
Self-Management in Stroke Survivors: Development and Implementation of the Look after Yourself (LAY) Intervention

 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Intervention Description
2.1. Item 1. Brief Name
2.2. Item 2. Why: Description of the Rational and Theory Essential to the Intervention
- -
- Identification of the evidence base for the LAY intervention.
- -
- Set-up of the LAY intervention in terms of contents, duration, and delivery.
- -
- Test the relevance of contents and the feasibility of sessions and the fine-tuning review process.
2.3. Item 3. What: Description of Materials
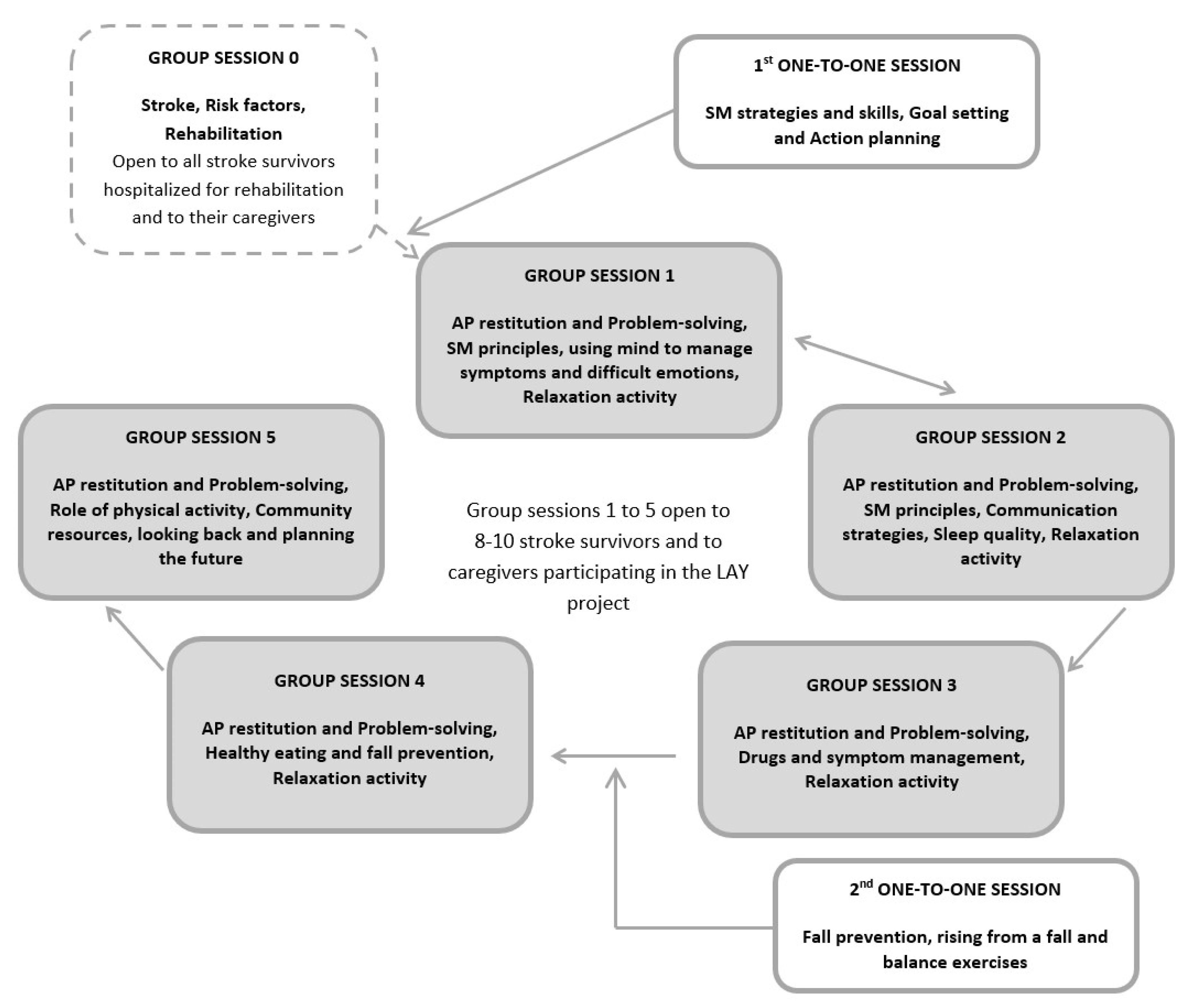
2.4. Item 4. What: Procedures Followed
- -
- Week 1: group session 0.
