
Effects of Cardiopulmonary Rehabilitation on the Muscle Function of Children with Congenital Heart Disease: A Prospective Cohort Study

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Measurements
2.3.1. Anthropometric Characteristics
2.3.2. Muscle Function
2.4. Intervention
2.5. Statistical Analyses
3. Results
3.1. Population
3.2. Program Adherence and Safety
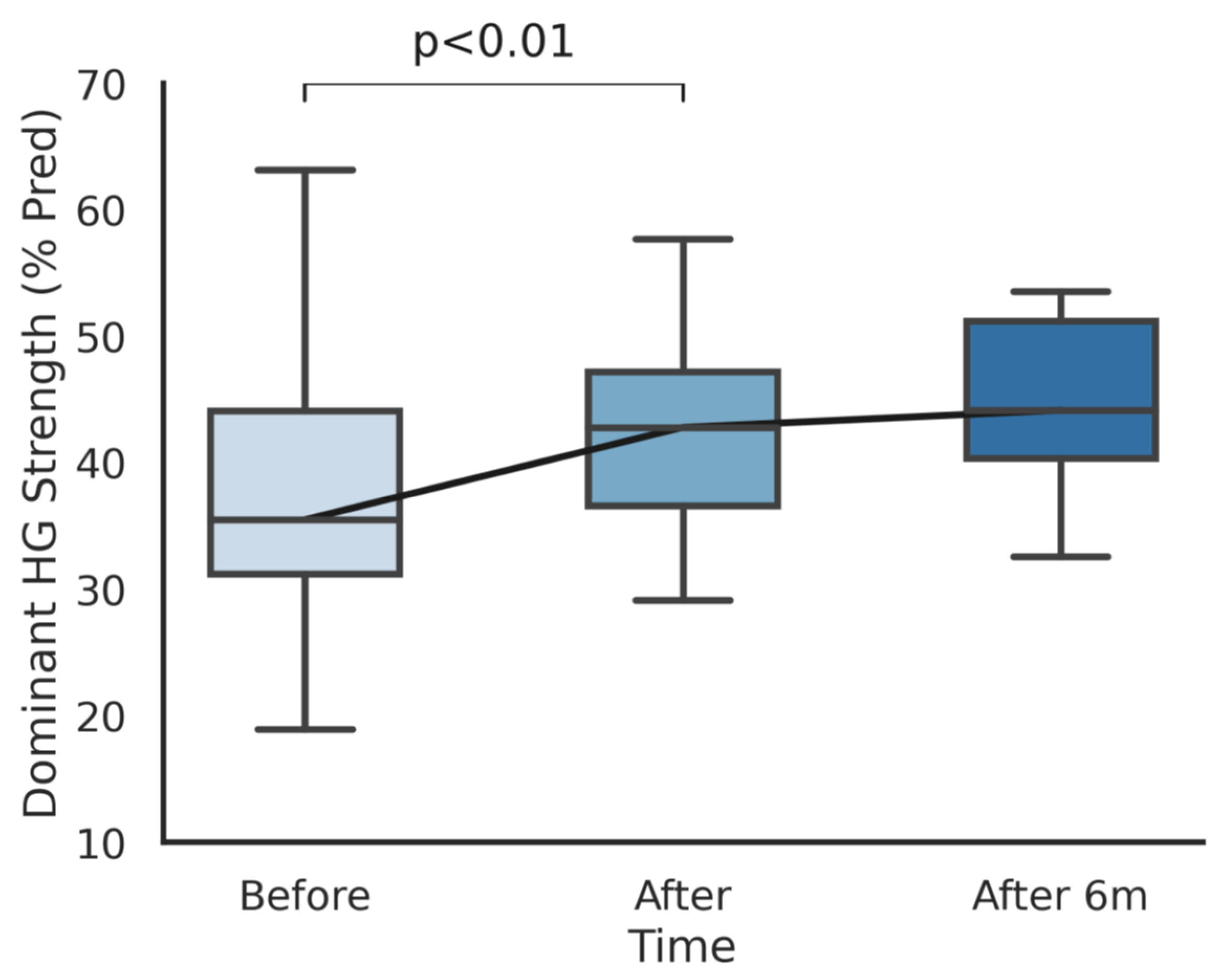
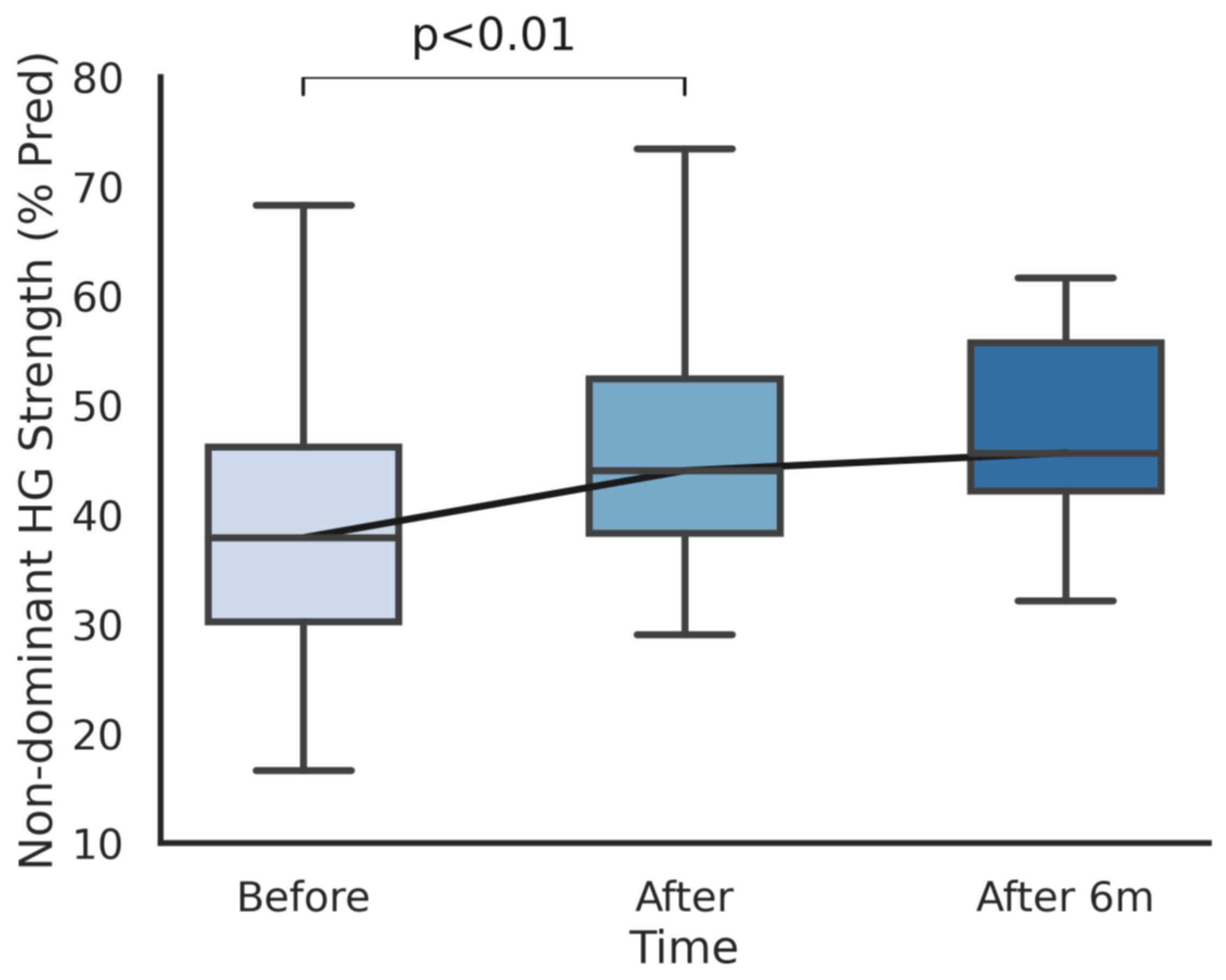
3.3. Muscle Function
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hoffman, J.I.E.; Kaplan, S. The incidence of congenital heart disease. J. Am. Coll. Cardiol. 2002, 39, 1890–1900. [Google Scholar] [CrossRef] [Green Version]
- Hoffman, J.I.E. The global burden of congenital heart disease. Cardiovasc. J. Afr. 2013, 24, 141–145. [Google Scholar] [CrossRef] [Green Version]
- Erikssen, G.; Liestøl, K.; Seem, E.; Birkeland, S.; Saatvedt, K.J.; Hoel, T.N.; Døhlen, G.; Skulstad, H.; Svennevig, J.L.; Thaulow, E.; et al. Achievements in congenital heart defect surgery: A prospective, 40-year study of 7038 patients. Circulation 2015, 131, 337–346. [Google Scholar] [CrossRef] [Green Version]
- Amedro, P.; Dorka, R.; Moniotte, S.; Guillaumont, S.; Fraisse, A.; Kreitmann, B.; Borm, B.; Bertet, H.; Barréa, C.; Ovaert, C.; et al. Quality of Life of Children with Congenital Heart Diseases: A Multicenter Controlled Cross-Sectional Study. Pediatr. Cardiol. 2015, 36, 1588–1601. [Google Scholar] [CrossRef] [PubMed]
- Fredriksen, P.M.; Therrien, J.; Veldtman, G.; Warsi, M.A.; Liu, P.; Siu, S.; Williams, W.; Granton, J.; Webb, G. Lung function and aerobic capacity in adult patients following modified Fontan procedure. Heart 2001, 85, 295–299. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baumgartner, H.; Bonhoeffer, P.; De Groot, N.M.; de Haan, F.; Deanfield, J.E.; Galie, N.; Gatzoulis, M.A.; Gohlke-Baerwolf, C.; Kaemmerer, H. ESC Guidelines for the management of grown-up congenital heart disease (new version 2010). Eur. Heart J. 2010, 31, 2915–2957. [Google Scholar] [CrossRef] [PubMed]
- Greutmann, M.; Le, T.L.; Tobler, D.; Biaggi, P.; Oechslin, E.N.; Silversides, C.K.; Granton, J.T. Generalised muscle weakness in young adults with congenital heart disease. Heart 2011, 97, 1164–1168. [Google Scholar] [CrossRef]
- Acosta-Dighero, R.; Torres-Castro, R.; Rodríguez-Núñez, I.; Rosales-Fuentes, J.; Vilaró, J.; Fregonezi, G.; Lopetegui, B. Physical activity assessments in children with congenital heart disease: A systematic review. Acta Paediatr. Int. J. Paediatr. 2020. [Google Scholar] [CrossRef]
