
Incidence of Reported Flu-Like Syndrome Cases in Brazilian Health Care Workers in 2020 (March to June)


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Data Organization and Variable
2.3. Data Analysis
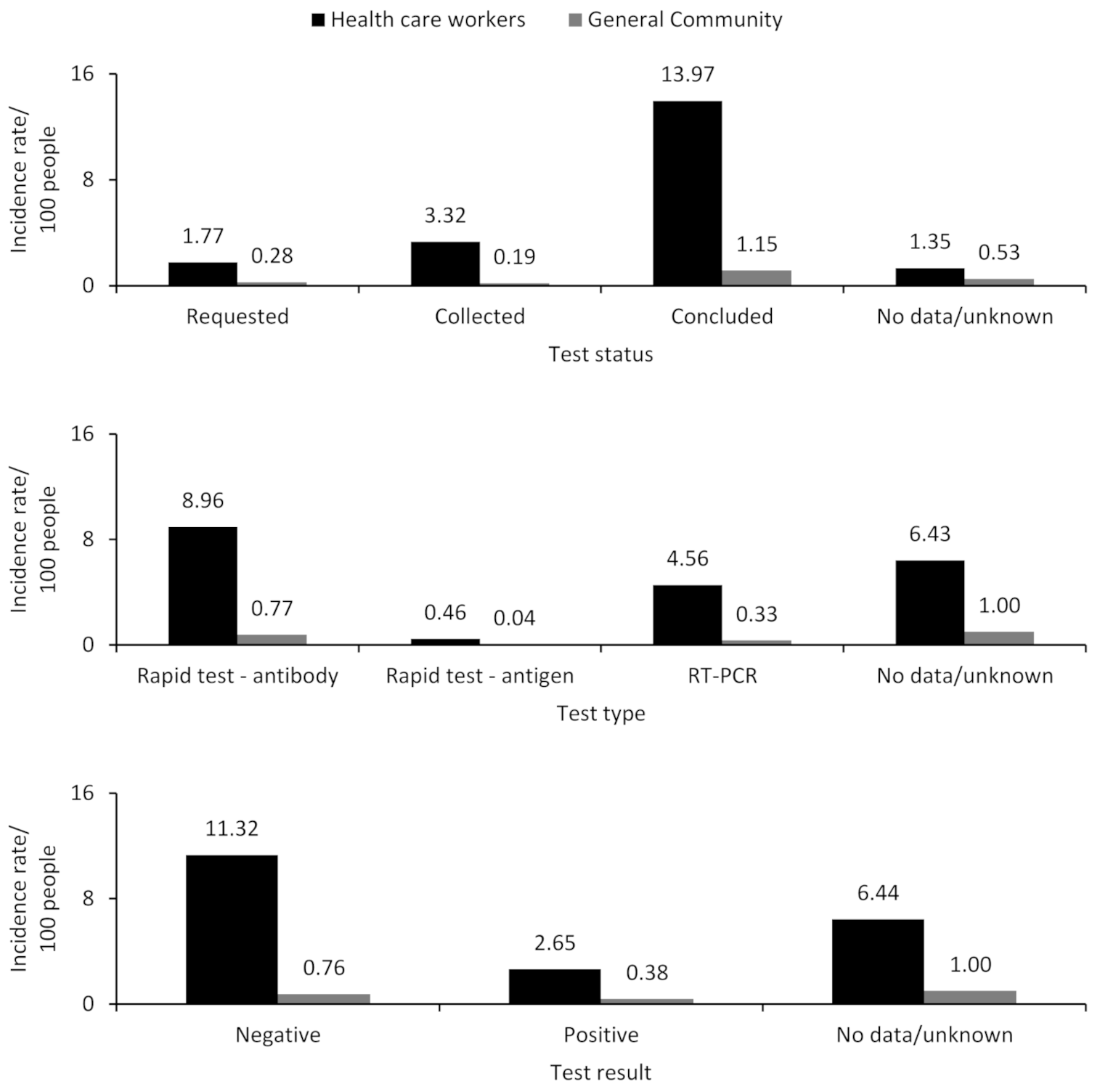
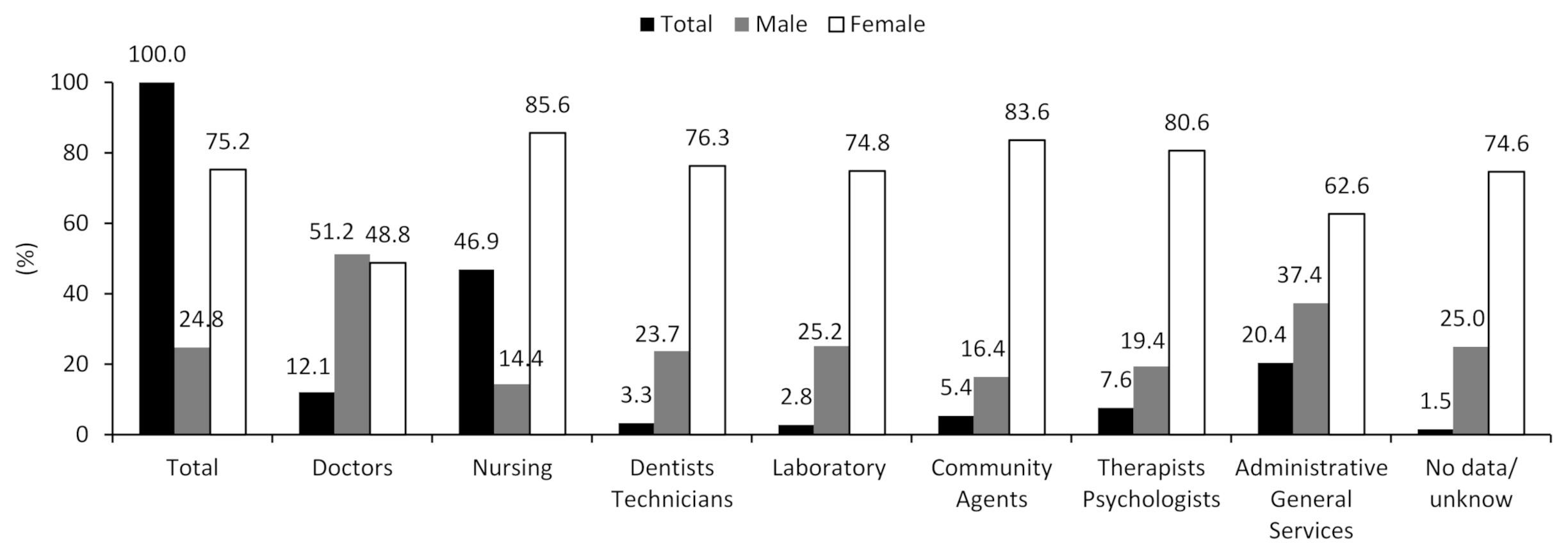
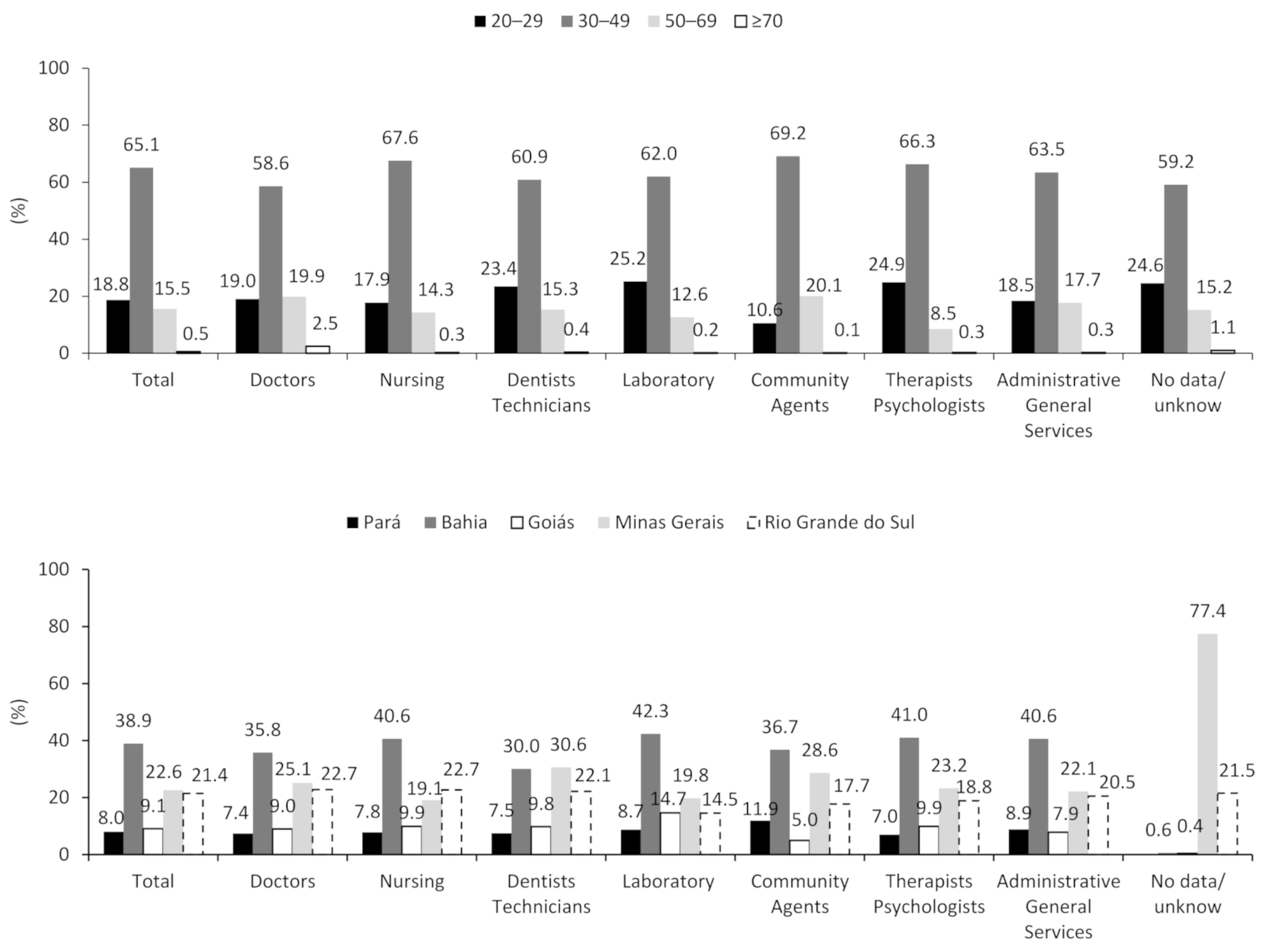
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lancet Team. Health and care workers are owed a better future. Lancet 2021, 397, 347. [Google Scholar] [CrossRef]
