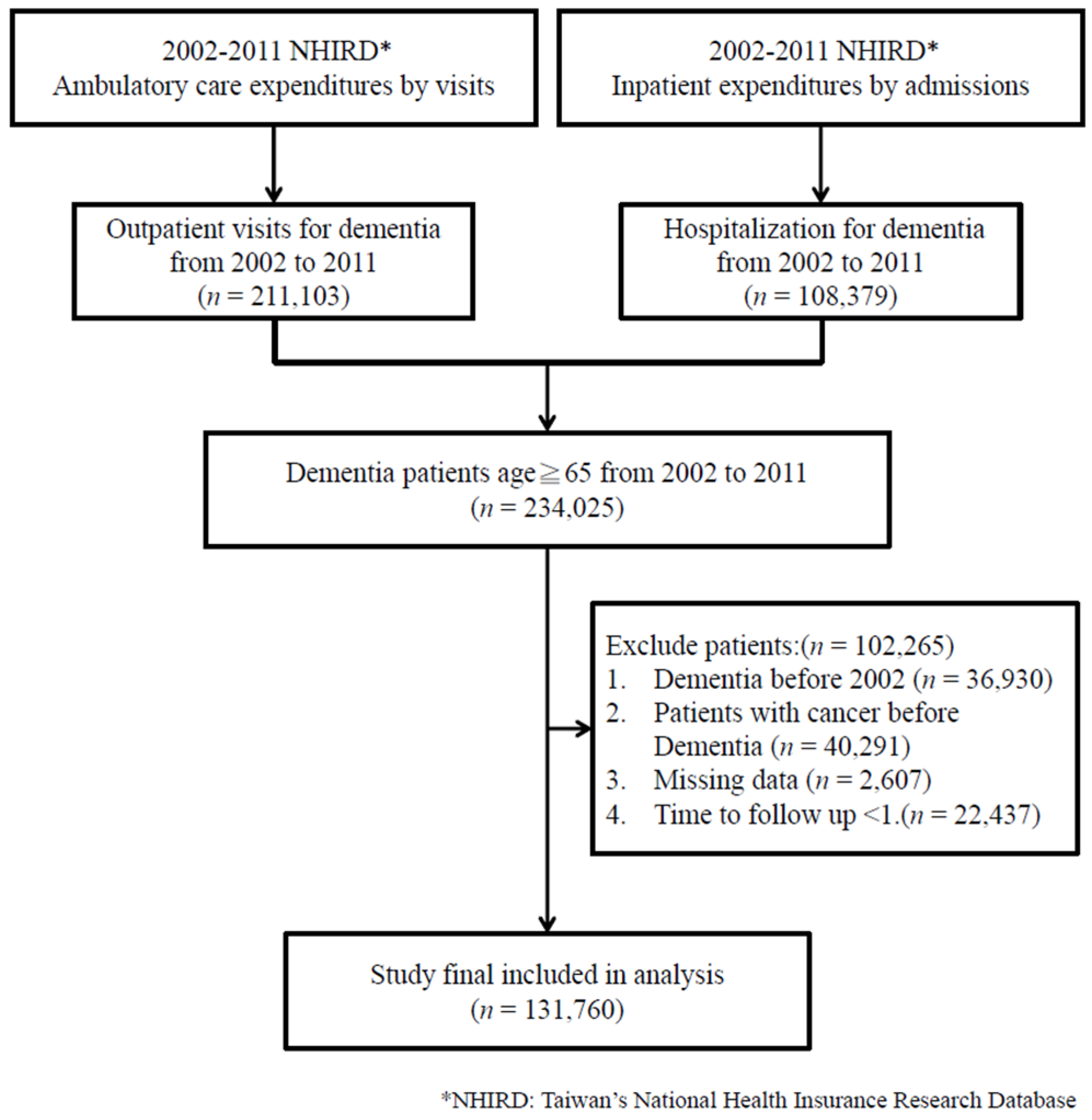
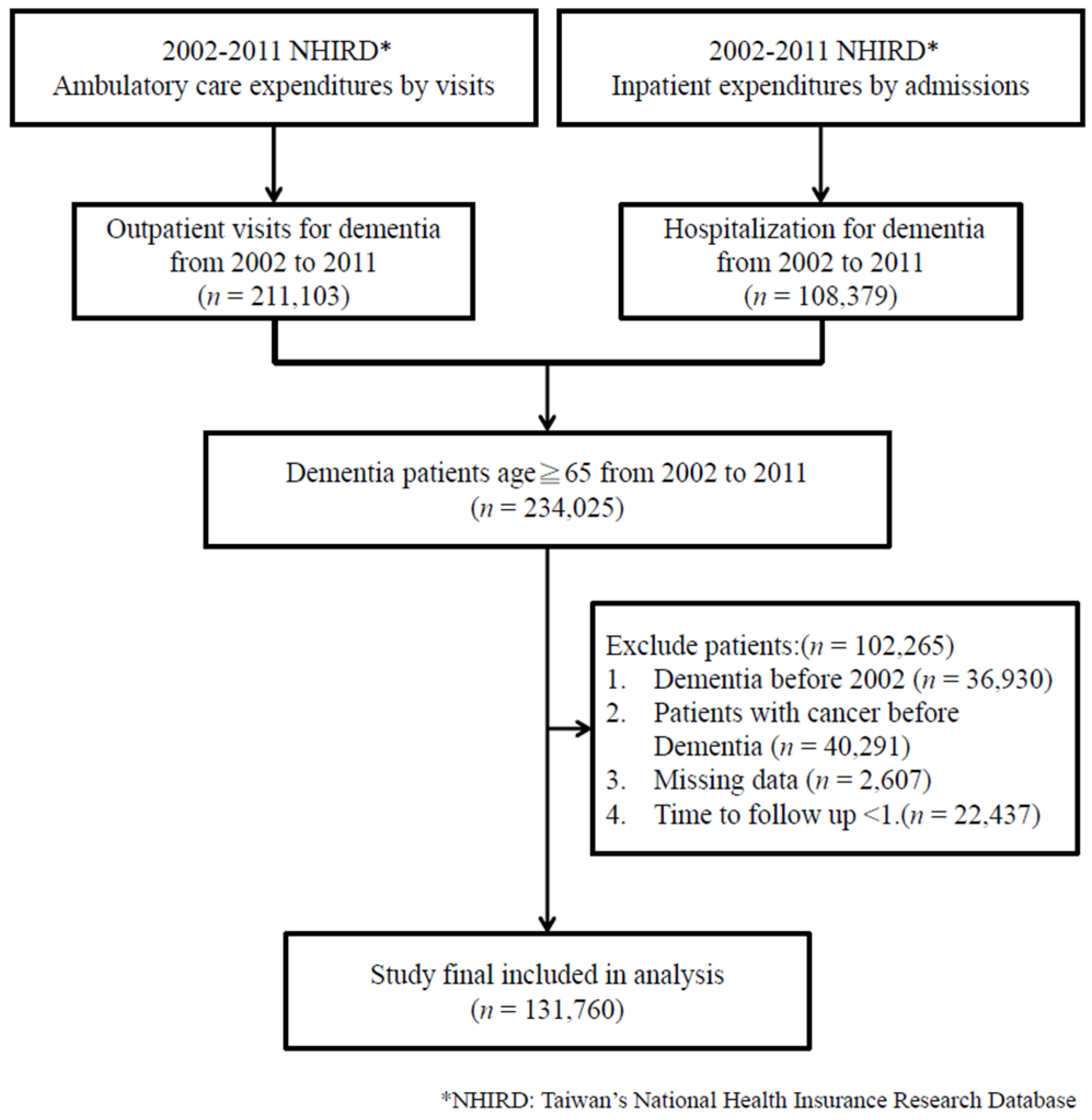
2.1. Data Source and Study Population
2.2. Measurements
2.3. Statistical Analysis
3. Results
3.1. Characteristics of the Study Group
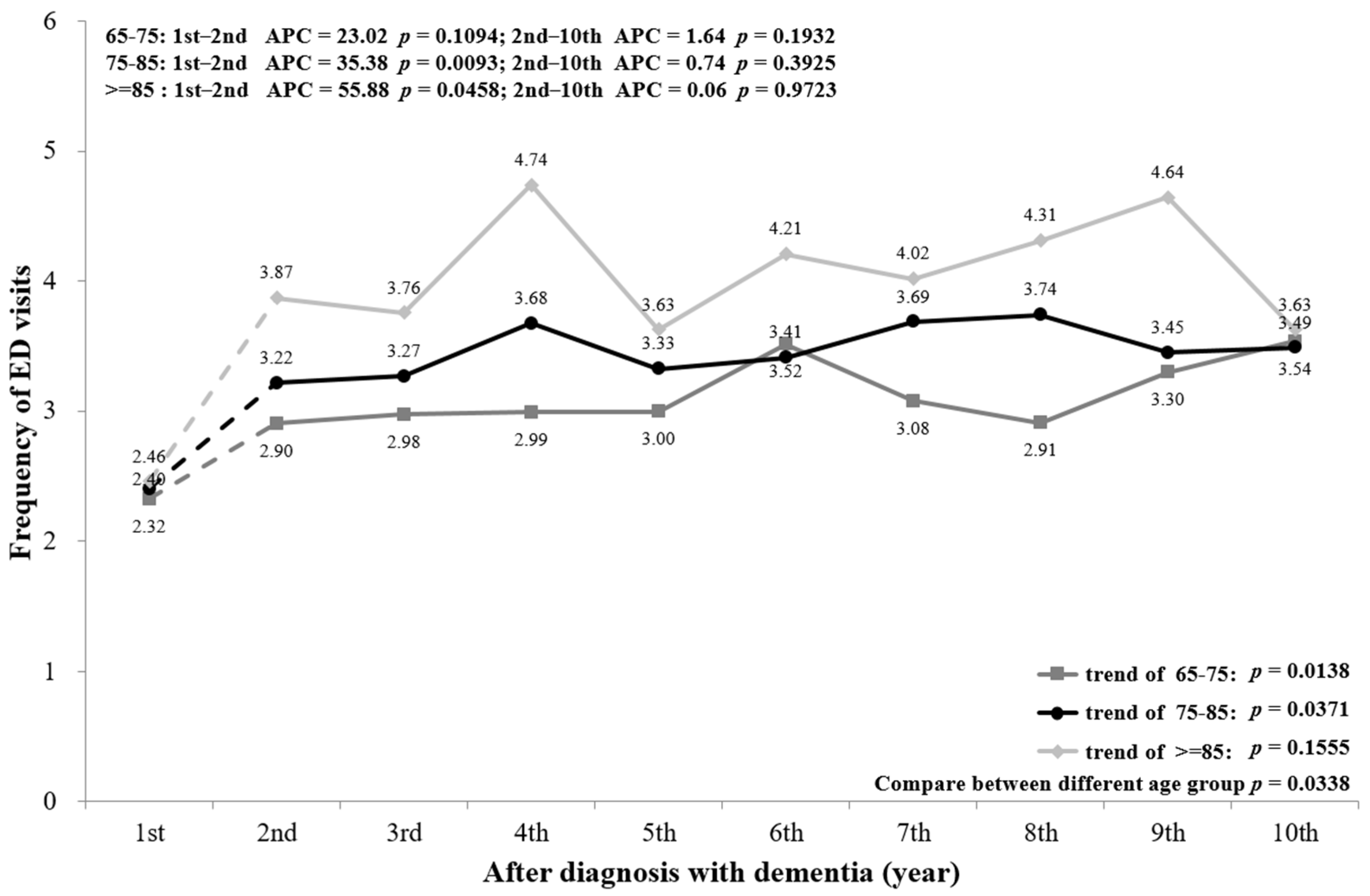
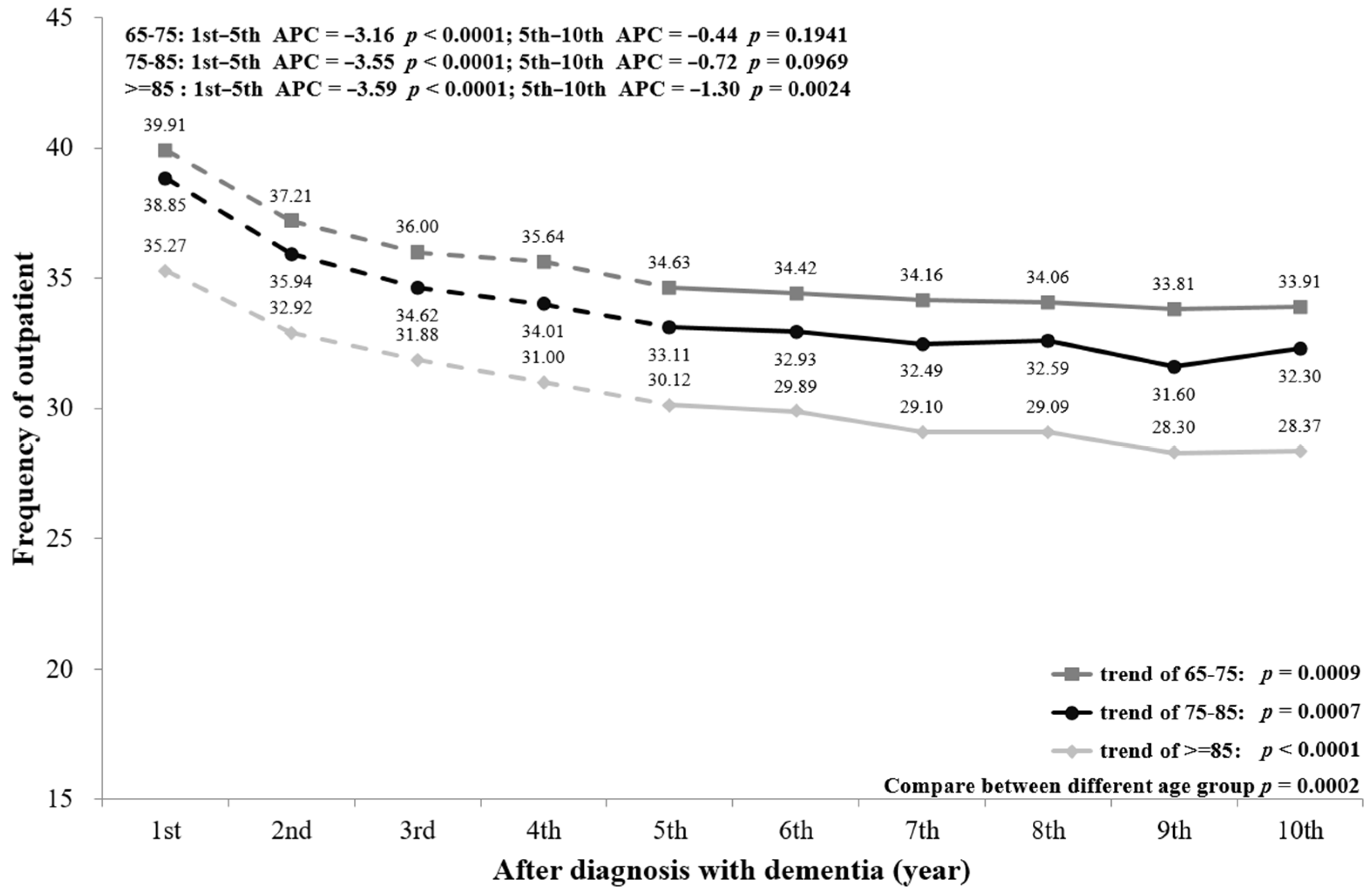
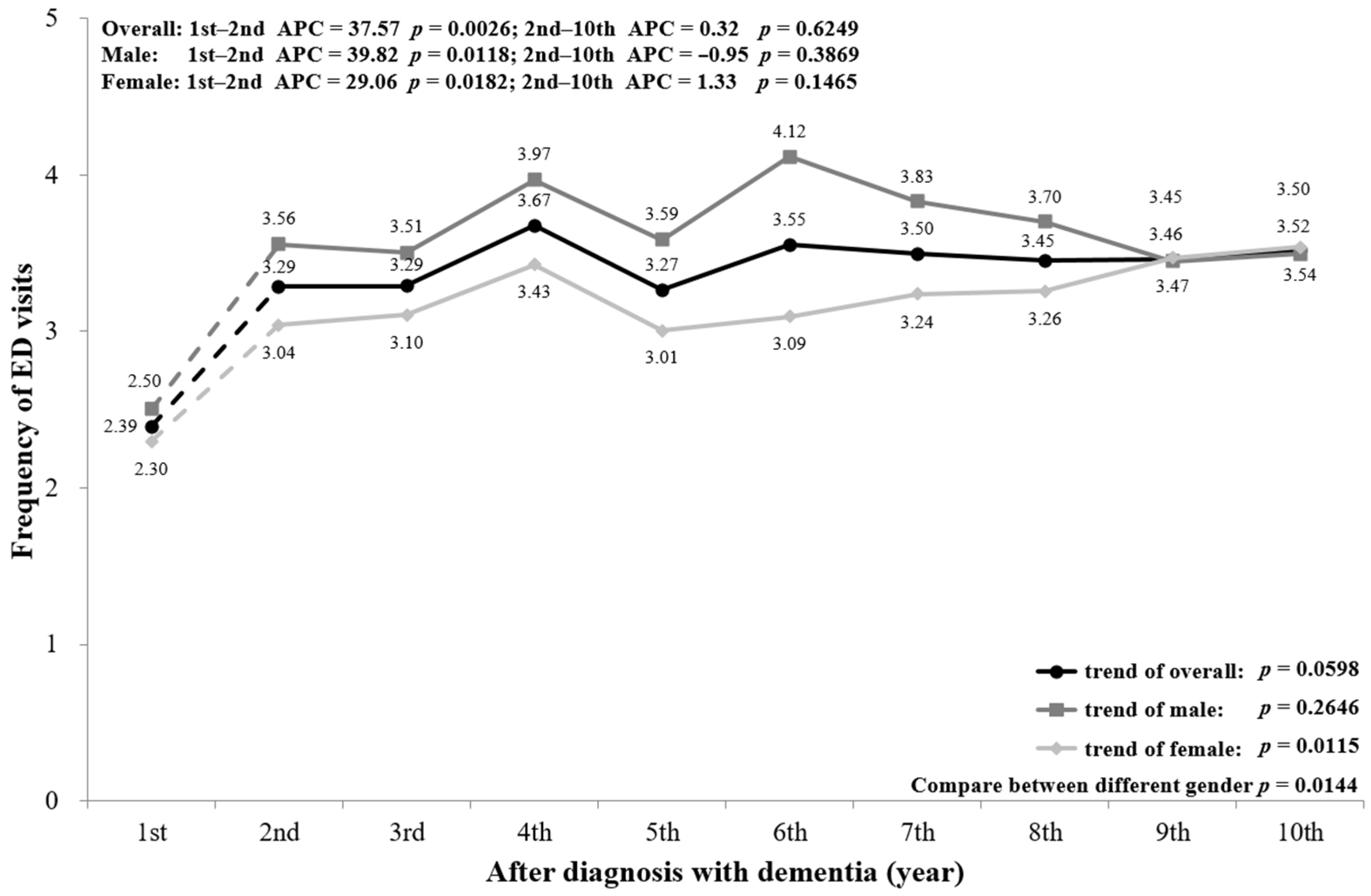
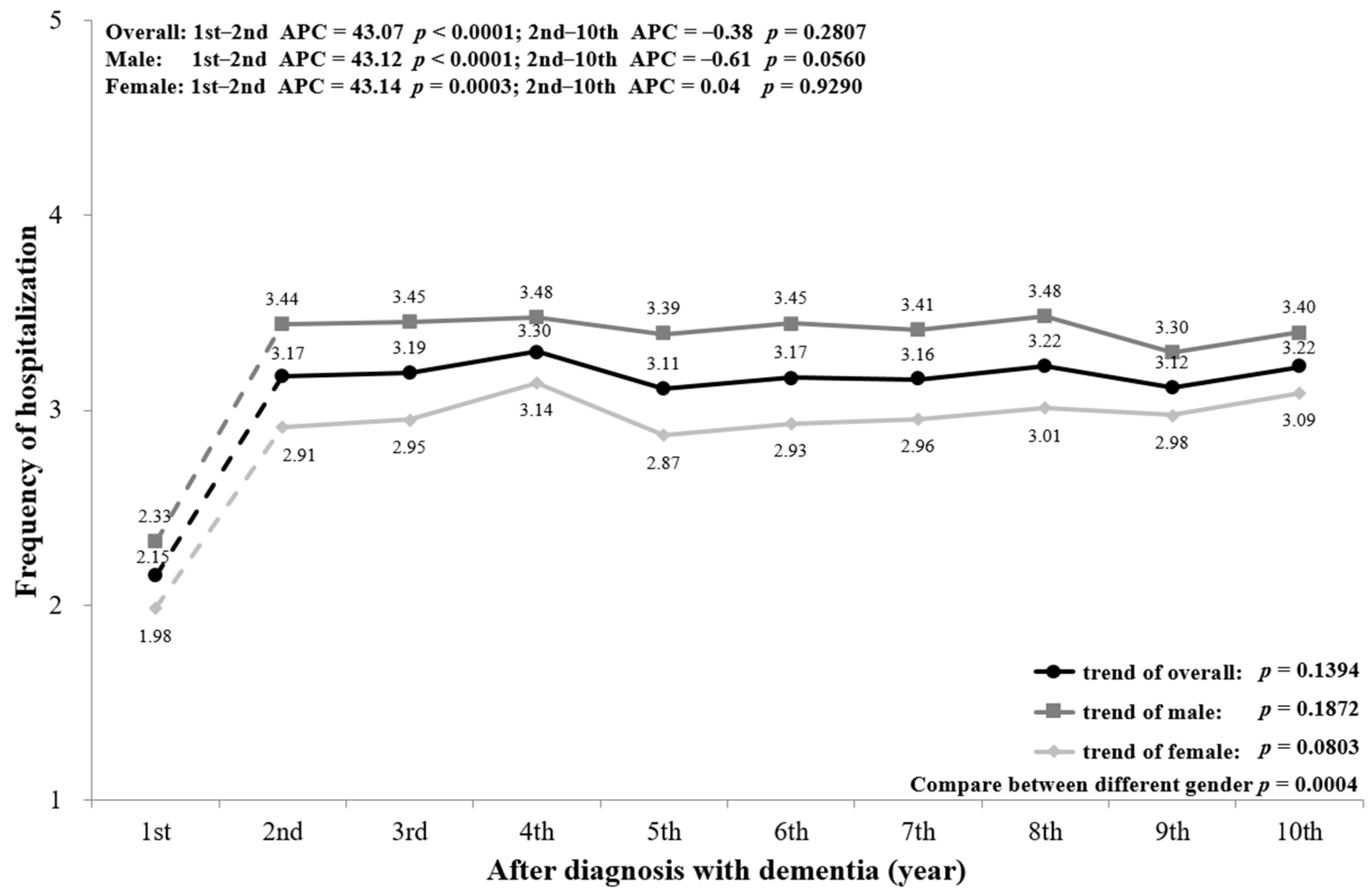
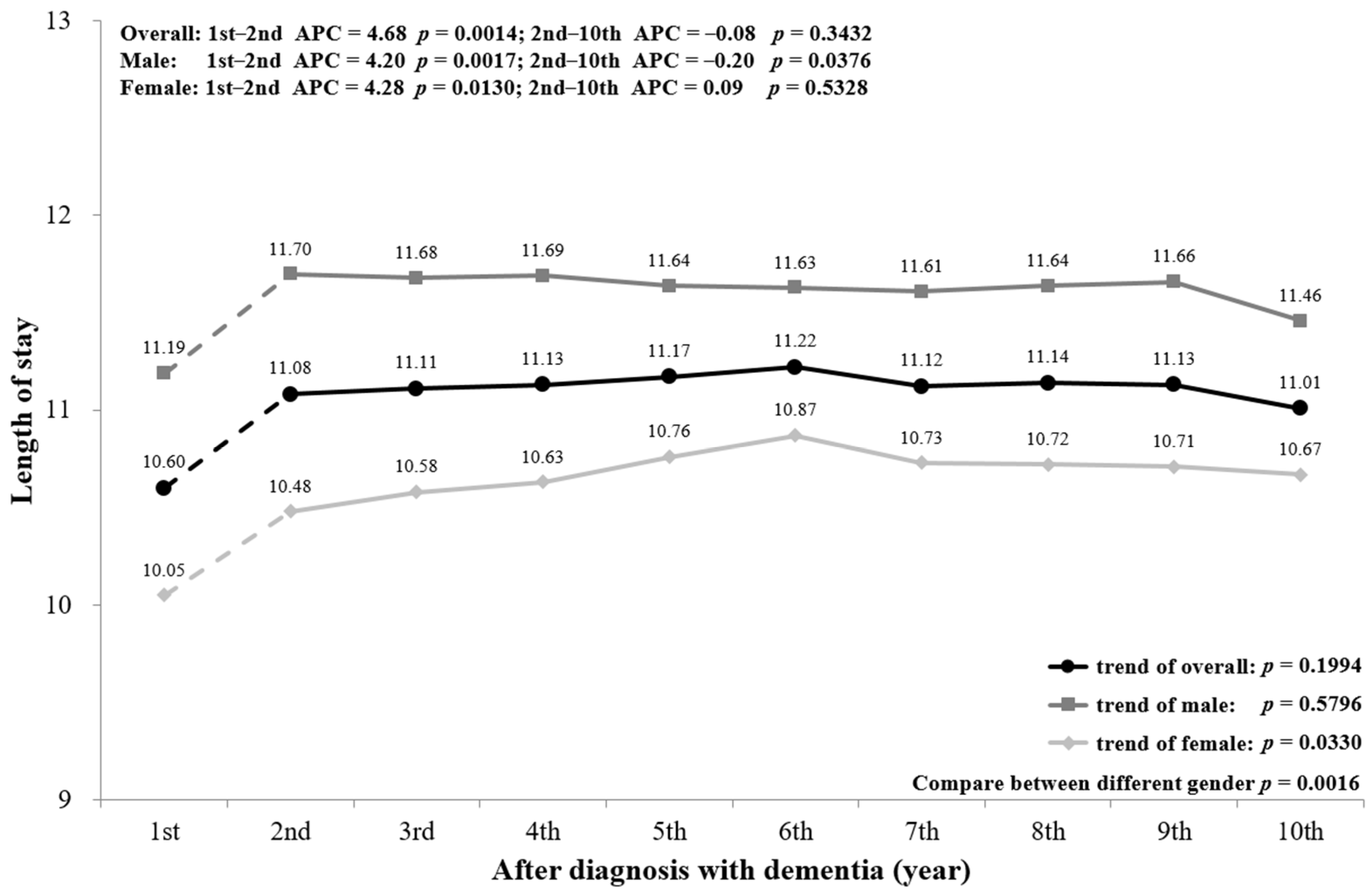
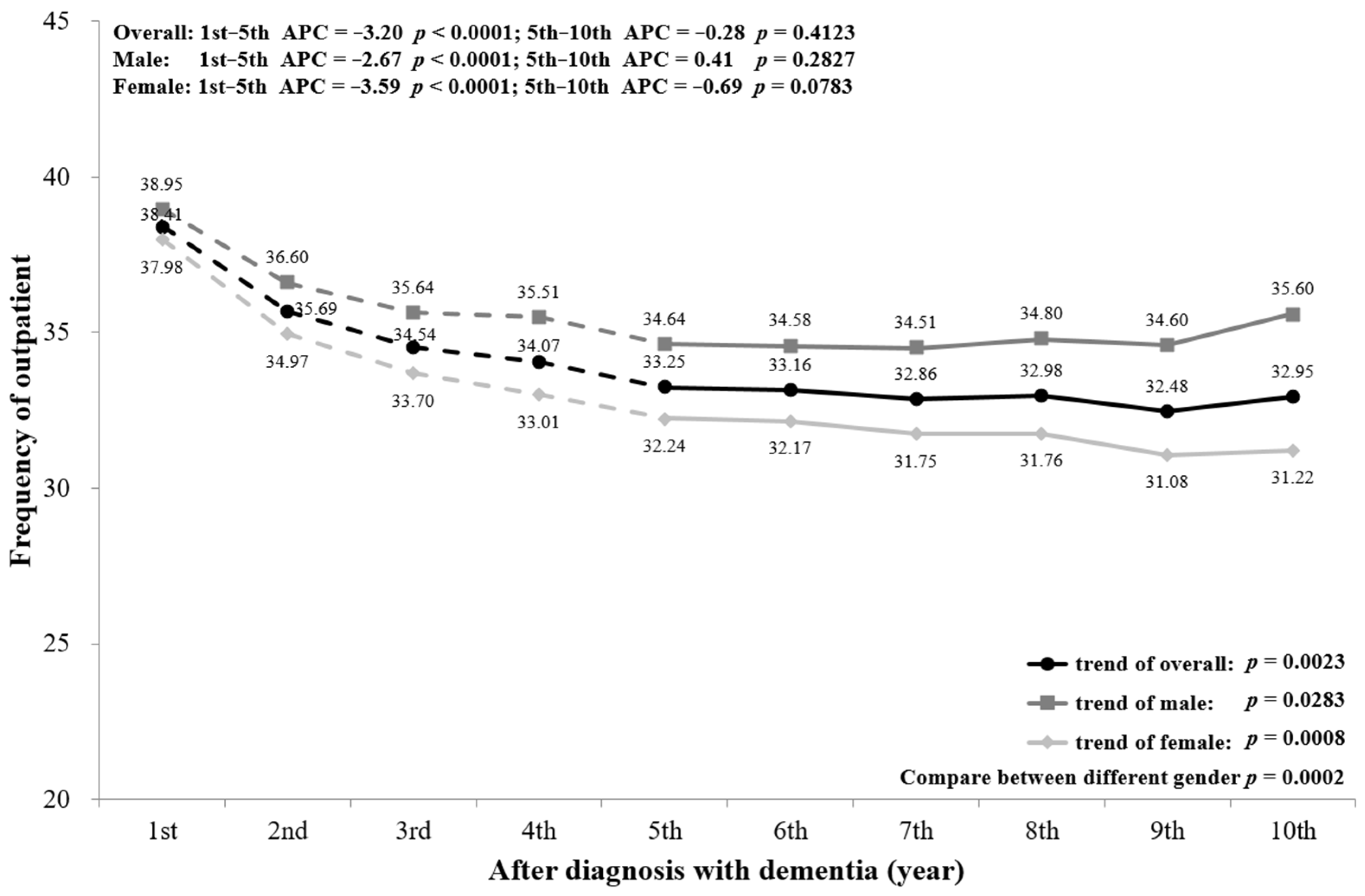
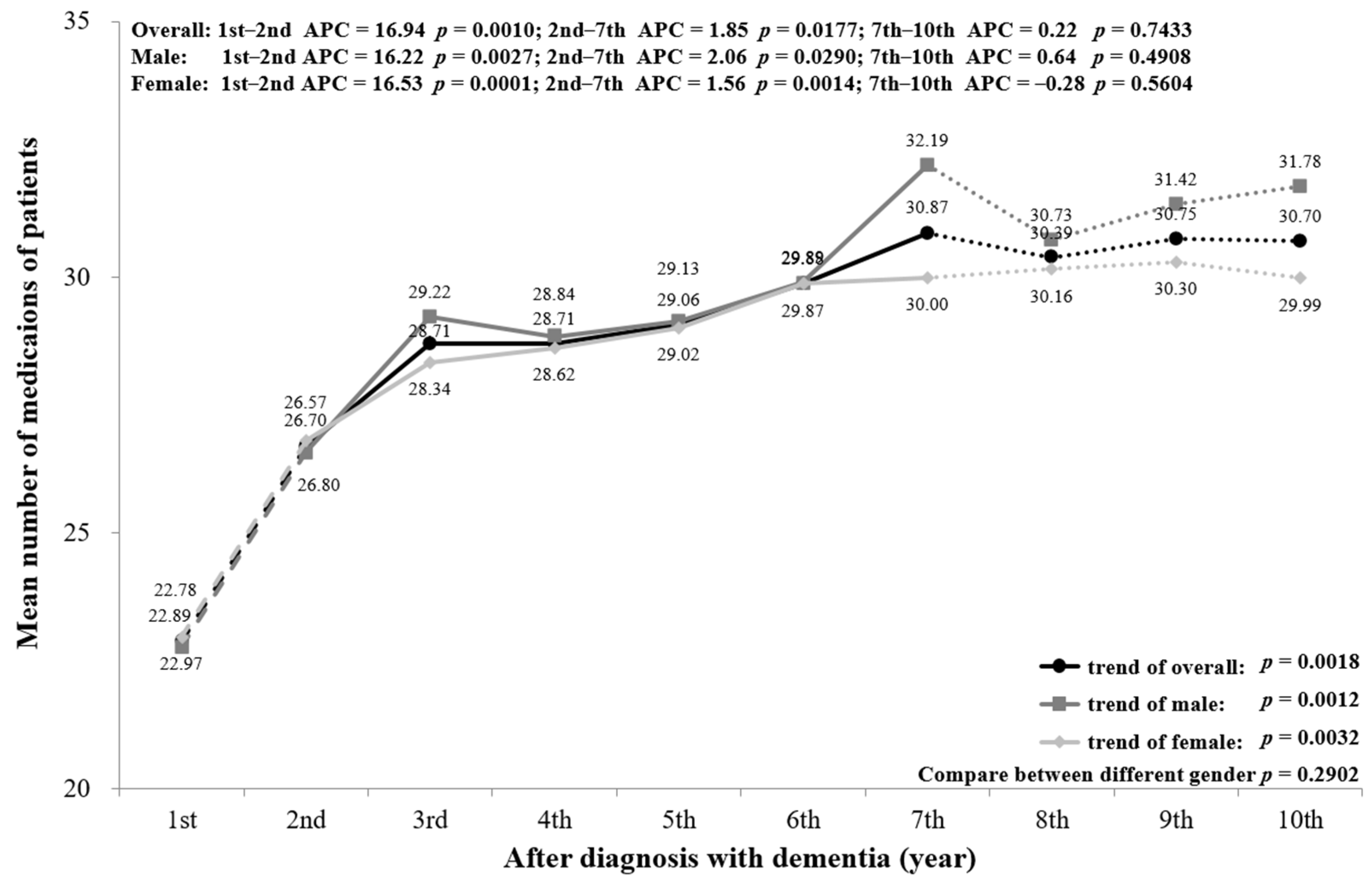
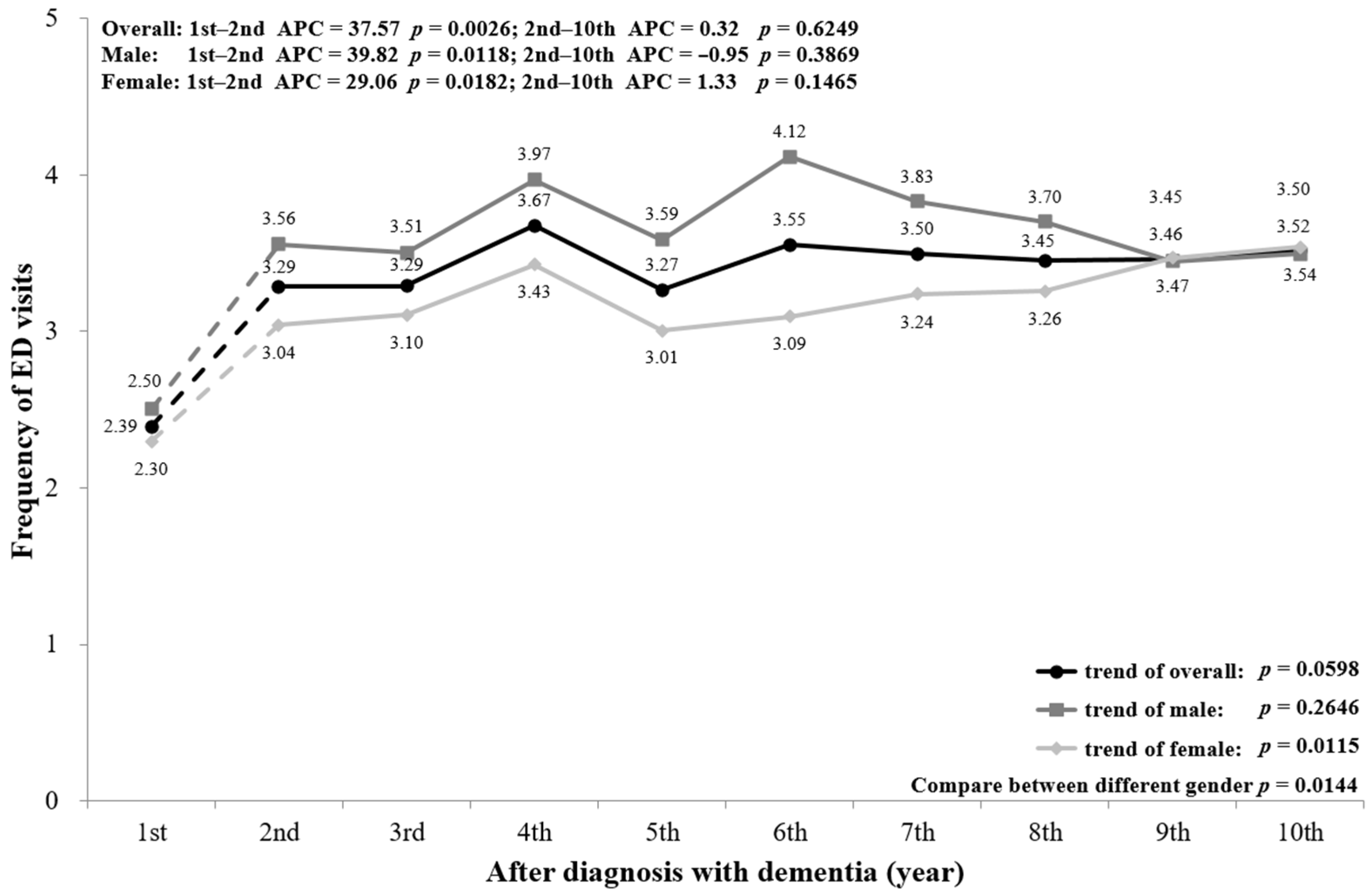
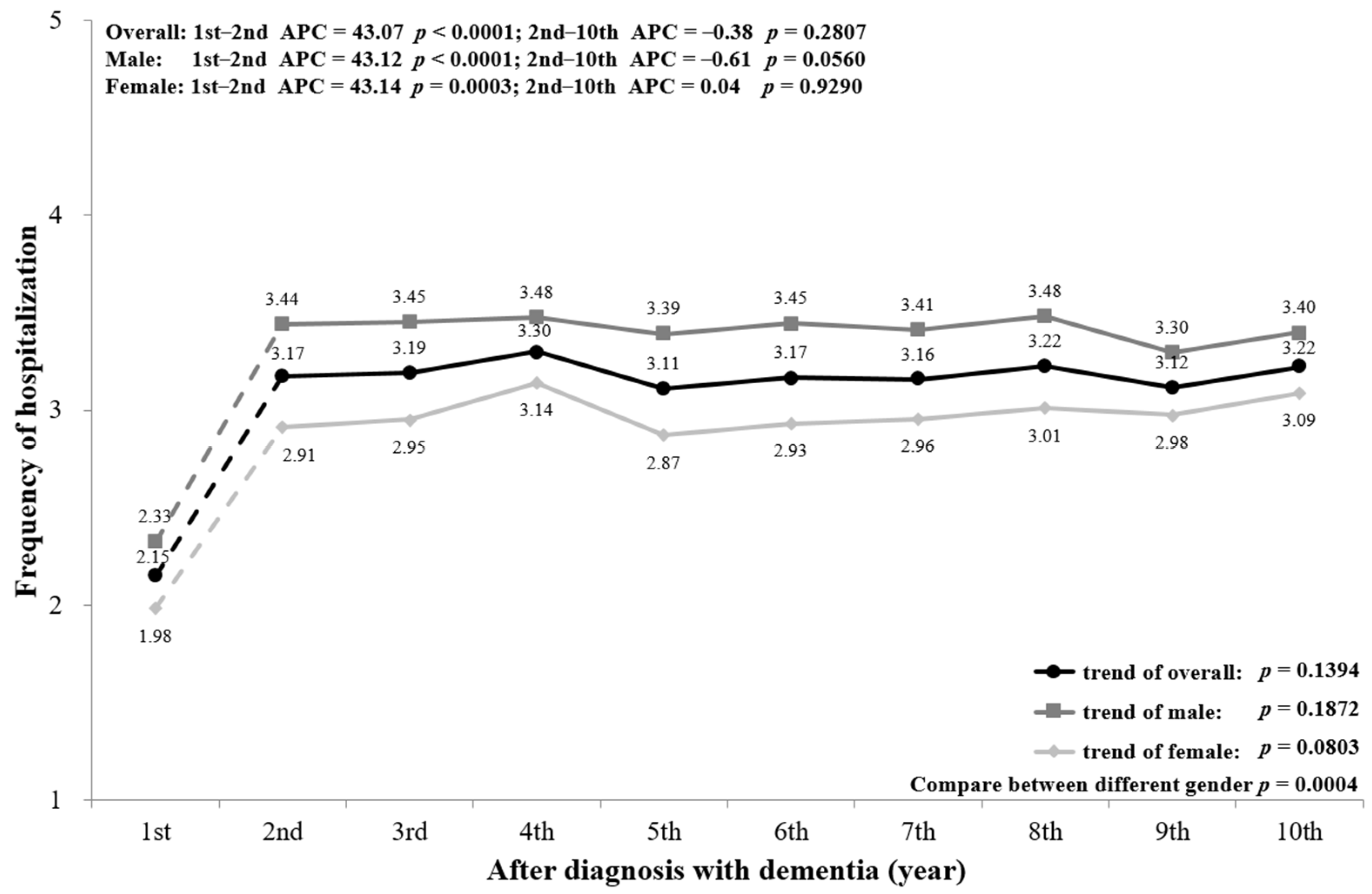
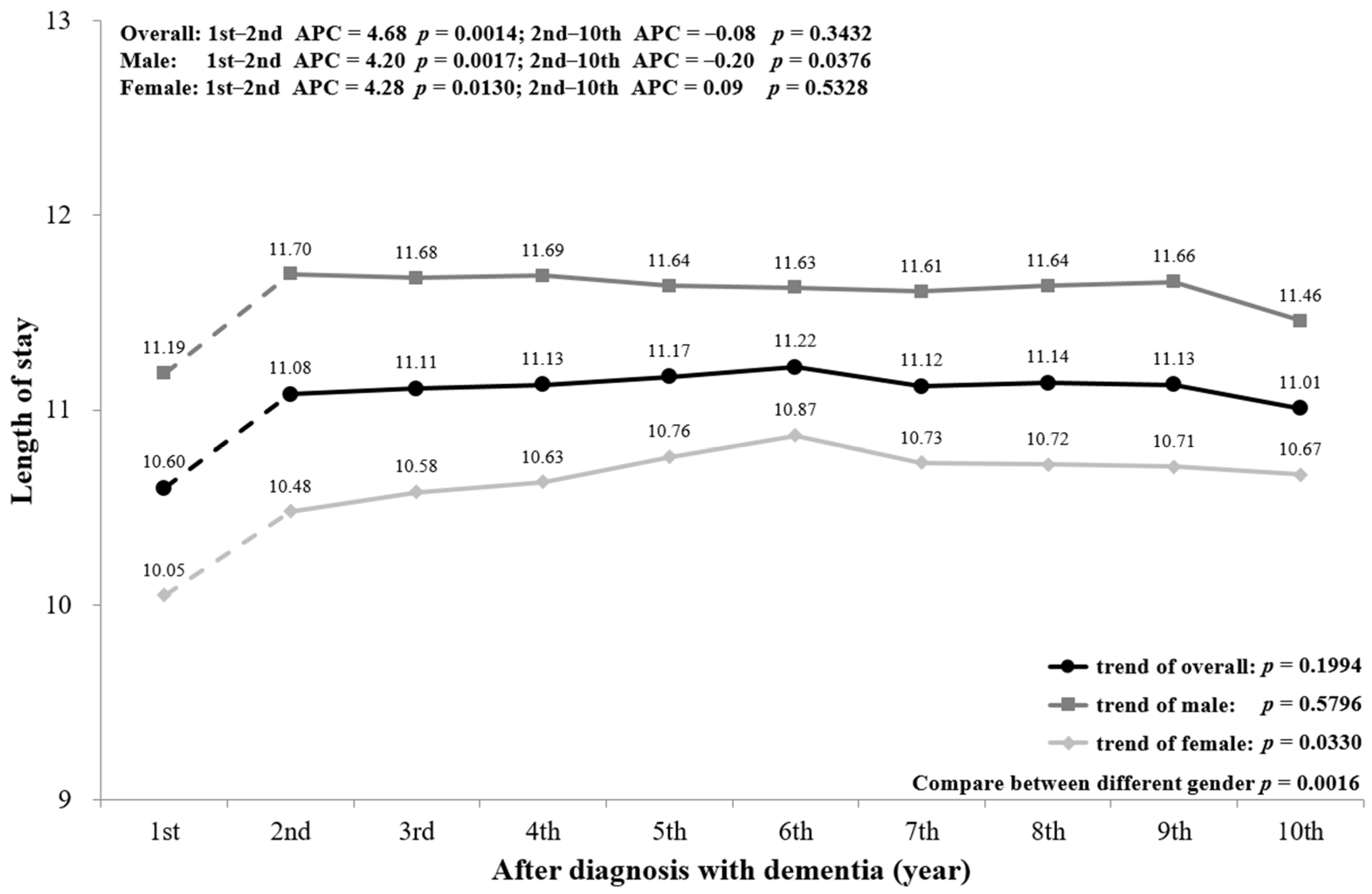
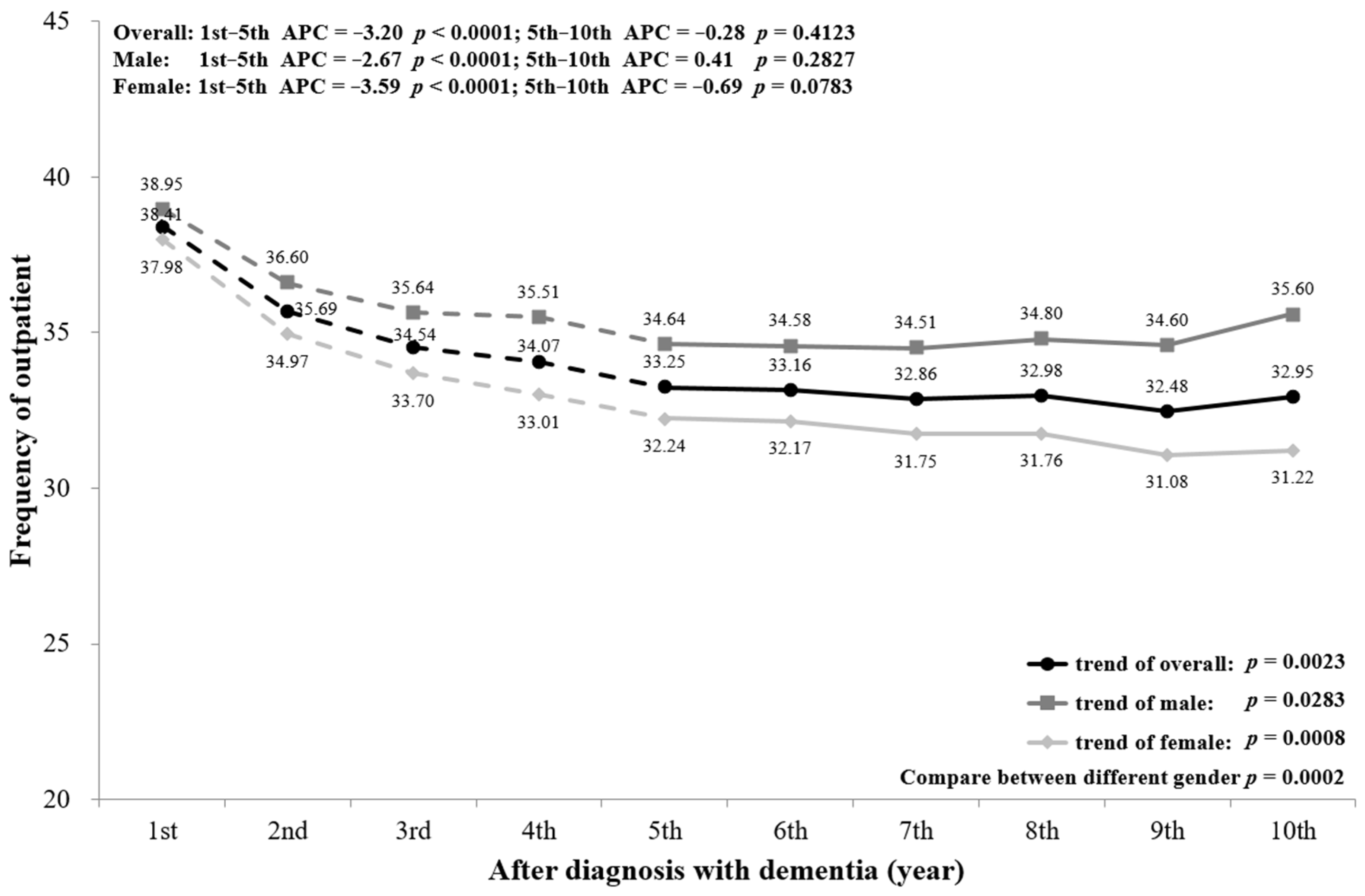
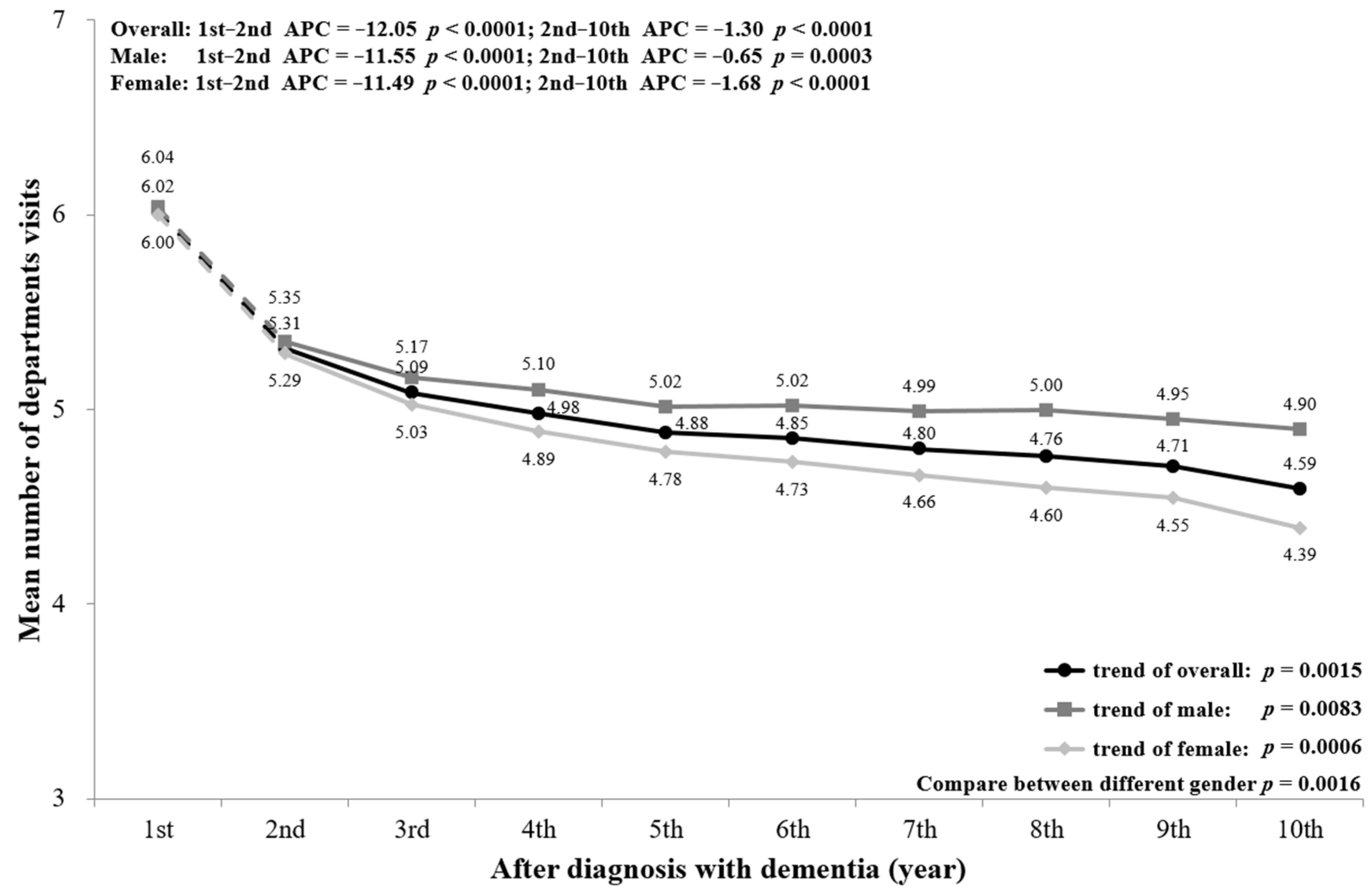
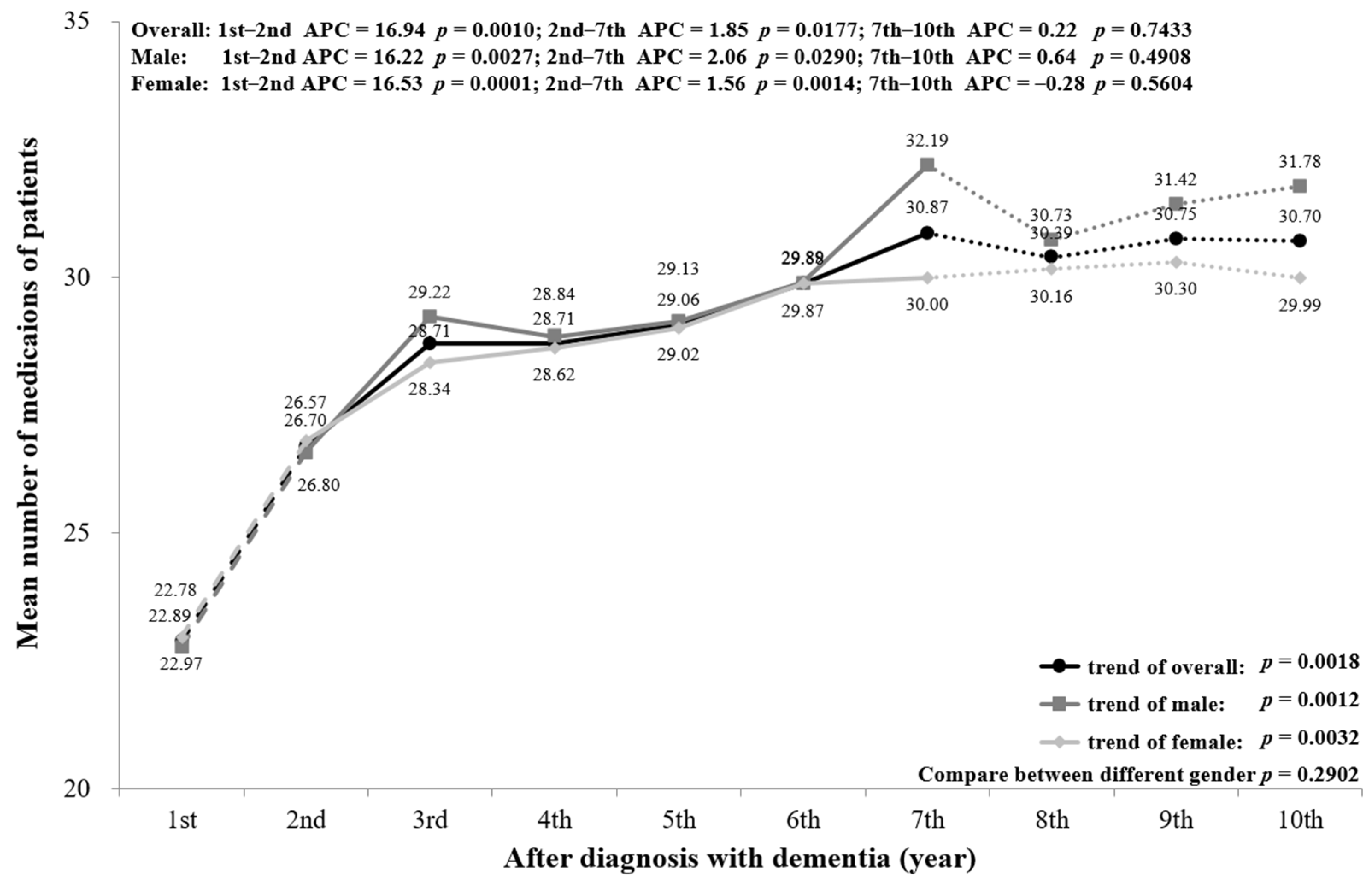
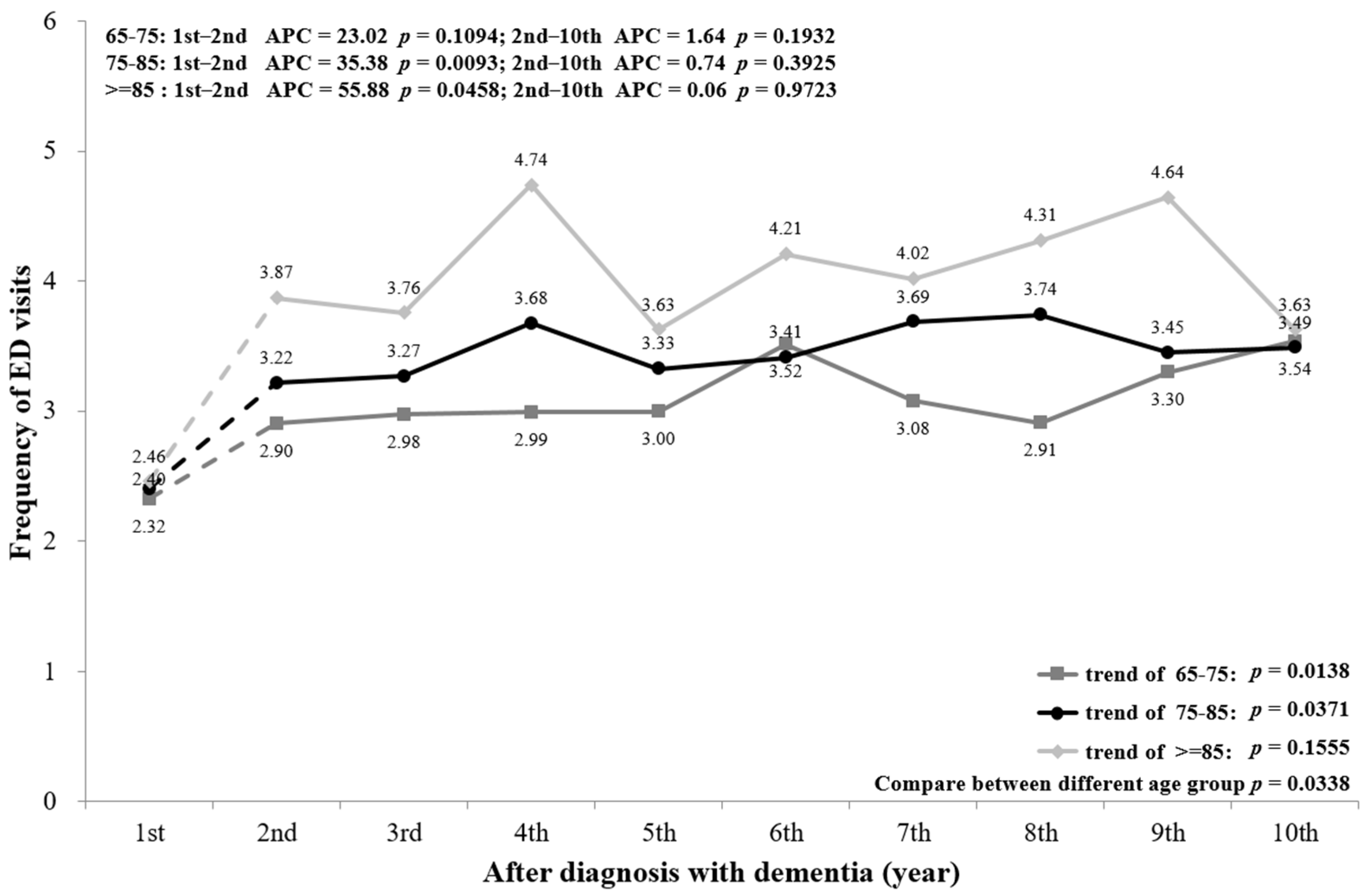
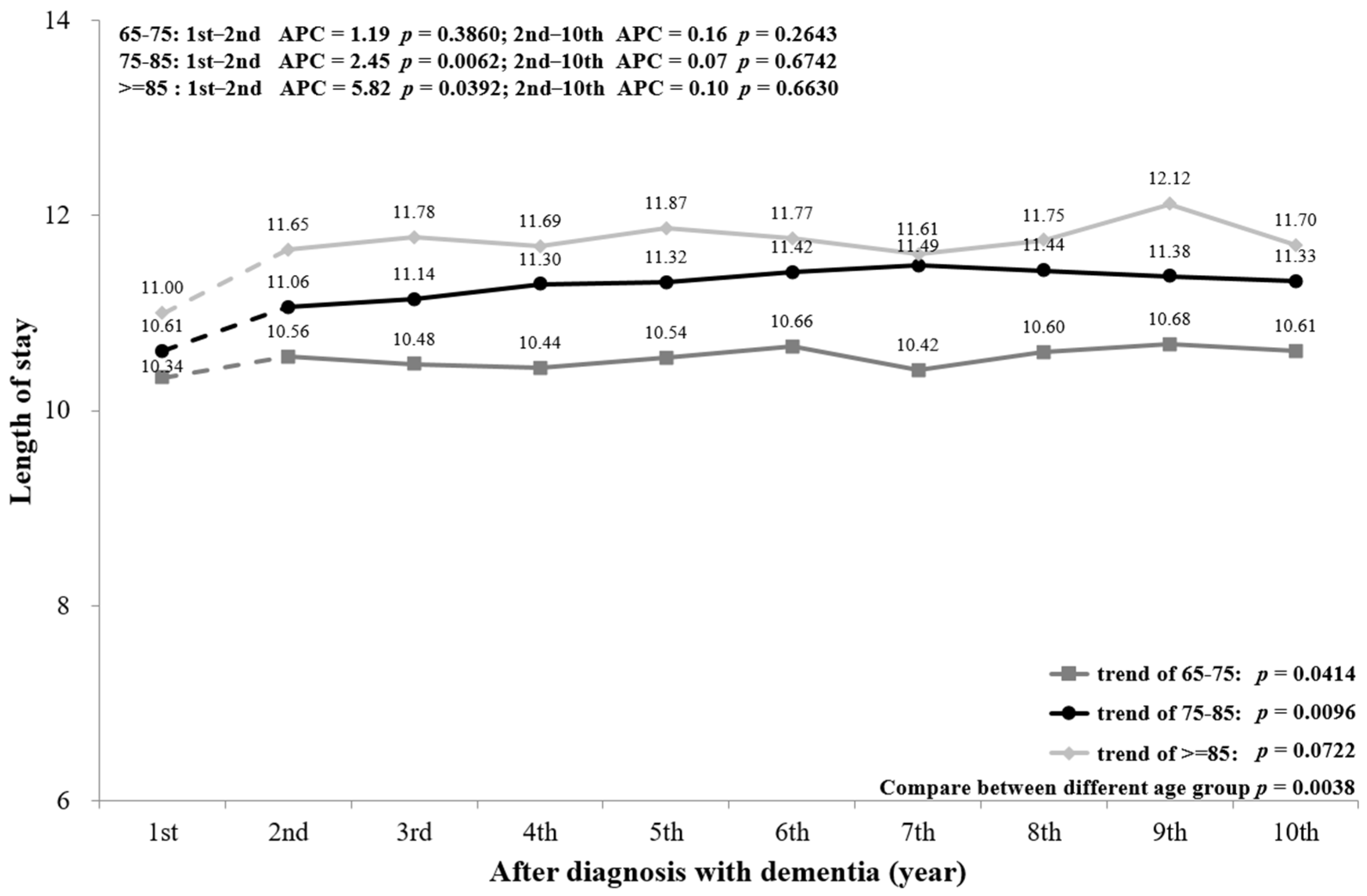
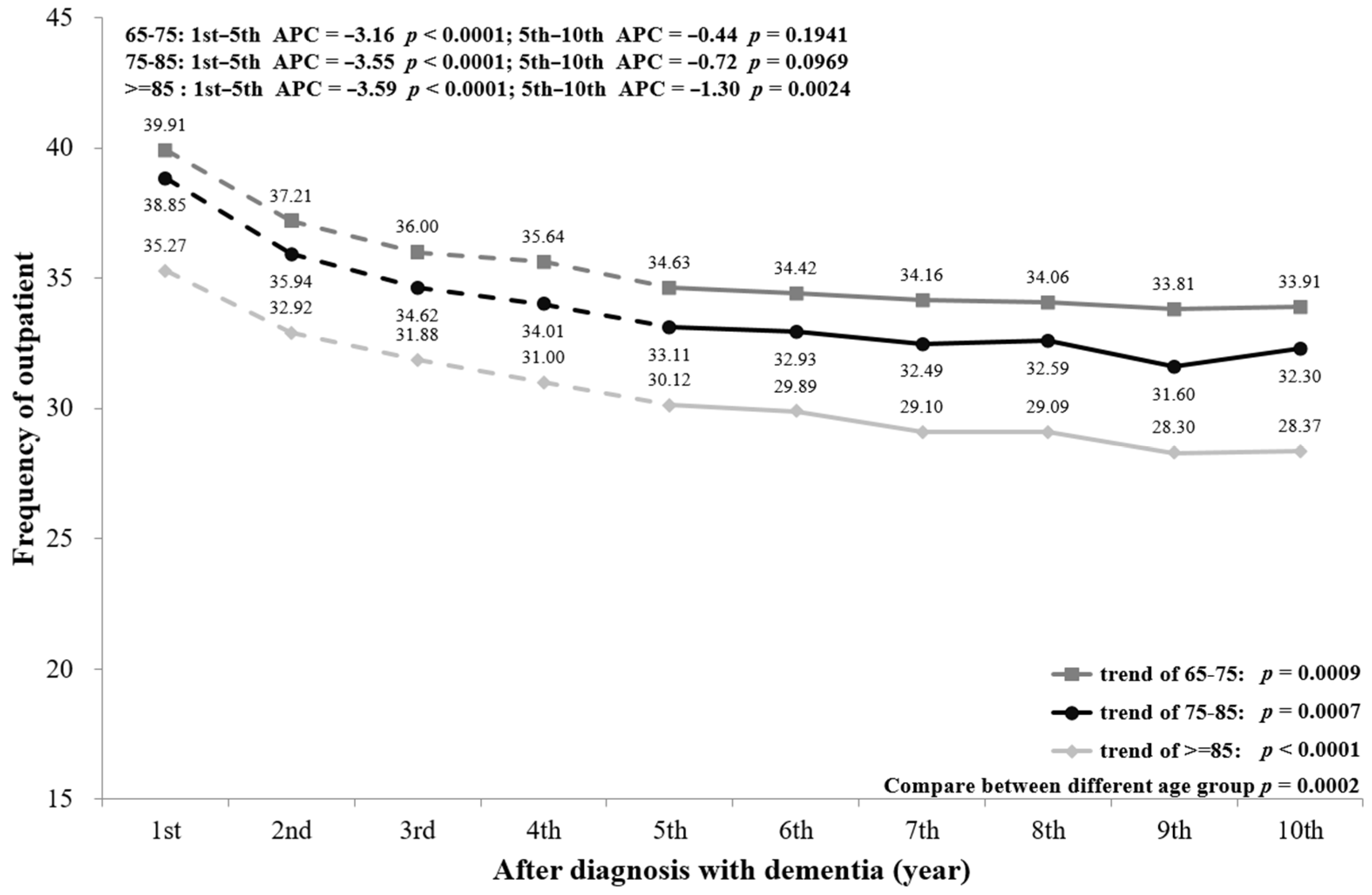
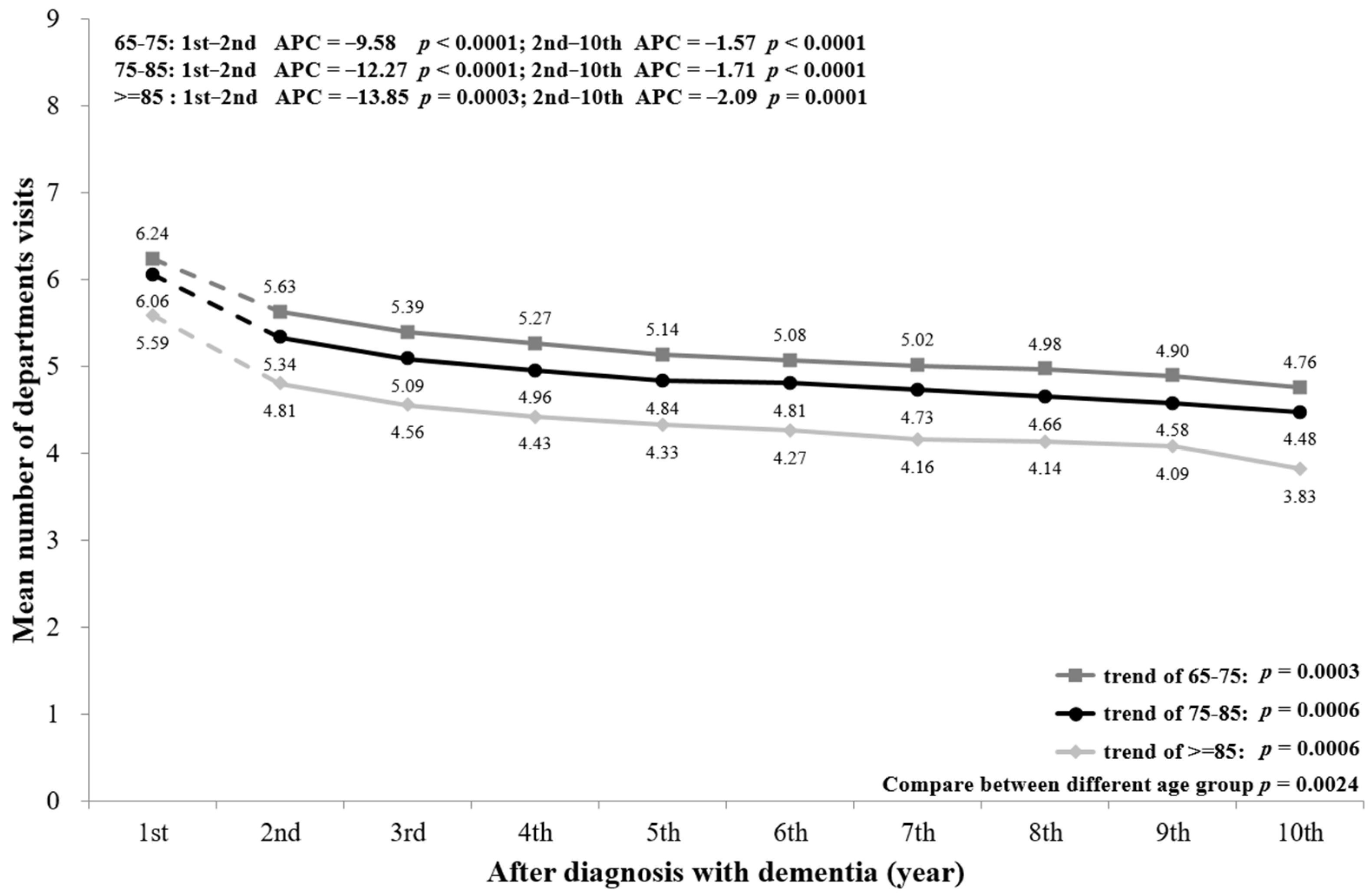
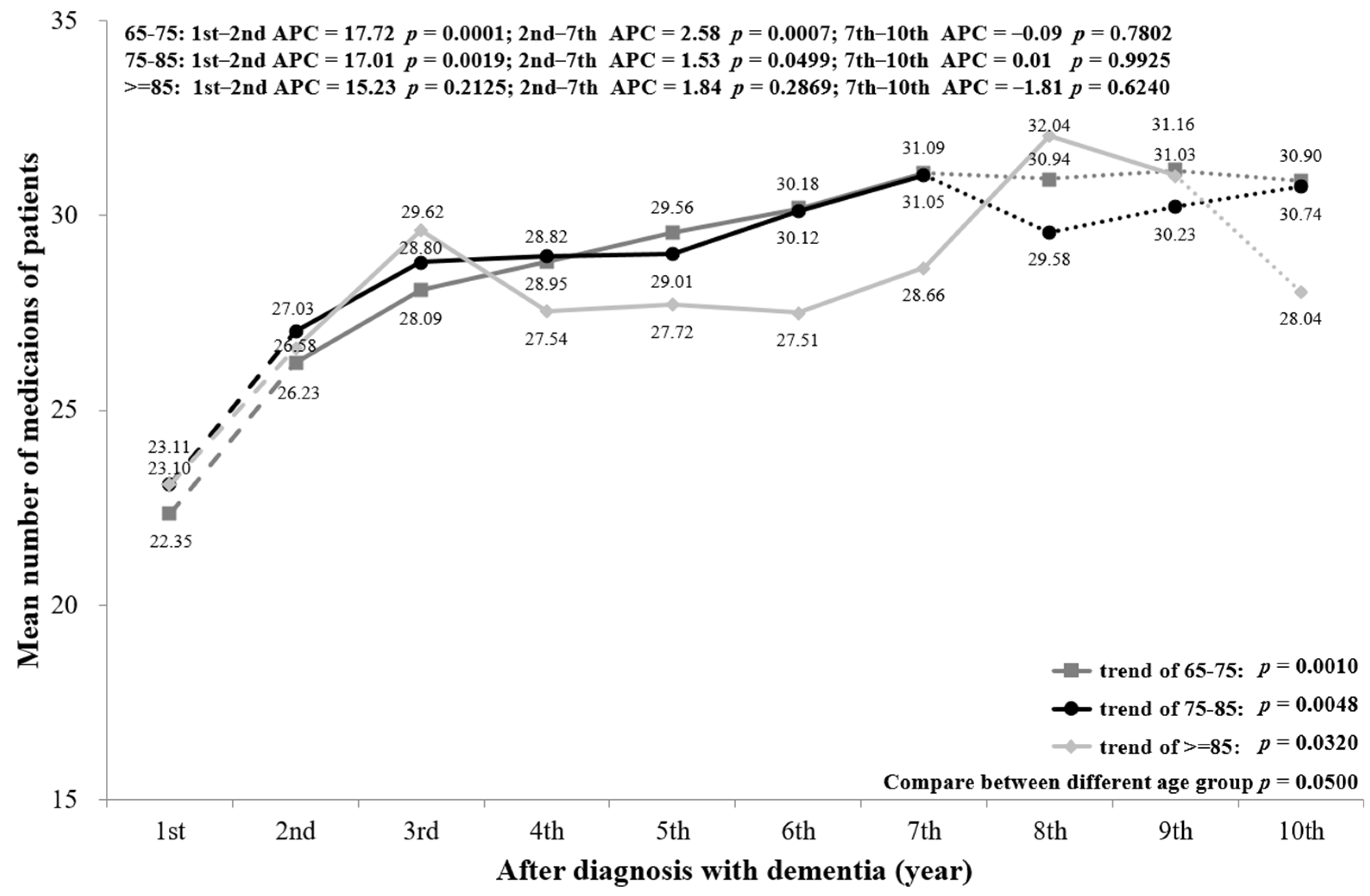
3.2. Utilization of Healthcare Services
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A




References
- Cunningham, E.L.; McGuinness, B.; Herron, B.; Passmore, A.P. Dementia. Ulst. Med. J. 2015, 84, 79–87. [Google Scholar]
- Chung, S.D.; Liu, S.P.; Sheu, J.J.; Lin, C.C.; Lin, H.C.; Chen, C.H. Increased healthcare service utilizations for patients with dementia: A population-based study. PLoS ONE 2014, 9, e105789. [Google Scholar] [CrossRef]
- Frytak, J.R.; Henk, H.J.; Zhao, Y.; Bowman, L.; Flynn, J.A.; Nelson, M. Health service utilization among Alzheimer’s disease patients: Evidence from managed care. Alzheimers Dement. 2008, 4, 361–367. [Google Scholar] [CrossRef]
