
Prospective Study on Factors Associated with Referral of Patients with Opioid Maintenance Therapy from Specialized Addictive Disorders Centers to Primary Care

Abstract
:1. Introduction
2. Materials and Methods
2.1. Aim and Design and Setting of the Study
2.1.1. Aim
2.1.2. Design
2.1.3. Setting
2.2. Characteristics of Participants and Materials
2.2.1. Participants
2.2.2. Data Collected
2.2.3. Sociodemographic and Medical Data
2.2.4. The TMSP
2.2.5. The TEAQV
2.3. Outcomes
2.4. Statistical Analysis
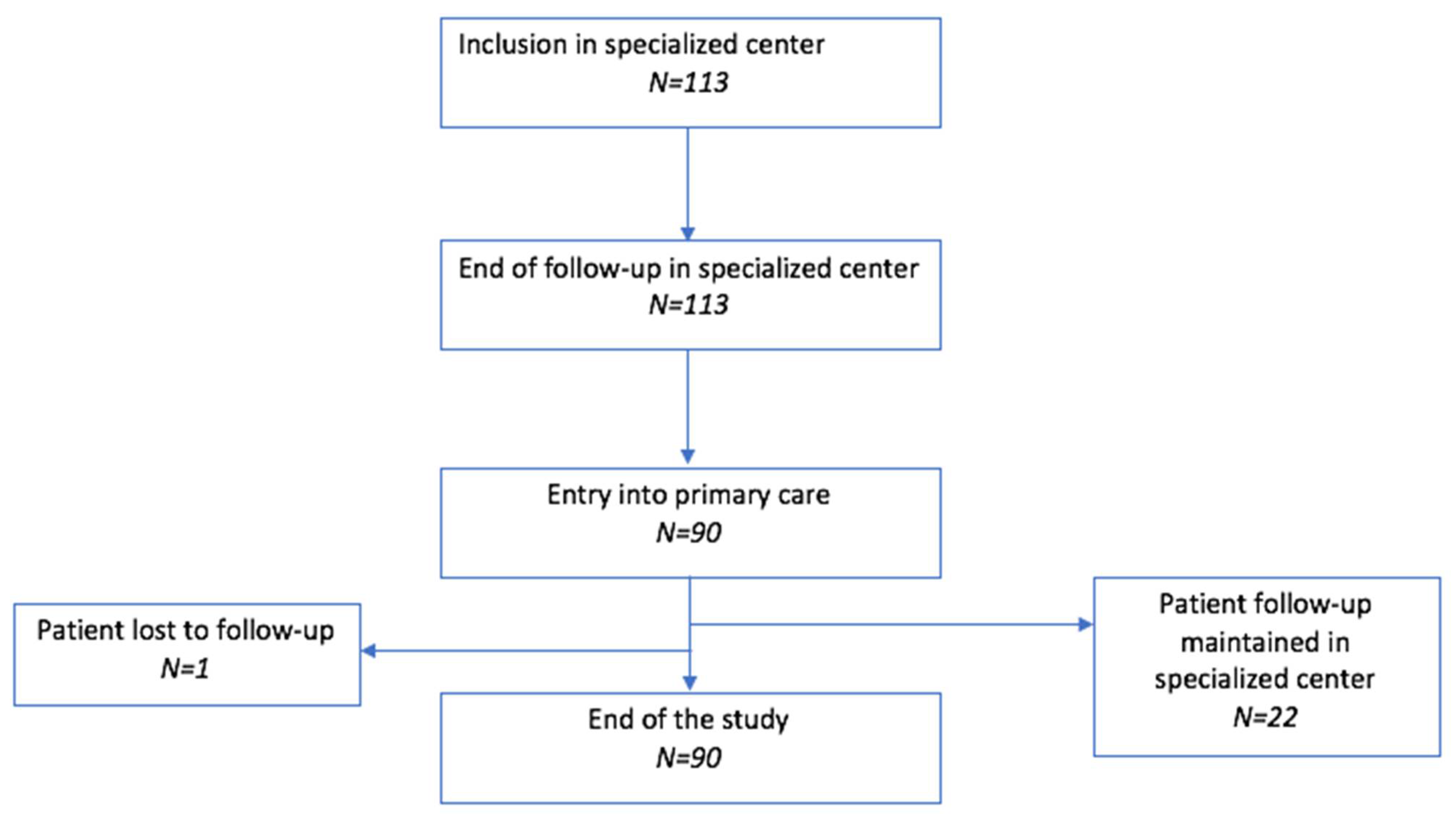
3. Results
3.1. Characteristics of the Patients
3.2. Primary Outcome
3.2.1. Whole Sample of Patients, Whether Referred or Not to Primary Care
3.2.2. Restricted to Patients Who Were Referred to Primary Care
3.3. Secondary Outcomes
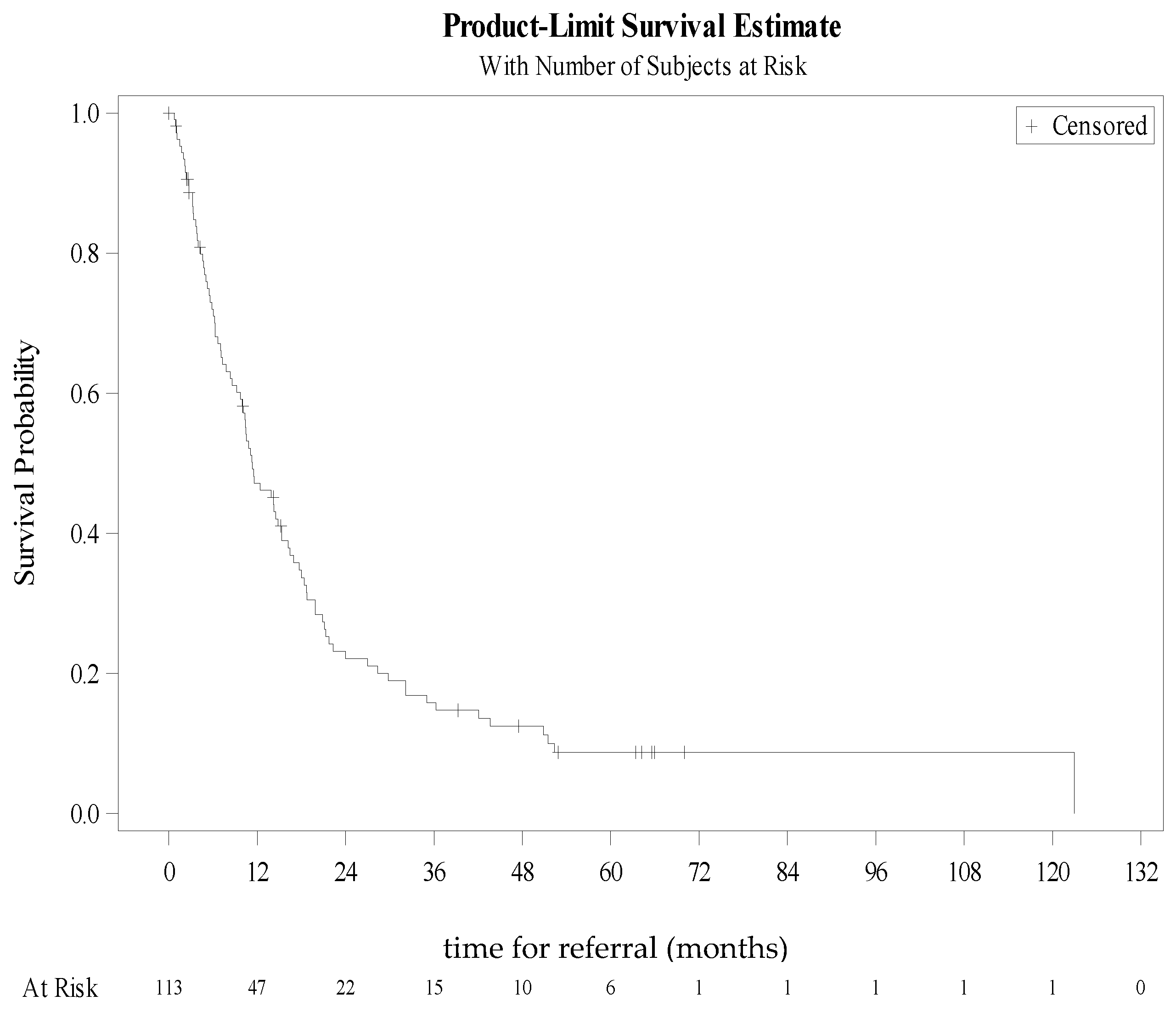
3.3.1. Time to Referral to General Practice
3.3.2. Patient Characteristics Associated with Primary Care Referral
3.4. Changes in Quality of Life (QoL)
3.4.1. Whole Sample of Patients, Whether Referred or Not to Primary Care
3.4.2. Restricted to Patients Who Were Referred to Primary Care
4. Discussion
4.1. Implications
4.2. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
The TMSP (Lowenstein & Gourarier)
- The first dimension concerns substance use “T “(type of substance, route of administration of the substance, number of substances consumed, and environment with or without substance use).
- 1 POINT: a single substance use by nasal route; little or no use of benzodiazepines, amphetamines/barbiturates or cocaine; no alcoholism; non-addicted partner; no drug dealing or addiction-related delinquency.