- Rhodes, J.; Curran, T.J.; Camil, L.; Rabideau, N.; Fulton, D.R.; Gauthier, N.S.; Gauvreau, K.; Jenkins, K.J. Impact of cardiac rehabilitation on the exercise function of children with serious congenital heart disease. Pediatrics 2005, 116, 1339–1345. [Google Scholar] [CrossRef]
- Longmuir, P.E.; Brothers, J.A.; De Ferranti, S.D.; Hayman, L.L.; Van Hare, G.F.; Matherne, G.P.; Davis, C.K.; Joy, E.A.; McCrindle, B.W. Promotion of physical activity for children and adults with congenital heart disease: A scientific statement from the American Heart Association. Circulation 2013, 127, 2147–2159. [Google Scholar] [CrossRef] [Green Version]
- Bernhardt, D.T.; Gomez, J.; Johnson, M.D.; Martin, T.J.; Rowland, T.W.; Small, E.; LeBlanc, C.; Malina, R.; Krein, C.; Young, J.C.; et al. Strength training by children and adolescents. Pediatrics 2001, 107, 1470–1472. [Google Scholar] [CrossRef] [Green Version]
- Faigenbaum, A.D.; Westcott, W.L.; Micheli, L.J.; Outerbridge, A.R.; Long, C.J.; LaRosa-Loud, R.; Zaichkowsky, L.D. The Effects of Strength Training and Detraining on Children. J. Strength Cond. Res. 1996, 10, 109–114. [Google Scholar] [CrossRef]
- Thompson, P. ACSM Guidelines for Exercise Testing and Prescription Benefits and Risks Associated with Physical Activity, 10th ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2017. [Google Scholar]
- Gomes-Neto, M.; Saquetto, M.B.; da Silva e Silva, C.M.; Conceição, C.S.; Carvalho, V.O. Impact of Exercise Training in Aerobic Capacity and Pulmonary Function in Children and Adolescents After Congenital Heart Disease Surgery: A Systematic Review with Meta-analysis. Pediatr. Cardiol. 2016, 37, 217–224. [Google Scholar] [CrossRef]
- Baumgartner, H.; De Backer, J.; Babu-Narayan, S.V.; Budts, W.; Chessa, M.; Diller, G.P.; Lung, B.; Kluin, J.; Lang, I.M.; Meijboom, F.; et al. 2020 ESC Guidelines for the management of adult congenital heart disease: The Task Force for the management of adult congenital heart disease of the European Society of Cardiology (ESC). Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Adult Congenital Heart Disease (ISACHD). Eur. Heart J. 2021, 42, 563–645. [Google Scholar]
- Cooper, D.; Weiler-Ravell, D. Gas Exchange Response to Exercise in Children. Am. Rev. Respir. Dis. 1984, 129, 547–548. [Google Scholar] [CrossRef] [Green Version]