- Schaller, S.; Mauskopf, J.; Kriza, C.; Wahlster, P.; Kolominsky-Rabas, P.L. The main cost drivers in dementia: A systematic review. Int. J. Geriatr. Psychiatry 2015, 30, 111–129. [Google Scholar] [CrossRef] [PubMed]
- Takizawa, C.; Thompson, P.L.; van Walsem, A.; Faure, C.; Maier, W.C. Epidemiological and economic burden of Alzheimer’s disease: A systematic literature review of data across Europe and the United States of America. J. Alzheimers Dis. 2015, 43, 1271–1284. [Google Scholar] [CrossRef] [PubMed]
- Wimo, A.; Guerchet, M.; Ali, G.C.; Wu, Y.T.; Prina, A.M.; Winblad, B. The worldwide costs of dementia 2015 and comparisons with 2010. Alzheimers Dement. 2017, 13, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Bynum, J.P.; Rabins, P.V.; Weller, W.; Niefeld, M.; Anderson, G.F.; Wu, A.W. The relationship between a dementia diagnosis, chronic illness, medicare expenditures, and hospital use. J. Am. Geriatr. Soc. 2004, 52, 187–194. [Google Scholar] [CrossRef]
- Arling, G.; Tu, W.; Stump, T.E.; Rosenman, M.B.; Counsell, S.R.; Callahan, C.M. Impact of dementia on payments for long-term and acute care in an elderly cohort. Med. Care 2013, 51, 575–581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldfeld, K.S.; Stevenson, D.G.; Hamel, M.B.; Mitchell, S.L. Medicare expenditures among nursing home residents with advanced dementia. Arch. Intern. Med. 2011, 171, 824–830. [Google Scholar] [CrossRef] [Green Version]
