
Occupational Disease as the Bane of Workers’ Lives: A Chronological Review of the Literature and Study of Its Development in Slovakia. Part 1


Abstract
:1. Introduction
2. Materials and Methods
2.1. General Overview
2.2. Data Sources and Evaluation Methods
3. Results and Discussion
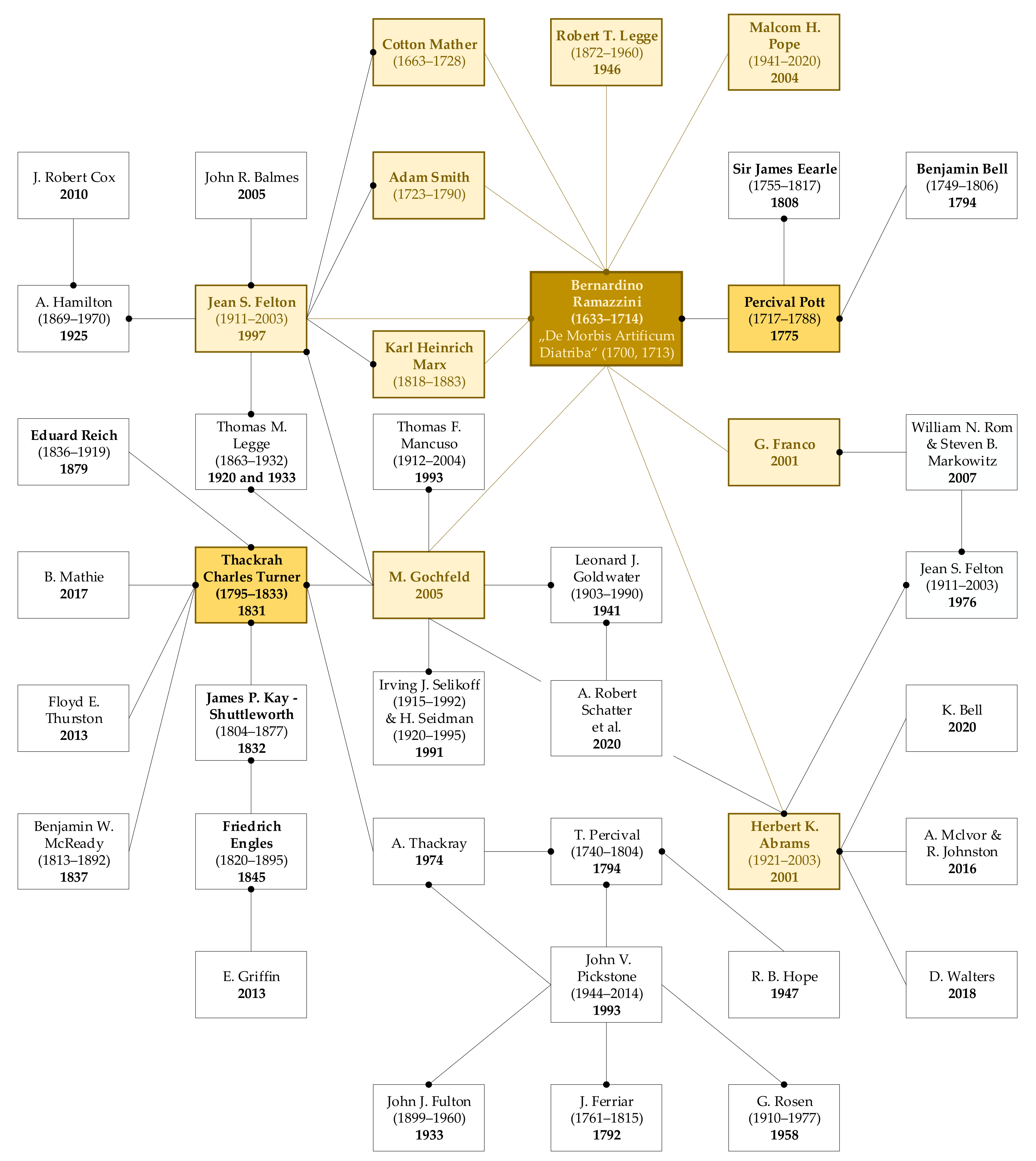
3.1. Chronological Review of the Literature Occupational Diseases
3.1.1. The 18th Century
3.1.2. The 19th Century
3.1.3. The 20th Century
3.2. Chronological Review of the List of Occupational Diseases Recommended by the International Labour Organization
3.2.1. The Era of Industrial Poisoning
3.2.2. Expansion of the ILO List of Occupational Diseases
3.2.3. Further Updates to the ILO List Appended to R194
3.3. Development of Occupational Diseases in Slovakia
3.3.1. Legislation
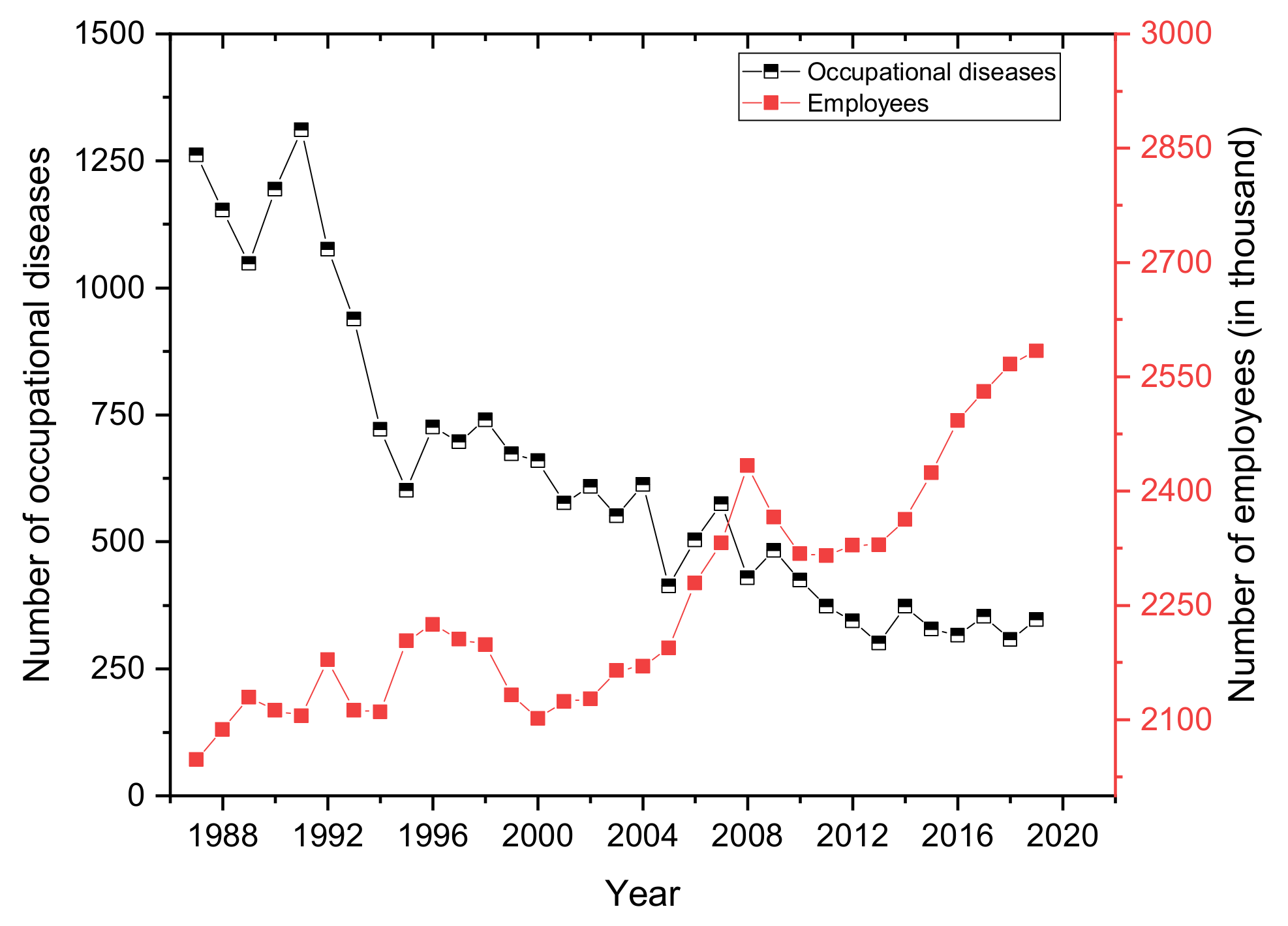
3.3.2. Development of the Incidence of Occupational Disease in Slovakia from 1987 to 2019
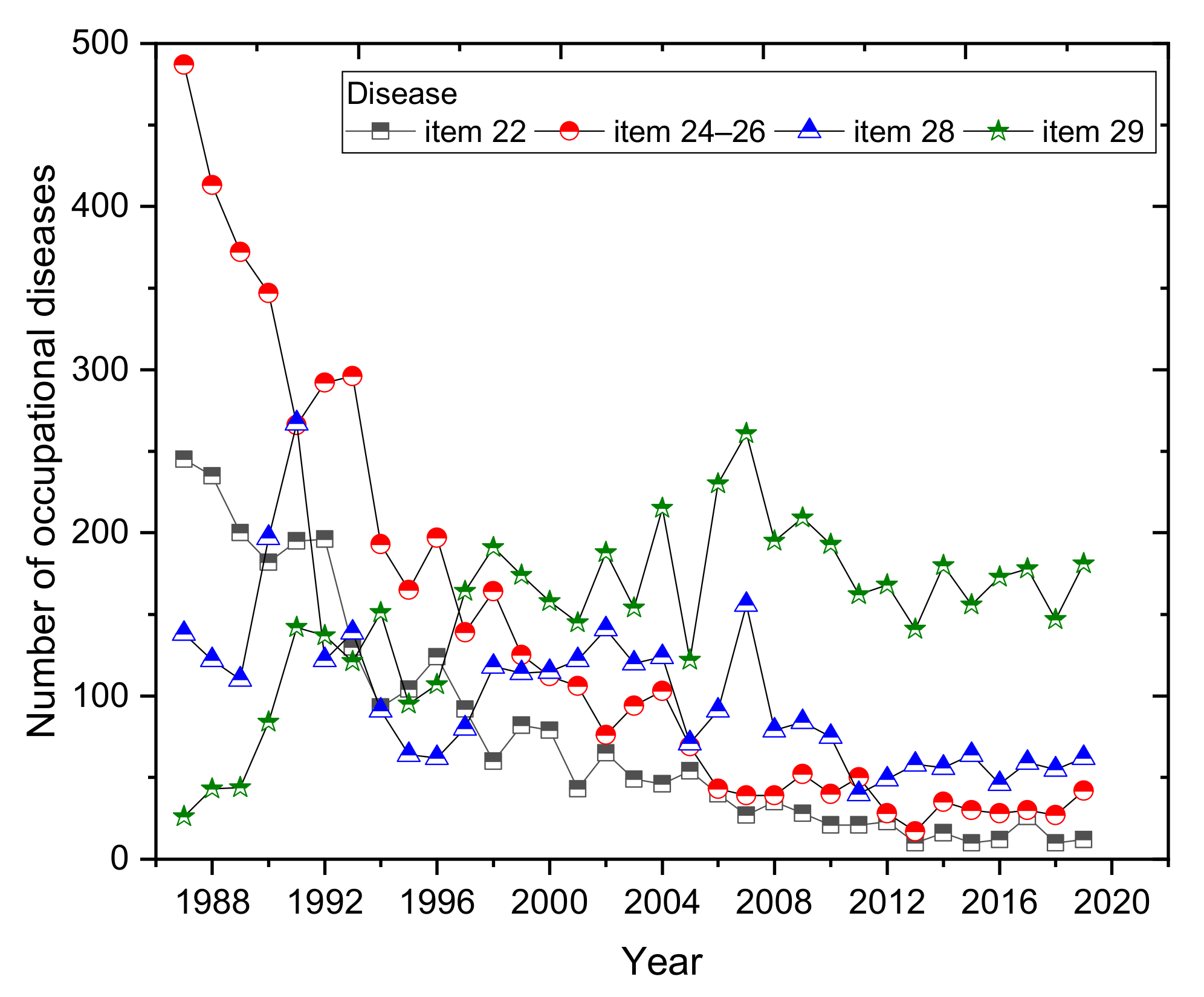
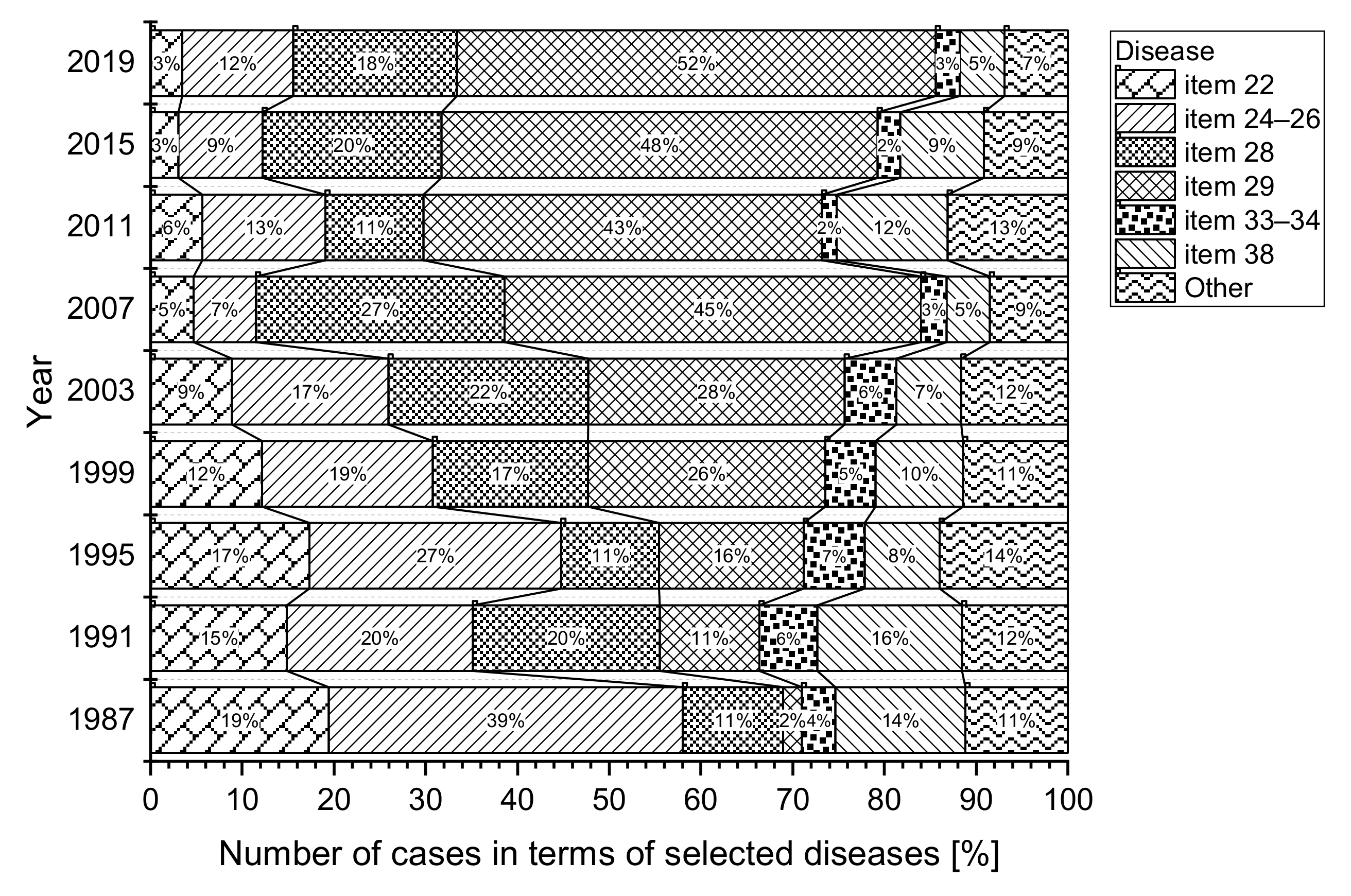
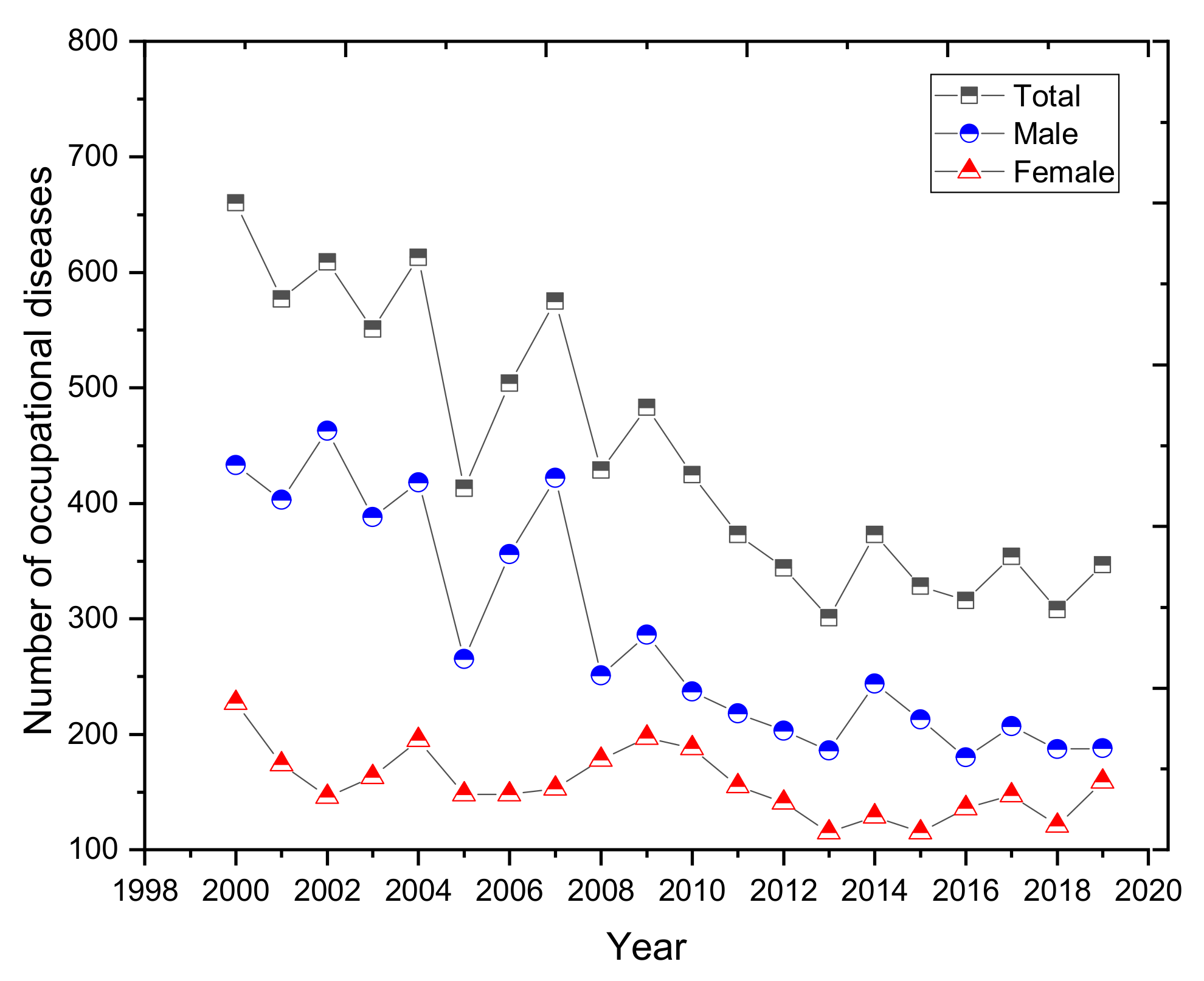
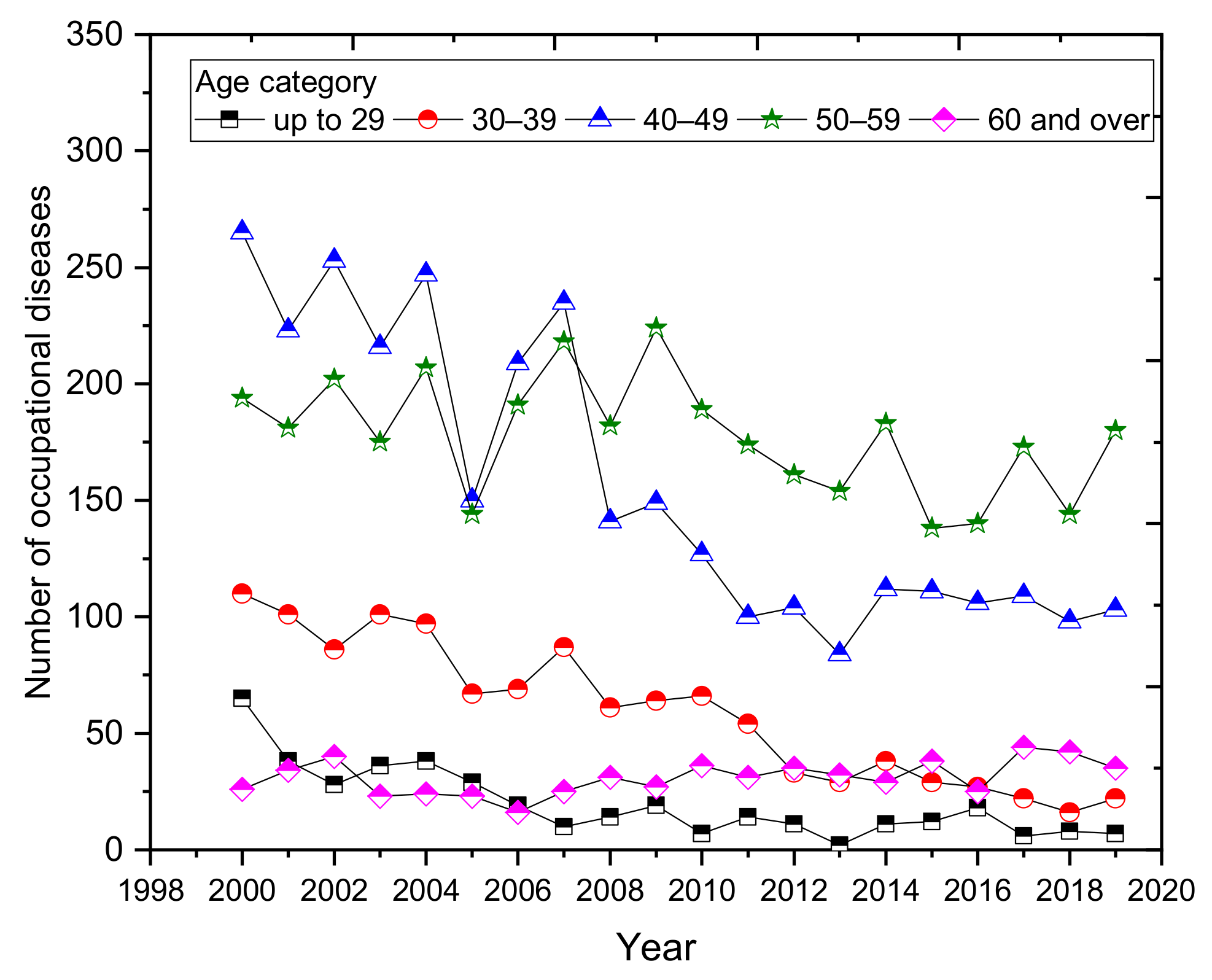
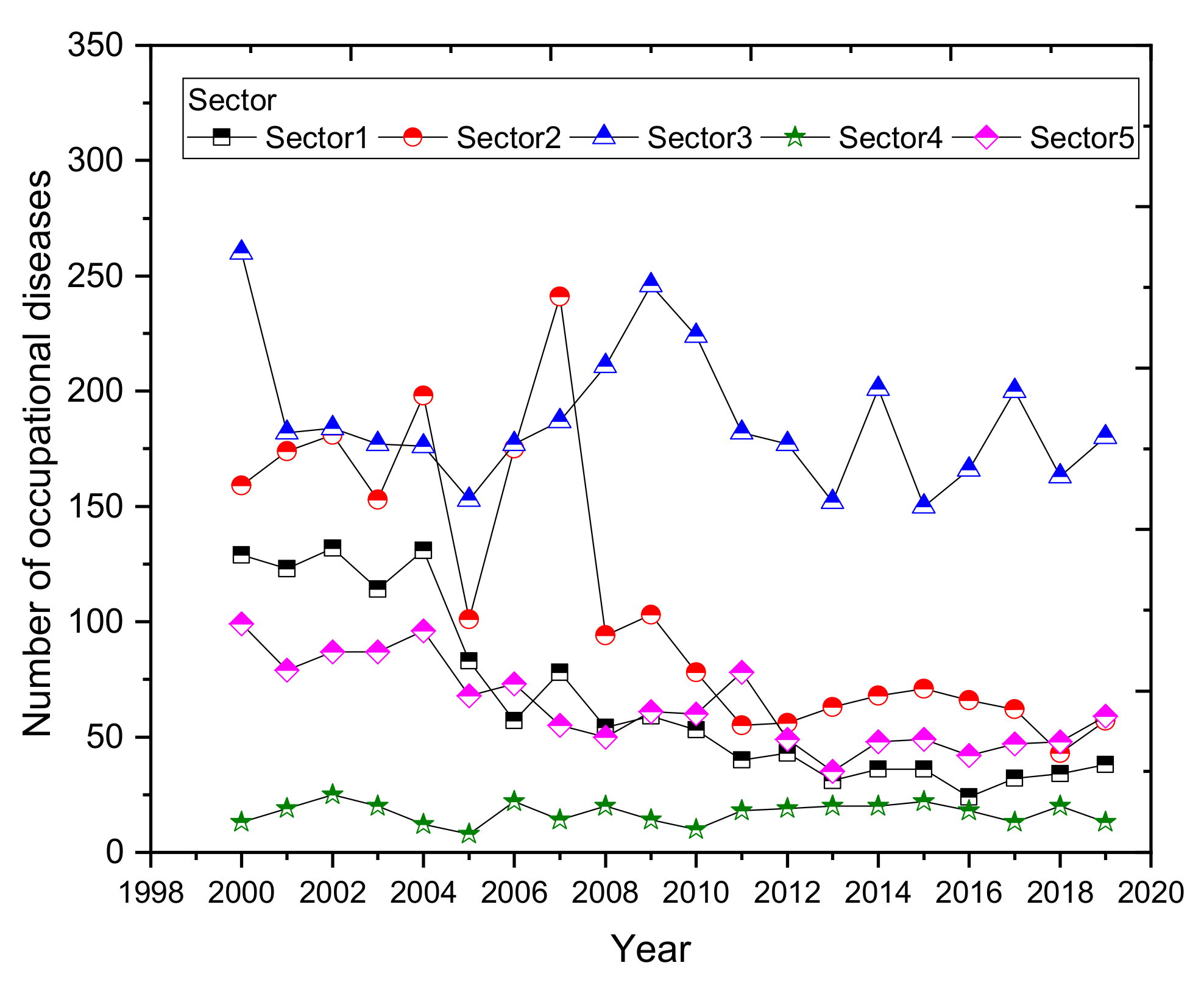
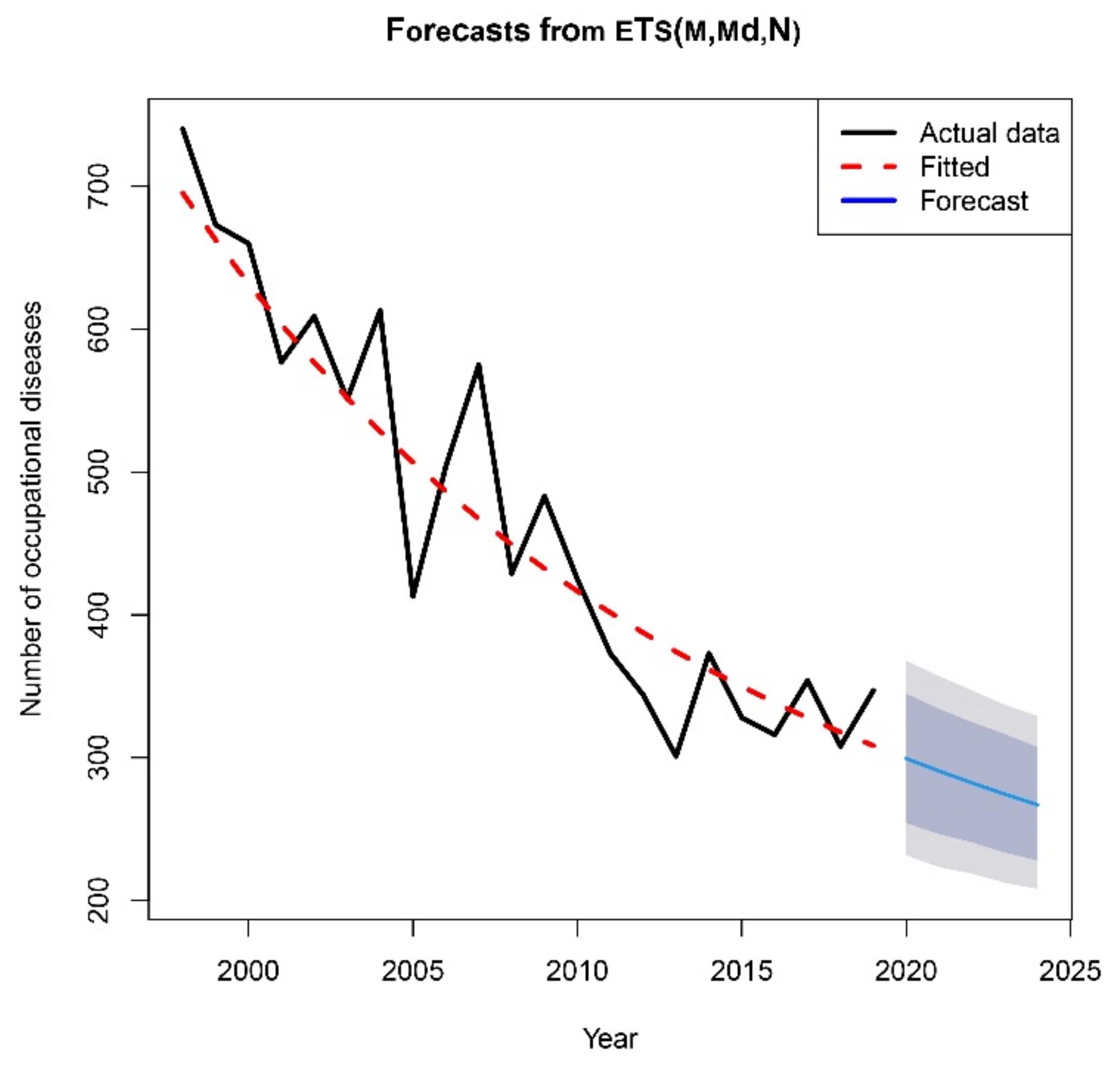
3.3.3. Analysis of the Development of Occupational Diseases in Slovakia over the Last 20 Years
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fellone, L.; Battista, G. Brief History of Occupational Health in Italy. Arch. Environ. Occup. Health 2019, 74, 42–49. [Google Scholar] [CrossRef]
- Abrams, H.K. A Short History of Occupational Health. J. Public Health Policy 2001, 22, 34–80. [Google Scholar] [CrossRef]
- Belkić, K.; Nedić, O. Occupational Medicine: Then and Now: Where we Could go From Here. Med. Pregl. 2014, 67, 139–148. [Google Scholar] [CrossRef] [PubMed]