- Carrascosa, A.; Yeste, D.; Moreno-Galdó, A.; Gussinyé, M.; Ferrández, Á.; Clemente, M.; Fernández-Cancio, M. Body mass index and tri-ponderal mass index of 1,453 healthy non-obese, non-undernourished millennial children. The Barcelona longitudinal growth study. An. Pediatría 2018, 89, 137–143. [Google Scholar] [CrossRef] [PubMed]
- Roberts, H.C.; Denison, H.J.; Martin, H.J.; Patel, H.P.; Syddall, H.; Cooper, C.; Sayer, A.A. A review of the measurement of grip strength in clinical and epidemiological studies: Towards a standardised approach. Age Ageing 2011, 40, 423–429. [Google Scholar] [CrossRef] [Green Version]
- Stark, T.; Walker, B.; Phillips, J.K.; Fejer, R.; Beck, R. Hand-held dynamometry correlation with the gold standard isokinetic dynamometry: A systematic review. PM R 2011, 3, 472–479. [Google Scholar] [CrossRef] [PubMed]
- Bohannon, R.W. Test-retest reliabilty of hand-held dynamometry during a single session of strength assessment. Phys Ther. 1986, 66, 206–208. [Google Scholar] [CrossRef]
- Hébert-Losier, K.; Newsham-West, R.J.; Schneiders, A.G.; Sullivan, S.J. Raising the standards of the calf-raise test: A systematic review. J. Sci. Med. Sport 2009, 12, 594–602. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Svantesson, U.; Österberg, U.; Thomeé, R.; Grimby, G. Muscle fatigue in a standing heel-rise test. Scand. J. Rehab. Med. 1998; 30, 67–72. [Google Scholar]
- Hébert, L.J.; Maltais, D.B.; Lepage, C.; Saulnier, J.; Crête, M.; Perron, M. Isometric muscle strength in youth assessed by hand-held dynamometry: A feasibility, reliability, and validity study: A feasibility, reliability, and validity study. Pediatr. Phys. Ther. 2011, 23, 289–299. [Google Scholar] [CrossRef] [PubMed]
- Neidenbach, R.C.; Oberhoffer, R.; Pieper, L.; Freilinger, S.; Ewert, P.; Kaemmerer, H.; Nagdyman, N.; Hager, A.; Müller, J. The value of hand grip strength (HGS) as a diagnostic and prognostic biomarker in congenital heart disease. Cardiovasc. Diagn. Ther. 2019, 9, S187–S197. [Google Scholar] [CrossRef] [PubMed]
- Pallone, G.; Palmieri, M.; Cariati, I.; Bei, R.; Masuelli, L.; D’arcangelo, G.; Tancredi, V. Different continuous training modalities result in distinctive effects on muscle structure, plasticity and function. Biomed. Rep. 2020, 12, 267–275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stout, K.K.; Daniels, C.J.; Aboulhosn, J.A.; Bozkurt, B.; Broberg, C.S.; Colman, J.M.; Crumb, S.R.; Dearani, J.A.; Fuller, S.; Gurvitz, M.; et al. 2018 AHA/ACC Guideline for the Management of Adults With Congenital Heart Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2019, 139. [Google Scholar] [CrossRef]