- Givens, J.L.; Selby, K.; Goldfeld, K.S.; Mitchell, S.L. Hospital transfers of nursing home residents with advanced dementia. J. Am. Geriatr. Soc. 2012, 60, 905–909. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.T.; Ali, G.C.; Guerchet, M.; Prina, A.M.; Chan, K.Y.; Prince, M. Prevalence of dementia in mainland China, Hong Kong and Taiwan: An updated systematic review and meta-analysis. Int. J. Epidemiol. 2018, 47, 709–719. [Google Scholar] [CrossRef] [Green Version]
- Fuh, J.L.; Wang, S.J. Dementia in Taiwan: Past, present, and future. Acta Neurol. Taiwan 2008, 17, 153–161. [Google Scholar] [PubMed]
- Chen, Y.H.; Ho, C.H.; Huang, C.C. Comparison of healthcare utilization and life-sustaining interventions between elderly patients with dementia and those with cancer near the end of life: A nationwide, population-based study in Taiwan. Geriatr. Gerontol. Int. 2017, 17, 2545–2551. [Google Scholar] [CrossRef] [PubMed]
- Chen, P.J.; Ho, C.H.; Liao, J.Y.; Smits, L.; Hsiung, C.A.; Yu, S.J.; Zhang, K.P.; Petersen, I.; Sampson, L.E. The Association between Home Healthcare and Burdensome Transitions at the End-of-Life in People with Dementia: A 12-Year Nationwide Population-Based Cohort Study. Int. J Environ. Res. Public Health 2020, 17, 9255. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Fay, M.P.; Feuer, E.J.; Midthune, D.N. Permutation tests for joinpoint regression with applications to cancer rates. Stat. Med. 2000, 19, 335–351. [Google Scholar] [CrossRef]
