
Process Evaluation of the SImplification of Medications Prescribed to Long-tErm Care Residents (SIMPLER) Cluster Randomized Controlled Trial: A Mixed Methods Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Document Analysis
2.3. Semi-Structured Interviews
2.4. Qualitative Data Analysis
2.5. Quantiative Data Analysis
3. Results
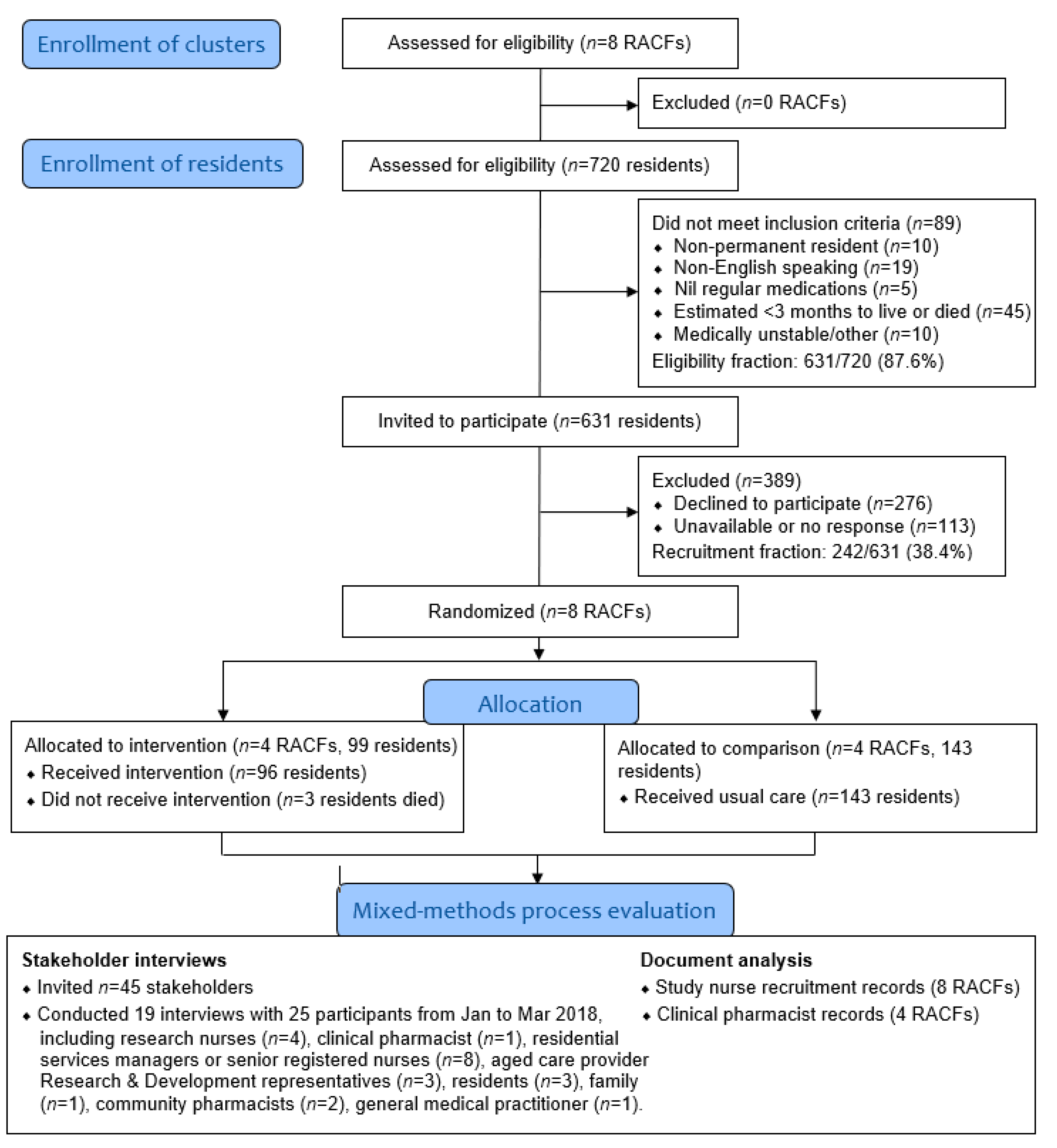
3.1. Recruitment of RACFs (Clusters)
“There was no reason not to jump on board… it made perfect sense. And we’d also get feedback from the staff, you know, that they’re very busy so anything that might reduce or improve the workflow for them was of interest.”[Residential Services Manager 1]
3.2. Recruitment and Reach among Residents
- Regular face-to-face meetings with senior research and development staff within the aged care provider organization, senior staff at each facility and the organization’s Client Safety Quality Unit
- Researcher embedded within the residential aged care provider organization (2 days per week) regularly liaised with senior staff at the RACFs
- Participation in face-to-face RACF medication advisory committee meetings, senior nursing handover meetings, RACF staff meetings, Resident meetings, and Consumer and Carer Reference Group meetings
- In one RACF, the research team delivered a medication-related continuing education session to RACF staff that was followed by SIMPLER study promotional information
- Posters in staff meeting rooms and in public areas of the RACF, written information in emails and newsletters to staff, residents, and family members
- Written letters, flyers, emails and/or telephone calls to family members, local community pharmacies and GPs
“Give back for the future and for other residents… if you want better conditions for yourself, you surely want them for other people too.”[Resident 1]
“I think my main thought there is how it’s going to benefit all of us.”[Resident 3]
- The resident, or the family, are not interested in participating in the study (n = 19)
- The resident is too confused or distressed, or the third-party does not wish to confuse, distress or both the resident (n = 13)
- The study or intervention is perceived as unnecessary, inappropriate, or would not benefit the resident (i.e., because the resident does not take many medications) (n = 12)
- The resident has been unwell recently (n = 8)
- The resident, or the third-party, are busy or lack time needed for involvement (n = 8)
- The resident has recently had their medications checked, or changed, whereby they do not want any further changes (n = 5)
- It is perceived that the resident would not be able to participate in the study, or would not be a beneficial participant (n = 4)
3.2.1. Communication and Promotion
“We were seeing that we were getting greater acceptance of the project through contact face to face than what we were over the phone.”[Research Nurse 1]
“It was only when we were first on the phone contacting the next of kin that we found that barrier was there. Not when I was actually on site talking to them.”[Research Nurse 3]
3.2.2. Relationships and Trust
“They [the residents] felt that they didn’t want to offend their GP by having somebody else look at things that the GP was already in control of.”[Research Nurse 1]
“It’s almost like not wanting to offend the doctor or just trusting that the doctor’s got it all right.”[Research Nurse 3]
“I think it was easier being introduced by a care worker or nursing staff when you go in the room. I know it sounds a bit silly but it’s almost like you’re not intruding… But we couldn’t always do that because the staff were busy.”[Research Nurse 3]
