
Cumulative Risks from Stressor Exposures and Personal Risk Factors in the Workplace: Examples from a Scoping Review

 , , and
, , and
Abstract
:1. Introduction
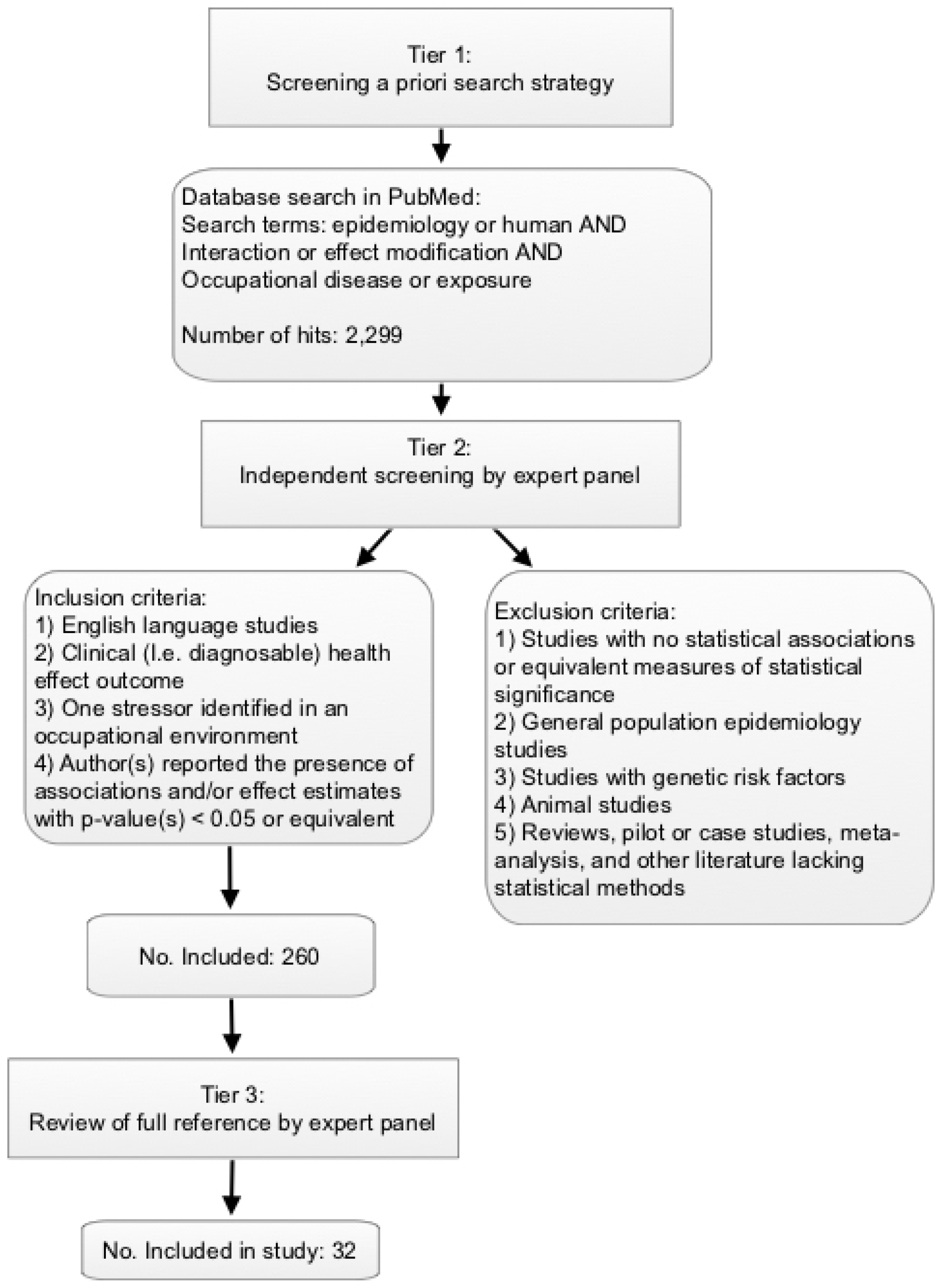
2. Materials and Methods
3. Results
4. Discussion
4.1. Strengths and Limitations
- Controlling noise and solvent exposures;
- Understanding the dose–response relationship and interactions of combined stressors;
- Considering the influence of common unmodifiable characteristics, including age, sex, and pre-existing health conditions;
- Understanding stressor exposures that are likely widespread, such as job strain, or those that may increase in likelihood or intensity in coming years, such as heat (particularly for outdoor workers);
- Understanding combination stressor exposures across more occupational categories (the present review captured predominantly manufacturing);
- Identifying personal characteristics, behaviors, community or psychosocial factors that mitigate or reduce risk.