- -
- Week 2: individual session 1 and group session 1.
- -
- Week 3: group session 2.
- -
- Week 4: group session 3.
- -
- Week 5: individual session 2 and group session 4.
- -
- Week 6: group session 5.
2.5. Item 5. Providers
2.6. Item 6. LAY Intervention Delivery
2.6.1. Group Sessions
2.6.2. One-to-One Sessions
2.7. Item 7. Where: Type of Location
2.8. Item 8. When and How Much
2.9. Item 9. Tailoring
- -
- During the first few weeks after the event, individuals need time to understand what has happened, so the program focuses on the development of coping and adaptation strategies from the very first rehabilitation phase.
- -
- -
- Furthermore, in the post-acute phase, stroke survivors may experience reduced attention span, memory capacities, and communication deficits; for these reasons, the CDSMP contents were simplified and individual sessions were introduced.
- -
- Both the individual sessions and the action plan guarantee the tailoring of the intervention to each patient because the individual sessions targeted at accidental fall prevention explored the patient’s specific performance and context, and because the action plan trained the individuals to identify their own significant goals and to solve their specific problems.
2.10. Item 10. Modifications during the Course of the Study
2.11. Item 11. How Well (Planned)
2.12. Item 12. How Well (Actual)
3. Discussion
3.1. Limitations of the Intervention
3.2. Strengths of the Intervention
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Béjot, Y.; Daubail, B.; Giroud, M. Epidemiology of stroke and transient ischemic attacks: Current knowledge and perspectives. Rev. Neurol. 2016, 172, 59–68. [Google Scholar] [CrossRef]
- Stevens, E.; Emmett, E.; Wang, Y.; McKevitt, C.; Wolfe, C.D.A. The Burden of Stroke in Europe. Stroke Alliance Eur. 2017, 51, 131. [Google Scholar]
- Langhorne, P.; Baylan, S. Early Supported Discharge Trialists. Early supported discharge services for people with acute stroke. Cochrane Database Syst. Rev. 2017, 13, CD000443. [Google Scholar]
- Lou, S.; Carstensen, K.; Møldrup, M.; Shahla, S.; Zakharia, E.; Nielsen, C.P. Early supported discharge following mild stroke: A qualitative study of patients’ and their partners’ experiences of rehabilitation at home. Scand. J. Caring Sci. 2017, 31, 302–311. [Google Scholar] [CrossRef] [PubMed]
- Rodgers, H.; Price, C. Stroke unit care, inpatient rehabilitation and early supported discharge. Clin. Med. 2017, 17, 173–177. [Google Scholar] [CrossRef]
- Cobley, C.S.; Fisher, R.J.; Chouliara, N.; Kerr, M.; Walker, M.F. A qualitative study exploring patients’ and carers’ experiences of Early Supported Discharge services after stroke. Clin. Rehabil. 2013, 27, 750–757. [Google Scholar] [CrossRef] [PubMed]
- Luker, J.; Lynch, E.; Bernhardsson, S.; Bennett, L.; Bernhardt, J. Stroke Survivors’ Experiences of Physical Rehabilitation: A Systematic Review of Qualitative Studies. Arch. Phys. Med. Rehabil. 2015, 96, 1698–1708.e10. [Google Scholar] [CrossRef]
- Royal College of Physicians. Intercollegiate Stroke Working Party. National Clinical Guideline for Stroke, 4th ed.; Royal College of Physicians: London, UK, 2012. [Google Scholar]
- Winstein, C.J.; Stein, J.; Arena, R.; Bates, B.; Cherney, L.R.; Cramer, S.C.; Deruyter, F.; Eng, J.J.; Fisher, B.; Harvey, R.L.; et al. Guidelines for Adult Stroke Rehabilitation and Recovery: A Guideline for Healthcare Professionals from the American Heart Association/American Stroke Association. Stroke 2016, 47, e98–e169. [Google Scholar] [CrossRef] [PubMed]