- Gómez-Ochoa, S.A.; Franco, O.H.; Rojas, L.Z.; Raguindin, P.F.; Roa-Díaz, Z.M.; Wyssmann, B.M.; Guevara, S.L.R.; Echeverría, L.E.; Glisic, M.; Muka, T. COVID-19 in health-care workers: A living systematic review and meta-analysis of prevalence, risk factors, clinical characteristics, and outcomes. Am. J. Epidemiol. 2021, 190, 161–175. [Google Scholar] [CrossRef] [PubMed]
- Ran, L.; Chen, X.; Wang, Y.; Wu, W.; Zhang, L.; Tan, X. Risk factors of healthcare workers with corona virus disease 2019: A retrospective cohort study in a designated hospital of Wuhan in China. Clin. Infect Dis. 2020, 71, 2218–2221. [Google Scholar] [CrossRef] [Green Version]
- Zhou, P.; Huang, Z.; Xiao, Y.; Huang, X.; Fan, X.G. Protecting Chinese healthcare workers while combating the 2019 novel coronavirus. Infect. Control Hosp. Epidemiol. 2020, 41, 745–746. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brasil. Ministério da Saúde. Conselho Nacional de Saúde. Parecer Técnico nº 128/2020. Proteção Física e Psicológica dos Trabalhadores da Saúde no Enfrentamento à Pandemia da COVID-19. Available online: http://renastonline.ensp.fiocruz.br/sites/default/files/arquivos/recursos/recomendacao_020_2020_cns.pdf (accessed on 24 March 2021).