- 2 POINTS: intravenous heroin addiction or poly-drug addiction (chronic drug intoxication; moderate alcohol use disorder; frequent use of cocaine, crack or amphetamines) or drug-addicted or heroin-addicted partner > 10 years or dealing or delinquency fostered by addiction.
- 5 POINTS: polydrug addiction by the intravenous route with major de-socialisation, history or current risk of major medical complications (overdose, infections, road accidents and major trauma) or repeated legal complications (incarceration); or associated severe alcohol use disorder.
- The second dimension concerns the medical score “M” (medical follow-up, compliance with treatment).
- 1 POINT: regular medical follow-up and compliance with prescribed treatments
- 2 POINTS: irregular medical follow-up and difficulties in treatment compliance.
- 5 POINTS: no medical follow-up (no knowledge of serological status; no vaccinations to date; no prophylactic treatment etc.)
- The third dimension concerns the social score “S” (social, workplace and familial situation).
- 1 POINT: social, professional and family situation not worrying or satisfactory
- 2 POINTS: social problems (no personal accommodation; papers not up to date-Social Security health insurance, 100% reimbursement status, RMI (minimum living allowance), residence permit, etc., pending lawsuits or convictions not followed up; no personal and legal resources or major debts) or family problems (loss of contact with parents and/or children)-
- POINTS: daily drifting (homeless or squatting) with complete marginalisation and situation of abandonment, and major legal risks.
- The fourth dimension concerns the psychiatric score “P” (psychiatric disorders).