- Baxter, P.J.; Aw, T.-C.; Cockcroft, A.; Durrington, P.; Harrington, J.M. Hunter’s Diseases of Occupations; Taylor & Francis Group: Abingdon, UK, 2010; pp. 3–33. [Google Scholar]
- Gochfeld, M. Chronologic History of Occupational Medicine. J. Occup. Environ. Med. 2005, 47, 96–114. [Google Scholar] [CrossRef]
- Waldron, T. Thomas Morison Legge (1863–1932): The First Medical Factory Inspector. J. Med. Biogr. 2004, 12, 202–209. [Google Scholar] [CrossRef] [PubMed]
- Pope, M.H. Bernardino Ramazzini: The Father of Occupational Medicine. Spine (Phila. Pa. 1976) 2004, 29, 2335–2338. [Google Scholar] [CrossRef] [PubMed]
- LaDou, J. The Rise and Fall of Occupational Medicine in the United States. Am. J. Prev. Med. 2002, 22, 285–295. [Google Scholar] [CrossRef]
- Brhel, P. Occupational Respiratory Diseases in the Czech Republic. Ind. Health 2003, 41, 121–123. [Google Scholar] [CrossRef] [Green Version]
- Kudász, F.; Nagy, K.; Nagy, I. Occupational diseases in Belgium, the Czech Republic and Hungary—A Comparison. Cent. Eur. J. Occup. Environ. Med. 2017, 23, 32–49. [Google Scholar]
- Gómez, M.G.; López, R.C.; Ortiz, Z.H.; Soria, F.S. Differences in the Recognition of Occupational Diseases by Sex, Occupation and Business Activity in Spain (1990–2009). Rev. Esp. Salud Publica 2017, 91, 1–12. [Google Scholar]
- Świątkowska, B.; Szeszenia-Dąbrowska, N. Long-term Epidemiological Observation of Asbestos-related Diseases in Poland, 1970–2015. Occup. Med. (Chic. Ill.) 2017, 67, 182–187. [Google Scholar] [CrossRef] [Green Version]
- Oksa, P.; Sauni, R.; Talola, N.; Virtanen, S.; Nevalainen, J.; Saalo, A.; Uitti, J. Trends in Occupational Diseases in Finland, 1975–2013: A Register Study. BMJ Open 2019, 9, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Das, B. Prevalence of Work-related Occupational Injuries and its Risk Factors Among Brickfield Workers in West Bengal, India. Int. J. Ind. Ergon. 2020, 80, 1–11. [Google Scholar] [CrossRef]