- Michaels, D.; Wagner, G.R. Occupational Safety and Health Administration (OSHA) and Worker Safety During the COVID-19 Pandemic. JAMA 2020, 324, 1389–1390. [Google Scholar] [CrossRef]
- Sikkema, R.S.; Pas, S.D.; Nieuwenhuijse, D.F.; O’Toole, A.; Verweij, J.; van der Linden, A.; Chestakova, I.; Schapendonk, C.; Pronk, M.; Lexmond, P.; et al. COVID-19 in health-care workers in three hospitals in the south of the Netherlands: A cross-sectional study. Lancet Infect Dis. 2020, 20, 1273–1280. [Google Scholar] [CrossRef]
- Taylor, J.; Carter, R.J.; Lehnertz, N.; Kazazian, L.; Sullivan, M.; Wang, X.; Garfin, J.; Diekman, S.; Plumb, M.; Bennet, M.E.; et al. Minnesota Long-Term Care COVID-19 Response Group. Serial testing for sars-cov-2 and virus whole genome sequenc-ing inform infection risk at two skilled nursing facilities with COVID-19 outbreaks-Minnesota, April–June 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 1288–1295. [Google Scholar] [CrossRef] [PubMed]
- Souza, W.M.; Buss, L.F.; Candido, D.S.; Carrera, J.P.; Li, S.; Zarebski, A.E.; Pereira, R.H.M.; Prete, C.A., Jr.; Souza-Santos, A.A.; Parag, K.V.; et al. Epidemiological and clinical characteristics of the COVID-19 epidemic in Brazil. Nat. Hum. Behav. 2020, 4, 856–865. [Google Scholar] [CrossRef]
- Silveira, M.F.; Barros, A.J.D.; Horta, B.L.; Pellanda, L.C.; Victora, G.D.; Dellagostin, O.A.; Struchiner, C.J.; Burattini, M.N.; Valim, A.R.M.; Berlezi, E.M.; et al. Repeated population-based surveys of antibodies against SARS-CoV-2 in Southern Brazil. Nat. Med. 2020, 26, 1196–1199. [Google Scholar] [CrossRef]
- Valente, E.P.; Damásio, L.C.V.C.; Luz, L.S.; Pereira, M.F.S.; Lazzerini, M. COVID-19 among health workers in Brazil: The silent wave. J. Glob. Health 2020, 10, 010379. [Google Scholar] [CrossRef]
- Brasil. Ministério da Saúde. Secretaria de Atenção Primária à Saúde (SAPS). Protocolo de Manejo Clínico do Coronavírus (COVID-19) na Atenção Primária à Saúde. Available online: https://portaldeboaspraticas.iff.fiocruz.br/atencao-crianca/atencao-primaria-orientacoes-do-ministerio-da-saude-sobre-covid-19/ (accessed on 31 January 2021).