- 1 POINT: no significant personality disorder
- 2 POINTS: moderate or controlled personality disorders, not decompensated (no history of suicide attempt, acting out or violence—in the last 6 months).
- 5 POINTS: significant personality disorders (history of suicide attempt, violent acts or repeated psychiatric hospitalizations) requiring specialist care.
- Stage A (the least severe)—Total score < 8 (4, 5, 6 and 7 points = no item scored 5 in any of the diagnostic dimensions).
- Stage B (severe)—Total score between 8 and 11 (8, 9, 10 and 11 points = one item scored 5 in one dimension or, for a total score of 8, 4 items rated 2).
- Stage C (very severe)—Total score between 12 and 16 (12, 13 or 14 points = 2 items scored 5 in the diagnostic dimensions.
- Stage D (extremely severe)—Total score 16 or more (16, 17 or 20 points = three or four items scored 5 in the diagnostic dimensions).
References
- Degenhardt, L.; Whiteford, H.A.; Ferrari, A.J.; Baxter, A.J.; Charlson, F.J.; Hall, W.D.; Freedman, G.; Burstein, R.; Johns, N.; Engell, R.E. Global burden of disease attributable to illicit drug use and dependence: Findings from the Global Burden of Disease Study 2010. Lancet 2013, 382, 1564–1574. [Google Scholar] [CrossRef]
- Guillou, L.M.; Victorri-Vigneau, C.; Grall-Bronnec, M.; Sebille-Rivain, V.; Venisse, J.L.; Jolliet, P. Impact des politiques de santé publique sur les consultations en addictologie à partir d’un suivi longitudinal de 1998 à 2007. Ann. Med. Psychiatry 2013, 171, 367–371. [Google Scholar]
- Guillou, L.M.; Rozaire, C.; Guillet, J.Y.; Victorri, V.C.; Le Reste, J.Y.; Grall, B.M. French Experience with Buprenorphine: Do Physicians Follow the Guidelines? PLoS ONE 2015, 10, e0137708. [Google Scholar]
- Soyka, M.; Kranzler, H.R.; van den Brink, W.; Krystal, J.; Moller, H.J.; Kasper, S. WFSBP Task Force on Treatment, Guidelines for Substance Use Disorders. The World Federation of Societies of Biological Psychiatry (WFSBP) guidelines for the biological treatment of substance use and related disorders. Part 2: Opioid dependence. World J. Biol. Psychiatry 2011, 12, 160–187. [Google Scholar] [CrossRef] [PubMed]
- Wisniewski, A.M.; Dlugosz, M.R.; Blondell, R.D. Reimbursement and practice policies among providers of buprenorphine-naloxone treatment. Subst. Abus. 2013, 34, 105–107. [Google Scholar] [CrossRef]
- ANAES. Stratégies thérapeutiques pour les personnes dépendantes des opiacés: Place des traitements de substitution. Presse Méd. 2004, 33, 41–47. [Google Scholar] [CrossRef]
- Drugs ACotMo. How Can Opioid Substitution Therapy Be Optimised to Maximise Recovery Outcomes for Service Users? 2019. Available online: https://www.gov.uk/government/publications/how-can-opioid-substitution-therapy-be-optimised-to-maximise-recovery-outcomes-for-service-users (accessed on 10 December 2020).
- Comer, S.; Cunningham, C.; Fishman, M.; Gordon, A.; Kampman, K.; Langleben, D.; Nordstromb, B.; Oslin, D.; Woody, G.; Wright, T.; et al. National Practice Guideline for the Use of Medications in the Treatment of Addiction Involving Opioid Use; American Society of Addiction Medicine: Chevi Chase, MA, USA, 2015. [Google Scholar]
- Dematteis, M.; Auriacombe, M.; D’Agnone, O.; Somaini, L.; Szerman, N.; Littlewood, R.; Alam, F.; Alho, H.; Benyamina, A.; Bobes, J.; et al. Recommendations for buprenorphine and methadone therapy in opioid use disorder: A European consensus. Expert Opin. Pharmacother. 2017, 18, 1987–1999. [Google Scholar] [CrossRef]
- O’Connor, A.M.; Cousins, G.; Durand, L.; Barry, J.; Boland, F. Retention of patients in opioid substitution treatment: A systematic review. PLoS ONE 2020, 15, e0232086. [Google Scholar] [CrossRef]
- Sordo, L.; Barrio, G.; Bravo, M.J.; Indave, B.I.; Degenhardt, L.; Wiessing, L.; Ferri, M.; Pastor-Barrusio, R. Mortality risk during and after opioid substitution treatment: Systematic review and meta-analysis of cohort studies. BMJ 2017, 357, 1550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- OEDT. European Report on Drugs 2018: Trends and Evolutions Luxembourg; Luxembourg Publications Office of the European Union: Luxembourg, 2018. [Google Scholar]
- CBHSQ. Quality CfBHSa. Key Substance Use and Mental Health Indicators in the United States: Resukts from the 2015 National Survey on Drug Use and Health 2016. Available online: https://www.samhsa.gov/data/sites/default/les/NSDUH-FFR1–2015/NSDUH-FFR1–2015/NSDUH-FFR1–2015.pdf (accessed on 20 October 2020).