- Fryer, C.E.; Luker, J.A.; McDonnell, M.N.; Hillier, S.L. Self management programmes for quality of life in people with stroke. Cochrane Database Syst. Rev. 2016, 22, CD010442. [Google Scholar] [CrossRef]
- Eng, J.J.; Bird, M.L.; Godecke, E.; Hoffmann, T.C.; Laurin, C.; Olaoye, O.A.; Solomon, J.; Teasell, R.; Watkins, C.L.; Walker, M.F. Moving stroke rehabilitation research evidence into clinical practice: Consensus-based core recommendations from the Stroke Recovery and Rehabilitation Roundtable. Int. J. Stroke. 2019, 14, 766–773. [Google Scholar] [CrossRef] [Green Version]
- Messina, R.; Dallolio, L.; Fugazzaro, S.; Rucci, P.; Iommi, M.; Bardelli, R.; Costi, S.; Denti, M.; Accogli, M.A.; Cavalli, E.; et al. The Look after Yourself (LAY) intervention to improve self-management in stroke survivors: Results from a quasi-experimental study. Patient Educ. Couns. 2020, 103, 1191–1200. [Google Scholar] [CrossRef]
- Hoffmann, T.C.; Glasziou, P.P.; Boutron, I.; Milne, R.; Perera, R.; Moher, D.; Altman, D.G.; Barbour, V.; Macdonald, H.; Johnston, M.; et al. Better reporting of interventions: Template for intervention description and rep-lication (TIDieR) checklist and guide. BMJ 2014, 348, g1687. [Google Scholar] [CrossRef] [Green Version]
- Lorig, K.R.; Hurwicz, M.L.; Sobel, D.; Hobbs, M.; Ritter, P.L. A national dissemination of an evidence-based self-management program: A process evaluation study. Patient Educ. Couns. 2005, 59, 69–79. [Google Scholar] [CrossRef] [PubMed]
- Bandura, A. Self-Efficacy. In Encyclopedia of Human Behavior; Ramachaudran, V.S., Ed.; Academic Press: New York, NY, USA, 1994; Volume 4, pp. 71–81, Reprinted in Encyclopedia of Mental Health; Friedman, H., Ed.; Academic Press: San Diego, CA, USA, 1998. [Google Scholar]
- Lennon, S.; McKenna, S.; Jones, F. Self-management programmes for people post stroke: A systematic review. Clin. Rehabil. 2013, 27, 867–878. [Google Scholar] [CrossRef]
- McKenna, S.; Jones, F.; Glenfield, P.; Lennon, S. Bridges self-management program for people with stroke in the community: A feasibility randomized controlled trial. Int. J. Stroke 2015, 10, 697–704. [Google Scholar] [CrossRef] [PubMed]
- Butler, C. The American Academy for Cerebral Palsy and Developmental Medicine Methodology to Develop Systematic Reviews of Treatment Interventions; Revision 1.2. 2008. Available online: http://www.aacpdm.org/membership/members/committees/treatment_outcomes_methodology.pdf (accessed on 7 January 2014).
- Allen, K.R.; Hazelett, S.; Jarjoura, D.; Wickstrom, G.C.; Hua, K.; Weinhardt, J.; Wright, K. Effectiveness of a post discharge care management model for stroke and transient is-chemic attack: A randomized trial. J. Stroke Cerebrovasc. Dis. 2002, 11, 88–98. [Google Scholar] [CrossRef]
- Allen, K.; Hazelett, S.; Jarjoura, D.; Hua, K.; Wright, K.; Weinhardt, J.; Kropp, D. A randomized trial testing the superiority of a post discharge care management model for stroke survivors. J. Stroke Cerebrovasc. Dis. 2009, 18, 443–452. [Google Scholar] [CrossRef] [Green Version]
- Cadilhac, D.A.; Hoffmann, S.; Kilkenny, M.; Lindley, R.; Lalor, E.; Osborne, R.H.; Batterbsy, M. A phase II multicentered, single-blind, randomized, controlled trial of the stroke self-management program. Stroke 2011, 42, 1673–1679. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Damush, T.M.; Ofner, S.; Yu, Z.; Plue, L.; Nicholas, G.; Williams, L.S. Implementation of a stroke self-management program: A randomized controlled pilot study of veterans with stroke. Transl. Behav. Med. 2011, 1, 561–572. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frank, G.; Johnston, M.; Morrison, V.; Pollard, B.; MacWalter, R. Perceived control and recovery from functional limitations: Preliminary evaluation of a workbook-based intervention for discharged stroke patients. Br. J. Health Psych. 2000, 5, 413–420. [Google Scholar] [CrossRef]