- Shepherd, H.; Livingston, G.; Chan, J.; Sommerlad, A. Hospitalisation rates and predictors in people with dementia: A systematic review and meta-analysis. BMC Med. 2019, 17, 130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knox, S.; Downer, B.; Haas, A.; Middleton, A.; Ottenbacher, K.J. Dementia Severity Associated With Increased Risk of Potentially Preventable Readmissions During Home Health Care. J. Am. Med. Dir. Assoc. 2020, 21, 519–524. [Google Scholar] [CrossRef] [PubMed]
- Livingston, G.; Huntley, J.; Sommerlad, A.; Ames, D.; Ballard, C.; Banerjee, S. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet 2020, 396, 413–446. [Google Scholar] [CrossRef]
- Sampson, E.L.; Candy, B.; Davis, S.; Gola, A.B.; Harrington, J.; King, M. Living and dying with advanced dementia: A prospective cohort study of symptoms, service use and care at the end of life. Palliat. Med. 2018, 32, 668–681. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van der Steen, J.T.; Radbruch, L.; Hertogh, C.M.P.M.; de Boer, M.E.; Hughes, J.C.; Larkin, P. White paper defining optimal palliative care in older people with dementia: A Delphi study and recommendations from the European Association for Palliative Care. Palliat. Med. 2014, 28, 197–209. [Google Scholar] [CrossRef] [Green Version]
- Miller, S.C.; Lima, J.C.; Mitchell, S.L. Influence of hospice on nursing home residents with advanced dementia who received Medicare-skilled nursing facility care near the end of life. J. Am. Geriatr. Soc. 2012, 60, 2035–2041. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gaugler, J.E.; Yu, F.; Krichbaum, K.; Wyman, J.F. Predictors of Nursing Home Admission for Persons with Dementia. Med. Care 2009, 47, 191–198. [Google Scholar] [CrossRef]