- Boden, L.I. The Occupational Safety and Health Administration at 50-the Failure to Improve Workers’ Compensation. Am. J. Public Health 2020, 110, 638–639. [Google Scholar] [CrossRef]
- Rushton, L.; Hutchings, S.J.; Fortunato, L.; Young, C.; Evans, G.S.; Brown, T. Occupational Cancer Burden in Great Britain. Br. J. Cancer 2012, 107, S3–S7. [Google Scholar] [CrossRef] [PubMed]
- Mehrdad, R. Introduction to Occupational Health Hazards. Int. J. Occup. Environ. Med. 2020, 11, 59–60. [Google Scholar] [CrossRef]
- Rom, W.N.; Markowitz, S.B. Environmental and Occupational Medicine; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2007; pp. 3–9. [Google Scholar]
- Quick, J.C.E.; Tetrick, L.E. Handbook of Occupational Health Psychology; American Psychological Association: Washington, DC, USA, 2011. [Google Scholar]
- Carder, M.; Bensefa-Colas, L.; Mattioli, S.; Noone, P.; Stikova, E.; Valenty, M.; Telle-Lamberton, M. A review of Occupational Disease Surveillance Systems in Modernet Countries. Occup. Med. 2015, 65, 615–625. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nicholson, P.J. Occupational Health in the European Union. Occup. Med. (Chic. Ill.) 2002, 52, 80–84. [Google Scholar] [CrossRef] [Green Version]
- Rushton, L. The Global Burden of Occupational Disease. Curr. Environ. Heal. Rep. 2017, 4, 340–348. [Google Scholar] [CrossRef] [Green Version]
- Moyo, D.; Zungu, M.; Kgalamono, S.; Mwila, C.D. Review of Occupational Health and Safety Organization in Expanding Economies: The Case of Southern Africa. Ann. Glob. Health 2015, 81, 495–502. [Google Scholar] [CrossRef]
- Bianchini, A.; Donini, F.; Pellegrini, M.; Saccani, C. An Innovative Methodology for Measuring the Effective Implementation of an Occupational Health and Safety Management System in the European Union. Saf. Sci. 2017, 92, 26–33. [Google Scholar] [CrossRef]