- Bhopal, R. Covid-19 worldwide: We need precise data by age group and sex urgently. BMJ 2020, 369, m1366. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pijls, B.G.; Jolani, S.; Atherley, A.; Derckx, R.T.; Dijkstra, J.I.; Franssen, G.H.; Hendriks, S.; Richters, A.; Venemans-Jellema, A.; Zalpuri, S.; et al. Demographic risk factors for COVID-19 infection, severity, ICU admission and death: A meta-analysis of 59 studies. BMJ Open 2021, 11, e044640. [Google Scholar] [CrossRef] [PubMed]
- Brasil. Ministério da Saúde. SRAG 2020: Banco de Dados de Síndrome Respiratória Aguda Grave. Available online: https://opendatasus.saude.gov.br/ (accessed on 22 March 2021).
- Iser, B.P.M.; Sliva, I.; Raymundo, V.T.; Poleto, M.B.; Schuelter-Trevisol, F.; Bobinski, F. Suspected COVID-19 case definition: A narrative review of the most frequent signs and symptoms among confirmed cases. Epidemiol. Serviços Saúde 2020, 29, e2020233. [Google Scholar]
- Brasil. Ministério da Saúde do Brasil (BR). Covid-19: Definição de Caso e Notificação [Internet]. 2020. Available online: https://coronavirus.saude.gov.br/definicao-de-caso-e-notificacao (accessed on 31 January 2021).
- Brasil. Ministério da Saúde. Sistema e-SUS Notifica. Available online: https://notifica.saude.gov.br/login (accessed on 2 March 2021).
- World Health Organization. Global Atlas of the Health Workforce. Available online: https://www.who.int/workforcealliance/knowledge/resources/hrhglobalatlas/en/ (accessed on 10 October 2020).
- Brasil. Ministério da Saúde. Cadastro Nacional de Estabelecimentos de Saúde. Available online: http://cnes.datasus.gov.br/ (accessed on 4 March 2021).
- Instituto Brasileiro de Geografia e Estatística. Pesquisa Nacional por Amostra de Domicílios: PNAD COVID19. Resultado mensal: Maio de 2020. Available online: https://biblioteca.ibge.gov.br/visualizacao/livros/liv101727.pdf (accessed on 19 March 2021).
- Lima, F.E.T.; Albuquerque, N.L.S.D.; Florencio, S.D.S.G.; Fontenele, M.G.M.; Queiroz, A.P.O.; Lima, G.A.; Barbosa, L.P. Time interval between onset of symptoms and COVID-19 testing in Brazilian state capitals, August 2020. Epidemiol. Serviços Saúde 2020, 30, e2020788. [Google Scholar] [CrossRef]
- Brasil. Ministério da Saúde. Secretaria de Vigilância em Saúde. Ficha de Investigação de SG Suspeito de Doença pelo Coronavírus 2019–COVID-19. Available online: https://egestorab.saude.gov.br/image/?file=20200429_N_Fichae-SUSVE_5220668342419003136.pdf (accessed on 17 March 2021).
- Brasil. Ministério da Saúde. Conselho Nacional de Saúde. Resolução nº 466, de 12 de Setembro de 2012. Available online: https://bvsms.saude.gov.br/bvs/saudelegis/cns/2013/res0466_12_12_2012.html (accessed on 11 February 2021).
- Brasil. Ministério da Saúde. Conselho Nacional de Saúde. Resolução nº 510, de 7 de Abril de 2016. Available online: http://bvsms.saude.gov.br/bvs/saudelegis/cns/2016/res0510_07_04_2016.html (accessed on 19 March 2021).
- Jesus, J.G.; Sacchi, C.; Candido, D.d.; Claro, I.M.; Sales, F.C.S.; Manuli, E.R.; da Silva, D.B.B.; de Paiva, T.M.; Pinho, M.A.B.; Santos, K.C.d.; et al. Importação e transmissão local antecipada de COVID-19 no Brasil, 2020. Rev. Inst. Med. Trop. 2020, 62, e30. [Google Scholar] [CrossRef] [PubMed]
- Magno, L.; Rossi, T.A.; Mendonça-Lima, F.W.D.; Santos, C.C.D.; Campos, G.B.; Marques, L.M. Challenges and proposals for scaling up COVID-19 testing and diagnosis in Brazil. Cien. Saude Coletiva. 2020, 25, 3355–3364. [Google Scholar] [CrossRef] [PubMed]
- Brasil. Ministério da Saúde. Secretaria de Vigilância em Saúde. Recomendações de Proteção aos Trabalhadores dos Serviços de Saúde no Atendimento de COVID-19 e Outras Síndromes Gripais, Brasília. 2020. Available online: https://portalarquivos.saude.gov.br/images/pdf/2020/April/16/01-recomendacoes-de-protecao.pdf (accessed on 19 March 2021).
