
Four Weeks of Detraining Induced by COVID-19 Reverse Cardiac Improvements from Eight Weeks of Fitness-Dance Training in Older Adults with Mild Cognitive Impairment

 , ,
, ,  , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants’ Screening
2.2. The Fitness and Dance Training Programs
2.3. Measurements
2.3.1. The Neuropsychological Test Battery “CERAD-Plus”
2.3.2. The Modified German version of the Physical Activity Readiness Questionnaire (PAR-Q)
2.3.3. Physical Performance and Heart Rate Data
2.4. Statistical Analysis
3. Results
3.1. Study Population
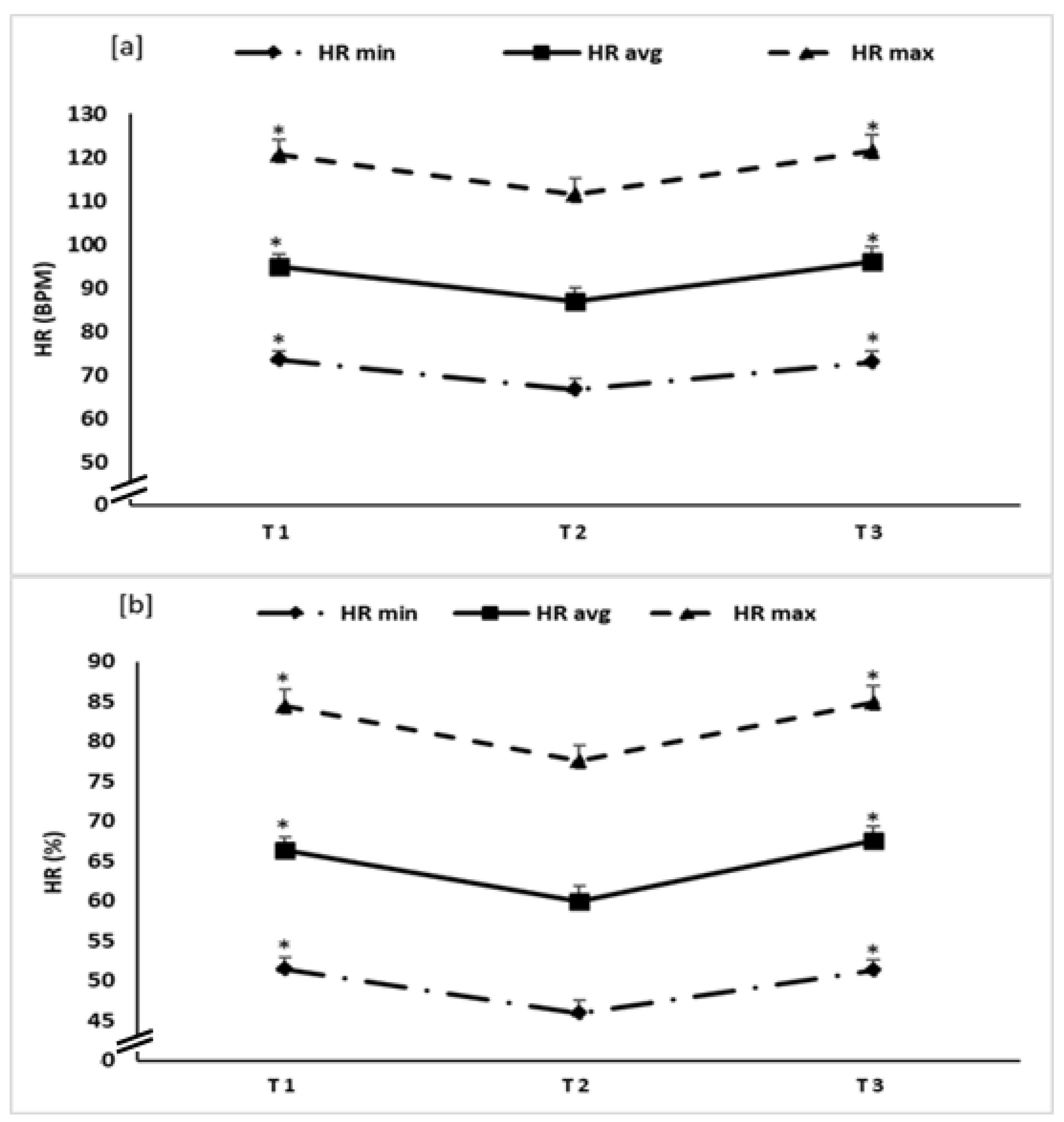
3.2. Effect of Training-Detraining on Min, Max and Avg HR
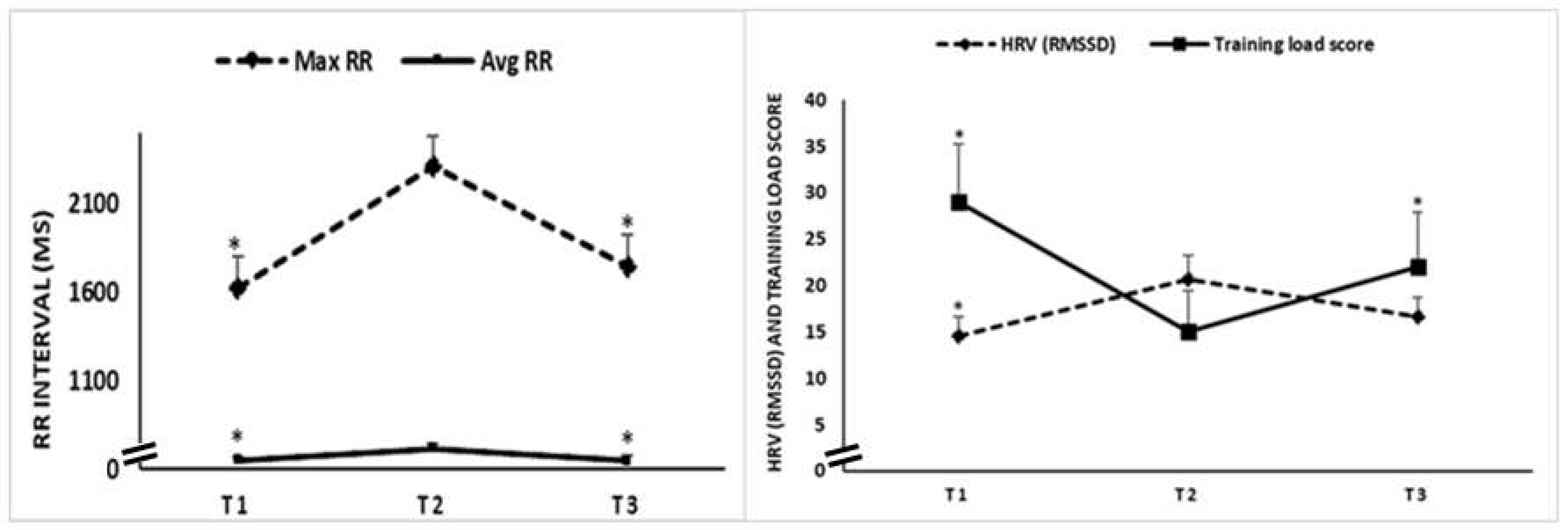
3.3. Effect of Training-Detraining on RR Intervals, HRV (RMSSD) and Training Load
3.4. Effect of Training-Detraining on Percentage of Time in HR Zones
3.5. Physical Performance Indicators during the Three Test Sessions
3.6. Responsiveness to Training/Detraining Adaptations
4. Discussion
5. Strength and Limitation
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hayflick, L. The future of ageing. Nature 2000, 408, 267–269. [Google Scholar] [CrossRef]
- Eurostat. Population Structure and Ageing. Available online: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Population_structure_and_ageing (accessed on 4 November 2019).