- Ning, H.; Zhou, Y.; Zhou, Z.; Cheng, S.; Huang, R. Challenges to Improving Occupational Health in China. Occup. Environ. Med. 2017, 74, 924–925. [Google Scholar] [CrossRef]
- Münsterberg, H. Psychology and Industrial Efficiency; A&C Black: London, UK, 1913; pp. 141–221. [Google Scholar]
- Aitken, H.G.J. Frederick Taylor: A Study in Personality and Innovation. Bus. Hist. Rev. 1971, 45, 129–131. [Google Scholar] [CrossRef]
- Witzel, M. Frank Bunker Gilbreth (1868–1924) Lillian Gilbreth (1878–1972). Fifty Key Figures in Management; Routledge: London, UK, 2003; pp. 140–145. [Google Scholar]
- Bourke, H. Mayo, George Elton (1880–1949). In Australian Dictionary of Biography; Melbourne University Publishing: Melbourne, Australia, 1986. [Google Scholar]
- Pracovný Stres Ovplyvňuje Výkon Dvoch Tretín Zamestnancov na Slovensku. Available online: https://www.grafton.sk/ (accessed on 25 May 2021).
- Legáth, Ľ.; Buchancová, J.; Kabátová, Z.; Kurča, E.; Lacko, M.; Turčanová Koprušáková, M. Pracovné Lekárstvo. Vybrané Kapitoly I; Osveta: Martin, Slovakia, 2020; p. 5. [Google Scholar]
- Buchancová, J. Pracovné Lekárstvo a Toxikológia, 1st ed.; Osveta: Martin, Slovakia, 2003; pp. 15–46. [Google Scholar]
- International Labour Organization. ILO List of Occupational Diseases Available (Revised 2010); International Labour Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Occupational and Work-Related Diseases. Available online: https://www.who.int (accessed on 20 April 2021).
- OSHA Laws & Regulations. OSH Act of 1970. Available online: https://www.osha.gov/laws-regs/oshact/completeoshact (accessed on 22 April 2021).
- Work-Related Diseases. Available online: https://osha.europa.eu/en/themes/work-related-diseases (accessed on 20 April 2021).