- Harwood, M.; Weatherall, M.; Talemaitoga, A.; Barber, P.A.; Gommans, J.; Taylor, W.; McPherson, K.; McNaughton, H. Taking charge after stroke: Promoting self-directed rehabilitation to improve quality of life-a randomized controlled trial. Clin. Rehabil. 2012, 26, 493–501. [Google Scholar] [CrossRef]
- Johnston, M.; Bonetti, D.; Joice, S.; Pollard, B.; Morrison, V.; Francis, J.J.; Macwalter, R. Recovery from disability after stroke as a target for a behavioural intervention: Results of a randomized controlled trial. Disabil. Rehabil. 2007, 29, 1117–1127. [Google Scholar] [CrossRef] [PubMed]
- Kendall, E.; Catalano, T.; Kuipers, P.; Posner, N.; Buys, N.; Charker, J. Recovery following stroke: The role of self-management education. Soc. Sci. Med. 2007, 64, 735–746. [Google Scholar] [CrossRef] [PubMed]
- Marsden, D.; Quinn, R.; Pond, N.; Golledge, R.; Neilson, C.; White, J.; McElduff, P.; Pollack, M. A multidisciplinary group programme in rural settings for community dwelling chronic stroke survivors and their carers: A pilot randomized controlled trial. Clin. Rehabil. 2010, 24, 328–341. [Google Scholar] [CrossRef] [PubMed]
- Lorig, K.R.; Ritter, P.; Stewart, A.L.; Sobel, D.S.; Brown, B.W.; Jr Bandura, A.; Gonzalez, V.M.; Laurent, D.D.; Holman, H.R. Chronic Disease Self-Management Program: 2-Year Health Status and Health Care Uti-lization Outcomes. Med. Care 2001, 39, 1217–1223. [Google Scholar] [CrossRef]
- Self-Management Resource Center. Available online: https://www.selfmanagementresource.com/programs/ (accessed on 7 January 2021).
- Lorig, K.; Ritter, P.L.; Villa, F.J.; Armas, J. Community-based peer-led diabetes self-management: A randomized trial. Diabetes Educ. 2009, 35, 641–651. [Google Scholar] [CrossRef]
- Risendal, B.; Dwyer, A.; Seidel, R.; Lorig, K.; Katzenmeyer, C.; Coombs, L.; Kellar-Guenther, Y.; Warren, L.; Franco, A.; Ory, M. Adaptation of the chronic disease self-management program for cancer survivors: Feasibility, acceptability, and lessons for implementation. J. Cancer Educ. 2014, 29, 762–771. [Google Scholar] [CrossRef] [PubMed]
- Franek, J. Self-management support interventions for persons with chronic disease: An evidence-based analysis. Ont. Health Technol. Assess Ser. 2013, 13, 1–60. [Google Scholar]
- Jones, F. Strategies to enhance chronic disease self-management: How can we apply this to stroke? Disabil. Rehabil. 2006, 28, 841–847. [Google Scholar] [CrossRef]
- Jones, F.; Riazi, A. Self-efficacy and self-management after stroke: A systematic review. Disabil. Rehabil. 2011, 33, 797–810. [Google Scholar] [CrossRef]
- Bovend’Eerdt, T.J.; Botell, R.E.; Wade, D.T. Writing SMART rehabilitation goals and achieving goal attainment scaling: A practical guide. Clin. Rehabil. 2009, 23, 352–361, published correction appears in Clin. Rehabil. 2010, 24, 382. [Google Scholar] [CrossRef]
- Lorig, K.; Laurent, D.; González, V.; Sobel, D.; Minor, M.; Gecht-Silver, M. Living a Healthy Life with Chronic Conditions: Self-Management of Heart Disease, Arthritis, Diabetes, Depression, Asthma, Bronchitis, Emphysema and Other Physical and Mental Health Conditions; Bull Publishing Company: Boulder, CO, USA, 2012. [Google Scholar]
- Educate Your Patients. National Stroke Association. 2019. Available online: https://www.stroke.org/we-can-help/healthcare-professionals/educate-your-patients/ (accessed on 24 April 2020).