4.2. Applying Combined Exposure Data to Improve Worker Health
- When establishing exposure limits through the risk assessment and management process:
- Different limits can be set in workplaces with the demonstrated potential for co-exposures to other stressors. For example, methylene chloride is metabolized in the human body to carbon monoxide (CO). NIOSH published a Recommended Exposure Limit (REL) for methylene chloride that was adjustable based on the presence and concentration of CO, because both exposures contribute to the formation of carboxyhemoglobin, which can impair delivery of oxygen to the tissues of the body and lead to abnormalities in functions of the central nervous system [54].
- Workplace exposure limits can be adjusted in consideration of exposures to the same chemical outside the workplace, e.g., aggregate exposure and relative source contribution, as described in Lentz et al. [10].
- When estimating risks:
- Risk estimates could account for common unmodifiable characteristics, such as age, sex, and race/ethnicity. Both disease occurrence and disease risk factors can vary by these unmodifiable characteristics due to biological mechanisms and social determinants of health. Age and sex were identified as important determinants of risk in several studies [21,24,25,29,42,44,45]; the interpretation and contribution of these factors varied in the context of each study and no overarching conclusions can be reached. One example of an existing risk methodology that takes age into account is EPA’s age-dependent adjustment factors in estimating child cancer risk from early-life exposures to mutagens [48,49].
- Established risk assessment practices typically apply an additivity assumption when combining exposures. Although the examples found in this review are few, some studies reported greater than additive interactions, suggesting that defaulting to additivity may underestimate risk in some situations.
- When selecting risk management options:
- An understanding of cumulative exposures can inform decisions among the hierarchy of controls if many workers have an unmodifiable characteristic or pre-existing condition that contributes to increased risk when co-exposure occurs.
4.3. COVID-19 and Worker Risk
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Acknowledgments
Conflicts of Interest
Author Statement
References
- National Research Council (US); Committee on Improving Risk Analysis Approaches Used by the U.S. EPA. Science and Decisions: Advancing Risk Assessment; National Academies Press: Washington, DC, USA, 2009. [Google Scholar]
- Williams, P.R.D.; Dotson, G.S.; Maier, A. Cumulative Risk Assessment (CRA): Transforming the Way We Assess Health Risks. Environ. Sci. Technol. 2012, 46, 10868–10874. [Google Scholar] [CrossRef] [Green Version]
- Schulte, P.A.; Pandalai, S.; Wulsin, V.; Chun, H. Interaction of Occupational and Personal Risk Factors in Workforce Health and Safety. Am. J. Public Health 2012, 102, 434–448. [Google Scholar] [CrossRef]
- U.S. EPA. Guidance on Cumulative Risk Assessment, Part 1. Planning and Scoping. 1997. Available online: https://www.epa.gov/risk/guidance-cumulative-risk-assessment-part-1-planning-and-scoping (accessed on 15 April 2021).
- Fox, M.A. Evaluating cumulative risk assessment for environmental justice: A community case study. Environ. Health Perspect. 2002, 110 (Suppl. 2), 203–209. [Google Scholar] [CrossRef]
- U.S. EPA. Framework for Cumulative Risk Assessment. 2003. Available online: https://www.epa.gov/risk/framework-cumulative-risk-assessment (accessed on 24 September 2020).