- Ferrer-Sargues, F.J.; Peiró-Molina, E.; Salvador-Coloma, P.; Carrasco Moreno, J.I.; Cano-Sánchez, A.; Vázquez-Arce, M.I.; Insa Albert, B.; Sepulveda Sanchis, P.; Cebrià i Iranzo, M.À. Cardiopulmonary rehabilitation improves respiratory muscle function and functional capacity in children with congenital heart disease. A prospective cohort study. Int. J. Environ. Res. Public Health 2020, 17, 4328. [Google Scholar] [CrossRef] [PubMed]
- Bohannon, R. Grip strength: A summary of studies comparing dominant and nondominant limb measurements. Percept. Mot. Skills 2003, 96 Pt 1, 728–730. [Google Scholar] [CrossRef]
- Witzel, C.; Sreeram, N.; Coburger, S.; Schickendantz, S.; Brockmeier, K.; Schoenau, E. Outcome of muscle and bone development in congenital heart disease. Eur. J. Pediatr. 2006, 165, 168–174. [Google Scholar] [CrossRef] [PubMed]
- Fricke, O.; Witzel, C.; Schickendantz, S.; Sreeram, N.; Brockmeier, K.; Schoenau, E. Mechanographic characteristics of adolescents and young adults with congenital heart disease. Eur. J. Pediatr. 2008, 167, 331–336. [Google Scholar] [CrossRef]
- Kröönström, L.A.; Johansson, L.; Zetterström, A.K.; Dellborg, M.; Eriksson, P.; Cider, Å. Muscle function in adults with congenital heart disease. Int. J. Cardiol. 2014, 170, 358–363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moalla, W.; Dupont, G.; Costes, F.; Gauthier, R.; Maingourd, Y.; Ahmaidi, S. Performance and muscle oxygenation during isometric exercise and recovery in children with congenital heart diseases. Int. J. Sports Med. 2006, 27, 864–869. [Google Scholar] [CrossRef]
- Mezzani, A.; Corrà, U.; Giannuzzi, P. Central adaptations to exercise training in patients with chronic heart failure. Heart Fail. Rev. 2008, 13, 13–20. [Google Scholar] [CrossRef] [PubMed]
- Moalla, W.; Elloumi, M.; Chamari, K.; Dupont, G.; Maingourd, Y.; Tabka, Z.; Ahmaidi, S. Training effects on peripheral muscle oxygenation and performance in children with congenital heart diseases. Appl. Physiol. Nutr. Metab. 2012, 37, 621–630. [Google Scholar] [CrossRef] [PubMed]
- Brassard, P.; Poirier, P.; Martin, J.; Noël, M.; Nadreau, E.; Houde, C.; Cloutier, A.; Perron, J.; Jobin, J. Impact of exercise training on muscle function and ergoreflex in Fontan patients: A pilot study. Int. J. Cardiol. 2006, 107, 85–94. [Google Scholar] [CrossRef] [PubMed]
