
Urinary Phthalate Levels Associated with the Risk of Nonalcoholic Fatty Liver Disease in Adults: The Korean National Environmental Health Survey (KoNEHS) 2012–2014


Abstract
:1. Introduction
2. Materials and Methods
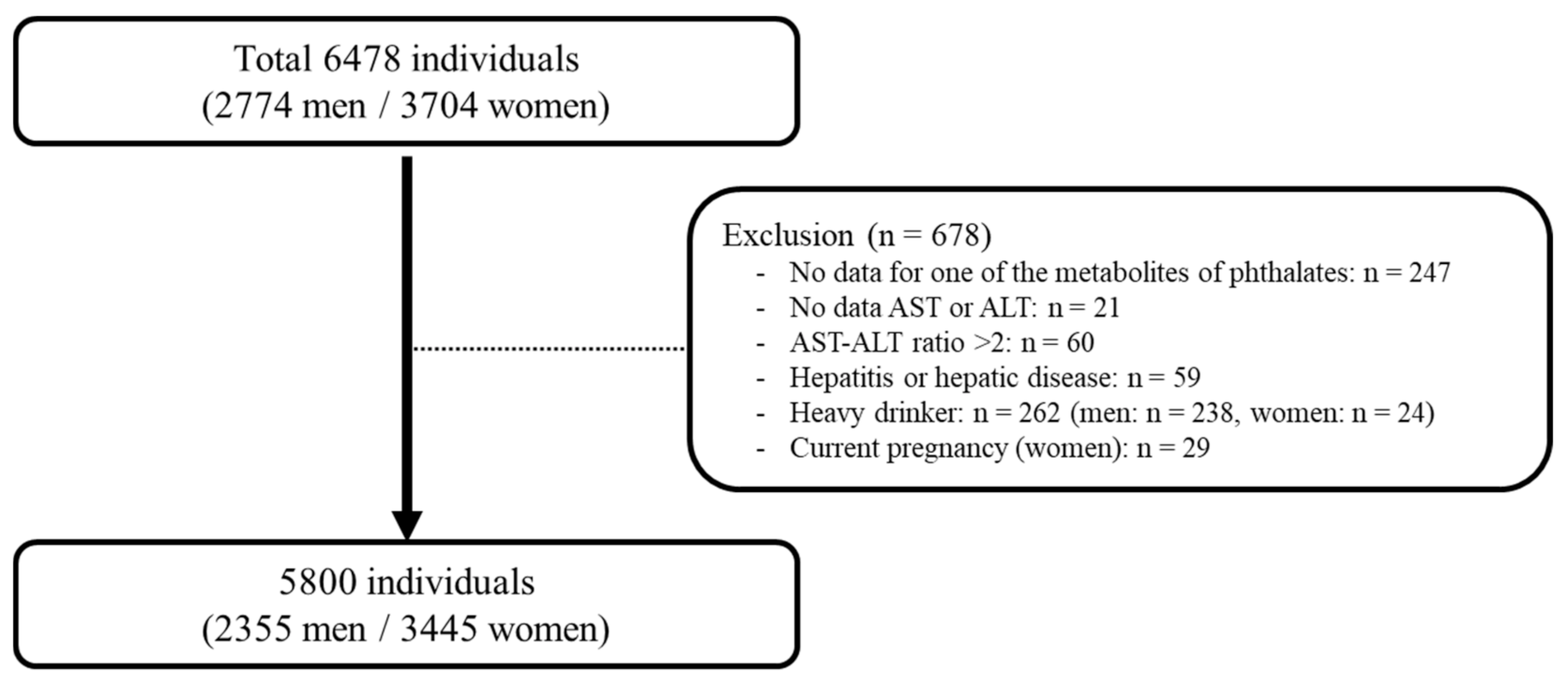
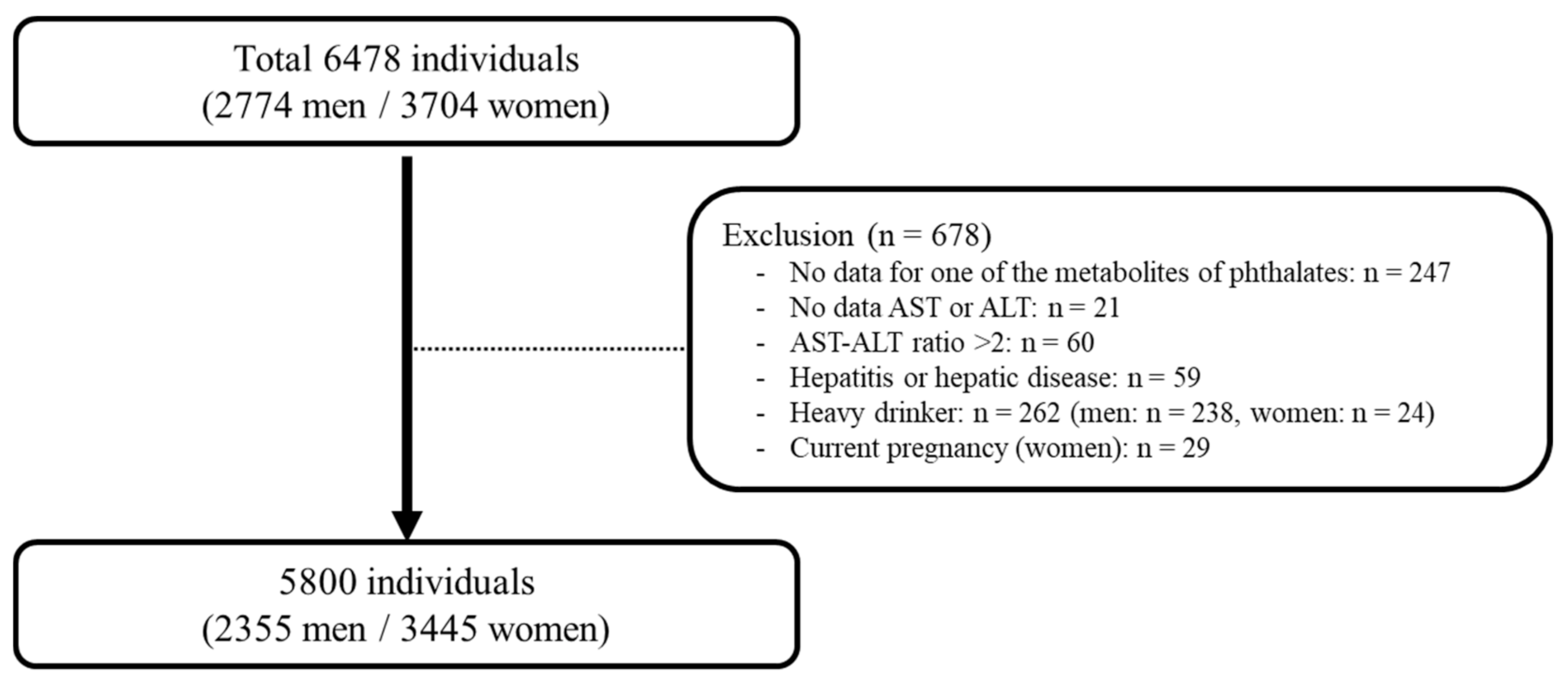
2.1. Study Design and Participants
2.2. Questionnaires and Anthropometric Parameters
2.3. Definition of NAFLD
2.4. Statistical Analysis
3. Results
3.1. General Characteristics
3.2. Urinary Levels of Phthalate Metabolites
3.3. The Association between Urinary Phthalate Metabolites and HSI Score
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Angulo, P. Nonalcoholic fatty liver disease. N. Engl. J. Med. 2002, 346, 1221–1231. [Google Scholar] [CrossRef] [Green Version]
- Loomba, R.; Sanyal, A.J. The global NAFLD epidemic. Nat. Rev. Gastroenterol. Hepatol. 2013, 10, 686–690. [Google Scholar] [CrossRef]
- Jeong, E.H.; Jun, D.W.; Cho, Y.K.; Choe, Y.G.; Ryu, S.; Lee, S.M.; Jang, E.C. Regional prevalence of non-alcoholic fatty liver disease in Seoul and Gyeonggi-do, Korea. Clin. Mol. Hepatol. 2013, 19, 266–272. [Google Scholar] [CrossRef] [PubMed]
- Sarwar, R.; Pierce, N.; Koppe, S. Obesity and nonalcoholic fatty liver disease: Current perspectives. Diabetes Metab. Syndr. Obes. 2018, 11, 533–542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, C.D.; Stengel, J.; Asike, M.I.; Torres, D.M.; Shaw, J.; Contreras, M.; Landt, C.L.; Harrison, S.A. Prevalence of nonalcoholic fatty liver disease and nonalcoholic steatohepatitis among a largely middle-aged population utilizing ultrasound and liver biopsy: A prospective study. Gastroenterology 2011, 140, 124–131. [Google Scholar] [CrossRef]
- Thayer, K.A.; Heindel, J.J.; Bucher, J.R.; Gallo, M.A. Role of environmental chemicals in diabetes and obesity: A National Toxicology Program workshop review. Environ. Health Perspect. 2012, 120, 779–789. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Polyzos, S.A.; Kountouras, J.; Deretzi, G.; Zavos, C.; Mantzoros, C.S. The emerging role of endocrine disruptors in pathogenesis of insulin resistance: A concept implicating nonalcoholic fatty liver disease. Curr. Mol. Med. 2012, 12, 68–82. [Google Scholar] [CrossRef]