- Machado, M.H. Perfil da Enfermagem no Brasil: Relatório Final. Rio de Janeiro; NERHUS-DAPS-ENSP/Fiocruz. 2017. Available online: https://pesquisa.bvsalud.org/portal/resource/pt/biblio-1094873 (accessed on 20 March 2021).
- Mostafa, A.; Kandil, S.; El-Sayed, M.H.; Girgis, S.; Hafez, H.; Yosef, M.; Saber, S.; Ezzelarab, H.; Ramadan, M.; Afifi, I.; et al. Universal COVID-19 screening of 4040 health care workers in a resource-limited setting: An Egyptian pilot model in a uni-versity with 12 public hospitals and medical centers. Int. J. Epidemiol. 2021, 50, 50–61. [Google Scholar] [CrossRef]
- Lancet Team. The gendered dimensions of COVID-19. Lancet 2020, 395, 1168. [Google Scholar] [CrossRef]
- Abbas, M.; Nunes, T.R.; Martischang, R.; Zingg, W.; Iten, A.; Pittet, D.; Harbarth, S. Nosocomial transmission and out-breaks of coronavirus disease 2019: The need to protect both patients and healthcare workers. Antimicrob. Resist. Infect. Control 2021, 10, 1–13. [Google Scholar] [CrossRef]
- Brasil. Ministério da Saúde. Portaria Nº 344, de 1º de fevereiro de 2017. Dispõe Sobre o Preenchimento do Quesito Raça/Cor nos Formulários dos Sistemas de Informação em Saúde. Diário Oficial da União, em: 02/02/2017. Available online: https://www.in.gov.br/web/dou/-/portaria-n-344-de-1-de-fevereiro-de-2017-20785508 (accessed on 18 January 2021).
- Oliveira, R.G.D.; Cunha, A.P.D.; Gadelha, A.G.D.S.; Carpio, C.G.; Oliveira, R.B.D.; Corrêa, R.M. Desigualdades raciais e a morte como horizonte: Considerações sobre a COVID-19 e o racismo estrutural. Cad. Saude Publica 2020, 36, e00150120. [Google Scholar] [CrossRef]
- Krastinova, E.; Garrait, V.; Lecam, M.T.; Coste, A.; Varon, E.; Delacroix, I.; Amine, S.A.; Jung, C.; Smati, M.; Cherbit, M. Household transmission and incidence of positive SARS-CoV-2 RT-PCR in symptomatic healthcare workers, clinical course and outcome: A French hospital experience. Occup. Environ. Med. 2020. Online ahead of print. [Google Scholar] [CrossRef]
- Hunter, E.; Price, D.A.; Murphy, E.; van der Loeff, I.S.; Baker, K.F.; Lendrem, D.; Lendrem, C.; Schmid, M.L.; Pareja-Cebrian, L.; Welch, A.; et al. First experience of COVID-19 screening of health-care workers in England. Lancet 2020, 395, e77–e78. [Google Scholar] [CrossRef]
- Wu, Z.; McGoogan, J.M. Characteristics of and important lessons from the coronavírus disease 2019 (COVID-19) outbreak in China: Summary of a report of 72314 cases from the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef]
- Bonilha, E.D.A.; Vico, E.S.R.; Freitas, M.D.; Barbuscia, D.M.; Galleguillos, T.G.B.; Okamura, M.N.; Santos, P.C.; Lira, M.M.T.A.; Torloni, M.R. Cobertura, completude e confiabilidade das informações do Sistema de Informações sobre Nasci-dos Vivos de maternidades da rede pública no município de São Paulo, 2011. Epidemiol. Serviços Saúde 2018, 27, e201712811. [Google Scholar]