- NIOSH. Mixed Exposures Research Agenda: A Report by the NORA Mixed Exposures Team (DHHS 2005-106). 2004. Available online: https://www.cdc.gov/niosh/docs/2005-106/pdfs/2005-106.pdf (accessed on 15 April 2021).
- Fox, M.A.; Brewer, L.E.; Martin, L. An Overview of Literature Topics Related to Current Concepts, Methods, Tools, and Applications for Cumulative Risk Assessment (2007–2016). Int. J. Environ. Res. Public Health 2017, 14, 389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- NIOSH. Current Intelligence Bulletin 69: NIOSH Practices in Occupational Risk Assessment. Available online: https://www.cdc.gov/niosh/docs/2020-106/ (accessed on 15 March 2021).
- Lentz, T.J.; Dotson, G.S.; Williams, P.R.; Maier, A.; Gadagbui, B.; Pandalai, S.P.; Lamba, A.; Hearl, F.; Mumtaz, M. Aggregate Exposure and Cumulative Risk Assessment—Integrating Occupational and Non-occupational Risk Factors. J. Occup. Environ. Hyg. 2015, 12 (Suppl. 1), S112–S126. [Google Scholar] [CrossRef] [Green Version]
- NIOSH. Fundamentals of Total Worker Health Approaches: Essential Elements for Advancing Worker Safety, Health, and Well-being. 2016. Available online: https://www.cdc.gov/niosh/docs/2017-112/default.html (accessed on 15 March 2021).
- Fox, M.A.; Spicer, K.; Chosewood, L.C.; Susi, P.; Johns, D.O.; Dotson, G.S. Implications of applying cumulative risk assessment to the workplace. Environ. Int. 2018, 115, 230–238. [Google Scholar] [CrossRef] [PubMed]
- Niemeier, R.T.; Williams, P.R.; Rossner, A.; Clougherty, J.E.; Rice, G.E. A Cumulative Risk Perspective for Occupational Health and Safety (OHS) Professionals. Int. J. Environ. Res. Public Health 2020, 17, 6342. [Google Scholar] [CrossRef]
- Wallace, B.C.; Small, K.; Brodley, C.E.; Lau, J.; Trikalinos, T.A. Deploying an interactive machine learning system in an evi-dence-based practice center: Abstrackr. In Proceedings of the 2nd ACM SIGHIT International Health Informatics Symposium (IHI ’12), Miami, FL, USA, 28 January 2012; pp. 819–824. [Google Scholar]
- Brown University Center for Evidence Synthesis in Health. Abstrackr. Available online: http://abstrackr.cebm.brown.edu/account/login (accessed on 23 February 2021).
- Andersen, A.; Berge, S.R.; Engeland, A.; Norseth, T. Exposure to nickel compounds and smoking in relation to incidence of lung and nasal cancer among nickel refinery workers. Occup. Environ. Med. 1996, 53, 708–713. [Google Scholar] [CrossRef] [PubMed]
- Christensen, C.H.; Platz, E.A.; Andreotti, G.; Blair, A.; Hoppin, J.A.; Koutros, S.; Lynch, C.F.; Sandler, D.P.; Alavanja, M.C. Coumaphos Exposure and Incident Cancer among Male Participants in the Agricultural Health Study (AHS). Environ. Health Perspect. 2010, 118, 92–96. [Google Scholar] [CrossRef] [Green Version]
- Henneberger, P.K.; Ferris, B.G.; Sheehe, P.R. Accidental Gassing Incidents and the Pulmonary Function of Pulp Mill Workers. Am. Rev. Respir. Dis. 1993, 148, 63–67. [Google Scholar] [CrossRef]
- Kamel, F.; Goldman, S.M.; Umbach, D.M.; Chen, H.; Richardson, G.; Barber, M.R.; Meng, C.; Marras, C.; Korell, M.; Kasten, M.; et al. Dietary fat intake, pesticide use, and Parkinson’s disease. Park. Relat. Disord. 2014, 20, 82–87. [Google Scholar] [CrossRef] [Green Version]