- Ben-Jonathan, N.; Hugo, E.R.; Brandebourg, T.D. Effects of bisphenol A on adipokine release from human adipose tissue: Implications for the metabolic syndrome. Mol. Cell. Endocrinol. 2009, 304, 49–54. [Google Scholar] [CrossRef] [Green Version]
- Lim, S.; Cho, Y.M.; Park, K.S.; Lee, H.K. Persistent organic pollutants, mitochondrial dysfunction, and metabolic syndrome. Ann. N. Y. Acad. Sci. 2010, 1201, 166–176. [Google Scholar] [CrossRef]
- Foulds, C.E.; Trevino, L.S.; York, B.; Walker, C.L. Endocrine-disrupting chemicals and fatty liver disease. Nat. Rev. Endocrinol. 2017, 13, 445–457. [Google Scholar] [CrossRef] [Green Version]
- Lu, C.; Wang, Y.; Sheng, Z.; Liu, G.; Fu, Z.; Zhao, J.; Zhao, J.; Yan, X.; Zhu, B.; Peng, S. NMR-based metabonomic analysis of the hepatotoxicity induced by combined exposure to PCBs and TCDD in rats. Toxicol. Appl. Pharmacol. 2010, 248, 178–184. [Google Scholar] [CrossRef] [PubMed]
- Wormuth, M.; Scheringer, M.; Vollenweider, M.; Hungerbuhler, K. What are the sources of exposure to eight frequently used phthalic acid esters in Europeans? Risk Anal. 2006, 26, 803–824. [Google Scholar] [CrossRef]
- Calafat, A.M.; Ye, X.; Silva, M.J.; Kuklenyik, Z.; Needham, L.L. Human exposure assessment to environmental chemicals using biomonitoring. Int. J. Androl. 2006, 29, 166–171; discussion 181–185. [Google Scholar] [CrossRef] [PubMed]
- Koch, H.M.; Bolt, H.M.; Preuss, R.; Angerer, J. New metabolites of di(2-ethylhexyl)phthalate (DEHP) in human urine and serum after single oral doses of deuterium-labelled DEHP. Arch. Toxicol. 2005, 79, 367–376. [Google Scholar] [CrossRef]
- Silva, M.J.; Barr, D.B.; Reidy, J.A.; Kato, K.; Malek, N.A.; Hodge, C.C.; Hurtz, D., III; Calafat, A.M.; Needham, L.L.; Brock, J.W. Glucuronidation patterns of common urinary and serum monoester phthalate metabolites. Arch. Toxicol. 2003, 77, 561–567. [Google Scholar] [CrossRef]
- Koch, H.M.; Bolt, H.M.; Angerer, J. Di(2-ethylhexyl)phthalate (DEHP) metabolites in human urine and serum after a single oral dose of deuterium-labelled DEHP. Arch. Toxicol. 2004, 78, 123–130. [Google Scholar] [CrossRef] [PubMed]
- Frederiksen, H.; Skakkebaek, N.E.; Andersson, A.M. Metabolism of phthalates in humans. Mol. Nutr. Food Res. 2007, 51, 899–911. [Google Scholar] [CrossRef] [PubMed]