3.2.3. Resistance to Change the Current Medication Regimen
“…some people have been, you know, taking their tablets in a certain way for a long time prior to them coming into residential care and…they don’t like change and they’re very reluctant and concerned that it’s going to affect their health… Or they’ve had previous bad experiences of changing medications.”[Registered Nurse 4]
“They had that thought that their medication was going to be changed to something different than what they were already taking, so there was a bit of explaining… that it wasn’t actually going to change what they were taking.”[Recruitment Assistant 1]
3.3. Delivery to RACFs and Individual Residents
“There were no issues around it [intervention delivery]. They [the clinical pharmacist] worked around when staff were doing their medication round and yeah it seemed to all go fairly quickly and smoothly, I can remember.”[Senior Registered Nurse 4]
“Talking with residents, well in the project I guess there was, talking with residents, they don’t necessarily understand that you’re just there as a project pharmacist, and they want you to change all sorts of medicines and things and I had to explain no, it was just around the simplification and that they’d need to see their regular pharmacist around other issues.”[Clinical Pharmacist]
3.4. Response of RACFs
“And different sites had different issues. Like one site, they’d already virtually simplified all the times themselves, I think that was the last site that I went to. So, it was really only doctor interventions. Whereas other sites had lots of timing interventions and not many doctor interventions.”[Clinical Pharmacist]
“Yeah, and I think that’s what you’d expect from human nature everywhere, that they’ve got a number of priorities in the facility and so depending on, yeah, what their other competing priorities were, some sites were super keen, other nurses I don’t, they just saw it as an extra workload.”[Clinical Pharmacist]
“And because we had that knowledge and you know we actually had another resident with a similar thing and we said look last time they said, this pharmacist said we could use a slow-release morphine tablet. It was just as effective and so you know we were able to use the knowledge that we got through the study for somebody else.”[Clinical nurse 4]
“I just think that some staff are more positive about research than others, basically. But in saying that I don’t think there was... I think all of the sites, there were some staff at the sites that were very positive about it but there was also some that were not so positive. But they were a minority.”[Research nurse 2]
“It just saves everyone time and doesn’t affect quality of the service, which is important… Definitely less for me to do during lunch run, which used to be busier … And I mean, I don’t spend an extra time in the morning, because if I give one extra, two extra tablets in the morning, that doesn’t make difference in the time I spend with the residents… But yeah, probably it benefits residents because I have more time to be involved in care planning or writing progress notes, which are always good to document…”[Enrolled Nurse 1]
3.5. Response of Residents and Other Individuals
“I think having another set of eyes coming through is good... Because she is, she’s on a hell of a lot of medication and if they’ve reduced the number of times that they’re giving to her, and they’re sort of giving it to her in one go, at least it’s not as disruptive.”[Resident family representative 1]