- Koutros, S.; Silverman, D.T.; Alavanja, M.C.; Andreotti, G.; Lerro, C.C.; Heltshe, S.; Lynch, C.F.; Sandler, D.P.; Blair, A.; Freeman, L.E.B. Occupational exposure to pesticides and bladder cancer risk. Int. J. Epidemiol. 2016, 45, 792–805. [Google Scholar] [CrossRef] [Green Version]
- Neuberger, M.; Rappe, C.; Bergek, S.; Cai, H.; Hansson, M.; Jäger, R.; Kundi, M.; Lim, C.; Wingfors, H.; Smith, A. Persistent Health Effects of Dioxin Contamination in Herbicide Production. Environ. Res. 1999, 81, 206–214. [Google Scholar] [CrossRef] [PubMed]
- Osterman, J.W.; Greaves, I.A.; Smith, T.J.; Hammond, S.K.; Robins, J.M.; Theriault, G. Work related decrement in pulmonary function in silicon carbide production workers. Occup. Environ. Med. 1989, 46, 708–716. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sancini, A.; Fioravanti, M.; Ciarrocca, M.; Palermo, P.; Fiaschetti, M.; Schifano, M.; Tomei, G.; Tomei, F. Pulmonary nodules in workers exposed to urban stressor. Environ. Res. 2010, 110, 519–525. [Google Scholar] [CrossRef]
- Schlünssen, V.; Schaumburg, I.; Taudorf, E.; Mikkelsen, A.B.; Sigsgaard, T. Respiratory Symptoms and Lung Function among Danish Woodworkers. J. Occup. Environ. Med. 2002, 44, 82–98. [Google Scholar] [CrossRef]
- Stern, F.B.; Halperin, W.E.; Hornung, R.W.; Ringenburg, V.L.; McCammon, C.S. Heart disease mortality among bridge and tunnel officers exposed to carbon monoxide. Am. J. Epidemiol. 1988, 128, 1276–1288. [Google Scholar] [CrossRef]
- Järup, L.; Pershagen, G. Arsenic Exposure, Smoking, and Lung Cancer in Smelter Workers—A Case-Control Study. Am. J. Epidemiol. 1991, 134, 545–551. [Google Scholar] [CrossRef] [PubMed]
- Sallmen, M.; Neto, M.; Mayan, O.N. Reduced fertility among shoe manufacturing workers. Occup. Environ. Med. 2007, 65, 518–524. [Google Scholar] [CrossRef]
- Yang, A.; Cheng, N.; Pu, H.; Liu, S.; Dai, M.; Zheng, T.; Bai, Y. Occupational metal exposures, smoking and risk of diabetes and prediabetes. Occup. Med. 2016, 67, 217–223. [Google Scholar] [CrossRef] [Green Version]
- Shortridge, L.A.; Lemasters, G.K.; Valanis, B.; Hertzberg, V. Menstrual cycles in nurses handling antineoplastic drugs. Cancer Nurs. 1995, 18, 439–444. [Google Scholar] [CrossRef] [PubMed]
- Fu, H.; Jing, X.; Yu, S.; Gu, X.; Wu, K.; Yang, J.; Qiu, S. Quantitative risk assessment for lung cancer from exposure to metal ore dust. Biomed. Environ. Sci. 1992, 5, 221–228. [Google Scholar]
- Coenraaos, P.J.; Foo, S.C.; Phoon, W.O.; Lun, K.C. Dermatitis in small-scale metal industries. Contact Dermat. 1985, 12, 155–160. [Google Scholar] [CrossRef]
- Attarchi, M.; Golabadi, M.; Labbafinejad, Y.; Mohammadi, S. Combined effects of exposure to occupational noise and mixed organic solvents on blood pressure in car manufacturing company workers. Am. J. Ind. Med. 2013, 56, 243–251. [Google Scholar] [CrossRef]
- Chang, T.-Y.; Wang, V.-S.; Hwang, B.-F.; Yen, H.-Y.; Lai, J.-S.; Liu, C.-S.; Lin, S.-Y. Effects of Co-exposure to Noise and Mixture of Organic Solvents on Blood Pressure. J. Occup. Health 2009, 51, 332–339. [Google Scholar] [CrossRef] [Green Version]