- Population Ageing in Europe: Facts, Implications and Policies Outcomes of EU Funded Research; European Commission: Brussels, 2014; ISBN 978-92-79-35063-4. [CrossRef]
- Vos, T.; Flaxman, A.D.; Naghavi, M.; Lozano, R.; Michaud, C.; Ezzati, M.; Shibuya, K.; A Salomon, J.; Abdalla, S.; Aboyans, V.; et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2163–2196. [Google Scholar] [CrossRef]
- Gazzaley, A.; Sheridan, M.A.; Cooney, J.W.; D’Esposito, M. Age-related deficits in component processes of working memory. Neuropsychology 2007, 21, 532–539. [Google Scholar] [CrossRef] [Green Version]
- Small, B.J.; Fratiglioni, L.; Viitanen, M.; Winblad, B.; Bäckman, L. The course of cognitive impairment in preclinical Alzheimer disease: Three- and 6-year follow-up of a population-based sample. Arch. Neurol. 2000, 57, 839–844. [Google Scholar] [CrossRef] [Green Version]
- Legdeur, N.; Heymans, M.W.; Comijs, H.C.; Huisman, M.; Maier, A.B.; Visser, P.J. Age dependency of risk factors for cognitive decline. BMC Geriatr. 2018, 18, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Kivipelto, M.; Ngandu, T.; Fratiglioni, L.; Viitanen, M.; Kåreholt, I.; Winblad, B.; Helkala, E.-L.; Tuomilehto, J.; Soininen, H.; Nissinen, A. Obesity and Vascular Risk Factors at Midlife and the Risk of Dementia and Alzheimer Disease. Arch. Neurol. 2005, 62, 1556–1560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fillit, H.; Nash, D.T.; Rundek, T.; Zuckerman, A. Cardiovascular risk factors and dementia. Am. J. Geriatr. Pharmacother. 2008, 6, 100–118. [Google Scholar] [CrossRef]
- Knopman, D.S.; Roberts, R. Vascular Risk Factors: Imaging and Neuropathologic Correlates. J. Alzheimer’s Dis. 2010, 20, 699–709. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zlokovic, B.V. Neurovascular pathways to neurodegeneration in Alzheimer’s disease and other disorders. Nat. Rev. Neurosci. 2011, 12, 723–738. [Google Scholar] [CrossRef] [PubMed]
- Norton, S.; E Matthews, F.; E Barnes, D.; Yaffe, K.; Brayne, C. Potential for primary prevention of Alzheimer’s disease: An analysis of population-based data. Lancet Neurol. 2014, 13, 788–794. [Google Scholar] [CrossRef] [Green Version]
- Gray, C.L.; Messer, L.C.; Rappazzo, K.M.; Jagai, J.S.; Grabich, S.C.; Lobdell, D.T. The association between physical inactivity and obesity is modified by five domains of environmental quality in U.S. adults: A cross-sectional study. PLoS ONE 2018, 13, e0203301. [Google Scholar] [CrossRef]
- Keaney, J.F.; Larson, M.G.; Vasan, R.S.; Wilson, P.W.F.; Lipinska, I.; Corey, D.; Massaro, J.M.; Sutherland, P.; Vita, J.A.; Benjamin, E.J. Obesity and systemic oxidative stress: Clinical correlates of oxidative stress in the Framingham Study. Arterioscler. Thromb. Vasc. Biol. 2003, 23, 434–439. [Google Scholar] [CrossRef] [Green Version]
- Yudkin, J.S.; Kumari, M.; Humphries, S.E.; Mohamed-Ali, V. Inflammation, obesity, stress and coronary heart disease: Is interleukin-6 the link? Atherosclerosis 2000, 148, 209–214. [Google Scholar] [CrossRef]
- Shimano, H. SREBPs: Physiology and pathophysiology of the SREBP family. FEBS J. 2009, 276, 616–621. [Google Scholar] [CrossRef] [PubMed]
- Liew, J.; Teo, S.P. Physical activity in older people with cardiac co-morbidities. J. Geriatr. Cardiol. 2018, 15, 557–558. [Google Scholar]
- Müller, P.; Schmicker, M.; Müller, N.G. Präventionsstrategien gegen Demenz. Z. Gerontol. Geriatr. 2017, 50, 89–95. [Google Scholar] [CrossRef] [PubMed]
- Rognmo, Ø.; Hetland, E.; Helgerud, J.; Hoff, J.; Slørdahl, S.A. High intensity aerobic interval exercise is superior to moderate intensity exercise for increasing aerobic capacity in patients with coronary artery disease. Eur. J. Cardiovasc. Prev. Rehabil. 2004, 11, 216–222. [Google Scholar] [CrossRef] [PubMed]
- Ades, P.A.; Savage, P.D.; Cress, M.E.; Brochu, M.A.R.T.I.N.; Lee, N.M.; Poehlman, E.T. Resistance training on physical per-formance in disabled older female cardiac patients. Med. Sci. Sports Exerc. 2003, 35, 1265–1270. [Google Scholar] [CrossRef]
- Huynh, Q.; Negishi, K.; De Pasquale, C.; Hare, J.L.; Leung, D.; Stanton, T.; Marwick, T.H. Validation of Predictive Score of 30-Day Hospital Readmission or Death in Patients with Heart Failure. Am. J. Cardiol. 2018, 121, 322–329. [Google Scholar] [CrossRef] [Green Version]
- Lautenschlager, N.T.; Cox, K.L.; Flicker, L.; Foster, J.K.; van Bockxmeer, F.M.; Xiao, J.; Greenop, K.R.; Almeida, O.P. Effect of physical activity on cognitive function in older adults at risk for Alzheimer disease: A randomized trial. JAMA 2008, 300, 1027–1037. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagamatsu, L.S.; Handy, T.C.; Hsu, C.L.; Voss, M.; Liu-Ambrose, T. Resistance training promotes cognitive and functional brain plasticity in seniors with probable mild cognitive impairment. Arch. Intern. Med. 2012, 172, 666–668. [Google Scholar] [CrossRef]