“I guess I probably don’t pay too much attention to the times the medications are given and maybe I should do that more. But yeah, I mean, because I think the two that I got, it was just like, oh yeah, well that makes sense. You know, let’s do that. I hadn’t really noticed that that was an issue. Yeah, which is probably good. Probably means that there’s good reason to do this sort of thing.”[General Practitioner 1]
“I did get some response back from two of the GPs saying yep, absolutely, really, really happy to support this.”[Research Nurse 1]
“So yeah, it was one of those things that I thought this can only help and benefit everybody.”[Community Pharmacist 2]
3.6. Future Implementation
“So, I think at point of entry would be a really, really good start. And then perhaps at, you know, significant health changes. I mean, could it be done annually and a medication review as well?”[Research Nurse 1]
“I don’t think you have to be automatic process, you know, it’s just on the needs of every [resident], needs are different. So definitely admission, definitely significant health status change, hospitalization. And then probably do some regular ones, but not too often. And then again, a RN or CN can make that call as well, to inform. So that’s one part of getting nurses involved, because they can easily, they can make that call and inform pharmacist.”[Enrolled nurse 1]
“So, if I was, ideally, in an ideal world, if I was able to commit as much time as I like to a facility and could be there all the time, I’d like to do it once a quarter as a routine thing and for all residents that came back from hospital.”[Clinical pharmacist 1]
3.7. Unintended Consequences
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sluggett, J.K.; Chen, E.Y.H.; Ilomäki, J.; Corlis, M.; Hilmer, S.N.; Van Emden, J.; Ooi, C.E.; Nguyen, K.-H.; Comans, T.; Hogan, M.; et al. SImplification of Medications Prescribed to Long-tErm care Residents (SIMPLER): Study protocol for a cluster randomised controlled trial. Trials 2018, 19, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Hamrick, I.; Nye, A.M.; Gardner, C.K. Nursing Home Medication Administration Cost Minimization Analysis. J. Am. Med. Dir. Assoc. 2007, 8, 173–177. [Google Scholar] [CrossRef] [PubMed]
- Sluggett, J.K.; Chen, E.Y.H.; Ilomäki, J.; Corlis, M.; Van Emden, J.; Hogan, M.; Caporale, T.; Keen, C.; Hopkins, R.; Ooi, C.E.; et al. Reducing the Burden of Complex Medication Regimens: SImplification of Medications Prescribed to Long-tErm care Residents (SIMPLER) Cluster Randomized Controlled Trial. J. Am. Med. Dir. Assoc. 2020, 21, 1114–1120.e4. [Google Scholar] [CrossRef] [PubMed]
- Lalic, S.; Sluggett, J.K.; Ilomaki, J.; Wimmer, B.C.; Tan, E.C.; Robson, L.; Emery, T.; Bell, J.S. Polypharmacy and Medication Regimen Complexity as Risk Factors for Hospitalization Among Residents of Long-Term Care Facilities: A Prospective Cohort Study. J. Am. Med. Dir. Assoc. 2016, 17, 1067.e1–1067.e6. [Google Scholar] [CrossRef] [PubMed]
- Wimmer, B.C.; Cross, A.J.; Jokanovic, N.; Wiese, M.D.; George, J.; Johnell, K.; Diug, B.; Bell, J.S. Clinical Outcomes Associated with Medication Regimen Complexity in Older People: A Systematic Review. J. Am. Ger. Soc. 2017, 65, 747–753. [Google Scholar] [CrossRef]
- Sluggett, J.K.; Hopkins, R.; Chen, E.Y.H.; Ilomäki, J.; Corlis, M.; Van Emden, J.; Hogan, M.; Caporale, T.; Ooi, C.E.; Hilmer, S.N.; et al. Impact of medication regimen simplification on medication administration times and health outcomes in residential aged care: 12-month follow-up of the SIMPLER randomized controlled trial. J. Clin. Med. 2020, 9, 1053. [Google Scholar] [CrossRef] [Green Version]