- Dulfer, K.; Duppen, N.; Kuipers, I.M.; Schokking, M.; van Domburg, R.T.; Verhulst, F.C.; Helbing, W.A.; Utens, E.M. Aerobic exercise influences quality of life of children and youngsters with congenital heart disease: A randomized controlled trial. J. Adolesc. Health 2014, 55, 65–72. [Google Scholar] [CrossRef] [PubMed]
- Small, C. Kinetic Control—The Management of Uncontrolled Movement; Elsevier: Amsterdam, The Netherlands, 2013; Volume 14. [Google Scholar] [CrossRef]
- Alves da Cruz, M.M.; Ricci-Vitor, A.L.; Bonini Borges, G.L.; Fernanda da Silva, P.; Ribeiro, F.; Marques Vanderlei, L.C. Acute Hemodynamic Effects of Virtual Reality–Based Therapy in Patients of Cardiovascular Rehabilitation: A Cluster Randomized Crossover Trial. Arch. Phys. Med. Rehabil. 2020, 101, 642–649. [Google Scholar] [CrossRef]
- Del Corral, T.; Cebrià Iranzo, M.À.; López-de-Uralde-Villanueva, I.; Martínez-Alejos, R.; Blanco, I.; Vilaró, J. Effectiveness of a home-based active video game programme in young cystic fibrosis patients. Respiration 2018, 95, 87–97. [Google Scholar] [CrossRef]
- Neshteruk, C.D.; Nezami, B.T.; Nino-Tapias, G.; Davison, K.K.; Ward, D.S. The influence of fathers on children’s physical activity: A review of the literature from 2009 to 2015. Prev. Med. 2017, 102, 12–19. [Google Scholar] [CrossRef]
- Moola, F.; Faulkner, G.E.J.; Kirsh, J.A.; Kilburn, J. Physical activity and sport participation in youth with congenital heart disease: Perceptions of children and parents. Adapt. Phys. Act. Q. 2008, 25, 49–70. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Total (n= 15) Mean ± SD (Range) | Boys (n= 9) Mean ± SD (Range) | Girls (n= 6) Mean ± SD (Range) | p-Value | |
|---|---|---|---|---|
| Age (years) | 14.4 ± 1.1 (12.4–15.7) | 14.4 ± 1.3 (12.4–15.7) | 14.5 ± 0.9 (13.3–15.8) | 0.43 |
| Height (cm) | 161.9 ± 9.9 (143–182) | 164.9 ± 10.7 (143–182) | 157.4 ± 7.3 (145–165) | 0.05 |
| Weight (kg) | 52.8 ± 12.5 (33–74.2) | 55.5 ± 12.9 (41.3–74.2) | 48.9 ± 11.9 (33–63) | 0.29 |
| BMI (kg/m2) | 20 ± 3.5 (14.8–25.4) | 20.3 ± 3.6 (14.8–25.4) | 19.5 ± 3.8 (15.7–24.3) | 0.11 |
| Before | After | Change (%) | Mean Difference | p-Value | |
|---|---|---|---|---|---|
| Dom Hand grip (kg) | 24 ± 8.6 | 28.1 ± 9.2 | 17 | 4.1 | <0.001 |
| N-Dom Hand grip (kg) | 21.9 ± 7.9 | 26.6 ± 9.2 | 21.4 | 4.7 | <0.001 |
| Dom Biceps brachii (N) | 118.1 ± 26.3 | 139.5 ± 37.8 | 18.1 | 21.4 | <0.001 |