- Varela, S.; Ayán, C.; Cancela, J.M.; Martín, V. Effects of two different intensities of aerobic exercise on elderly people with mild cognitive impairment: A randomized pilot study. Clin. Rehabil. 2011, 26, 442–450. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, T.; Shimada, H.; Makizako, H.; Doi, T.; Yoshida, D.; Ito, K.; Shimokata, H.; Washimi, Y.; Endo, H.; Kato, T. A ran-domized controlled trial of multicomponent exercise in older adults with mild cognitive impairment. PLoS ONE 2013, 8, e61483. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Müller, P.; Rehfeld, K.; Lüders, A.; Schmicker, M.; Hökelmann, A.; Kaufman, J.; Müller, N.G.; Müller, M.P. Effekte eines Tanz- und eines Gesundheitssporttrainings auf die graue Hirnsubstanz gesunder Senioren. Sportwissenschaft 2016, 46, 213–222. [Google Scholar] [CrossRef]
- Müller, P.; Rehfeld, K.; Schmicker, M.; Hökelmann, A.; Dordevic, M.; Lessmann, V.; Brigadski, T.; Kaufmann, J.; Müller, N.G. Evolution of Neuroplasticity in Response to Physical Activity in Old Age: The Case for Dancing. Front. Aging Neurosci. 2017, 9, 56. [Google Scholar] [CrossRef] [Green Version]
- Müller, P.; Rehfeld, K.; Schmicker, M.; Müller, N. P52. Future directions for physical exercise as personalized medicine. Clin. Neurophysiol. 2018, 129, e88. [Google Scholar] [CrossRef]
- Rehfeld, K.; Müller, P.; Aye, N.; Schmicker, M.; Dordevic, M.; Kaufmann, J.; Hökelmann, A.; Müller, N.G. Dancing or Fitness Sport? The Effects of Two Training Programs on Hippocampal Plasticity and Balance Abilities in Healthy Seniors. Front. Hum. Neurosci. 2017, 11, 305. [Google Scholar] [CrossRef]
- Rehfeld, K.; Lüders, A.; Hökelmann, A.; Lessmann, V.; Kaufmann, J.; Brigadski, T.; Müller, P.; Müller, N.G. Dance training is superior to repetitive physical exercise in inducing brain plasticity in the elderly. PLoS ONE 2018, 13, e0196636. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamacher, D.; Hamacher, D.; Rehfeld, K.; Schega, L. Motor-cognitive dual-task training improves local dynamic stability of normal walking in older individuals. Clin. Biomech. 2015, 32, 138–141. [Google Scholar] [CrossRef]
- Hamacher, D.; Hamacher, D.; Rehfeld, K.; Hökelmann, A.; Schega, L. The Effect of a Six-Month Dancing Program on Mo-tor-Cognitive Dual-Task Performance in Older Adults. JAPA 2015, 23, 647–652. [Google Scholar] [CrossRef] [PubMed]
- Morente-Oria, H.; Ruiz-Montero, P.J.; Chiva-Bartoll, Ó.; González-Fernández, F.T. Effects of 8-Weeks Concurrent Strength and Aerobic Training on Body Composition, Physiological and Cognitive Performance in Older Adult Women. Sustainability 2020, 12, 1944. [Google Scholar] [CrossRef] [Green Version]
- Bentlage, E.; Ammar, A.; How, D.; Ahmed, M.; Trabelsi, K.; Chtourou, H.; Brach, M. Practical Recommendations for Maintaining Active Lifestyle during the COVID-19 Pandemic: A Systematic Literature Review. Int. J. Environ. Res. Public Health 2020, 17, 6265. [Google Scholar] [CrossRef] [PubMed]
- Chtourou, H.; Trabelsi, K.; H’Mida, C.; Boukhris, O.; Glenn, J.M.; Brach, M.; Bentlage, E.; Bott, N.; Shephard, R.J.; Ammar, A.; et al. Staying Physically Active During the Quarantine and Self-Isolation Period for Controlling and Mitigating the COVID-19 Pandemic: A Systematic Overview of the Literature. Front. Psychol. 2020, 11, 11. [Google Scholar] [CrossRef]
- Müller, P.; Ammar, A.; Zou, L.; Müller, N.G. COVID-19 and physical (In-) activity. Dtsch. Z. Sportmed. 2021, 72, 45–46. [Google Scholar] [CrossRef]
- Müller, P.; Ammar, A.; Zou, L.; Apfelbacher, C.; Erickson, K.I.; Müller, N.G. COVID-19, physical (in-)activity, and dementia prevention. Alzheimers Dement. (N. Y.) 2020, 6, e12091. [Google Scholar] [CrossRef]
- Ammar, A.; Trabelsi, K.; Brach, M.; Chtourou, H.; Boukhris, O.; Masmoudi, L.; Bouaziz, B.; Bentlage, E.; How, D.; Ahmed, M.; et al. Effects of home confinement on mental health and lifestyle behaviours during the COVID-19 outbreak: Insight from the ECLB-COVID19 multicenter study. Biol. Sport 2021, 38, 9–21. [Google Scholar] [CrossRef]
- Grande, A.J.; Keogh, J.; Silva, V.; Scott, A.M. Exercise versus no exercise for the occurrence, severity, and duration of acute respiratory infections. Cochrane Database Syst. Rev. 2020, 4, CD010596. [Google Scholar] [CrossRef] [Green Version]
- Hansen, A.L.; Johnsen, B.H.; Sollers, J.J.; Stenvik, K.; Thayer, J.F. Heart rate variability and its relation to prefrontal cognitive function: The effects of training and detraining. Graefe’s Arch. Clin. Exp. Ophthalmol. 2004, 93, 263–272. [Google Scholar] [CrossRef]
- Gamelin, F.; Berthoin, S.; Sayah, H.; Libersa, C.; Bosquet, L. Effect of Training and Detraining on Heart Rate Variability in Healthy Young Men. Int. J. Sports Med. 2007, 28, 564–570. [Google Scholar] [CrossRef] [PubMed]
- Schulz, K.F.; Altman, D.G.; Moher, D. CONSORT 2010 Statement: Updated guidelines for reporting parallel group randomised trials. BMJ 2010, 340, 332. [Google Scholar] [CrossRef]
- Petersen, R.C. Mild cognitive impairment as a diagnostic entity. J. Intern. Med. 2004, 256, 183–194. [Google Scholar] [CrossRef] [PubMed]