- Dugré, N.; Bell, J.S.; Hopkins, R.E.; Ilomäki, J.; Chen, E.Y.H.; Corlis, M.; Van Emden, J.; Hogan, M.; Sluggett, J.K. Impact of Medication Regimen Simplification on Medication Incidents in Residential Aged Care: SIMPLER Randomized Controlled Trial. J. Clin. Med. 2021, 10, 1104. [Google Scholar] [CrossRef]
- Chen, E.Y.H.; Bell, J.S.; Ilomäki, J.; Keen, C.; Corlis, M.; Van Emden, J.; Hilmer, S.N.; Sluggett, J.K. Medication regimen complexity in 8 Australian residential aged care facilities: Impact of age, length of stay, comorbidity, frailty, and dependence in activities of daily living. Clin. Interv. Aging 2019, 14, 1783–1795. [Google Scholar] [CrossRef] [Green Version]
- Chen, E.Y.H.; Sluggett, J.K.; Ilomäki, J.; Hilmer, S.N.; Corlis, M.; Picton, L.J.; Dean, L.; Alderman, C.P.; Farinola, N.; Gailer, J.; et al. Development and validation of the Medication Regimen Simplification Guide for Residential Aged CarE (MRS GRACE). Clin. Interv. Aging 2018, 13, 975–986. [Google Scholar] [CrossRef] [Green Version]
- Liu, H.; Lindley, R.; Alim, M.; Felix, C.; Gandhi, D.B.C.; Verma, S.J.; Tugnawat, D.K.; Syrigapu, A.; Ramamurthy, R.K.; Pandian, J.D.; et al. Protocol for process evaluation of a randomised controlled trial of family-led rehabilitation post stroke (ATTEND) in India. BMJ Open 2016, 6, e012027. [Google Scholar] [CrossRef] [Green Version]
- Grant, A.; Treweek, S.; Dreischulte, T.; Foy, R.; Guthrie, B. Process evaluations for cluster-randomised trials of complex interventions: A proposed framework for design and reporting. Trials 2013, 14, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lam, H.R.; Chow, S.; Taylor, K.; Chow, R.; Lam, H.; Bonin, K.; Rowbottom, L.; Herrmann, N. Challenges of conducting research in long-term care facilities: A systematic review. BMC Geriatr. 2018, 18, 242. [Google Scholar] [CrossRef] [Green Version]
- Hall, S.; Longhurst, S.; Higginson, I.J. Challenges to conducting research with older people living in nursing homes. BMC Geriatr. 2009, 9, 38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baker, F.A.; Stretton-Smith, P.A.; Sousa, T.V.; Clark, I.; Cotton, A.; Gold, C.; Lee, Y.-E.C. Resource assessment in trials undertaken in residential care homes: Experiences from the Australian MIDDEL cluster randomised controlled trial research team. Contemp. Clin. Trials Commun. 2020, 20, 100675. [Google Scholar] [CrossRef] [PubMed]
- Zermansky, A.G.; Alldred, D.P.; Petty, D.R.; Raynor, D.K. Striving to recruit: The difficulties of conducting clinical research on elderly care home residents. J. R. Soc. Med. 2007, 100, 258–261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sluggett, J.K.; Ilomäki, J.; Seaman, K.L.; Corlis, M.; Bell, J.S. Medication management policy, practice and research in Australian residential aged care: Current and future directions. Pharmacol. Res. 2017, 116, 20–28. [Google Scholar] [CrossRef]
- Anrys, P.; Strauven, G.; Roussel, S.; Vande Ginste, M.; De Lepeleire, J.; Foulon, V.; Spinewine, A. Process evaluation of a complex intervention to optimize quality of prescribing in nursing homes (COME-ON study). Implement. Sci. 2019, 14, 104. [Google Scholar] [CrossRef] [Green Version]
- Klingshirn, H.; Müller, M.; Beutner, K.; Hirt, J.; Strobl, R.; Grill, E.; Meyer, G.; Saal, S. Implementation of a complex intervention to improve participation in older people with joint contractures living in nursing homes: A process evaluation of a cluster-randomised pilot trial. BMC Geriatr. 2020, 20, 270. [Google Scholar] [CrossRef]