- Drumond, E.D.F.; Machado, C.J.; Vasconcelos, M.D.R.; França, F. Utilização de dados secundários do SIM, Sinasc e SIH na produção científica brasileira de 1990 a 2006. Rev. Bras. Estud. Popul. 2009, 26, 7–19. [Google Scholar] [CrossRef] [Green Version]
- Baker, M.G.; Peckham, T.K.; Seixas, N.S. Estimating the burden of United States workers exposed to infection or disease: A key factor in containing risk of COVID-19 infection. PLoS ONE 2020, 15, e0232452. [Google Scholar] [CrossRef] [PubMed]
- Calò, F.; Russo, A.; Camaioni, C.; de Pascalis, C.N. Burden, risk assessment, surveillance and management of SARS-CoV-2 infection in health workers: A scoping review. Infect Dis. Poverty 2020, 9, 1–11. [Google Scholar] [CrossRef]
- Baqui, B.I.; Marra, V.; Ercole, A.; van der Schaar, M. Ethnic and regional variations in hospital mortality from COVID-19 in Brazil: A cross-sectional observational study. Lancet Global Health 2020, 8, E1018–E1026. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Total b | HCWs | General Community | p-Value c | |||
|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | ||
| Sex | |||||||
| Male | 501,179 | 45.48 | 46,123 | 24.79 | 442,022 | 49.77 | p < 0.001 |
| Female | 600,623 | 54.51 | 139,910 | 75.20 | 446,010 | 50.22 | |
| No data/unknown | 104 | 0.01 | 11 | 0.01 | 19 | 0.00 | |
| Age group (years) | |||||||
| 20–29 | 244,101 | 22.15 | 34,885 | 18.75 | 202,984 | 22.86 | p < 0.001 |
| 30–49 | 579,704 | 52.61 | 121,206 | 65.15 | 443,173 | 49.90 | |
| 50–69 | 221,189 | 20.07 | 28,914 | 15.54 | 187,142 | 21.07 | |
| 70 or older | 56,912 | 5.16 | 1039 | 0.56 | 54,752 | 6.17 | |
| States | |||||||
| Pará | 163,377 | 14.83 | 14,961 | 8.04 | 147,014 | 16.55 | p < 0.001 |
| Bahia | 287,179 | 26.06 | 72,398 | 38.91 | 211,064 | 23.77 | |
| Goiás | 109,194 | 9.91 | 16,882 | 9.07 | 90,212 | 10.16 | |
| Minas Gerais | 348,586 | 31.63 | 41,965 | 22.56 | 287,701 | 32.40 | |
| Rio Grande do Sul | 193,570 | 17.57 | 39,838 | 21.41 | 152,060 | 17.12 | |
| Total | 1,101,906 | 100.00 | 186,044 | 100.00 | 888,051 | 100.00 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Assunção, A.Á.; Maia, E.G.; Jardim, R.; de Araújo, T.M. Incidence of Reported Flu-Like Syndrome Cases in Brazilian Health Care Workers in 2020 (March to June). Int. J. Environ. Res. Public Health 2021, 18, 5952. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115952
Assunção AÁ, Maia EG, Jardim R, de Araújo TM. Incidence of Reported Flu-Like Syndrome Cases in Brazilian Health Care Workers in 2020 (March to June). International Journal of Environmental Research and Public Health. 2021; 18(11):5952. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115952
Chicago/Turabian StyleAssunção, Ada Ávila, Emanuella Gomes Maia, Renata Jardim, and Tânia Maria de Araújo. 2021. "Incidence of Reported Flu-Like Syndrome Cases in Brazilian Health Care Workers in 2020 (March to June)" International Journal of Environmental Research and Public Health 18, no. 11: 5952. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115952