- Saitz, R.; Daaleman, T.P. Now is the Time to Address Substance Use Disorders in Primary Care. Ann. Fam. Med. 2017, 15, 306–308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lapeyre-Mestre, M.; Llau, M.E.; Gony, M.; Navel, A.M.; Bez, J.; Grau, M.; Montastruc, J.L. Opiate maintenance with buprenorphine in ambulatory care: A 24-week follow-up study of new users. Drug Alcohol Depend. 2003, 72, 297–303. [Google Scholar] [CrossRef]
- Fatseas, M.; Auriacombe, M. Why buprenorphine is so successful in treating opiate addiction in France. Curr. Psychiatry Rep. 2007, 9, 358–364. [Google Scholar] [CrossRef] [PubMed]
- Auriacombe, M.; Fatseas, M.; Dubernet, J.; Daulouede, J.P.; Tignol, J. French field experience with buprenorphine. Am. J. Addict. 2004, 13 (Suppl. S1), S17–S28. [Google Scholar] [CrossRef]
- Addiction. Emcfdad. European Drug Report 2019: Trends and Developments; Luxembourg Publications Office of the European Union: Luxembourg, 2019. [Google Scholar]
- Feroni, I.; Aubisson, S.; Bouhnik, A.D.; Paraponaris, A.; Masut, A.; Coudert, C.; Obadia, Y. Collaboration between general practitioners and pharmacists in the management of patients on high-dosage buprenorphine treatment. Prescribers practices. Presse Med. 2005, 34, 1213–1219. [Google Scholar] [CrossRef]
- LaBelle, C.T.; Han, S.C.; Bergeron, A.; Samet, J.H. Office-Based Opioid Treatment with Buprenorphine (OBOT-B): Statewide Implementation of the Massachusetts Collaborative Care Model in Community Health Centers. J. Subst. Abuse Treat. 2016, 60, 6–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dupouy, J.; Maumus-Robert, S.; Mansiaux, Y.; Pariente, A.; Lapeyre-Mestre, M. Primary Care of Opioid use Disorder: The End of the French Model? Eur. Addict. Res. 2020, 26, 346–354. [Google Scholar] [CrossRef]
- Guillou, L.M.; Sebille-Rivain, V.; Victorri, V.C.; Foucher, Y.; Venisse, J.L.; Jolliet, P. Buprenorphine prescription compliance: An original observational and longitudinal study. J. Psychoact. Drugs. 2014, 46, 162–167. [Google Scholar] [CrossRef]
- Eastwood, B.; Strang, J.; Marsden, J. Continuous opioid substitution treatment over five years: Heroin use trajectories and outcomes. Drug Alcohol Depend. 2018, 188, 200–208. [Google Scholar] [CrossRef] [Green Version]
- Dayal, P.; Balhara, Y.P.S. A naturalistic study of predictors of retention in treatment among emerging adults entering first buprenorphine maintenance treatment for opioid use disorders. J. Subst. Abuse Treat. 2017, 80, 1–5. [Google Scholar] [CrossRef]
- Weinstein, Z.M.; Kim, H.W.; Cheng, D.M.; Quinn, E.; Hui, D.; Labelle, C.T.; Drainoni, M.L.; Bachman, S.; Samet, J.H. Long-term retention in Office Based Opioid Treatment with buprenorphine. J. Subst. Abuse Treat. 2017, 74, 65–70. [Google Scholar] [CrossRef] [Green Version]
- Hui, D.; Weinstein, Z.M.; Cheng, D.M.; Quinn, E.; Kim, H.; Labelle, C.; Samet, J.H. Very early disengagement and subsequent re-engagement in primary care Office Based Opioid Treatment (OBOT) with buprenorphine. J. Subst. Abuse Treat. 2017, 79, 9–12. [Google Scholar] [CrossRef]
- Loxterkamp, D. Medication-Assisted Treatment Should Be Part of Every Family Physician’s Practice: Yes. Ann. Fam. Med. 2017, 15, 309–310. [Google Scholar] [CrossRef] [Green Version]
- DeFlavio, J.R.; Rolin, S.A.; Nordstrom, B.R.; Kazal, L.A., Jr. Analysis of barriers to adoption of buprenorphine maintenance therapy by family physicians. Rural Remote Health. 2015, 15, 3019. [Google Scholar]
- Décret no2007–877 du 14 Mai 2007 Relatif aux Missions des Centres de Soins, d’Accompagnement et de Prévention en Addictologie; JORF (112); République Française: Paris, France, 2007.