- Clyne, B.; Cooper, J.A.; Hughes, C.M.; Fahey, T.; Smith, S.M. A process evaluation of a cluster randomised trial to reduce potentially inappropriate prescribing in older people in primary care (OPTI-SCRIPT study). Trials 2016, 17, 386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grant, A.; Dreischulte, T.; Guthrie, B. Process evaluation of the data-driven quality improvement in primary care (DQIP) trial: Active and less active ingredients of a multi-component complex intervention to reduce high-risk primary care prescribing. Implement. Sci. 2017, 12, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bowen, G.A. Document analysis as a qualitative research method. Qual. Res. J. 2009, 9, 27–40. [Google Scholar] [CrossRef] [Green Version]
- Sluggett, J.K.; Ooi, C.E.; Gibson, S.; Angley, M.T.; Corlis, M.; Hogan, M.; Caporale, T.; Hughes, G.A.; Van Emden, J.; Bell, J.S. Simplifying Medication Regimens for People Receiving Community-Based Home Care Services: Outcomes of a Non-Randomized Pilot and Feasibility Study. Clin. Interv. Aging 2020, 15, 797–809. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Braun, V.; Clarke, V. Thematic Analysis: A Reflexive Approach. Available online: https://www.psych.auckland.ac.nz/en/about/thematic-analysis.html (accessed on 12 April 2021).
- Commonwealth Department of Health and Ageing. The National Strategy for Quality Use of Medicines; Publication Number 3024; Commonwealth of Australia: Canberra, Australia, 2002.
- Australian Institute of Health and Welfare. Aged Care Data Snapshot-2017. Available online: https://www.gen-agedcaredata.gov.au/Resources/Access-data/2018/January/Aged-care-data-snapshot%E2%80%942017 (accessed on 12 April 2021).
- Australian Institute of Health and Welfare. Australia’s Welfare 2017; Australia’s Welfare Services no. 13. AUS 214; AIHW: Canberra, Australia, 2017.
- Hughes, G.A.; Bell, J.S.; Chen, E.Y.H.; Ooi, C.E.; Caporale, T.; Hogan, M.; Corlis, M.; Van Emden, J.; Sluggett, J.K. Would you like to participate? Factors impacting on participant recruitment for quality use of medicines interventions in residential aged care. Res. Soc. Adm. Pharm. 2019, 15, e12. [Google Scholar] [CrossRef]
- Hoyle, D.J.; Peterson, G.M.; Bindoff, I.K.; Clinnick, L.M.; Bindoff, A.D.; Breen, J.L. Clinical impact of antipsychotic and benzodiazepine reduction: Findings from a multicomponent psychotropic reduction program within long-term aged care. Int. Psychogeriatr. 2020, 1–13. [Google Scholar] [CrossRef]
- Beattie, E.; Fielding, E.; O’Reilly, M.; Brooks, D.; MacAndrew, M.; McCrow, J. Recruitment of individuals with dementia and their carers for social research: Lessons learned from nine studies. Res. Gerontol. Nurs. 2018, 11, 119–128. [Google Scholar] [CrossRef]
- Clegg, A.; Relton, C.; Young, J.; Witham, M. Improving recruitment of older people to clinical trials: Use of the cohort multiple randomised controlled trial design. Age Ageing 2015, 44, 547–550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McMurdo, M.E.T.; Roberts, H.; Parker, S.; Wyatt, N.; May, H.; Goodman, C.; Jackson, S.; Gladman, J.; O’Mahony, S.; Ali, K.; et al. Comprehensive Clinical Research Network. Improving recruitment of older people to research through good practice. Age Ageing 2011, 40, 659–665. [Google Scholar] [CrossRef] [Green Version]
- The Multi-Regional Clinical Trials Center of Brigham and Women’s Hospital and Harvard. Health Literacy in Clinical Research. Available online: https://mrctcenter.org/health-literacy/ (accessed on 12 April 2021).