- Zákon č. 461/2003 Z. z., o Sociálnom Poistení. Republic of Slovakia: Bratislava, Slovakia, 2003. (In Slovak)
- European Framework Directive 89/391/EEC on the Introduction of Measures to Encourage Improvements in the Safety and Health of Workers at Work; European Agency for Safety and Health at Work: Brussels, Belgium, 1989.
- Zákon č. 311/2011 Z. z., Zákonník Práce. Republic of Slovakia: Bratislava, Slovakia, 2011. (In Slovak)
- Zákon č. 355/2007 Z. z., o Ochrane, Podpore a Rozvoji Verejného Zdravia a o Zmene a Doplnení Niektorých Zákonov; Republic of Slovakia: Bratislava, Slovakia, 2007. (In Slovak)
- Montgomery, D.C.; Jennings, C.L.; Kulahci, M. Wiley Series in Probability and Statistics; John Wiley: Hoboken, NJ, USA, 2015; pp. 25–96. [Google Scholar]
- Hyndman, R.J.; Athanasopoulos, G. Forecasting: Principles and Practice; OTexts: Melbourne, VIC, Australia, 2018; pp. 237–284. [Google Scholar]
- Lumnitzer, E.; Piňosová, M.; Andrejiová, M.; Hricová, B. Methodology of Complex Health Risk Assessment in Industry II; MUSKA sp. z o.o.: Zręcin, Poland, 2013; pp. 15–29. (In Slovak) [Google Scholar]
- Ramazzini, B. De Morbis Artificum Diatriba, 1700; Fundacentro: São Paulo, Brazil, 2000. [Google Scholar]
- Felton, J.S. History of occupational medicine. The Heritage of Bernardino Ramazzini. Occup. Med. (Chic. Ill.) 1997, 47, 167–179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramazzini, B. Diseases of Workers. Am. J. Public Health 1713, 91. [Google Scholar]
- Araujo-Alvarez, J.M.; Trujillo-Ferrara, J.G. De Morbis Artificum Diatriba 1700–2000. Salud Publica Mex. 2002, 44, 362–370. [Google Scholar] [CrossRef] [PubMed]
- Bartholomew, M. James Lind’s Treatise of the Scurvy (1753). Postgrad. Med. J. 2002, 78, 695–696. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scopoli, G.A. De Hydrargyro Idriensi Tentamina Physico-Chemico-Medica; Press Mark: Venice, Italy, 1761; pp. 109–160. [Google Scholar]
- Percivall, P. Chirurgical Observations Relative to the Cataract, the Polypus of the Nose, the Cancer of the Scrotum, the Different Kinds of Ruptures, and the Mortification of the Toes and Feet; T.J. Carnegy: London, UK, 1775; pp. 1–40. [Google Scholar]
- Plotkin, M. Ben “Catastrofe Morboso de las Minas Mercuriales de la Villa de Almaden del Azogue”(1778) de Jose Pares y Franques. Bull. Hist. Med. 1999, 73, 506–507. [Google Scholar] [CrossRef]
- Thackrah, C.T. The Effects of Arts, Trades, and Professions: And of Civic States and Habits of Living, on Health and Longevity: With Suggestions for the Removal of Many of the Agents which Produce Disease, and Shorten and Duration of Life; Longman, Rees, Orme, Brown, Green, & Longman: London, UK, 1832; pp. 84–89. [Google Scholar]
- Mathie, B. Charles Turner Thackrah, 1795-1833, “The Father of Occupational Medicine”. Occup. Med. (Chic. Ill.) 2017, 67, 251–253. [Google Scholar] [CrossRef] [Green Version]
- Melicow, M.M. Percivall Pott (1713–1788) 200th Anniversary of First Report of Occupation-Induced Cancer of Scrotum in Chimney Sweepers (1775). Urology 1975, 6, 745–749. [Google Scholar] [CrossRef]
- Bell, B. A System of Surgery; Ch. Elliot & G. Robinson: Edinburgh, UK.
- Harrison, E. Pathological and Practical Observations on Spinal Diseases. Oxford Univ. 1827, 297. [Google Scholar]
- Kay-Shuttleworth, J.P. The Moral and Physical Condition of the Working Classes Employed in the Cotton Manufacture in Manchester. Biol. Cent. 1832, 2, 120. [Google Scholar]
- Koch, R. Die Ätiologie der Milzbrand-Krankheit, begründet auf die Entwicklungsgeschichte des Bacillus Anthracis; (1876); Schwalbe, J., Ed.; Robert Koch-Institut: Berlin, Germany, 2010; pp. 1–23. [Google Scholar]
- Blevins, S.M.; Bronze, M.S. Robert Koch and the ‘Golden Age’ of Bacteriology’. Int. J. Infect. Dis. 2010, 14, 744–751. [Google Scholar] [CrossRef] [Green Version]
- Sowards, W. Louis Pasteur, Anthrax, and Rabies. Available online: https://www.passporthealthusa.com/2015/08/louis-pasteur-anthrax-and-rabies/ (accessed on 6 April 2021).
- McCready, B.W. On the Influence of Trades, Professions, and Occupations in the United States, in the Production of Disease (Reprinted 1972); Arno Press: New York, NY, USA, 1837; pp. 1–129. [Google Scholar]
- Chadwick, E. Report to Her Majesty’s Principal Secretary of State for the Home Department, from the Poor Law Commissioners, on an Inquiry into the Sanitary Condition of the Labouring Population of Great Britain; HM Stationery Office: London, UK, 1842; pp. 5–23. [Google Scholar]
- Engels, F. The Condition of the Working Class in England (Reprinted 1969); Panther Books: London, UK, 1845; pp. 2–19. [Google Scholar]
- Virchow, R.C. Report on the Typhus Epidemic in Upper Silesia. 1848. Am. J. Public Health 2006, 96, 2102–2105. [Google Scholar] [CrossRef] [PubMed]
- Ireland, G.H. The Preventable Causes of Disease, Injury, and Death in American Manufactories and Workshops, and the Best Means and Appliances for Preventing and Avoiding Them; Republican Press: Concord, NH, USA, 1886; pp. 1–19. [Google Scholar]
- Legge, T.M.; Goadby, K.W. Lead Poisoning and Lead Absorption: The Symptoms, Pathology and Prevention, with Special Reference to their Industrial Origin and an Account of the Principle Processes Involving Risk. Am. J. Sociol. 1913, 18, 336. [Google Scholar]
- John, B. Andrews, 1880-1943. In Social Service Review; JSTOR: New York, NY, USA, 1943; Volume 17, pp. 97–98. Available online: www.jstor.org/stable/30000928 (accessed on 30 May 2021).
- Andrews, J.B. Anthrax as an Occupational Disease. Am. J. Public Health Nations Health 1917, 155. [Google Scholar]
- Saposs, D.J.; Sumner, H.L.; Mittelman, E.B.; Hoagland, H.E.; Andrews, J.B.; Andrews, J.B.; Perlman, S. History of Labor in the United States; Macmillan: Basingstoke, UK, 1918; Volume 32, pp. 667–673. [Google Scholar]
- Cox, R. Environmental Communication and the Public Sphere; Sage Publications: Thousand Oaks, CA, USA, 2010; pp. 46–53. [Google Scholar]
- Hamilton, A. Industrial Poisons in the United States. Nature 1925, 116. [Google Scholar] [CrossRef]
- Hamilton, A.; Hardy, H.L. Industrial Toxicology; Wiley: Hoboken, NJ, USA, 1949; pp. 200–360. [Google Scholar]
- Hamilton, A. Exploring the Dangerous Trades: The Autobiography of Alice Hamilton; Little, Brown and Company: Boston, MA, USA, 1943; pp. 3–38. [Google Scholar]
- Sicherman, B. Alice Hamilton: A Life in Letters; University of Illinois Press: Champaign, IL, USA, 2003; pp. 11–33. [Google Scholar]
- Hueper, W.C. Occupational Tumors and Allied Diseases; Charles C. Thomas: Springfield, IL, USA; Baltimore, MD, USA, 1942; pp. 154–169. [Google Scholar]
- Hueper, W.C. Silicosis, Asbestosis, and Cancer of the Lung. Am. J. Clin. Pathol. 1955, 25, 1388–1390. [Google Scholar] [CrossRef] [Green Version]
- Selikoff, I.J.; Hammond, E.C.; Churg, J. Asbestos Exposure, Smoking, and Neoplasia. JAMA J. Am. Med. Assoc. 1968, 204, 106–112. [Google Scholar] [CrossRef]
- Hueper, W.C.; Conway, W.D. Chemical Carcinogenesis and Cancers; Charles C. Thomas: Springfield, IL, USA, 1964; pp. 10–15. [Google Scholar]
- Hueper, W.C. Occupational and Environmental Cancers of the Urinary System; Yale University Press: New Haven, CT, USA, 1969; pp. 29–88. [Google Scholar]
- Kehoe, R.A. Occupational Medicine and Public Health. Public Health Rep. 1961, 76, 645–649. [Google Scholar] [CrossRef]
- Kehoe, R.A. Experimental Studies on the Inhalation of Lead by Human Subjects. Pure Appl. Chem. 1961, 3, 129–144. [Google Scholar] [CrossRef]
- Needleman, H.L. Clair Patterson and Robert Kehoe: Two views of Lead Toxicity. Environ. Res. 1998, 78. [Google Scholar] [CrossRef]
- Nriagu, J.O. Clair Patterson and Robert Kehoe’s Paradigm of “Show Me the Data” on Environmental Lead Poisoning. Environ. Res. 1998, 78. [Google Scholar] [CrossRef]