| N-Dom Biceps brachii (N) | 116.7 ± 27.2 | 132.4 ± 26.4 | 13.4 | 15.7 | <0.001 |
| Dom Quadriceps fem (N) | 160.5 ± 40.8 | 204 ± 48.7 | 27.4 | 44 | <0.001 |
| N-Dom Quadriceps fem (N) | 152.8 ± 48.3 | 184.9 ± 44.1 | 21 | 32.1 | <0.001 |
| Dom Single-heel rise (rep) | 10.4 ± 7.5 | 16 ± 8.3 | 53.8 | 5.6 | 0.018 |
| N-Dom Single-heel rise (rep) | 9.2 ± 6.3 | 16.6 ± 8.1 | 80.4 | 7.4 | <0.001 |
| After | After 6 m | Change (%) | Mean Difference | p-Value | |
|---|---|---|---|---|---|
| Dom Hand grip (kg) | 28.1 ± 9.2 | 29.7 ± 10 | 5.7 | 1.6 | ns |
| N-Dom Hand grip (kg) | 26.6 ± 9.2 | 27.8 ± 8.8 | 4.5 | 1.2 | ns |
| Dom Biceps brachii (N) | 139.5 ± 37.8 | 145.5 ± 47.1 | 4.3 | 6 | ns |
| N-Dom Biceps brachii (N) | 132.4 ± 26.4 | 138.5 ± 43.5 | 4.6 | 6.1 | ns |
| Dom Quadriceps fem (N) | 204 ± 48.7 | 189.5 ± 49.4 | −9.2 | −14.5 | ns |
| N-Dom Quadriceps fem (N) | 184.9 ± 44.1 | 188.6 ± 49.2 | 2 | 3.7 | ns |
| Dom Single-heel rise (rep) | 16 ± 8.3 | 18 ± 7 | 12.5 | 2 | ns |
| N-Dom Single-heel rise (rep) | 16.6 ± 8.1 | 20.7 ± 7.1 | 29.3 | 4.1 | ns |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ferrer-Sargues, F.J.; Peiró-Molina, E.; Cebrià i Iranzo, M.À.; Carrasco Moreno, J.I.; Cano-Sánchez, A.; Vázquez-Arce, M.I.; Insa Albert, B.; Salvador-Coloma, P. Effects of Cardiopulmonary Rehabilitation on the Muscle Function of Children with Congenital Heart Disease: A Prospective Cohort Study. Int. J. Environ. Res. Public Health 2021, 18, 5870. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115870
Ferrer-Sargues FJ, Peiró-Molina E, Cebrià i Iranzo MÀ, Carrasco Moreno JI, Cano-Sánchez A, Vázquez-Arce MI, Insa Albert B, Salvador-Coloma P. Effects of Cardiopulmonary Rehabilitation on the Muscle Function of Children with Congenital Heart Disease: A Prospective Cohort Study. International Journal of Environmental Research and Public Health. 2021; 18(11):5870. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115870
Chicago/Turabian StyleFerrer-Sargues, Francisco José, Esteban Peiró-Molina, Maria Àngels Cebrià i Iranzo, José Ignacio Carrasco Moreno, Ana Cano-Sánchez, María Isabel Vázquez-Arce, Beatriz Insa Albert, and Pablo Salvador-Coloma. 2021. "Effects of Cardiopulmonary Rehabilitation on the Muscle Function of Children with Congenital Heart Disease: A Prospective Cohort Study" International Journal of Environmental Research and Public Health 18, no. 11: 5870. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115870