- Gaugler, J.E.; Yu, F.; Davila, H.W.; Shippee, T. Alzheimer’s disease and nursing homes. Health Aff. 2014, 33, 650–657. [Google Scholar] [CrossRef]
- Renom-Guiteras, A.; Thurmann, P.A.; Miralles, R.; Klaassen-Mielke, R.; Thiem, U.; Stephan, A. Potentially inappropriate medication among people with dementia in eight European countries. Age Ageing 2018, 47, 68–74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chuang, H.Y.; Wen, Y.W.; Chen, L.K.; Hsiao, F.Y. Medication appropriateness for patients with dementia approaching the end of their life. Geriatr. Gerontol. Int. 2017, 17 (Suppl. 1), 65–74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tommelein, E.; Mehuys, E.; Petrovic, M.; Somers, A.; Colin, P.; Boussery, K. Potentially inappropriate prescribing in community-dwelling older people across Europe: A systematic literature review. Eur. J. Clin. Pharmacol. 2015, 71, 1415–1427. [Google Scholar] [CrossRef] [PubMed]
- Delgado, J.; Bowman, K.; Clare, L. Potentially inappropriate prescribing in dementia: A state-of-the-art review since 2007. BMJ Open 2020, 10, e029172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thorpe, J.M.; Thorpe, C.T.; Kennelty, K.A.; Gellad, W.F.; Schulz, R. The impact of family caregivers on potentially inappropriate medication use in noninstitutionalized older adults with dementia. Am. J. Geriatr. Pharmacother. 2012, 10, 230–241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lau, D.T.; Mercaldo, N.D.; Harris, A.T.; Trittschuh, E.; Shega, J.; Weintraub, S. Polypharmacy and potentially inappropriate medication use among community-dwelling elders with dementia. Alzheimer Dis. Assoc. Disord. 