- Hoffmann, T.C.; Légaré, F.; Simmons, M.B.; McNamara, K.; McCaffery, K.; Trevena, L.J.; Hudson, B.; Glasziou, P.P.; Del Mar, C.B. Shared decision making: What do clinicians need to know and why should they bother? Med. J. Aust. 2014, 201, 35–39. [Google Scholar] [CrossRef] [PubMed]
- Sluggett, J.K.; Bell, J.S.; Lang, C.; Corlis, M.; Whitehead, C.; Wesselingh, S.L.; Inacio, M.C. Variation in Provision of Collaborative Medication Reviews on Entry to Long-Term Care Facilities. J. Am. Med. Dir. Assoc. 2021, 22, 148–155.e1. [Google Scholar] [CrossRef]
- Staykov, E.; Qureshi, D.; Scott, M.; Talarico, R.; Hsu, A.T.; Howard, M.; Costa, A.P.; Fung, C.; Ip, M.; Liddy, C.; et al. Do Patients Retain their Family Physicians after Long-Term Care Entry? A Retrospective Cohort Study. J. Am. Med. Dir. Assoc. 2020, 21, 1951–1957. [Google Scholar] [CrossRef] [PubMed]
- Wurmbach, V.S.; Schmidt, S.J.; Lampert, A.; Frick, E.; Metzner, M.; Bernard, S.; Thürmann, P.A.; Wilm, S.; Mortsiefer, A.; Altiner, A.; et al. Development of an algorithm to detect and reduce complexity of drug treatment and its technical realisation. BMC Med. Inform. Decis. Mak. 2020, 20, 154. [Google Scholar] [CrossRef] [PubMed]
- Lepelley, M.; Genty, C.; Lecoanet, A.; Allenet, B.; Bedouch, P.; Mallaret, M.-R.; Gillois, P.; Bosson, J.-L. Electronic Medication Regimen Complexity Index at admission and complications during hospitalization in medical wards: A tool to improve quality of care? Int. J. Qual. Health Care 2017, 30, 32–38. [Google Scholar] [CrossRef] [PubMed]
- McDonald, M.V.; Feldman, P.H.; Barrón-Vayá, Y.; Peng, T.R.; Sridharan, S.; Pezzin, L.E. Outcomes of clinical decision support (CDS) and correlates of CDS use for home care patients with high medication regimen complexity: A randomized trial. J. Eval. Clin. Pract. 2016, 22, 10–19. [Google Scholar] [CrossRef] [Green Version]
- Westbury, J.L.; Gee, P.; Ling, T.; Brown, D.T.; Franks, K.H.; Bindoff, I.; Bindoff, A.; Peterson, G.M. RedUSe: Reducing antipsychotic and benzodiazepine prescribing in residential aged care facilities. Med. J. Aust. 2018, 208, 398–403. [Google Scholar] [CrossRef] [PubMed]
- Sluggett, J.K.; Harrison, S.L.; Ritchie, L.A.; Clough, A.J.; Rigby, D.; Caughey, G.E.; Tan, E.C.K. High-Risk Medication Use in Older Residents of Long-Term Care Facilities: Prevalence, Harms, and Strategies to Mitigate Risks and Enhance Use. Sr. Care Pharm. 2020, 35, 419–433. [Google Scholar] [CrossRef]
- McDerby, N.; Kosari, S.; Bail, K.; Shield, A.; Peterson, G.; Naunton, M. The effect of a residential care pharmacist on medication administration practices in aged care: A controlled trial. J. Clin. Pharm. Ther. 2019, 44, 595–602. [Google Scholar] [CrossRef]
- Pharmaceutical Society of Australia. Submission to the Royal Commission into Aged Care Quality and Safety; PSA: Canberra, Australia, 2019. [Google Scholar]
- Royal Commission into Aged Care Quality and Safety. Final Report: Care, Dignity and Respect. Volume 1. Summary and Recommendations; Commonwealth of Australia: Canberra, Australia, 2021.