- Lynch, J.; Mead, G.; Greig, C.; Young, A.; Lewis, S.; Sharpe, M. Fatigue after stroke: The development and evaluation of a case definition. J. Psychosom. Res. 2007, 63, 539–544. [Google Scholar] [CrossRef]
- Hinkle, J.L.; Becker, K.J.; Kim, J.S.; Choi-Kwon, S.; Saban, K.L.; McNair, N.; Mead, G.E.; American Heart Association Council on Cardiovascular and Stroke Nursing and Stroke Council. Post-stroke fatigue: Emerging evidence and approaches to management: A scientific statement for healthcare professionals from the American Heart Association. Stroke 2017, 48, e159–e170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lorig, K.R.; Holman, H. Self-management education: History, definition, outcomes, and mechanisms. Ann. Behav. Med. 2003, 26, 1–7. [Google Scholar] [CrossRef]
- Plant, S.; Tyson, S.F. A multicentre study of how goal-setting is practised during inpatient stroke rehabilitation. Clin. Rehabil. 2018, 32, 263–272. [Google Scholar] [CrossRef] [Green Version]
- Funnell, M.M. Peer-based behavioural strategies to improve chronic disease self-management and clinical outcomes: Evidence, logistics, evaluation considerations and needs for future research. Fam. Pract. 2010, 27 (Suppl. 1), 17–22. [Google Scholar] [CrossRef] [Green Version]
- Clark, E.; MacCrosain, A.; Ward, N.S.; Jones, F. The key features and role of peer support within group self-management interventions for stroke? A systematic review. Disabil. Rehabil. 2018, 16, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Parke, H.L.; Epiphaniou, E.; Pearce, G.; Taylor, S.J.; Sheikh, A.; Griffiths, C.J.; Greenhalgh, T.; Pinnock, H. Self-Management Support Interventions for Stroke Survivors: A Systematic Me-ta-Review. PLoS ONE 2015, 10, e0131448. [Google Scholar] [CrossRef] [PubMed]
- Dallolio, L.; Messina, R.; Calugi, S.; Fugazzaro, S.; Bardelli, R.; Rucci, P.; Fantini, M.P.; Cavalli, E.; Taricco, M.; Look after Yourself Project. Self-management and self-efficacy in stroke survivors: Val-idation of the Italian version of the Stroke Self-Efficacy Questionnaire. Eur. J. Phys. Rehabil. Med. 2018, 54, 68–74. [Google Scholar] [PubMed]


{kind=link}
| Study | Sample Size | Experimental Self-Management Program | Duration of the Program | Timing of the Program Initiation | Program Leader | Setting of Delivery | Theoretical Basis/Model |
|---|---|---|---|---|---|---|---|
| Allen, 2002 [19] | 96 | Individualized intervention, including an initial home biopsychosocial assessment and education visit, and a team-based development and implementation of an individualized treatment plan focused on health promotion and psychosocial well-being. | 3 months | Within 1 month post-discharge from stroke unit | Advanced practice nurse care manager | Participants’ homes | Wagner’s chronic care model |
| Allen, 2009 [20] | 380 | As for Allen 2002 [19]. The average time spent on intervention was 8.5 h/patient and included a minimum of 2 home visits and periodic phone calls | 6 months | Within 2 months from post-stroke unit admission | Advanced practice nurse care manager | Participants’ homes | Wagner’s chronic care model |
| Cadilhac, 2011 [21] | 143 | Weekly 2½-hour group sessions including targeted stroke-specific information and strategies to ensure retention of learning and skills | 8 weeks | At least 3 months post stroke | National Stroke Foundation’s Stroke Educator and a trained peer facilitator | Community | Stanford CDSMP |
| Damush, 2011 [22] | 63 | 6 biweekly 20-min telephone calls guided by a standardized manual and targeted to building self-efficacy using goal setting and behavioral contracting | 3 months of intervention + 3 months of telephone monitoring and reinforcement | Within 1 month from stroke | Trained nurse, physician, and social scientist | Telephone calls | Stanford CDSMP |
| Frank, 2000 [23] | 41 | Two one-to-one sessions plus weekly telephone calls guided by a workbook including information, coping resources, relaxation techniques, problem-solving skills, and rehearsing planning | 1 month | Within 24 months from stroke | Researcher | Participants’ homes | Control cognitions (including self-efficacy) |
| Harwood, 2011 [24] | 139 | 80-min one-to-one session guided by a specific workbook and designed to engage the patient and his/her family in the process of recovery and self-directed rehabilitation, plus/or 80-min inspirational dvd about stroke, stroke recovery, and promoting self-directed rehabilitation strategies | 80 min | 6 to 12 weeks post-stroke | Trained research assistants | Community | Self-efficacy principles |
| Johnston, 2007 [25] | 203 | 3 one-to-one and 2 telephone sessions guided by a workbook. The workbook provided information about stroke and recovery and included activities designed to allow the patient to attain the coping skills to encourage self-management. An audio relaxation cassette tape was provided. | 5 weeks | Within 2 weeks from hospital discharge | Researcher | Participants’ homes | Control cognitions (including self-efficacy) |