- Finger, J.D.; Gößwald, A.; Härtel, S.; Müters, S.; Krug, S.; Hölling, H.; Kuhnert, R.; Bös, K. Measurement of cardiorespiratory fitness in the study on adult health in Germany (DEGS1). Fed. Health Gaz. 2013, 56, 885–893. [Google Scholar] [CrossRef] [Green Version]
- Alden, D.; Austin, C.; Sturgeon, R. A Correlation Between the Geriatric Depression Scale Long and Short Forms. J. Gerontol. 1989, 44, P124–P125. [Google Scholar] [CrossRef] [PubMed]
- Ammar, A.; Chtourou, H.; Hammouda, O.; Turki, M.; Ayedi, F.; Kallel, C.; Abdelkarim, O.; Hoekelmann, A.; Souissi, N. Relationship between biomarkers of muscle damage and redox status in response to a weightlifting training session: Effect of time-of-day. Acta Physiol. Hung. 2016, 103, 243–261. [Google Scholar] [CrossRef] [Green Version]
- Ammar, A.; Chtourou, H.; Souissi, N. Effect of Time-of-Day on Biochemical Markers in Response to Physical Exercise. J. Strength Cond. Res. 2017, 31, 272–282. [Google Scholar] [CrossRef]
- Chtourou, H.; Engel, F.A.; Fakhfakh, H.; Fakhfakh, H.; Hammouda, O.; Ammar, A.; Trabelsi, K.; Souissi, N.; Sperlich, B. Diurnal Variation of Short-Term Repetitive Maximal Performance and Psychological Variables in Elite Judo Athletes. Front. Physiol. 2018, 9, 1499. [Google Scholar] [CrossRef] [Green Version]
- Trabelsi, K.; Ammar, A.; Masmoudi, L.; Boukhris, O.; Chtourou, H.; Bouaziz, B.; Brach, M.; Bentlage, E.; How, D.; Ahmed, M.; et al. Globally altered sleep patterns and physical activity levels by confinement in 5056 individuals: ECLB COVID-19 international online survey. Biol. Sport 2021, 38, 495–506. [Google Scholar] [CrossRef]
- Chtourou, H.; Trabelsi, K.; Ammar, A.; Shephard, R.J.; Bragazzi, N.L. Acute Effects of an “Energy Drink” on Short-Term Maximal Performance, Reaction Times, Psychological and Physiological Parameters: Insights from a Randomized Double-Blind, Placebo-Controlled, Counterbalanced Crossover Trial. Nutrients 2019, 11, 992. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morris, J.C.; Heyman, A.; Mohs, R.C.; Hughes, J.P.; Van Belle, G.; Fillenbaum, G.; Mellits, E.D.; Clark, C. The Consortium to Establish a Registry for Alzheimer’s Disease (CERAD). Part I. Clinical and neuropsychological assessment of Alzheimer’s disease. Neurology 1989, 39, 1159. [Google Scholar] [CrossRef]
- Schmid, N.S.; Ehrensperger, M.M.; Berres, M.; Beck, I.R.; Monsch, A.U. The Extension of the German CERAD Neuropsychological Assessment Battery with Tests Assessing Subcortical, Executive and Frontal Functions Improves Accuracy in Dementia Diagnosis. Dement. Geriatr. Cogn. Disord. Extra 2014, 4, 322–334. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American College of Sports Medicine. ACSM’s Guidelines for Exercise Testing and Prescription; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2006. [Google Scholar]
- Gilgen-Ammann, R.; Schweizer, T.; Wyss, T. RR interval signal quality of a heart rate monitor and an ECG Holter at rest and during exercise. Graefe’s Arch. Clin. Exp. Ophthalmol. 2019, 119, 1525–1532. [Google Scholar] [CrossRef]
- Speer, K.E.; Semple, S.; Naumovski, N.; McKune, A.J. Measuring Heart Rate Variability Using Commercially Available Devices in Healthy Children: A Validity and Reliability Study. Eur. J. Investig. Health Psychol. Educ. 2020, 10, 390–404. [Google Scholar] [CrossRef] [Green Version]
- Task Force of the European Society of Cardiology the North American Society of Pacing Electrophysiology. Heart rate variability: Standards of measurement, physiological interpretation, and clinical use. Circulation 1996, 93, 1043–1065. [Google Scholar] [CrossRef] [Green Version]
- Laborde, S.; Mosley, E.; Thayer, J.F. Heart Rate Variability and Cardiac Vagal Tone in Psychophysiological Research—Recommendations for Experiment Planning, Data Analysis, and Data Reporting. Front. Psychol. 2017, 8, 213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quintana, D.S.; Heathers, J. Considerations in the assessment of heart rate variability in biobehavioral research. Front. Psychol. 2014, 5, 805. [Google Scholar] [CrossRef] [PubMed]
- Fox, J.L.; O’Grady, C.J.; Scanlan, A.T.; Sargent, C.; Stanton, R. Validity of the Polar Team Pro Sensor for measuring speed and distance indoors. J. Sci. Med. Sport 2019, 22, 1260–1265. [Google Scholar] [CrossRef] [PubMed]
- Steinacker, J.M.; Liu, Y.; Reissnecker, S. Criteria for termination of ergometry. Sports Medicine Standards. Dtsch. Z. Sportmed. 2002, 53, 228–229. [Google Scholar]
- Scharhag-Rosenberger, F.; Schommer, K. Spiroergometry in sports medicine. German Z Sportmed. 2013, 64, 362–366. [Google Scholar]
- Shaffer, F.; Ginsberg, J.P. An Overview of Heart Rate Variability Metrics and Norms. Front. Public Health 2017, 5, 258. [Google Scholar] [CrossRef] [Green Version]