- Breitenstein, S.M.; Gross, D.; Garvey, C.A.; Hill, C.; Fogg, L.; Resnick, B. Implementation fidelity in community-based interventions. Res. Nurs. Health 2010, 33, 164–173. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | Australian Permanent RACF Population a (n = 178,713 Residents) | Permanent Resident Population within the Participating Organization (n = 703, 8 RACFs) c | Residents Participating in SIMPLER | ||
|---|---|---|---|---|---|
| All Residents (n = 242, 8 RACFs) | Residents at Intervention RACFs (n = 99, 4 RACFs) | Residents at Comparison RACFs (n = 143, 4 RACFs) | |||
| Age (years), mean (SD) | 59% aged ≥ 85 years a | 86.4 | 86.0 (8.1) | 85.7 (7.8) | 86.2 (8.3) |
| Male (n, %) | 58,104 (32.5%) a | 180 (25.6%) | 63 (26.0%) | 32 (32.3) | 31 (21.7%) |
| Dementia (n, %) | 52% b | 356 (50.6%) | 131 (54.1%) | 54 (54.6%) | 77 (53.9%) |
| Metropolitan location (n, %) | 124,348 (69.6%) a | 529 (75.2%) | 194 (80.2%) | 67 (67.7%) | 127 (88.8%) |
| N (%) or Median (IQR) | |
|---|---|
| Time between study entry and intervention delivery (days) | 28 (15–35) |
| Total number of days spent delivering the intervention at each RACF [range] | 1 to 3 |
| Pharmacist was able to discuss simplification recommendations with resident and/or family a | 20 (31.7%) |
| Number of residents or family members who did not want to proceed with simplification when it was possible b | 1 (5.0%) |
| Time spent delivering intervention (minutes) | |
| Generating recommendations | 12 (12–12) |
| Report preparation & communicating findings to RN/GP c | 20 (20–20) |
| Speaking with residents and/or family b | 15 (15–15) |
| Total time spent per resident | 32 (12–35) |
| No. of residents for whom the pharmacist recommended a referral be made for a Residential Medication Management Review | 4 (4.1%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sluggett, J.K.; Hughes, G.A.; Ooi, C.E.; Chen, E.Y.H.; Corlis, M.; Hogan, M.E.; Caporale, T.; Van Emden, J.; Bell, J.S. Process Evaluation of the SImplification of Medications Prescribed to Long-tErm Care Residents (SIMPLER) Cluster Randomized Controlled Trial: A Mixed Methods Study. Int. J. Environ. Res. Public Health 2021, 18, 5778. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115778
Sluggett JK, Hughes GA, Ooi CE, Chen EYH, Corlis M, Hogan ME, Caporale T, Van Emden J, Bell JS. Process Evaluation of the SImplification of Medications Prescribed to Long-tErm Care Residents (SIMPLER) Cluster Randomized Controlled Trial: A Mixed Methods Study. International Journal of Environmental Research and Public Health. 2021; 18(11):5778. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115778
Chicago/Turabian StyleSluggett, Janet K., Georgina A. Hughes, Choon Ean Ooi, Esa Y. H. Chen, Megan Corlis, Michelle E. Hogan, Tessa Caporale, Jan Van Emden, and J. Simon Bell. 2021. "Process Evaluation of the SImplification of Medications Prescribed to Long-tErm Care Residents (SIMPLER) Cluster Randomized Controlled Trial: A Mixed Methods Study" International Journal of Environmental Research and Public Health 18, no. 11: 5778. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115778