2010, 24, 56–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wucherer, D.; Eichler, T.; Hertel, J.; Kilimann, I.; Richter, S.; Michalowsky, B. Potentially Inappropriate Medication in Community-Dwelling Primary Care Patients who were Screened Positive for Dementia. J. Alzheimers Dis. 2017, 55, 691–701. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Unutmaz, G.D.; Soysal, P.; Tuven, B.; Isik, A.T. Costs of medication in older patients: Before and after comprehensive geriatric assessment. Clin. Interv. Aging 2018, 13, 607–613. [Google Scholar] [CrossRef] [PubMed]
- Sharmin, S.B.; Hamish, A.J.; Prasad, S.N. Determinants of prescribing potentially inappropriate medications in a nationwide cohort of community dwellers with dementia receiving a comprehensive geriatric assessment. Int. J. Geriatr. Psychiatry 2019, 34, 153–161. [Google Scholar]
- O’Caoimh, R.; Cornally, N.; McGlade, C.; Gao, Y.; O’Herlihy, E.; Svendrovski, A. Reducing inappropriate prescribing for older adults with advanced frailty: A review based on a survey of practice in four countries. Maturitas 2019, 126, 1–10. [Google Scholar] [CrossRef]
- Kase, Y.; Hattori, Y.; Umeda-Kameyama, Y.; Kojima, T.; Ogawa, S.; Akishita, M. Improvement in polypharmacy and medication regimen complexity among older inpatients with dementia in a geriatric ward. Geriatr. Gerontol. Int. 2019, 19, 461–462. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Year from Diagnosis | n | Women, n (%) | Deaths During Year, n (%) | Diagnosed Age (Mean ± SD) | Patients with Loss to Follow up |