- Coswig, V.; Barbalho, M.; Raiol, R.; Del Vecchio, F.B.; Ramirez-Campillo, R.; Gentil, P. Effects of high vs moderate-intensity intermittent training on functionality, resting heart rate and blood pressure of elderly women. J. Transl. Med. 2020, 18, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Hopkins, W.G. Measures of Reliability in Sports Medicine and Science. Sports Med. 2000, 30, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Barbalho, M.D.S.M.; Gentil, P.; Izquierdo, M.; Fisher, J.; Steele, J.; Raiol, R.D.A. There are no no-responders to low or high resistance training volumes among older women. Exp. Gerontol. 2017, 99, 18–26. [Google Scholar] [CrossRef]
- Gurd, B.J.; Giles, M.D.; Bonafiglia, J.T.; Raleigh, J.P.; Boyd, J.C.; Ma, J.K.; Zelt, J.G.; Scribbans, T.D. Incidence of nonresponse and individual patterns of response following sprint interval training. Appl. Physiol. Nutr. Metab. 2016, 41, 229–234. [Google Scholar] [CrossRef] [PubMed]
- Herold, F.; Müller, P.; Gronwald, T.; Müller, N.G. Dose–response matters!—A perspective on the exercise prescription in ex-ercise–cognition research. Front. Psychol. 2019, 10, 2338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herold, F.; Törpel, A.; Hamacher, D.; Budde, H.; Gronwald, T. A Discussion on Different Approaches for Prescribing Physical Interventions—Four Roads Lead to Rome, but Which One Should We Choose? J. Pers. Med. 2020, 10, 55. [Google Scholar] [CrossRef]
- Impellizzeri, F.M.; Marcora, S.M.; Coutts, A.J. Internal and External Training Load: 15 Years On. Int. J. Sports Physiol. Perform. 2019, 14, 270–273. [Google Scholar] [CrossRef] [PubMed]
- Reimers, A.K.; Knapp, G.; Reimers, C.-D. Effects of Exercise on the Resting Heart Rate: A Systematic Review and Meta-Analysis of Interventional Studies. J. Clin. Med. 2018, 7, 503. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akwa, L.G.; Moses, M.O.; Emikpe, A.O.; Baffour-Awuah, B.; Asamoah, B.; Addai-Mensah, O.; Annani-Akollor, M.; Osei, F.; Appiah, E.J. Lipid profile, cardiorespiratory function and quality of life of postmenopausal women improves with aerobic exercise. J. Hum. Sport Exerc. 2017, 12, 12. [Google Scholar] [CrossRef] [Green Version]
- Broman, G.; Quintana, M.; Lindberg, T.; Jansson, E.; Kaijser, L. High intensity deep water training can improve aerobic power in elderly women. Graefe’s Arch. Clin. Exp. Ophthalmol. 2006, 98, 117–123. [Google Scholar] [CrossRef]
- Schmidt, J.F.; Hansen, P.R.; Andersen, T.R.; Andersen, L.J.; Hornstrup, T.; Krustrup, P.; Bangsbo, J. Cardiovascular adaptations to 4 and 12 months of football or strength training in 65- to 75-year-old untrained men. Scand. J. Med. Sci. Sports 2014, 24, 86–97. [Google Scholar] [CrossRef] [Green Version]
- Whitehurst, M.; Menendez, E. Endurance Training in Older Women—Lipid and Lipoprotein Responses. Phys. Sportsmed. 1991, 19, 95–103. [Google Scholar] [CrossRef]
- Cononie, C.C.; Graves, J.E.; Pollock, M.L.; Phillips, M.I.; Sumners, C.; Hagberg, J.M. Effect of exercise training on blood pressure in 70- to 79-yr-old men and women. Med. Sci. Sports Exerc. 1991, 23, 505–511. [Google Scholar] [CrossRef] [PubMed]
- Gurjão, A.L.D.; Carneiro, N.H.; Ceccato, M.; Gobbi, S.; Gonçalves, R.; Filho, J.C.J. Efeito do treinamento com pesos na pressão arterial de repouso em idosas normotensas. Rev. Bras. Med. Esporte 2013, 19, 160–163. [Google Scholar] [CrossRef] [Green Version]
- Marinda, F.; Magda, G.; Ina, S.; Brandon, S.; Abel, T.; Ter Goon, D. Effects of a mat pilates program on cardiometabolic pa-rameters in elderly women. Pak. J. Med. Sci. 2013, 29, 500–504. [Google Scholar] [CrossRef] [PubMed]
- Stiller-Moldovan, C.; Kenno, K.; McGowan, C.L. Effects of isometric handgrip training on blood pressure (resting and 24 h ambulatory) and heart rate variability in medicated hypertensive patients. Blood Press. Monit. 2012, 17, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Delecluse, C.; Colman, V.; Roelants, M.; Verschueren, S.; Derave, W.; Ceux, T.; Eijnde, B.O.; Seghers, J.; Pardaens, K.; Brumagne, S.; et al. Exercise programs for older men: Mode and intensity to induce the highest possible health-related benefits. Prev. Med. 2004, 39, 823–833. [Google Scholar] [CrossRef]
- Ohkubo, T.; Hozawa, A.; Nagatomi, R.; Fujita, K.; Sauvaget, C.; Watanabe, Y.; Anzai, Y.; Tamagawa, A.; Tsuji, I.; Imai, Y.; et al. Effects of exercise training on home blood pressure values in older adults: A randomized controlled trial. J. Hypertens. 2001, 19, 1045–1052. [Google Scholar] [CrossRef] [PubMed]
- Wood, R.H.; Reyes, R.; Welsch, M.A.; Favaloro-Sabatier, J.; Sabatier, M.; Matthew Lee, C.; Johnson, L.G.; Hooper, P.F. Con-current cardiovascular and resistance training in healthy older adults. Med. Sci. Sports Exerc. 2001, 33, 1751–1758. [Google Scholar] [CrossRef]
- Levy, W.; Cerqueira, M.D.; Harp, G.D.; Johannessen, K.-A.; Abrass, I.B.; Schwartz, R.S.; Stratton, J.R. Effect of endurance exercise training on heart rate variability at rest in healthy young and older men. Am. J. Cardiol. 1998, 82, 1236–1241. [Google Scholar] [CrossRef]
- Varas-Diaz, G.; Subramaniam, S.; Delgado, L.; Phillips, S.A.; Bhatt, T. Effect of an Exergaming-Based Dance Training Paradigm on Autonomic Nervous System Modulation in Healthy Older Adults: A Randomized Controlled Trial. J. Aging Phys. Act. 2021, 29, 1–9. [Google Scholar] [CrossRef]