| Kendall, 2007 [26] | 100 | 2-h group sessions including both generic chronic condition and stroke-specific self-management education regarding health and well-being, group interaction and support, problem solving | 7 weeks | 3 months post-stroke | Trained healthcare professionals | Community | Stanford CDSMP |
| Marsden, 2010 [27] | 26 | Weekly 2½-hour group session including physical activity and education, always addressing nutritional counseling | 7 weeks | At least 1 month post-discharge from all stroke therapy programs | Multidisciplinary stroke team members | Local community public hospital | Not described |
| McKenna, 2013 [17] | 25 | Weekly one-to-one sessions up to one hour/week, with the support of a stroke workbook, to promote specific self-management behaviors, such as enabling patients to set personalized goals, plan feasible actions, record progress, and problem solving. | 6 weeks | Within 4 weeks of commencing rehabilitation in the community | Trained members of the community stroke team | Community | Self-efficacy principles |
| Group Sessions | ||||
|---|---|---|---|---|
| Session n° | Structure | Specific Topics | Specific Activities | |
| 0 |
|
| Brainstorming Active participation Group discussion | |
| 1 | Common Structure |
| Using mind to manage symptoms Difficult emotions management | |
| 2 | Good communication (help request) Enjoying a good quality sleep | |||
| 3 | Drugs management Pain and fatigue management | |||
| 4 | Healthy diet Falls prevention and balance exercises | |||
| 5 | Physical activity Community services | |||
| Individual sessions | ||||
| Session 1 Before the 1st group session |
| |||
| Session 2 Before the 4th group session |
| |||
| Main Sources of Self-Efficacy | Technique/Instrument | In LAY Intervention |
|---|---|---|
| Mastery experiences | Breaking the task into smaller, achievable components to achieve a positive result in a task or skill | Weekly realistic action plan |
| Vicarious experiences | Observe someone perceived to be a peer (model) successfully performing a task, i.e., learning from others’ experiences of the post-stroke recovery period | Interactive group sessions |
| Verbal persuasion | Persuasion and verification from significant individuals (stroke professional or key family member) to increase an individual’s belief about his/her personal level of skill | Successful action plans shared during group sessions Positive feedback from health professionals |
| Physiological feedback | Interpretation of individual’s physical sensations and emotions and feelings as positive | Training in positive thinking Training in relaxation techniques |
| Self-management abilities | Technique/Instrument | In LAY Intervention |
| Problem solving | Information on stroke, risk factors, care pathway, and consequences of stroke | Repetition of problem-solving technique in individual and group sessions |
| Decision making | Repetition of how to make decisions | Goal setting and decision making in individual and group sessions |
| Appropriate resource utilization | Giving information to facilitate knowledge and access to community resources | Oral information in a group session and written information in patients Manual |
| Partnership with healthcare professionals | Training in how to ask for help | Training patients’ ability to communicate and collaborate in a group session |
| Taking necessary actions | Action plan as a good instrument to focus on achievable goals | Training in action planning every week for 6 weeks |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fugazzaro, S.; Denti, M.; Accogli, M.A.; Costi, S.; Pagliacci, D.; Calugi, S.; Cavalli, E.; Taricco, M.; Bardelli, R.; on behalf of Look after Yourself Project. Self-Management in Stroke Survivors: Development and Implementation of the Look after Yourself (LAY) Intervention. Int. J. Environ. Res. Public Health 2021, 18, 5925. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115925
Fugazzaro S, Denti M, Accogli MA, Costi S, Pagliacci D, Calugi S, Cavalli E, Taricco M, Bardelli R, on behalf of Look after Yourself Project. Self-Management in Stroke Survivors: Development and Implementation of the Look after Yourself (LAY) Intervention. International Journal of Environmental Research and Public Health. 2021; 18(11):5925. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115925
Chicago/Turabian StyleFugazzaro, Stefania, Monica Denti, Monia Allisen Accogli, Stefania Costi, Donatella Pagliacci, Simona Calugi, Enrica Cavalli, Mariangela Taricco, Roberta Bardelli, and on behalf of Look after Yourself Project. 2021. "Self-Management in Stroke Survivors: Development and Implementation of the Look after Yourself (LAY) Intervention" International Journal of Environmental Research and Public Health 18, no. 11: 5925. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115925