- Seidman, H.; Selikoff, I.J. Decline in Death Rates among Asbestos Insulation Workers 1967–1986 Associated with Diminution of Work Exposure to Asbestos. Ann. N. Y. Acad. Sci. 1990, 609, 300–317. [Google Scholar] [CrossRef]
- Selikoff, I.J. Asbestos Disease—1990–2020: The Risks of Asbestos Risk Assessment. Toxicol. Ind. Health 1991, 7, 117–127. [Google Scholar] [CrossRef] [PubMed]
- LaDou, J. Jean Spencer Felton. Occup. Med. (Chic. Ill.) 2004, 54, 268–269. [Google Scholar] [CrossRef] [Green Version]
- Felton, J.S.; Kennedy, J.F. 200 Years of Occupational Medicine in the U.S. J. Occup. Environ. Med. 1976, 18, 809–817. [Google Scholar] [CrossRef]
- Felton, J.S. The Occupational History: A Neglected Area in the Clinical History. J. Fam. Pract. 1980, 11, 33–39. [Google Scholar] [PubMed]
- Felton, J.S. Occupational Medicine-epitomes of Progress: Asbestos-related Diseases. West. J. Med. 1980, 133, 149–150. [Google Scholar] [PubMed]
- Felton, J.S. Organization and Operation of an Occupational Health Program. J. Occup. Environ. Med. 1964, 6, 132–151. [Google Scholar] [CrossRef] [PubMed]
- Felton, J.S.; Perkins, D.C.; Lewin, M. A Survey of Medicine and Medical Practice for the Rehabilitation Counselor; US Department of Health, Education, and Welfare, Vocational Rehabilitation Administration: Washington, DC, USA, 1966; pp. 4–86. [Google Scholar]
- Felton, J.S. Radiographic Search for Asbestos-related Disease in a Naval Shipyard. Ann. N. Y. Acad. Sci. 1979, 330, 341–352. [Google Scholar] [CrossRef] [PubMed]
- Felton, J.S. Classical Syndromes in Occupational Medicine: Phosphorus Necrosis—A Classical Occupational Disease. Am. J. Ind. Med. 1982, 3, 77–120. [Google Scholar] [CrossRef]
- Tannen, T. Obituary: Thomas F. Mancuso. Lancet 2004, 364, 410. [Google Scholar] [CrossRef]
- Michaels, D. In Memoriam: Thomas F. Mancuso, MD, MPH 1912–2004. Am. J. Ind. Med. 2005, 47, 1–3. [Google Scholar] [CrossRef]
- Marcuso, T.F.; Hupper, W.C. Occupational Cancer and other Health Hazards in a Chromate Plant: A Medical Appraisal. I. Lung Cancers in Chromate Workers. Ind. Med. Surg. 1951, 20, 358–363. [Google Scholar]
- Marcuso, T.F. Occupational Cancer and other Health Hazards in a Chromate Plant: A Medical Appraisal. II. Clinical and Toxicologic Aspects. Ind. Med. Surg. 1951, 20, 393–407. [Google Scholar]
- Mancuso, T.F. Chromium as an Industrial Carcinogen: Part I. Am. J. Ind. Med. 1997, 31, 129–139. [Google Scholar] [CrossRef]
- Mancuso, T.F. Chromium as an Industrial Carcinogen: Part II. Chromium in Human Tissues. Am. J. Ind. Med. 1997, 31, 140–147. [Google Scholar] [CrossRef]
- Mancuso, T.F.; Stewart, A.; Kneale, G. Radiation Exposures of Hanford Workers Dying from Cancer and other Causes. Health Phys. 1977, 33, 369–385. [Google Scholar] [CrossRef]
- Stockhausen, S. Libellus de Lithargyrii Fumo Noxio Morbifico Eiusque Metallico Frequentiori Morbo, Vulgo Dicto Die Hüttenkatze; Duncker: München, Germany, 1656; pp. 1–133. [Google Scholar]
- Baker, G. An Essay concerning the Cause of the Endemial Colic of Devonshire; Hughes, J., Ed.; GALE: Farmington Hills, MI, USA, 1767; pp. 1–60. [Google Scholar]
- Shattuck, L. Report of the Sanitary Commission of Massachusetts; Dutt. Wentworth State Printers: Boston, MA, USA, 1850. [Google Scholar]
- Oliver, T. Dangerous Trades: The Historical, Social, and Legal, Aspects of Industrial Occupations as Affecting health; J. Murray: London, UK, 1902; pp. 1–23. [Google Scholar]
- Legge, T.M. Chronic Benzol Poisoning. J. Ind. Hyg. 1919, 1920, 539–541. [Google Scholar]
- Legge, T.M. Industrial Diseases under the Medieval Trade Guilds. J. Ind. Hyg. 1920, 1, 476–477. [Google Scholar]
- Legge, T.M. Charles Turner Thackrah: A Pioneer in Industrial Hygiene. J. Ind. Hyg. 1920, 1, 578–581. [Google Scholar]
- Legge, T.M. Industrial Maladies. Br. Med. J. 1929, 1, 467–468. [Google Scholar]
- Legge, T.M. A Historical Background of Industrial Hygiene. Am. Ind. Hyg. Assoc. Q. 1946, 7, 5–8. [Google Scholar] [CrossRef]
- Eastman, C. Work-Accidents and the Law; Charities Publication Committee: New York, NY, USA, 1910; Volume 2, p. 458. [Google Scholar]
- Fitch, J.A. The Steel Workers (Reprinted 2014); University of Pittsburgh Press: Pittsburgh, PA, USA, 1910; pp. 1–437. [Google Scholar]
- Thompson, W.G. The Occupational Diseases: Their Causation, Symptoms, Treatment and Prevention; D. Appleton and Company: Boston, MA, USA, 1914; p. 724. [Google Scholar]
- Hamilton, A. A Study of Spastic Anemia in the Hands of Stonecutters. Bull. U. S. Bur. Labor Stat. 1918, 236, 53–66. [Google Scholar]
- Evans, R.D. Radium Poisoning a Review of Present Knowledge. Am. J. Public Heal. Nations Heal. 1933, 23, 1017–1023. [Google Scholar] [CrossRef]
- Hardy, H.L.; Tabershaw, I.R. Delayed Chemical Pneumonitis Occurring in Workers Exposed to Beryllium Compounds. J. Ind. Hyg. Toxicol. 1946, 28, 197–211. [Google Scholar] [PubMed]
- Goldwater, L.J. Disturbances in the Blood Following Exposure to Benzol. J. Lab. Clin. Med. 1941, 26, 957–973. [Google Scholar] [CrossRef]
- Goldwater, L.J. Strengthening Environmental Standards. J. Occup. Environ. Med. 1976, 18. [Google Scholar] [CrossRef]
- Selikoff, I.J.; Seidman, H. Asbestos-Associated Deaths among Insulation Workers in the United States and Canada, 1967–1987. Ann. N. Y. Acad. Sci. 1991, 643, 1–14. [Google Scholar] [CrossRef]
- Kim, E.-A.; Kang, S.-K. Historical Review of the List of Occupational Diseases Recommended by the International Labour Organization (ILO). Ann. Occup. Environ. Med. 2013, 25, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Walters, D.; Work, C. An International Comparison of Occupational Disease and Injury Compensation Schemes; Cardiff University: Cardiff, UK, 2007; pp. 1–49. [Google Scholar]
- Parsons, C. Liability Rules, Compensation Systems and Safety at Work in Europe. Geneva Pap. Risk Insur. 2002, 27, 358–382. [Google Scholar] [CrossRef]
- International Labour Office. The Labour Provisions of the Peace Treaties; International Labour Office: Geneva, Switzerland, 1920. [Google Scholar]
- Foner, P.S. History of the Labor Movement in the United States. Am. Hist. Rev. 1990, 95, 273. [Google Scholar] [CrossRef]
- R003—Anthrax Prevention Recommendation, 1919 (No. 3); International Labour Organization: Geneva, Switzerland, 1919.
- R004—Lead Poisoning (Women and Children) Recommendation, 1919 (No. 4); International Labour Organization: Geneva, Switzerland, 1919.
- Brook, I. Spores, Plagues and History: The Story of Anthrax. BMJ 2004, 329, 577. [Google Scholar] [CrossRef] [Green Version]
- Turnbull, P.C.B. Introduction: Anthrax History, Disease and Ecology. Curr. Top. Microbiol. Immunol. 2002, 271, 1–19. [Google Scholar] [CrossRef]
- Ameille, J. Hunters Diseases of Occupations. 10th Edition. Eur. Respir. Rev. 2011, 20, 302. [Google Scholar]
- Netolitzky, A. Hygiene der Textilindustrie. Handbuch der Hygiene. Ind. Hyg. 1897, 8, 1102–1103. [Google Scholar]
- Rohé, G.H. The Hygiene of Occupations. Public Health Pap. Rep. 1884, 10, 165–173. [Google Scholar] [PubMed]
- Fassett, D.W. Organic Acids, Anhydrides, Lactones, Acid Halides and Amides, Thioacids in Industrial Hygiene and Toxicology; Wiley-Interscience: New York, NY, USA, 1811. [Google Scholar]
- C018—Workmen’s Compensation (Occupational Diseases) Convention, 1925 (No. 18); International Labour Organization: Geneva, Switzerland, 1925.
- C042—Workmen’s Compensation (Occupational Diseases) Convention (Revised), 1934 (No. 42); International Labour Organization: Geneva, Switzerland, 1934.
- C121—Employment Injury Benefits Convention, 1964 (No. 121); International Labour Organization: Geneva, Switzerland, 1964.