- Morata, T.C.; Dunn, D.E.; Kretschmer, L.W.; Lemasters, G.K.; Keith, R.W. Effects of occupational exposure to organic solvents and noise on hearing. Scand. J. Work Environ. Health 1993, 19, 245–254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sliwinska-Kowalska, M.; Zamyslowska-Szmytke, E.; Szymczak, W.; Kotylo, P.; Fiszer, M.; Wesolowski, W.; Pawlaczyk-Luszczynska, M. Exacerbation of noise-induced hearing loss by co-exposure to workplace chemicals. Environ. Toxicol. Pharmacol. 2005, 19, 547–553. [Google Scholar] [CrossRef]
- Jones, R.N.; Butcher, B.T.; Hammad, Y.Y.; Diem, J.E.; Glindmeyer, H.W.; Lehrer, S.B.; Hughes, J.M.; Weill, H. Interaction of atopy and exposure to cotton dust in the bronchoconstrictor response. Occup. Environ. Med. 1980, 37, 141–146. [Google Scholar] [CrossRef] [Green Version]
- Wong, R.-H.; Chen, P.-C.; Wang, J.-D.; Du, C.-L.; Cheng, T.-J. Interaction of Vinyl Chloride Monomer Exposure and Hepatitis B Viral Infection on Liver Cancer. J. Occup. Environ. Med. 2003, 45, 379–383. [Google Scholar] [CrossRef] [PubMed]
- Pouryaghoub, G.; Mehrdad, R.; Mohammadi, S. Interaction of smoking and occupational noise exposure on hearing loss: A cross-sectional study. BMC Public Health 2007, 7, 137. [Google Scholar] [CrossRef] [Green Version]
- Zhao, Y.; Tao, L.; Davis, R.; Heyer, N.; Yang, Q.; Qiu, W.; Li, N.; Zhu, L.; Zhang, H.; Zeng, L. Effect of cigarette smoking on noise-induced hearing loss in workers exposed to occupational noise in China. Noise Health 2013, 15, 67–72. [Google Scholar] [CrossRef] [PubMed]
- Heilskov-Hansen, T.; Mikkelsen, S.; Svendsen, S.W.; Thygesen, L.C.; Hansson, G.Å.; Thomsen, J.F. Exposure–response relationships between movements and postures of the wrist and carpal tunnel syndrome among male and female house painters: A retrospective cohort study. Occup. Environ. Med. 2016, 73, 401–408. [Google Scholar] [CrossRef]
- Hornung, R.W.; Deddens, J.A.; Roscoe, R.J. Modifiers of Lung Cancer Risk in Uranium Miners from the Colorado Plateau. Health Phys. 1998, 74, 12–21. [Google Scholar] [CrossRef]
- Howe, G.R.; Nair, R.C.; Newcombe, H.B.; Miller, A.B.; Abbatt, J.D. Lung cancer mortality (1950-80) in relation to radon daugh-ter exposure in a cohort of workers at the eldorado beaverlodge uranium mine. J. Natl. Cancer Inst. 1986, 77, 357–362. [Google Scholar] [PubMed]
- Schubauer-Berigan, M.K.; Daniels, R.D.; Pinkerton, L.E. Radon Exposure and Mortality Among White and American Indian Uranium Miners: An Update of the Colorado Plateau Cohort. Am. J. Epidemiol. 2009, 169, 718–730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, G.H.; Sampson, L.A.; Fink, D.S.; Wang, J.; Russell, D.; Gifford, R.; Fullerton, C.; Ursano, R.; Galea, S. Gender, Position of Authority, and the Risk of Depression and Posttraumatic Stress Disorder among a National Sample of U.S. Reserve Component Personnel. Women’s Health Issues 2016, 26, 268–277. [Google Scholar] [CrossRef] [Green Version]
- Heraclides, A.M.; Chandola, T.; Witte, D.R.; Brunner, E.J. Work Stress, Obesity and the Risk of Type 2 Diabetes: Gender-Specific Bidirectional Effect in the Whitehall II Study. Obesity 2012, 20, 428–433. [Google Scholar] [CrossRef] [PubMed]