- Eggenberger, P.; Annaheim, S.; Kündig, K.A.; Rossi, R.M.; Münzer, T.; De Bruin, E.D. Heart Rate Variability Mainly Relates to Cognitive Executive Functions and Improves Through Exergame Training in Older Adults: A Secondary Analysis of a 6-Month Randomized Controlled Trial. Front. Aging Neurosci. 2020, 12, 197. [Google Scholar] [CrossRef]
- Stein, P.K.; Ehsani, A.A.; Domitrovich, P.P.; Kleiger, R.E.; Rottman, J.N. Effect of exercise training on heart rate variability in healthy older adults. Am. Heart J. 1999, 138, 567–576. [Google Scholar] [CrossRef]
- Jakubec, A.; Stejskal, P.; Kovácová, L.; Elfmark, M.; Rehová, I.; Botek, M.; Petr, M. Changes in heart rate variability after a six month long aerobic dance or step-dance programm in women 40-65 years old: The influence of different degrees of adherence, intensity and initial levels. Acta Univ. Palacki. Olomuc. Gymn. 2008, 38, 35–44. [Google Scholar]
- Shen, T.-W.; Wen, H.-J. Aerobic Exercise Affects T-wave Alternans and Heart Rate Variability in Postmenopausal Women. Int. J. Sports Med. 2013, 34, 1099–1105. [Google Scholar] [CrossRef]
- Soares-Miranda, L.; Sattelmair, J.; Chaves, P.; Duncan, G.; Siscovick, D.S.; Stein, P.K.; Mozaffarian, D. Response to letter regarding article, “physical activity and heart rate variability in older adults: The cardiovascular health study”. Circulation 2015, 131, e349-50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schroeder, E.B.; Liao, D.; Chambless, L.E.; Prineas, R.J.; Evans, G.W.; Heiss, G. Hypertension, blood pressure, and heart rate variability: The Atherosclerosis Risk in Communities (ARIC) study. Hypertension 2003, 42, 1106–1111. [Google Scholar] [CrossRef] [Green Version]
- Schroeder, E.B.; Chambless, L.E.; Liao, D.; Prineas, R.J.; Evans, G.W.; Rosamond, W.D.; Heiss, G. Diabetes, Glucose, Insulin, and Heart Rate Variability: The Atherosclerosis Risk in Communities (ARIC) study. Diabetes Care 2005, 28, 668–674. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dekker, J.M.; Crow, R.S.; Folsom, A.R.; Hannan, P.J.; Liao, D.; Swenne, C.A.; Schouten, E.G. Low heart rate variability in a 2-minute rhythm strip predicts risk of coronary heart disease and mortality from several causes: The ARIC Study. Athero-sclerosis Risk in Communities. Circulation 2000, 102, 1239–1244. [Google Scholar] [CrossRef] [PubMed]
- Kubota, Y.; Chen, L.; Whitsel, E.A.; Folsom, A.R. Heart rate variability and lifetime risk of cardiovascular disease: The Atherosclerosis Risk in Communities Study. Ann. Epidemiol. 2017, 27, 619–625. [Google Scholar] [CrossRef]
- Hartaigh, B.Ó.; Gill, T.M.; Shah, I.; Hughes, A.; Deanfield, J.; Kuh, D.; Hardy, R. Association between resting heart rate across the life course and all-cause mortality: Longitudinal findings from the Medical Research Council (MRC) National Survey of Health and Development (NSHD). J. Epidemiol. Commun. Health 2014, 68, 883–889. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aune, D.; Sen, A.; o’Hartaigh, B.; Janszky, I.; Romundstad, P.R.; Tonstad, S.; Vatten, L.J. Resting heart rate and the risk of cardiovascular disease, total cancer, and all-cause mortality—A systematic review and dose-response meta-analysis of pro-spective studies. Nutr. Metab. Cardiovasc. Dis. 2017, 27, 504–517. [Google Scholar] [CrossRef]
- Stein, P.K.; Barzilay, J.I.; Chaves, P.H.M.; Domitrovich, P.P.; Gottdiener, J.S. Heart rate variability and its changes over 5 years in older adults. Age Ageing 2008, 38, 212–218. [Google Scholar] [CrossRef] [Green Version]
- Bahrainy, S.; Levy, W.; Busey, J.M.; Caldwell, J.H.; Stratton, J.R. Exercise training bradycardia is largely explained by reduced intrinsic heart rate. Int. J. Cardiol. 2016, 222, 213–216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, J.-S.; Chow, S.-E. Effects of exercise training and detraining on oxidized low-density lipoprotein-potentiated platelet function in men. Arch. Phys. Med. Rehabil. 2004, 85, 1531–1537. [Google Scholar] [CrossRef] [PubMed]
- Lombardi, F.; Malliani, A.; Pagani, M.; Cerutti, S. Heart rate variability and its sympatho-vagal modulation. Cardiovasc. Res. 1996, 32, 208–216. [Google Scholar] [CrossRef]
- Nunan, D.; Sandercock, G.R.H.; Brodie, D.A. A Quantitative Systematic Review of Normal Values for Short-Term Heart Rate Variability in Healthy Adults. Pacing Clin. Electrophysiol. 2010, 33, 1407–1417. [Google Scholar] [CrossRef]
- Adjei, T.; Von Rosenberg, W.; Nakamura, T.; Chanwimalueang, T.; Mandic, D.P. The ClassA Framework: HRV Based Assessment of SNS and PNS Dynamics Without LF-HF Controversies. Front. Physiol. 2019, 10, 505. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ernst, G. Heart-Rate Variability-More than Heart Beats? Front Public Health 2017, 5, 240. [Google Scholar] [CrossRef] [PubMed]
- Thayer, J.F.; Åhs, F.; Fredrikson, M.; Sollers, J.J.; Wager, T.D. A meta-analysis of heart rate variability and neuroimaging studies: Implications for heart rate variability as a marker of stress and health. Neurosci. Biobehav. Rev. 2012, 36, 747–756. [Google Scholar] [CrossRef]