- Lowenstein, W.; Gourarier, L.; Cottel, A.; Lebeau, B.; Hefez, S. La Méthadone et Les Traitements de Substitution; Doin: Paris, France, 1996. [Google Scholar]
- Grabot, D.; Martin, C.; Auriacombe, M.; Tignol, J. Tableau d’évaluation assitée de la qualité de vie (TEAQV). L’Encéphale 1996, 22, 181–186. [Google Scholar]
- Strada, L.; Vanderplascheen, W.; Buchholz, A.; Schulte, B.; Muller, A.E.; Verthein, U. Measuring quality of life in opioid-dependent people: A systematic review of assessment instruments. Qual. Life Res. 2017, 26, 3187–3200. [Google Scholar] [CrossRef] [Green Version]
- Pan, W. Akaike’s information criterion in generalized estimating equations. Biometrics 2001, 57, 120–125. [Google Scholar] [CrossRef] [PubMed]
- Teoh, B.F.J.; Yee, A.; Habil, M.H.; Danaee, M. Effectiveness of Methadone Maintenance Therapy and Improvement in Quality of Life Following a Decade of Implementation. J. Subst. Abuse Treat. 2016, 69, 50–56. [Google Scholar] [CrossRef] [PubMed]
- Ling, W.; Charuvastra, C.; Collins, J.F.; Batki, S.; Brown, L.S., Jr.; Kintaudi, P.; Wesson, D.R.; McNicholas, L.; Tusel, D.J.; Malkerneker, U. Buprenorphine maintenance treatment of opiate dependence: A multicenter, randomized clinical trial. Addiction 1998, 93, 475–486. [Google Scholar] [CrossRef]
- Amato, L.; Davoli, M.; Ferri, M.; Gowing, L.; Perucci, C.A. Effectiveness of interventions on opiate withdrawal treatment: An overview of systematic reviews. Drug Alcohol Depend. 2004, 73, 219–226. [Google Scholar] [CrossRef] [PubMed]
- Barnett, P.G.; Rodgers, J.H.; Bloch, D.A. A meta-analysis comparing buprenorphine to methadone for treatment of opiate dependence. Addiction 2001, 96, 683–690. [Google Scholar] [CrossRef]
- Dugosh, K.; Abraham, A.; Seymour, B.; McLoyd, K.; Chalk, M.; Festinger, D. A Systematic Review on the Use of Psychosocial Interventions in Conjunction with Medications for the Treatment of Opioid Addiction. J. Addict. Med. 2016, 10, 93–103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- OFDT. Drogues et Addictions, Données Essentielles; OFDT: Paris, France, 2019. [Google Scholar]
- Koehl, J.L.; Zimmerman, D.E.; Bridgeman, P.J. Medications for management of opioid use disorder. Am. J. Health Syst. Pharm. 2019, 76, 1097–1103. [Google Scholar] [CrossRef] [PubMed]
- Rich, K.M.; Bia, J.; Altice, F.L.; Feinberg, J. Integrated Models of Care for Individuals with Opioid Use Disorder: How Do We Prevent HIV and HCV? Curr. HIV/AIDS Rep. 2018, 15, 266–275. [Google Scholar] [CrossRef] [Green Version]
- Cao, X.B.; Wu, Z.Y.; Rou, K.M.; Pang, L.; Luo, W.; Wang, C.H.; Li, J.H. National Methadone maintenance Treatmetn Working Group [Characteristics and associated factors of long-term retention for methadone maintenance treatment patients]. Zhonghua Yu Fang Yi Xue Za Zhi 2012, 46, 995–998. [Google Scholar] [PubMed]