- Clays, E.; Casini, A.; Van Herck, K.; De Bacquer, D.; Kittel, F.; De Backer, G.; Holtermann, A. Do psychosocial job resources buffer the relation between physical work demands and coronary heart disease? A prospective study among men. Int. Arch. Occup. Environ. Health 2016, 89, 1299–1307. [Google Scholar] [CrossRef]
- Sabbath, E.L.; Glymour, M.M.; Descatha, A.; Leclerc, A.; Zins, M.; Goldberg, M.; Berkman, L.F. Biomechanical and psychosocial occupational exposures: Joint predictors of post-retirement functional health in the French GAZEL cohort. Adv. Life Course Res. 2013, 18, 235–243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barton, H.A.; Cogliano, V.J.; Flowers, L.; Valcovic, L.; Setzer, R.W.; Woodruff, T.J. Assessing Susceptibility from Early-Life Exposure to Carcinogens. Environ. Health Perspect. 2005, 113, 1125–1133. [Google Scholar] [CrossRef]
- U.S. EPA. Supplemental Guidance for Assessing Susceptibility from Early-Life Exposure to Carcinogens. Available online: https://www.epa.gov/risk/supplemental-guidance-assessing-susceptibility-early-life-exposure-carcinogens (accessed on 23 February 2021).
- NIOSH. Productive Aging and Work. Available online: https://www.cdc.gov/niosh/topics/productiveaging/default.html (accessed on 5 February 2021).
- OSHA, NIOSH. Preventing Hearing Loss Caused by Chemical (Ototoxicity) and Noise Exposure. 2018. Available online: https://www.cdc.gov/niosh/docs/2018-124/default.html (accessed on 15 April 2021).
- Moretto, A.; Bachman, A.; Boobis, A.; Solomon, K.R.; Pastoor, T.P.; Wilks, M.F.; Embry, M.R. A framework for cumulative risk assessment in the 21st century. Crit. Rev. Toxicol. 2017, 47, 85–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Solomon, K.R.; Wilks, M.F.; Bachman, A.; Boobis, A.; Moretto, A.; Pastoor, T.P.; Phillips, R.; Embry, M.R. Problem formulation for risk assessment of combined exposures to chemicals and other stressors in humans. Crit. Rev. Toxicol. 2016, 46, 835–844. [Google Scholar] [CrossRef] [Green Version]
- NIOSH. Criteria for a Recommended Standard: Occupational Exposure to Methylene Chloride (DHHS 76-138). Available online: https://www.cdc.gov/niosh/docs/76-138/default.html (accessed on 15 April 2021).
- ACGIH. TLVs and BEIs Based on the Documentation of the Threshold Limit Values for Chemical Substances and Physical Agents and Biological Exposure Indices. Cincinnati, Ohio: American Conference of Governmental Industrial Hygienists. 2021. Available online: https://www.acgih.org/science/tlv-bei-guidelines/ (accessed on 15 April 2021).
- Ajufo, E.; Rao, S.; Navar, A.M.; Pandey, A.; Ayers, C.R.; Khera, A. U.S. population at increased risk of severe illness from COVID-19. Am. J. Prev. Cardiol. 2021, 6, 100156. [Google Scholar] [CrossRef]
- Azar, K.M.J.; Shen, Z.; Romanelli, R.J.; Lockhart, S.H.; Smits, K.; Robinson, S.; Brown, S.; Pressman, A.R. Disparities in Outcomes among COVID-19 Patients in a Large Health Care System in California. Health Aff. 2020, 39, 1253–1262. [Google Scholar] [CrossRef] [PubMed]
- CDC. People at Increased Risk. Available online: https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/index.html (accessed on 23 February 2021).