|---|---|---|---|---|---|
| 1st year | 131,760 | 72,955 (55.37) | 0 | 78.71 ± 6.92 | 0 |
| 2nd year | 131,760 | 72,955 (55.37) | 15,617 (11.85) | 78.71 ± 6.92 | 0 |
| 3rd year | 116,143 | 65,702 (56.57) | 12,988 (11.18) | 78.34 ± 6.81 | 12,101 (10.42) |
| 4th year | 91,054 | 52,241 (57.37) | 10,207 (11.21) | 77.85 ± 6.69 | 11,821 (12.98) |
| 5th year | 69,026 | 39,920 (57.83) | 7790 (11.29) | 77.36 ± 6.57 | 10,039 (14.54) |
| 6th year | 51,197 | 29,958 (58.52) | 5739 (11.21) | 76.90 ± 6.48 | 8083 (15.79) |
| 7th year | 37,375 | 22,090 (59.10) | 4091 (10.95) | 76.47 ± 6.39 | 7070 (18.92) |
| 8th year | 26,214 | 15,482 (59.06) | 2792 (10.65) | 76.06 ± 6.30 | 5672 (21.64) |
| 9th year | 17,750 | 10,459 (58.92) | 1698 (9.57) | 75.64 ± 6.23 | 4888 (27.54) |
| 10th year | 11,164 | 6611 (59.22) | 953 (8.54) | 75.41 ± 6.19 | 4134 (37.03) |
| Patients with Dementia (n = 131,760) | |
|---|---|
| Age at diagnosis, n (%) | |
| 65–75 | 71,278 (43.53) |
| 75–85 | 52,326 (31.96) |
| ≥85 | 8156 (4.98) |
| Gender, n (%) | |
| Male | 58,805 (44.63) |
| Female | 72,955 (55.37) |
| Death, n (%) | |
| Yes | 61,875 (46.96) |
| No | 69,885 (53.04) |
| Time to follow, median (Q1–Q3) | 4.16 (2.69–6.37) |
| Variable of healthcare utilization | |
| Emergency frequency, n (%) | 111,845 (84.89) |
| Mean ± SD | 1.42 ± 1.90 |
| Median (Q1–Q3) | 0.90 (0.45–1.76) |
| Hospitalization frequency, n (%) | 110,221 (83.65) |
| Mean ± SD | 1.36 ± 1.41 |