- Feng, N.; Lin, C.; Hsieh, J.; Rou, K.; Li, L. Family Related Factors and Concurrent Heroin Use in Methadone Maintenance Treatment in China. Subst. Use Misuse 2018, 53, 1674–1680. [Google Scholar] [CrossRef]
- Wittchen, H.U.; Apelt, S.M.; Soyka, M.; Gastpar, M.; Backmund, M.; Golz, J.; Kraus, M.R.; Tretter, F.; Schäfer, M.; Siegert, J.; et al. Feasibility and outcome of substitution treatment of heroin-dependent patients in specialized substitution centers and primary care facilities in Germany: A naturalistic study in 2694 patients. Drug Alcohol Depend. 2008, 95, 245–257. [Google Scholar] [CrossRef] [Green Version]
- Moran, L.; Keenan, E.; Elmusharaf, K. Barriers to progressing through a methadone maintenance treatment programme: Perspectives of the clients in the Mid-West of Ireland’s drug and alcohol services. BMC Health Serv. Res. 2018, 18, 911. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, R.P.; Kelly, S.M.; O’Grady, K.E.; Mitchell, S.G.; Peterson, J.A.; Reisinger, H.S.; Agar, M.H.; Brown, B.S. Attitudes toward buprenorphine and methadone among opioid-dependent individuals. Am. J. Addict. 2008, 17, 396–401. [Google Scholar] [CrossRef]
- Aletraris, L.; Edmond, M.B.; Paino, M.; Fields, D.; Roman, P.M. Counselor training and attitudes toward pharmacotherapies for opioid use disorder. Subst. Abus. 2016, 37, 47–53. [Google Scholar] [CrossRef] [Green Version]
- Carrieri, P.M.; Michel, L.; Lions, C.; Cohen, J.; Vray, M.; Mora, M.; Marcellin, F.; Spire, B.; Morel, A.; Roux, P.; et al. Methadone induction in primary care for opioid dependence: A pragmatic randomized trial (ANRS Methaville). PLoS ONE 2014, 9, e112328. [Google Scholar] [CrossRef] [Green Version]
- Korownyk, C.; Perry, D.; Ton, J.; Kolber, M.R.; Garrison, S.; Thomas, B.; Allan, G.M.; Bateman, C.; De Queiroz, R.; Kennedy, D.; et al. Managing opioid use disorder in primary care: PEER simplified guideline. Can. Fam. Physician 2019, 65, 321–330. [Google Scholar] [PubMed]
- Guan, Q.; Khuu, W.; Spithoff, S.; Kiran, T.; Kahan, M.; Tadrous, M.; Martins, D.; Leece, P.; Gomes, T. Patterns of physician prescribing for opioid maintenance treatment in Ontario, Canada in 2014. Drug Alcohol Depend. 2017, 177, 315–321. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | n = 113 | % |
|---|---|---|
| Sociodemographic Variables | ||
| Age, years, mean (SD) | 28.6 (6.2) | |
| Gender, Male | 85 | 75.2 |
| With social support | 111 | 98.23 |
| Living with a partner | 48 | 42.48 |
| Children | 38 | 33.63 |
| Drug users among persons around | 95 | 84.07 |
| Drug users among spouses | 20 | 17.70 |
| Drug users among friends | 92 | 81.42 |
| Stable housing | 86 | 76.11 |
| Professional activity | 66 | 58.41 |
| Regular income | 68 | 60.18 |
| Comorbidities | ||
| Psychiatric comorbidities | 47 | 41.59 |
| Medical comorbidities | 9 | 7.96 |
| Knowledge of serological status | 55 | 48.67 |