- Gawkrodger, D.J. Occupational Skin Cancers. Occup. Med. (Chic. Ill.) 2004, 54, 458–463. [Google Scholar] [CrossRef] [Green Version]
- Fritschi, L.; Driscoll, T. Cancer Due to Occupation in Australia. Aust. N. Z. J. Public Health 2006, 30, 213–219. [Google Scholar] [CrossRef]
- Staloff, R.T.; Sataloff, J. Occupational Hearing Loss; CRC Press: Boca Raton, FL, USA, 2006; Volume 3. [Google Scholar]
- Kryter, K.D. The Effects of Noise on Man. J. Speech Hear. Disord. Monogr. Suppl. 1950, 1. [Google Scholar] [CrossRef]
- Thurston, F.E. The Worker’s Ear: A History of Noise-induced Hearing Loss. Am. J. Ind. Med. 2013, 56, 367–377. [Google Scholar] [CrossRef] [PubMed]
- Schilling, R.S.F.; Lond, M.D.; Reader, D.I.H. Byssinosis in Cotton and other Textile Workers. Lancet 1956, 271, 261–265. [Google Scholar] [CrossRef]
- Ratifications of C121—Employment Injury Benefits Convention, 1964 [Schedule I Amended in 1980] (No. 121); International Labour Organization: Geneva, Switzerland, 1964.
- Kang, S.K.; Ahn, Y.S.; Chung, H.K. Occupational Cancer in Korea in the 1990s. Korean Med. J. Inf. 2001, 13, 351–359. [Google Scholar] [CrossRef]
- Bulbulyan, M.; Zahm, S.H.; Zaridze, D.G. Occupational Cancer Mortality among Urban Women in the Former USSR. Cancer Causes Control 1992, 3, 299–307. [Google Scholar] [CrossRef] [PubMed]
- González, C.A.; Agudo, A. Occupational Cancer in Spain. Environ. Health Perspect. 1999, 107, 273–277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brüske-Hohlfeld, I. Occupational Cancer in Germany. Environ. Health Perspect. 1999, 107, 253–258. [Google Scholar] [CrossRef] [Green Version]
- Teschke, K.; Barroetavena, M.C. Occupational Cancer in Canada: What do we know? CMAJ 1992, 147, 1501–1507. [Google Scholar]
- Aubrun, J.C.; Binet, S.; Bozec, C.; Brochard, P.; Dimerman, S.; Fontaine, B. Occupational Cancer in France: Epidemiology, Toxicology, Prevention, and Compensation. Environ. Health Perspect. 1999, 107, 245–252. [Google Scholar] [CrossRef]
- Merler, E.; Vineis, P.; Alhaique, D.; Miligi, L. Occupational cancer in Italy. Environ. Health Perspect. 1999, 107. [Google Scholar]
- 90/326/EEC: European Schedule of Occupational Diseases; European Commission: Brussels, Belgium, 1990.
- 2003/670/EC: European Schedule of Occupational Diseases; European Commission: Brussels, Belgium, 2003.
- R194—List of Occupational Diseases Recommendation, 2002 (No. 194); International Labour Organization: Geneva, Switzerland, 2002.
- Recording and Notification of Occupational Accidents and Diseases and ILO List of Occupational Diseases; International Labour Organization: Geneva, Switzerland, 2002.
- MEULOD/2005/10 Meeting of Experts on Updating the List of Occupational Diseases; International Labour Organization: Geneva, Switzerland, 2005.
- GB.307/STM/2/4 Meeting of Experts on the Revision of the List of Occupational Diseases; International Labour Organization: Geneva, Switzerland, 2010.
- MEULOD/2005/1 Report on the Replies to the Questionnaire on the Updating of the “List of Occupational Diseases” Annexed to the List of Occupational Diseases Recommendation, 2002 (No. 194) and on the Amendments to the List of Occupational Diseases Submitted to the Committee on Occupational Accidents and Diseases of the 90th Session of the International Labour Conference in 2002; International Labour Organization: Geneva, Switzerland, 2005.
- MEULOD/2005/3 Technical Backgrounder on the Modified and Newly Introduced Items Proposed to be Included in the Updated List of Occupational Diseases Annexed to the List of Occupational Diseases Recommendation, 2002 (No. 194); International Labour Organization: Geneva, Switzerland, 2005.
- Placitus, S.; Henisch, G. Artzney-Buch Sexti Platonici Philosophi von Vöglen, Wilden und Zamen Thieren: Wie Man Dieselb in der Artzney für Allerhandt Kranckheiten Brauchen Soll; Perna: Basel, Switzerland, 1574. [Google Scholar]
- Placitus, S. Sexti Placiti De Medicamentis ex Animalibus, Libellus; Petreius: Nuremberg, Germany, 1538. [Google Scholar]
- Pekařová, K. Prírodovedné a Lékarske Spolky na Území Slovenska (1850–1918): So Zvláštnym Zreteľom na Zdravotnícko-Medicínsku Tematiku a Biologické Vedy v ich Publikacňých Aktivitách; University Library in Bratislava: Bratislava, Slovakia, 2010; pp. 10–47. [Google Scholar]
- Borguľová, J. Lekár s humoristickým perom—Rodák, na ktorého sa trocha zabúda. Bystrický Permon. 2005, 3, 9. (In Slovak) [Google Scholar]
- Csáky, K. Híres Selmecbányai Tanárok; Lilium Aurum: Dunajská Streda, Slovakia, 2003. [Google Scholar]
- 1/2011 Vestník MZ SR Odborné Usmernenie MZ SR č. OOFŽP-7674/2010, Ktorým sa Upravuje Postup pri Objektivizácii Fyzikálnych Faktorov Životného Prostredia a Pracovného Prostredia; Republic of Slovakia: Bratislava, Slovakia, 2011. (In Slovak)
- Vyhláška č. 448/2007 Z. z., o Podrobnostiach o Faktoroch Práce a Pracovného Prostredia vo Vzťahu ku Kategorizácii Prác z Hľadiska Zdravotných Rizík a o Náležitostiach Návrhu na Zaradenie Prác do Kategórií; Republic of Slovakia: Bratislava, Slovakia, 2007. (In Slovak)
- Zákon č. 124/2006 Z. z., o Bezpečnosti a Ochrane Zdravia pri Práci a o Zmene a Doplnení Niektorých Zákonov; Republic of Slovakia: Bratislava, Slovakia, 2006. (In Slovak)
- Zákon č. 395/2006 Z. z., o Minimálnych Požiadavkách na Poskytovanie a Používanie Osobných Ochranných Pracovných Prostriedkov; Republic of Slovakia: Bratislava, Slovakia, 2006. (In Slovak)
- Beyan, A.C.; Demiral, Y.; Cimrin, A. Employment Status Changes of Workers after Referral to an Occupational Disease Clinic. J. Occup. Health 2018, 60, 494–501. [Google Scholar] [CrossRef] [PubMed]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Item | Name of Disease | Conditions under Which They Arise |
|---|---|---|
| 21 | Skin cancer diseases | In the manufacture, processing, use and transport of harmful substances causing skin cancer |
| 22 | Occupational dermatoses—Skin diseases apart from skin cancer and communicable skin diseases. | Exposure to the influence of chemical, physical (except ionizing radiation) and biological pollutants in the working environment and at work, causing occupational dermatosis |
| 23 | Diseases on pulmonary cancer from radioactive substances | When exposed to the stated hazard |
| 24–26 1 | Infectious and parasitic diseases including tropical infectious diseases and parasitic diseases and diseases transmissible from animals to humans. | When exposed to the stated hazard |
| 28 | Vibration disease—Diseases of bones, joints, muscles, vessels, and nerves limbs caused at work with vibrating tools and device. | When in contact with sources of vibration |
| 29 | Diseases of bones, joints, tendons, and nerves of limbs from long-term, inordinate, one-sided workload. | When exposed to the stated hazard |
| 33–34 2 | Pneumoconiosis | When exposed to the stated hazard |
| 38 | Hearing defect from noise by which loss hearing occurs, according to Fowler, with harm younger for those younger than 30 years at least 40%. Harm for those older than 30 years is then such that the presented level is increased by 1% every two years until 50 years of age of the harmed person, and since that time, loss of hearing must exceeded 50%. | When exposed to excessive noise |
| 46 | Tumor diseases emergent due to work with settled chemical carcinogens in damaged working environment and demonstrative in particular targeted organons, which are not included in this list. | When exposed to the risk of chemical carcinogenicity and a carcinogen is proven in the work environment, it is predominantly assessed by the National Commission for the Assessment of Occupational Diseases as the main causal factor in the development of a given cancer |
| Period | Figure | Publication Title |
|---|---|---|
| - | Hippokrates (460–370 BC) | “The Father of Medicine” First Recorded Mention of Occupational Diseases |
| - | Titus Lucretius Carus (99–55 BC) | Drew attention to the short life of miners in connection with their work |
| - | Gaius Plinius Secundus (AD 23–79) | Observed toxicity in the mining and processing of zinc and sulfur |
| - | Marcus Valerius Martialis (AD 40–102) | Warned of the danger of work with sulfur and blindness in blacksmiths |
| - | Aelius Claudius Galenus (AD 129–217) | Mentioned the risks arising in copper sulfate extraction in Cyprus |
| 1473 | Ulrich Ellenbog (1435–1499) | Pamphlet on Lead and Mercury Poisoning Among Gold Miners |
| 1534–38 | Paracelsus (1493–1541) | On miners’ diseases (1534) “Dosis Facit Venenum” (1538) |
| 1556 | Georg Agricola (1494–1555) | “De Re Metallica libri XII” (postmorte) |
| 1656 | Samuel Stockhausen (1649–1656) | “Libellus de lithargyrii fumo noxio morbifico eiusque metallico frequentiori morbo, vulgo dicto Die Hüttenkatze” [101] |