- Mutambudzi, M.; Niedzwiedz, C.; Macdonald, E.B.; Leyland, A.; Mair, F.; Anderson, J.; Celis-Morales, C.; Cleland, J.; Forbes, J.; Gill, J.; et al. Occupation and risk of severe COVID-19: Prospective cohort study of 120 075 UK Biobank participants. Occup. Environ. Med. 2021, 78, 307–314. [Google Scholar] [CrossRef]
- Selden, T.M.; Berdahl, T.A. Risk of Severe COVID-19 among Workers and Their Household Members. JAMA Intern. Med. 2021, 181, 120. [Google Scholar] [CrossRef]
- NIOSH. Exposome and Exposomics. Available online: https://www.cdc.gov/niosh/topics/exposome/default.html (accessed on 2 February 2021).
- Wild, C.P. The exposome: From concept to utility. Int. J. Epidemiol. 2012, 41, 24–32. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Stressor or Risk Factor Combination | Number of Articles | Work-Related Stressor Exposure(s) a | Personal Risk Factors a | Health Effect(s) a | References |
|---|---|---|---|---|---|
| Chemical and personal | 16 | Solvents, solvents and oil, soluble nickel, metal ore dust, urban air, arsenic and metals from smelting (2), pesticides (3), mixed dust (2), wood dust, CO, TCDD, antineoplastic drugs | Age (4), family history, sex, saturated fat intake, smoking or not smoking (9) | Asthma, bladder cancer, dermatitis, lung cancer, lung function, pulmonary nodules, diabetes, Parkinson’s, heart disease, liver damage, female fertility, menstrual dysfunction | [16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31] |
| Chemical and physical | 4 | Solvents and noise (4) | Hypertension (2), hearing loss (2) | [32,33,34,35] | |
| Chemical and biological | 2 | Cotton dust, vinyl chloride | Atopy, HepB surface antigen positive | Lung function, liver cancer | [36,37] |
| Physical and personal | 2 | Noise (2) | Smoking (2) | Hearing loss | [38,39] |
| Physical exertion and personal | 1 | Increasing wrist velocity | Sex | Carpal tunnel syndrome diagnosis or surgery | [40] |
| Radon and personal | 3 | Radon (3) | Age (3) | Lung cancer | [41,42,43] |
| Psycho-social and personal | 2 | Military authority, work stress | Sex, sex and obesity | PTSD, diabetes | [44,45] |
| Physical exertion and psycho-social | 2 | High physical demand and job strain, biomechanical exposure, and low social support | Heart disease, physical functioning disability | [46,47] |
| Measure of Association (CI) | Occupational Stressor 1 | Occupational Stressor 2 | Personal Risk Factor | Health Effect | Reference |
|---|---|---|---|---|---|
| OR = 184.5 (15–infinity) | Vinyl chloride | HBsAg + | Liver cancer | [37] | |
| RR = 47 (5.3–415.7) | Cumulative dust | Smoking | Lung cancer | [30] | |
| OR = 29.6 (2.6–335.6) | As >100 mg/m3-yrs | Smoking | Lung cancer ^ | [26] | |
| OR = 21.5 (5–26) | Mixed solvents (styrene, toluene) | Noise | Hearing loss | [35] | |
| OR = 20.2 (3.8–26) | Mixed solvents (hexane, toluene) | Noise | Hearing loss | [35] | |
| OR = 14.22 (3.21–40.84) | Organic solvents | Noise | High blood pressure | [32] | |
| OR = 13.5 (1.5–117.8) | Organic solvents | Noise | High blood pressure | [33] | |
| RR = 10.9 (4.1–28.9) | Toluene | Noise | Hearing loss | [34] | |
| OR = 10.4 (1.2–86.6) | As 15 to <100 mg/m3-yrs | Smoking | Lung cancer ^ | [26] | |