| HIV + | 1 | 0.88 |
| HCV+ | 5 | 4.42 |
| Patients not taking precautions to reduce risks of virus transmission | 36 | 31.86 |
| Damage associated with Opioid Use disorders | ||
| Familial damage | 43 | 38.05 |
| Professional damage | 53 | 46.90 |
| Medical damage | 26 | 23.01 |
| Legal damage | 29 | 25.66 |
| Variables | At Inclusion in the Specialized Center n = 113 % (n) | Last Visit in the Specialized Center n = 113 % (n) | First Visit in Primary Care n = 90 % (n) | Last Visit in Primary Care n = 90 % (n) |
|---|---|---|---|---|
| TMSP Scale | ||||
| S- Socio-personal axis | ||||
| Satisfactory social, professional, familial situation | 49.6 (56) | 65.5 (74) | 83.3 (75) | 77.8 (70) |
| Social or family problem | 40.7 (46) | 30.1 (34) | 16.7 (15) | 14.4 (13) |
| Daily drifting and major legal risks | 9.7 (11) | 3.5 (4) | 0.0 (0) | 1.1 (1) |
| Missing data | 0.0 (0) | 0.9 (1) | 0.0 (0) | 6.7 (6) |
| M- Medical follow-up axis | ||||
| Regular follow-up and treatment compliance | 49.6 (56) | 82.3 (93) | 95.6 (86) | 86.7 (78) |
| Irregular follow-up and treatment compliance issues | 44.3 (50) | 15.0 (17) | 3.3 (3) | 4.4 (4) |
| No follow-up | 6.2 (7) | 1.8 (2) | 1.1 (1) | 1.1 (1) |
| Missing data | 0.0 (0) | 0.9 (1) | 0.0 (0) | 7.8 (7) |
| P- Psychiatric approach axis | ||||
| No significant personality disorder | 58.4 (66) | 74.3 (84) | 81.1 (73) | 74.4 (67) |
| Moderate personality disorders | 32.7 (37) | 18.6 (21) | 18.9 (17) | 15.6 (14) |
| Major personality disorders requiring specialized environment support | 8.9 (10) | 6.2 (7) | 0.0 (0) | 2.2 (2) |
| Missing data | 0.0 (0) | 0.9 (1) | 0.0 (0) | 7.8 (7) |
| T- Substance addiction axis | ||||
| 1 point | 49.6 (56) | 85.8 (97) | 95.6 (86) | 76.7 (69) |
| 2 points | 44.3 (50) | 10.6 (12) | 4.4 (4) | 11.1 (10) |
| 5 points | 6.2 (7) | 2.7 (3) | 0.0 (0) | 4.4 (4) |
| Missing data | 0.0 (0) | 0.9 (1) | 0.0 (0) | 7.8 (7) |
| Stages of severity | ||||
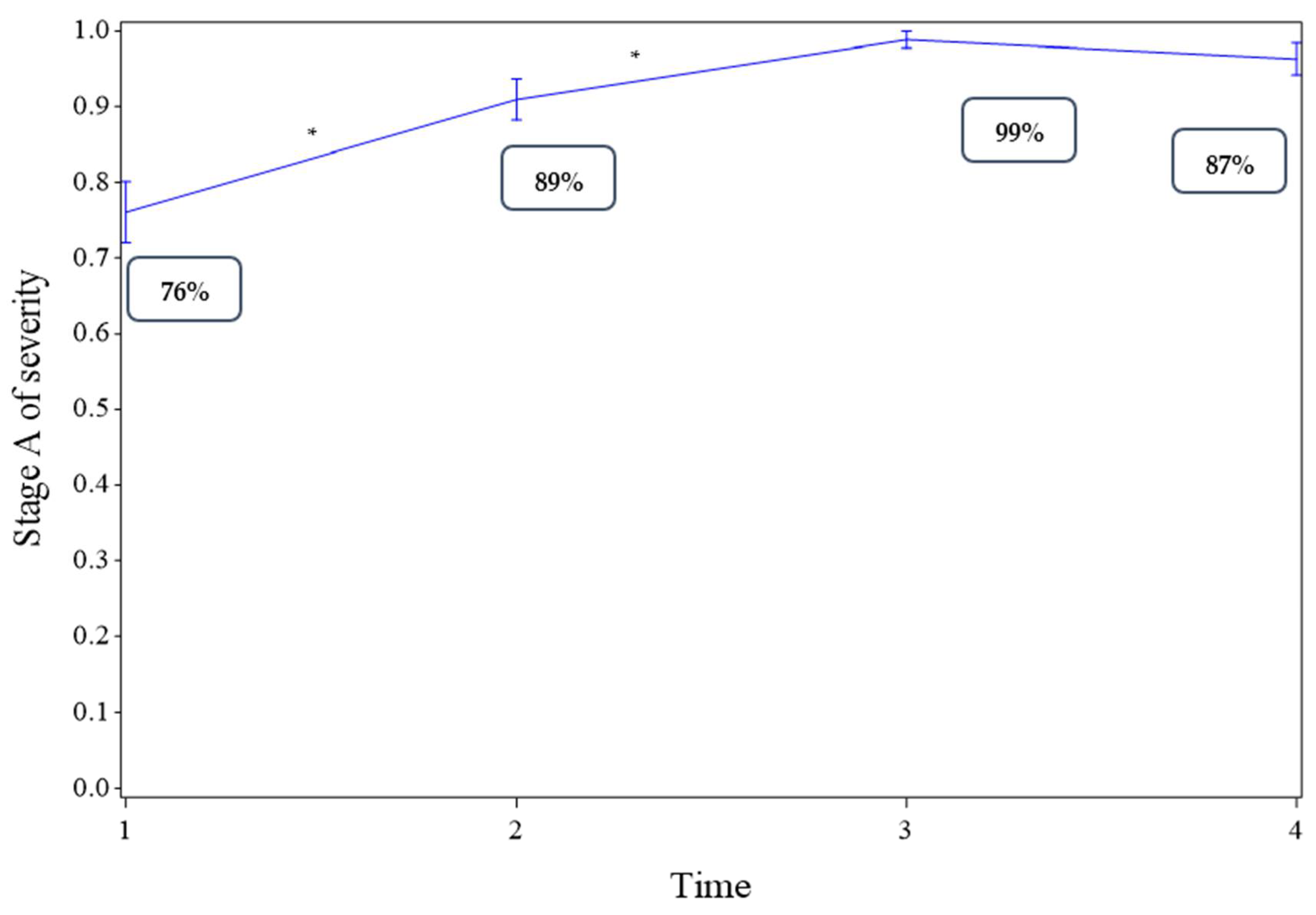
| Stage A | 76.1 (86) | 89.4 (101) | 98.9 (89) | 86.7 (78) |
| Stage B | 15.0 (17) | 4.4 (5) | 1.1 (1) | 1.1 (1) |
| Stage C | 6.2 (7) | 3.5 (4) | 0.0 (0) | 1.1 (1) |
| Stage D | 2.7 (3) | 0.9 (1) | 0.0 (0) | 1.1 (1) |
| Missing data | 0.0 (0) | 1.8 (2) | 0.0 (0) | 10.0 (9) |
| TEAQV Scale | ||||
| Physical condition | ||||
| Extremely bad | 1.8 (2) | 1.8 (2) | 1.1 (1) | 1.1 (1) |
| Very bad | 10.6 (12) | 1.8 (2) | 1.1 (1) | 0.0 (0) |
| Quite bad | 28.3 (32) | 6.2 (7) | 1.1 (1) | 4.4 (4) |
| Medium | 31.9 (36) | 9.7 (11) | 11.1 (10) | 11.1 (10) |
| Quite good | 20.4 (23) | 36.3 (41) | 31.1 (28) | 34.4 (31) |
| Very good | 6.2 (7) | 38.1 (43) | 43.3 (39) | 34.4 (31) |
| Excellent | 0.9 (1) | 6.2 (7) | 11.1 (10) | 14.4 (13) |
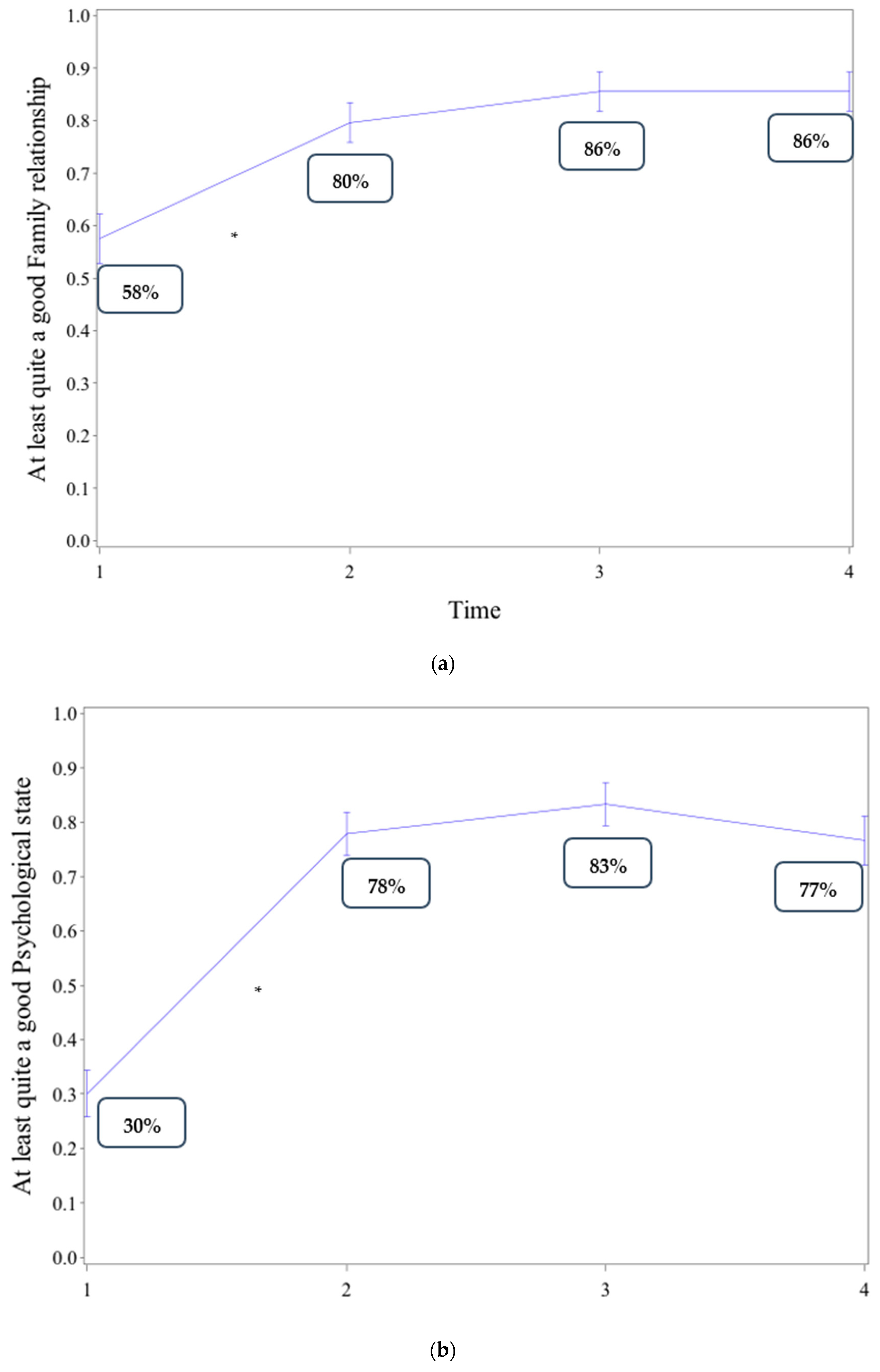
| Psychological state | ||||
| Extremely bad | 4.4 (5) | 0.9 (1) | 1.1 (1) | 1.1 (1) |