| Median (Q1–Q3) | 0.89 (0.42–1.78) |
| Length of stay per admission per year | |
| Mean ± SD | 16.85 ± 23.07 |
| Median (Q1–Q3) | 8.60 (3.09–21.06) |
| Outpatient frequency, n (%) | 131,760 (100) |
| Mean ± SD | 34.44 ± 22.29 |
| Median (Q1–Q3) | 29.73 (18.57–45.33) |
| Number of department visits | |
| Mean ± SD | 5.92 ± 2.69 |
| Median (Q1–Q3) | 5.60 (4.04–7.47) |
| Patients with chronic prescriptions, n (%) | 90,418 (68.62) |
| Number of medications for chronic prescriptions | |
| Mean ± SD | 17.22 ± 18.37 |
| Median (IQ25–IQ75) | 10.69 (3.42–25.40) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, Y.-H.; Lai, Y.-C.; Wu, Y.-C.; Sasaki, J.; Tsai, K.-T.; Ho, C.-H. Healthcare Utilization in Different Stages among Patients with Dementia: A Nationwide Population-Based Study. Int. J. Environ. Res. Public Health 2021, 18, 5705. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115705
Chen Y-H, Lai Y-C, Wu Y-C, Sasaki J, Tsai K-T, Ho C-H. Healthcare Utilization in Different Stages among Patients with Dementia: A Nationwide Population-Based Study. International Journal of Environmental Research and Public Health. 2021; 18(11):5705. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115705
Chicago/Turabian StyleChen, Yu-Han, Yi-Chen Lai, Yu-Cih Wu, Jun Sasaki, Kang-Ting Tsai, and Chung-Han Ho. 2021. "Healthcare Utilization in Different Stages among Patients with Dementia: A Nationwide Population-Based Study" International Journal of Environmental Research and Public Health 18, no. 11: 5705. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115705