| 1700–13 | Bernardino Ramazzini (1633–1714) | “De Morbis Artificum Diatriba” (1700 rev. 1713) |
| 1753 | James Lind (1716–1794) | Treatise of the Scurvy |
| 1761 | Giovanni Antonio Scopoli (1723–1788) | “De Hydroargyro Idriensi Tentamina on the symptoms of mercury poisoning among mercury miners” |
| 1767 | George Baker (1722–1809) | An Essay Concerning the Cause of the Endemial Colic of Devonshire [102] |
| 1775 | Percival Pott (1714–1788) | Chirurgical Observations Relative to the Cataract, the Polypus of the Nose, the Cancer of the Scrotum, the Different Kinds of Ruptures, and the Mortification of the Toes and Feet |
| 1778 | José Parés y Franqués (1720–1798) | Catastrofe Morboso de las Minas Mercuriales de la Villa de Almaden del Azogue |
| 1832 | Charles Turner Thackrah (1795–1833) | The Effects of Arts, Trades, and Professions: and of Civic States and Habits of Living, on Health and Longevity: with Suggestions for the Removal of Many of the Agents which Produce Disease, and Shorten and Duration of Life |
| 1832 | James Phillips Kay-Shuttleworth (1804–1877) | The Moral and Physical Condition of the Working Classes Employed in the Cotton Manufacture in Manchester |
| 1833 | Great Britain | Factories Act adopted to improve the conditions of children working in factories (textile industry) |
| 1837 | Benjamin William McCready (1813–1892) | On the Influence of Trades, Professions, and Occupations in the United States, in the Production of Disease |
| 1842 | Edwin Chadwick (1800–1890) | Into the Sanitary Condition of the Labouring Population of Great Britain |
| 1844 | Robert Peel (1788–1850) | Health and Morals of Apprentices Act 1802 Cotton Mills and Factories Act 1819 Factories Act 1844 |
| 1845 | Frederick Engels (1820–1895) | The Condition of the Working Class in England |
| 1848 | Rudolf Virchow (1821–1902) | Report on the Typhus Epidemic in Upper Silesia |
| 1850 | Lemuel Shattuck (1793–1859) | Report of the Sanitary Commission of Massachusetts [103] |
| 1866–73 | William H. Sylvis (1828–1869) | Founder of the National Labor Union in the USA |
| 1869 | Massachusetts | Introduction the first State Bureau of Statistics of Labor |
| 1878 | Knights of Labor | Requests a federal act on occupational safety and health |
| 1880 | Great Britain | Initiates a law on compensation for workers paid by the employer |
| 1886 | George H. Ireland (1850–1916) | The Preventable Causes of Disease, Injury, and Death in American Manufactories and Workshops, and the Best Means and Appliances for Preventing and Avoiding Them |
| 1902 | Thomas Oliver (1853–1942) | Dangerous Trades: Dangerous Trades: The Historical, Social, and Legal, Aspects of Industrial Occupations as Affecting health [104] |
| 1905–34 | Thomas Morison Legge (1863–1932) | Industrial Anthrax (1905) |
| Lead Poisoning and Lead Absorption: The Symptoms, Pathology and Prevention, with Special Reference to their Industrial Origin and an Account of the Principle Processes Involving Risk (1912) | ||
| Chronic Benzol Poisoning (1919) [105] | ||
| Industrial Diseases Under the Medieval Trade Guilds (1920) [106] | ||
| Charles Turner Thackrah: A Pioneer in Industrial Hygiene (1920) [107] | ||
| Industrial Maladies (1934) [108] | ||
| A Historical Background of Industrial Hygiene (1946) [109] | ||
| 1910 | Crystal Eastman (1881–1928) | Work-accidents and the Law [110] |
| 1910 | John Andrews Fitch (1881–1959) | The Steel Workers [111] |
| 1914 | William Gilman Thompson (1856–1927) | The Occupational Diseases: Their Causation, Symptoms, Treatment and Prevention [112] |
| 1919 | Switzerland | 11 April 1919 creation of the ILO—International Labour Organization |
| 1918–43 | Alice Hamilton (1869–1970) | A Study of Spastic Anemia in the Hands of Stonecutters [113] (1918) |
| Industrial Poisons in the United States (1925) | ||
| Industrial toxicology (1934 rev. 1949) | ||
| Exploring the Dangerous Trades: The Autobiography of Alice Hamilton (1943) | ||
| 1942–64 | Wilhelm Carl Hueper (1894–1978) | Occupational Tumors and Allied Diseases (1942) |
| Chemical Carcinogenesis and Cancers (1964) | ||
| 1933 | Robley D. Evans (1907–1995) | Radium Poisoning A Review of Present Knowledge [114] |
| 1946 | Harriet Louise Hardy (1906–1993) | Delayed Chemical Pneumonitis Occurring in Workers Exposed to Beryllium Compounds [115] |
| 1948 | Switzerland | 7 April 1948 creation of the WHO—World Health Organization |
| 1953–61 | Robert A. Kehoe (1893–1992) | Experimental Studies on the Inhalation of Lead by Human Subjects (1953) |
| Occupational Medicine and Public Health (1961) | ||
| 1941–76 | Leonard J. Goldwater (1903–1992) | Disturbances in the Blood Following Exposure to Benzol [116] (1941) |
| Fifteen Years of Cardiac Work Classification (1959) | ||
| Strengthening Environmental Standards [117] (1976) | ||
| 1970 | Washington DC | 29 December 1970 creation of the NIOS—National Institute for Occupational Health and safety |
| 1971 | Washington DC | 28 April 1971 creation of the OSHA—Occupational Health and safety Administration |
| 1994 | Spain | 18 June 1994 creation of the EU-OSHA—European Agency for Occupational health and safety |
| 1968–91 | Irving Selikoff (1915–1992) | Asbestos Exposure, Smoking, and Neoplasia (1968) |
| Decline in Death Rates among Asbestos Insulation Workers 1967–1986 Associated with Diminution of Work Exposure to Asbestos (1990) | ||
| Associated with Diminution of Work Exposure to Asbestos (1990) | ||
| Asbestos Disease—1990–2020: The Risks of Asbestos Risk Assessment (1991) | ||
| Asbestos-Associated Deaths among Insulation Workers in the United States and Canada [118] (1991) | ||
| 1951–97 | Thomas F. Mancuso (1912–2004) | Occupational Cancer and other Health Hazards in a Chromate Plant: A Medical Appraisal. I. Lung Cancers in Chromate Workers. (1951) |
| Occupational Cancer and other Health Hazards in a Chromate Plant: A Medical Appraisal. II. Clinical and Toxicologic Aspects. (1951) | ||
| Radiation Exposures of Hanford Workers Dying from Cancer and other Causes (1977) | ||
| Chromium as an industrial carcinogen: Part I. (1997) | ||
| Chromium as an Industrial Carcinogen: Part II. Chromium in Human Tissues (1997) |
| Item | 1987–2002 | 2003–2019 | Total | Decrease/Increase | % * |
|---|---|---|---|---|---|
| 21–23 c | 144 | 33 | 177 | −111 | −77.08 |
| 22 | 2125 | 440 | 2565 | −1685 | −79.29 |
| 24–26 | 3750 | 766 | 4516 | −2984 | −79.57 |
| 28 | 2002 | 1289 | 3291 | −713 | −35.61 |
| 29 | 1970 | 3065 | 5035 | +1095 | +55.58 |
| 33–34 | 637 | 258 | 895 | −379 | −59.50 |
| 38 | 1684 | 513 | 2197 | −1171 | −69.54 |
| 46 | (-) | 37 | 37 | (x) | (x) |
| Total | 14,008 | 7037 | 21,025 | −6971 | −49.76 |
| Indicator | Category |
|---|---|
| Gender | Male, Female |
| Age category | up to 29 years, from 30 to 39 years, 40 to 49 years, 50 to 59 years old, 60 and over |
| Economic activity sector | Agriculture and Forestry (Sector 1) |
| Mining and Quarrying (Sector 2), | |
| Industrial Production (Sector 3), Construction (Sector 4) |
| Model | AIC | Model | AIC |
|---|---|---|---|
| ETS(M,M,N) | 248.35 | ETS(M,N,N) | 254.86 |
| ETS(M,Md,N) | 248.14 | ETS(A,N,N) | 258.33 |
| ETS(M,A,N) | 254.72 | ETS(A,A,N) | 253.66 |
| ETS(M,Ad,N) | 253.92 | ETS(A,Ad,N) | 249.88 |
| Year | Forecast | 80% Prediction Interval | 95% Prediction Interval | ||
|---|---|---|---|---|---|
| Lower | Upper | Lower | Upper | ||
| 2020 | 299.38 | 254.18 | 344.74 | 231.71 | 367.80 |
| 2021 | 290.63 | 246.54 | 334.08 | 223.35 | 357.01 |
| 2022 | 282.32 | 240.71 | 324.82 | 218.81 | 347.09 |
| 2023 | 274.44 | 233.58 | 316.49 | 212.41 | 336.98 |
| 2024 | 266.95 | 228.05 | 307.34 | 208.11 | 329.02 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Piňosová, M.; Andrejiova, M.; Badida, M.; Moravec, M. Occupational Disease as the Bane of Workers’ Lives: A Chronological Review of the Literature and Study of Its Development in Slovakia. Part 1. Int. J. Environ. Res. Public Health 2021, 18, 5910. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115910
Piňosová M, Andrejiova M, Badida M, Moravec M. Occupational Disease as the Bane of Workers’ Lives: A Chronological Review of the Literature and Study of Its Development in Slovakia. Part 1. International Journal of Environmental Research and Public Health. 2021; 18(11):5910. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115910
Chicago/Turabian StylePiňosová, Miriama, Miriam Andrejiova, Miroslav Badida, and Marek Moravec. 2021. "Occupational Disease as the Bane of Workers’ Lives: A Chronological Review of the Literature and Study of Its Development in Slovakia. Part 1" International Journal of Environmental Research and Public Health 18, no. 11: 5910. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115910