| Very bad | 14.2 (16) | 3.5 (4) | 0.0 (0) | 0.0 (0) |
| Quite bad | 23.9 (27) | 7.1 (8) | 1.1 (1) | 7.8 (7) |
| Medium | 27.4 (31) | 10.6 (12) | 14.4 (13) | 14.4 (13) |
| Quite good | 22.1 (25) | 33.6 (38) | 35.6 (32) | 38.9 (35) |
| Very good | 7.1 (8) | 39.8 (45) | 40.0 (36) | 28.9 (26) |
| Excellent | 0.9 (1) | 4.4 (5) | 7.8 (7) | 8.9 (8) |
| Socio-professional integration | ||||
| Extremely bad | 11.5 (13) | 3.5 (4) | 2.2 (2) | 3.3 (3) |
| Very bad | 3.5 (4) | 5.3 (6) | 5.6 (5) | 6.7 (6) |
| Quite bad | 16.8 (19) | 9.7 (11) | 3.3 (3) | 12.2 (11) |
| Medium | 24.8 (28) | 16.8 (19) | 21.1 (19) | 11.1 (10) |
| Quite good | 23.9 (27) | 25.7 (29) | 11.1 (10) | 16.7 (15) |
| Very good | 15.0 (17) | 28.3 (32) | 28.9 (26) | 37.8 (34) |
| Excellent | 4.4 (5) | 10.6 (12) | 27.8 (25) | 12.2 (11) |
| Family relationships | ||||
| Extremely bad | 8.9 (10) | 4.4 (5) | 1.1 (1) | 2.2 (2) |
| Very bad | 4.4 (5) | 0.0 (0) | 1.1 (1) | 1.1 (1) |
| Quite bad | 10.6 (12) | 2.7 (3) | 1.1 (1) | 1.1 (1) |
| Medium | 18.6 (21) | 13.3 (15) | 11.1 (10) | 10.0 (9) |
| Quite good | 17.7(20) | 22.1 (25) | 17.8 (16) | 17.8 (16) |
| Very good | 31.0 (35) | 42.5 (48) | 42.2 (38) | 46.7 (42) |
| Excellent | 8.9 (10) | 15.0 (17) | 25.6 (23) | 21.1 (19) |
| Variables Associated with Time to Referral to PCPs | |||
|---|---|---|---|
| Variable | Hazard Ratio | CI 95% | p-Value |
| Having a partner, yes vs. no | 1.755 | [1.103–2.790] | 0.018 |
| Having children, yes vs. no | 1.836 | [1.164–2.895] | 0.009 |
| Stage of severity A vs. B, C, or D | 2.412 | [1.284–4.528] | 0.006 |
| Knowledge of serological status, yes vs. no | 0.601 | [0.392–0.922] | 0.020 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guillou-Landreat, M.; Levassor, P.; Guerlais, M.; Sebille, V.; Victorri-Vigneau, C. Prospective Study on Factors Associated with Referral of Patients with Opioid Maintenance Therapy from Specialized Addictive Disorders Centers to Primary Care. Int. J. Environ. Res. Public Health 2021, 18, 5749. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115749
Guillou-Landreat M, Levassor P, Guerlais M, Sebille V, Victorri-Vigneau C. Prospective Study on Factors Associated with Referral of Patients with Opioid Maintenance Therapy from Specialized Addictive Disorders Centers to Primary Care. International Journal of Environmental Research and Public Health. 2021; 18(11):5749. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115749
Chicago/Turabian StyleGuillou-Landreat, Morgane, Philippe Levassor, Marylène Guerlais, Veronique Sebille, and Caroline Victorri-Vigneau. 2021. "Prospective Study on Factors Associated with Referral of Patients with Opioid Maintenance Therapy from Specialized Addictive Disorders Centers to Primary Care" International Journal of Environmental Research and Public Health 18, no. 11: 5749. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115749