- Culty, M.; Thuillier, R.; Li, W.; Wang, Y.; Martinez-Arguelles, D.B.; Benjamin, C.G.; Triantafilou, K.M.; Zirkin, B.R.; Papadopoulos, V. In utero exposure to di-(2-ethylhexyl) phthalate exerts both short-term and long-lasting suppressive effects on testosterone production in the rat. Biol. Reprod. 2008, 78, 1018–1028. [Google Scholar] [CrossRef] [Green Version]
- Parks, L.G.; Ostby, J.S.; Lambright, C.R.; Abbott, B.D.; Klinefelter, G.R.; Barlow, N.J.; Gray, L.E., Jr. The plasticizer diethylhexyl phthalate induces malformations by decreasing fetal testosterone synthesis during sexual differentiation in the male rat. Toxicol. Sci. 2000, 58, 339–349. [Google Scholar] [CrossRef]
- Hatch, E.E.; Nelson, J.W.; Qureshi, M.M.; Weinberg, J.; Moore, L.L.; Singer, M.; Webster, T.F. Association of urinary phthalate metabolite concentrations with body mass index and waist circumference: A cross-sectional study of NHANES data, 1999–2002. Environ. Health 2008, 7, 27. [Google Scholar] [CrossRef] [Green Version]
- Buser, M.C.; Murray, H.E.; Scinicariello, F. Age and sex differences in childhood and adulthood obesity association with phthalates: Analyses of NHANES 2007-2010. Int. J. Hyg. Environ. Health 2014, 217, 687–694. [Google Scholar] [CrossRef]
- Gayathri, N.S.; Dhanya, C.R.; Indu, A.R.; Kurup, P.A. Changes in some hormones by low doses of di (2-ethyl hexyl) phthalate (DEHP), a commonly used plasticizer in PVC blood storage bags & medical tubing. Indian J. Med. Res. 2004, 119, 139–144. [Google Scholar] [PubMed]
- Stahlhut, R.W.; van Wijngaarden, E.; Dye, T.D.; Cook, S.; Swan, S.H. Concentrations of urinary phthalate metabolites are associated with increased waist circumference and insulin resistance in adult U.S. males. Environ. Health Perspect. 2007, 115, 876–882. [Google Scholar] [CrossRef] [Green Version]
- Gollamudi, R.; Prasanna, H.R.; Rao, R.H.; Lawrence, W.H.; Autian, J. Impaired metabolism of di(2-ethylhexyl) phthalate (DEHP) in old rats—An in vitro study. J. Toxicol. Environ. Health 1983, 12, 623–632. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.J.; Park, M.S.; Lee, E.J.; Hong, Y.P. The Development of Metabolic Derangement in Male Offspring after Perinatal Exposure to Di-(2-Ethylhexyl) Phthalate. Biomed. Environ. Sci. 2018, 31, 531–534. [Google Scholar] [CrossRef]
- Hao, C.; Cheng, X.; Xia, H.; Ma, X. The endocrine disruptor mono-(2-ethylhexyl) phthalate promotes adipocyte differentiation and induces obesity in mice. Biosci. Rep. 2012, 32, 619–629. [Google Scholar] [CrossRef] [Green Version]