| SRR = 9.5 (3.7–25) | Radon | Smoking | Lung cancer ^ | [43] | |
| OR = 7.9 (1–63.1) | As 0.25 to <15 mg/m3-yrs | Smoking | Lung cancer ^ | [26] | |
| OR = 7.8 (4.7–13) | Noise | Smoking | Hearing loss | [38] | |
| OR = 7.17 (2.64–19.5) | Oil | Solvent | Dermatitis | [31] | |
| OR = 6.45 (1.07–38.98) | Dust exposure | Female sex | Asthma | [24] | |
| Adjusted IRR = 6.37 (3.64–11.3) | Increasing wrist velocity | Sex | Carpal tunnel syndrome surgery + | [40] | |
| RR = 5.81 (2.44–10.68) | Rn >5 WLM | Age of first exposure 30–39 | Lung cancer | [42] | |
| OR = 5.8 (2.3–14.6) | Rotenone | Higher saturated fat intake | Parkinson’s disease | [19] | |
| OR = 5.25 (1.66–16.6) | Solvent | Smoking | Increased female fertility | [27] | |
| RR = 5.1 (1.3–20.5) | Soluble Nickel | Smoking | Lung cancer | [16] | |
| RR = 4.43 (2.1–7.65) | Rn >5 WLM | Age of first exposure >40 | Lung cancer | [42] | |
| OR = 4.2 (1.5–12) | Paraquat | Low saturated fat intake | Parkinson’s disease | [19] | |
| Adjusted IRR = 4.11(2.61–6.48) | Increasing wrist velocity | Sex | Carpal tunnel syndrome diagnosis + | [40] | |
| HR = 3.63 (1.08–12.22) | High physical work demand | Low social support | Coronary heart disease | [46] | |
| PR = 3.6 (2.4–5.4) | Metal exposure | Smoking | Diabetes mellitus | [28] | |
| OR = 3.43 (1.61–7.32) | Administering antineoplastic drugs | Age | Menstrual dysfunction | [29] | |
| OR = 3.28 (1.10–9.92) | Oil | Solvent | Age > 35 | Dermatitis | [31] |
| RR = 3.03 (1.46–6.29) | Pesticide | Smoking | Bladder cancer | [20] | |
| RR = 2.97 (p < 0.001) | Rn WLM | Age < 60 | Lung Cancer | [41] | |
| OR = 2.66 (1.42–4.99) | Solvent | Coffee | Increased female fertility | [27] | |
| RR = 2.14 (1.02–4.52) | Urban air pollutants | Smoking | Pulmonary nodules | [23] | |
| HR = 2.01 (1.06–3.92 | Work Stress | Female sex, Obesity | Type 2 diabetes | [45] | |
| RR = 1.91 (1.23–2.95) | Coumaphos | Family history of prostate cancer | Prostate cancer | [17] | |
| RR = 1.91 (1.61–2.26) | Biomechanical | Psychosocial job strain | Physical function disability ^ | [47] | |
| OR = 1.94 (1.31–2.88) | Noise | Smoking | Hearing loss + | [39] | |
| PR = 1.4 (1.0–2.3) | Metals | Smoking | Diabetes mellitus | [28] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fox, M.A.; Niemeier, R.T.; Hudson, N.; Siegel, M.R.; Dotson, G.S. Cumulative Risks from Stressor Exposures and Personal Risk Factors in the Workplace: Examples from a Scoping Review. Int. J. Environ. Res. Public Health 2021, 18, 5850. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115850
Fox MA, Niemeier RT, Hudson N, Siegel MR, Dotson GS. Cumulative Risks from Stressor Exposures and Personal Risk Factors in the Workplace: Examples from a Scoping Review. International Journal of Environmental Research and Public Health. 2021; 18(11):5850. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115850
Chicago/Turabian StyleFox, Mary A., Richard Todd Niemeier, Naomi Hudson, Miriam R. Siegel, and Gary Scott Dotson. 2021. "Cumulative Risks from Stressor Exposures and Personal Risk Factors in the Workplace: Examples from a Scoping Review" International Journal of Environmental Research and Public Health 18, no. 11: 5850. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115850