- Müllers, P.; Taubert, M.; Müller, N.G. Physical Exercise as Personalized Medicine for Dementia Prevention? Front. Physiol. 2019, 10, 672. [Google Scholar] [CrossRef]
- Atkinson, G.; Batterham, A.M. True and false interindividual differences in the physiological response to an intervention. Exp. Physiol. 2015, 100, 577–588. [Google Scholar] [CrossRef] [Green Version]
- Atkinson, G.; Williamson, P.; Batterham, A.M. Issues in the determination of “responders” and “non-responders” in physio-logical research. Exp. Physiol. 2019, 104, 1215–1225. [Google Scholar] [CrossRef]
- Rodrigues, L.; Bherer, L.; Bosquet, L.; Vrinceanu, T.; Nadeau, S.; Lehr, L.; Bobeuf, F.; Kergoat, M.J.; Vu, T.T.M.; Berryman, N. Effects of an 8-week training cessation period on cognition and functional capacity in older adults. Exp. Gerontol. 2020, 134, 110890. [Google Scholar] [CrossRef] [PubMed]
- Bosquet, L.; Berryman, N.; Dupuy, O.; Mekary, S.; Arvisais, D.; Bherer, L.; Mujika, I. Effect of training cessation on muscular performance: A meta-analysis. Scand. J. Med. Sci. Sports 2013, 23, e140–e149. [Google Scholar] [CrossRef] [PubMed]
- Vitale, J.A.; Bonato, M.; Borghi, S.; Messina, C.; Albano, D.; Corbetta, S.; Sconfienza, L.M.; Banfi, G. Home-Based Resistance Training for Older Subjects during the COVID-19 Outbreak in Italy: Preliminary Results of a Six-Months RCT. Int. J. Environ. Res. Public Health 2020, 17, 9533. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Physical Performance Parameters | |
|---|---|
| Total distance (m) | Total distance during the training session, particularly during the Dance choreographies and the fitness Dance parts (in meters). |
| Distance/min (m/min) | Average distance per minute during the training session, particularly during the Dance choreographies and the fitness Dance parts (in meters). |
| Maximum speed (km/h) | Maximum speed during the training session. Particularly during the Dance choreographies and the fitness Dance parts (kilometre/hour) |
| Average speed (km/h) | Average speed during the training session, particularly during the Dance choreographies and the fitness Dance parts (kilometre/hour) |
| Physiological parameters | |
| Minimum Heart rate (HRmin) | Resting HR before the training session calculated as (bpm) and as % of the HR max (% HR max). A recording duration of 3 min, prior to test sessions, in a standing position was used. In the absence of pathologies or use of pharmaceuticals, a low resting HR indicates, in general, a healthy heart. |
| Maximal heart rate (HRmax) | Maximal HR during the training session calculated as “bpm” and as % of the HR max (% HR max). |
| Average heart rate (HRavg) | Average HR during the training session calculated as “bpm” and as % of the HR max (% HR max). |
| Average RR interval (Avg RR) | Average beat-to-beat interval during the training session (ms). Increase over time means that fitness is improving. |
| Maximum RR interval (Max RR) | Maximum time between successive heartbeats (beat-to-beat interval) recorded during the training session (milliseconds). |
| HRV (RMSSD) | The root mean square of successive differences between normal heartbeats (RMSSD) is obtained by first calculating each successive time difference between heartbeats in milliseconds (ms). Each of the values is then squared and the result is averaged before the square root of the total is obtained. The RMSSD reflects the beat-to-beat variance in HR and reflects short-term HR variability HRV [62]. High resting-state HRV is related to improved health and indicates that the heart is functioning well, and that the autonomic nervous system is adapting to the demands placed on it. https://www.polar.com/blog/heart-rate-variability-and-orthostatic-test-lets-talk-polar/ (accessed on 20 April 2021) |
| Time in HR zone 1 | HR zones are a way to monitor the training intensity. There are five HR zones based on the intensity of training with regard to the maximum heart rate. The % of HR max in each zone are as following: Zone 1: 50–60%, Zone 2: 60–70%, Zone 3: 70–80%, Zone 4: 80–90%, Zone 5: 90–100%. (https://www.polar.com/blog/running-heart-rate-zones-basics/). In the present paper, the time in each HR zone was calculated as % of the whole session time (e.g., spending 20 min in zone 1 during a 90 min session → Time in HR zone 1 = 22.22%) |
| Time in HR zone 2 | |
| Time in HR zone 3 | |
| Time in HR zone 4 | |
| Time in HR zone 5 | |
| Training Load | |
| Training load score | Training Load includes textual feedback on the strenuousness of a single training session. It is based on the intensity and duration of a training session, with the intensity of a session measured using HR, and the calculation is further affected by personal information such as age, sex, weight, VO2max, and training history. As a participant’s fitness improves, the same training session creates less training load. https://support.polar.com/en/support/the_what_and_how_of_training_load (accessed on 20 April 2021) |