- Knight, B.L.; Hebbachi, A.; Hauton, D.; Brown, A.M.; Wiggins, D.; Patel, D.D.; Gibbons, G.F. A role for PPARalpha in the control of SREBP activity and lipid synthesis in the liver. Biochem. J. 2005, 389, 413–421. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, H.; Zhang, W.; Rui, B.B.; Yang, S.M.; Xu, W.P.; Wei, W. Di(2-ethylhexyl) phthalate exacerbates non-alcoholic fatty liver in rats and its potential mechanisms. Environ. Toxicol. Pharmacol. 2016, 42, 38–44. [Google Scholar] [CrossRef]
- Zhang, W.; Shen, X.Y.; Zhang, W.W.; Chen, H.; Xu, W.P.; Wei, W. The effects of di 2-ethyl hexyl phthalate (DEHP) on cellular lipid accumulation in HepG2 cells and its potential mechanisms in the molecular level. Toxicol. Mech. Methods 2017, 27, 245–252. [Google Scholar] [CrossRef]
- Huff, M.; da Silveira, W.A.; Carnevali, O.; Renaud, L.; Hardiman, G. Systems Analysis of the Liver Transcriptome in Adult Male Zebrafish Exposed to the Plasticizer (2-Ethylhexyl) Phthalate (DEHP). Sci. Rep. 2018, 8, 2118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feige, J.N.; Gerber, A.; Casals-Casas, C.; Yang, Q.; Winkler, C.; Bedu, E.; Bueno, M.; Gelman, L.; Auwerx, J.; Gonzalez, F.J.; et al. The pollutant diethylhexyl phthalate regulates hepatic energy metabolism via species-specific PPARalpha-dependent mechanisms. Environ. Health Perspect. 2010, 118, 234–241. [Google Scholar] [CrossRef]
- Bai, J.; He, Z.; Li, Y.; Jiang, X.; Yu, H.; Tan, Q. Mono-2-ethylhexyl phthalate induces the expression of genes involved in fatty acid synthesis in HepG2 cells. Environ. Toxicol. Pharmacol. 2019, 69, 104–111. [Google Scholar] [CrossRef]
- Zhang, Y.; Ge, S.; Yang, Z.; Li, Z.; Gong, X.; Zhang, Q.; Dong, W.; Dong, C. Disturbance of di-(2-ethylhexyl) phthalate in hepatic lipid metabolism in rats fed with high fat diet. Food Chem. Toxicol. 2020, 146, 111848. [Google Scholar] [CrossRef]
- An, S.; Lee, E.; Jeong, S.-H.; Hong, Y.-p.; Ahn, S.; Yang, Y.-J. Perinatal exposure to di-(2-ethylhexyl) phthalate induces hepatic lipid accumulation mediated by diacylglycerol acyltransferase 1. Hum. Exp. Toxicol. 2021, 09603271211003314. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Kim, D.; Kim, H.J.; Lee, C.H.; Yang, J.I.; Kim, W.; Kim, Y.J.; Yoon, J.H.; Cho, S.H.; Sung, M.W.; et al. Hepatic steatosis index: A simple screening tool reflecting nonalcoholic fatty liver disease. Dig. Liver Dis. 2010, 42, 503–508. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.W.; Lee, H.W.; Kim, B.K.; Park, J.Y.; Kim, D.Y.; Ahn, S.H.; Han, K.H.; Kim, S.U. Hepatic Steatosis Index in the Detection of Fatty Liver in Patients with Chronic Hepatitis B Receiving Antiviral Therapy. Gut Liver 2020. [Google Scholar] [CrossRef] [Green Version]
- Kim, D.; Yoo, E.R.; Li, A.A.; Cholankeril, G.; Tighe, S.P.; Kim, W.; Harrison, S.A.; Ahmed, A. Elevated urinary bisphenol A levels are associated with non-alcoholic fatty liver disease among adults in the United States. Liver Int. 2019, 39, 1335–1342. [Google Scholar] [CrossRef] [PubMed]
- Jia, Y.; Liu, T.; Zhou, L.; Zhu, J.; Wu, J.; Sun, D.; Xu, J.; Wang, Q.; Chen, H.; Xu, F.; et al. Effects of Di-(2-ethylhexyl) Phthalate on Lipid Metabolism by the JAK/STAT Pathway in Rats. Int. J. Environ. Res. Public Health 2016, 13, 1085. [Google Scholar] [CrossRef]
- Lv, Z.; Cheng, J.; Huang, S.; Zhang, Y.; Wu, S.; Qiu, Y.; Geng, Y.; Zhang, Q.; Huang, G.; Ma, Q.; et al. DEHP induces obesity and hypothyroidism through both central and peripheral pathways in C3H/He mice. Obesity 2016, 24, 368–378. [Google Scholar] [CrossRef] [Green Version]
- Das, K.; Das, K.; Mukherjee, P.S.; Ghosh, A.; Ghosh, S.; Mridha, A.R.; Dhibar, T.; Bhattacharya, B.; Bhattacharya, D.; Manna, B.; et al. Nonobese population in a developing country has a high prevalence of nonalcoholic fatty liver and significant liver disease. Hepatology 2010, 51, 1593–1602. [Google Scholar] [CrossRef]
- Cho, H.C. Prevalence and Factors Associated with Nonalcoholic Fatty Liver Disease in a Nonobese Korean Population. Gut Liver 2016, 10, 117–125. [Google Scholar] [CrossRef]
- Feldman, A.; Eder, S.K.; Felder, T.K.; Kedenko, L.; Paulweber, B.; Stadlmayr, A.; Huber-Schonauer, U.; Niederseer, D.; Stickel, F.; Auer, S.; et al. Clinical and Metabolic Characterization of Lean Caucasian Subjects With Non-alcoholic Fatty Liver. Am. J. Gastroenterol. 2017, 112, 102–110. [Google Scholar] [CrossRef]
- Kim, S.H.; On, J.W.; Pyo, H.; Ko, K.S.; Won, J.C.; Yang, J.; Park, M.J. Percentage fractions of urinary di(2-ethylhexyl) phthalate metabolites: Association with obesity and insulin resistance in Korean girls. PLoS ONE 2018, 13, e0208081. [Google Scholar] [CrossRef]