| Variable | Mean ± SD | Range |
|---|---|---|
| Gender | ||
| Female (%) | 50% | |
| Anthropometric | ||
| Age (years) | 73 ± 4.4 | 67 to 79 |
| Height (m) | 1.72 ± 0.08 | 160 to 183 |
| Body mass (kg) | 75.33 ± 6.39 | 63 to 84 |
| BMI (kg/m2) | 25.45 ± 1.97 | 20.9 to 27.8 |
| CERAD-Plus (z scores) | ||
| Verbal Fluency | −0.38 ± 1.07 | −1.51 to 2.44 |
| Boston Naming | −0.40 ± 0.74 | −1.59 to 1.04 |
| MMSE | −2.26 ± 0.67 | −3.31 to −0.66 |
| Word List Learning | −1.41 ± 0.74 | −2.27 to −0.11 |
| Word List Recall | −1.27 ± 0.99 | −2.75 to 0.20 |
| Word List Intrusions | −0.46 ± 1.32 | −2.46 to 0.86 |
| Word List Savings | −0.97 ± 1.16 | −2.73 to 1.01 |
| Word List Recognizing | −0.83 ± 1.11 | −2.00 to 0.97 |
| Figures Drawing | −0.23 ± 1.38 | −2.63 to 1.02 |
| Figures Recall | −0.67 ± 1.35 | −2.35 to 1.17 |
| Figures Saving | −0.40 ± 1.31 | −2.18 to 2.01 |
| TMT-A | −0.51 ± 0.84 | −2.12 to 0.98 |
| TMT-B | −0.59 ± 0.86 | −1.51 to 0.96 |
| S Words | 0.24 ± 1.15 | −1.49 to 1.67 |
| PAR-Q | ||
| Yes responses | 1.67 ± 0.89 | 0–3 |
| No responses | 7.33 ± 0.89 | 3–9 |
| Cardiorespiratory fitness | ||
| VO2max (l/min) | 23.08 ± 7.86 | 14 to 34 |
| HR max (beat/min) | 143.27 ± 18.17 | 118–169 |
| T1 | T2 | T3 | Δ from T1 to T2 | Δ from T2 to T3 | Friedman ANOVA | p Value | Effect Size | |
|---|---|---|---|---|---|---|---|---|
| % time in HR zone 1 (50–59%) | 19.4 ± 19.2 * | 44.0 ± 29.7 | 21.1 ± 19.5 * | 25 ± 25 | −23 ± 25 | test = 16.16 | <0.0005 | 0.67 |
| % time in HR zone 2 (60–69%) | 47.6 ± 15.0 | 42.4 ± 19.0 | 49.8 ± 17.2 | −05 ± 24 | 07 ± 25 | test = 1.16 | 0.55 | 0.04 |
| % time in HR zone 3 (70–79%) | 29.1 ± 21.6 * | 12.5 ± 13.6 | 24.8 ± 20.8* | −17 ± 17 | 12 ± 13 | test = 18.16 | <0.0005 | 0.75 |
| % time in HR zone 4 (80–89%) | 03.7 ± 04.0 | 01.3 ± 01.6 | 03.7 ± 02.7 * | −02 ± 04 | 02 ± 02 | test = 8.41 | 0.01 | 0.35 |
| % time in HR zone 5 (90–100%) | 0.1 ± 0.4 | 00 | 00 | −0.1 ± 0.4 | 00 | test = 2.0 | 0.36 | 0.08 |
| T1 | T2 | T3 | Δ from T1 to T2 | Δ from T2 to T3 | ANOVA | p Value | Effect Size | |
|---|---|---|---|---|---|---|---|---|
| Total distance [m] | 712.0 ± 409.5 * | 1049.9 ± 493.4 | 702.6 ± 454.1 * | 338 ± 290 | −347 ± 410 | F = 7.64 | 0.003 | 0.41 |
| Distance/min [m/min] | 08.4 ± 4.6 * | 12.4 ± 06.1 | 10.2 ± 06.4 | 04 ± 04 | −02 ± 05 | F = 4.26 | 0.02 | 0.27 |
| Maximum speed [km/h] | 07.3 ± 2.7 | 07.8 ± 02.3 | 07.1 ± 02.3 | 0.5 ± 03 | −0.7 ± 02 | test = 1.16 | 0.55 | 0.04 |
| Average speed [km/h] | 0.5 ± 0.3 * | 0.8 ± 0.4 | 0.6 ± 0.4 | 0.3 ± 0.2 | −0.2 ± 0.3 | F = 5.45 | 0.01 | 0.33 |
| Responsiveness to Training/Detraining Adaptations | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Participants Number | HR (bpm) | HRV Related Parameters (ms) | Physical Performance and Strenuousness Indicators | ||||||
| HR Min | HR Avg | HR Max | Max RR | Avg RR | HRV (RMSSD) | Total Distance (m) | Avg Speed (km/h) | Load Score | |
| Responsiveness to 8 week Fitness-Dance training | |||||||||
| RT | −1.51 | −2.26 | −2.01 | 241.85 | 22.01 | 1.3 | 71.16 | 0.07 | −11.9 |
| Responders | 11 | 10 | 9 | 9 | 9 | 11 | 10 | 9 | 6 |
| Non-Responders | 1 | 2 | 3 | 3 | 3 | 1 | 2 | 3 | 6 |
| Non-responders % | 8% | 17% | 25% | 25% | 25% | 8% | 17% | 25% | 50% |
| Responsiveness to 4 week COVID-19-induced detraining | |||||||||
| RT | 1.11 | 2.01 | 2.21 | −332 | −24.9 | −2.5 | −129 | −0.08 | 1.59 |
| Responders | 11 | 9 | 10 | 8 | 9 | 7 | 7 | 5 | 5 |
| Non-Responders | 1 | 3 | 2 | 4 | 3 | 5 | 5 | 8 | 8 |
| % Responders | 92% | 75% | 83% | 67% | 75% | 58% | 58% | 42% | 42% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ammar, A.; Boukhris, O.; Halfpaap, N.; Labott, B.K.; Langhans, C.; Herold, F.; Grässler, B.; Müller, P.; Trabelsi, K.; Chtourou, H.; et al. Four Weeks of Detraining Induced by COVID-19 Reverse Cardiac Improvements from Eight Weeks of Fitness-Dance Training in Older Adults with Mild Cognitive Impairment. Int. J. Environ. Res. Public Health 2021, 18, 5930. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115930
Ammar A, Boukhris O, Halfpaap N, Labott BK, Langhans C, Herold F, Grässler B, Müller P, Trabelsi K, Chtourou H, et al. Four Weeks of Detraining Induced by COVID-19 Reverse Cardiac Improvements from Eight Weeks of Fitness-Dance Training in Older Adults with Mild Cognitive Impairment. International Journal of Environmental Research and Public Health. 2021; 18(11):5930. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115930
Chicago/Turabian StyleAmmar, Achraf, Omar Boukhris, Nicole Halfpaap, Berit Kristin Labott, Corinna Langhans, Fabian Herold, Bernhard Grässler, Patrick Müller, Khaled Trabelsi, Hamdi Chtourou, and et al. 2021. "Four Weeks of Detraining Induced by COVID-19 Reverse Cardiac Improvements from Eight Weeks of Fitness-Dance Training in Older Adults with Mild Cognitive Impairment" International Journal of Environmental Research and Public Health 18, no. 11: 5930. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115930