- Rengarajan, S.; Parthasarathy, C.; Anitha, M.; Balasubramanian, K. Diethylhexyl phthalate impairs insulin binding and glucose oxidation in Chang liver cells. Toxicol. Vitro 2007, 21, 99–102. [Google Scholar] [CrossRef]
- Sinha, R.A.; Singh, B.K.; Yen, P.M. Direct effects of thyroid hormones on hepatic lipid metabolism. Nat. Rev. Endocrinol. 2018, 14, 259–269. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Zhao, L.; Wei, L.; Li, L. DEHP reduces thyroid hormones via interacting with hormone synthesis-related proteins, deiodinases, transthyretin, receptors, and hepatic enzymes in rats. Environ. Sci. Pollut. Res. Int. 2015, 22, 12711–12719. [Google Scholar] [CrossRef] [PubMed]
- Meeker, J.D.; Calafat, A.M.; Hauser, R. Di(2-ethylhexyl) phthalate metabolites may alter thyroid hormone levels in men. Environ. Health Perspect. 2007, 115, 1029–1034. [Google Scholar] [CrossRef]
- Mantovani, A.; Nascimbeni, F.; Lonardo, A.; Zoppini, G.; Bonora, E.; Mantzoros, C.S.; Targher, G. Association Between Primary Hypothyroidism and Nonalcoholic Fatty Liver Disease: A Systematic Review and Meta-Analysis. Thyroid 2018, 28, 1270–1284. [Google Scholar] [CrossRef] [PubMed]
- Fedchuk, L.; Nascimbeni, F.; Pais, R.; Charlotte, F.; Housset, C.; Ratziu, V.; Group, L.S. Performance and limitations of steatosis biomarkers in patients with nonalcoholic fatty liver disease. Aliment. Pharmacol. Ther. 2014, 40, 1209–1222. [Google Scholar] [CrossRef]
- Kang, Y.; Park, J.; Youn, K. Association between urinary phthalate metabolites and obesity in adult Korean population: Korean National Environmental Health Survey (KoNEHS), 2012–2014. Ann. Occup Environ. Med. 2019, 31, e23. [Google Scholar] [CrossRef]

{kind=link}
| Variables | Non-NAFLD (n = 4405) | NAFLD (n = 1395) | p-Value |
|---|---|---|---|
| Age (years) | 45.79 ± 0.41 | 47.70 ± 0.62 | 0.005 |
| Gender (%, men) | 46.68 ± 0.79 | 50.50 ± 1.75 | 0.061 |
| BMI (kg/m2) | 22.81 ± 0.05 | 28.20 ± 0.10 | <0.001 |
| Drinking Status (%) | 0.054 | ||
| Never | 29.90 ± 0.91 | 34.01 ± 1.69 | |
| Former | 4.97 ± 0.40 | 3.98 ± 0.62 | |
| Current | 65.12 ± 1.00 | 61.99 ± 1.79 | |
| Smoking Status (%) | 0.013 | ||
| Never | 65.75 ± 0.89 | 61.59 ± 1.78 | |
| Former | 15.23 ± 0.65 | 14.29 ± 1.26 | |
| Current | 19.00 ± 0.80 | 24.10 ± 1.69 | |
| Physical activity (%) | 0.013 | ||
| No | 61.43 ± 0.12 | 66.64 ± 1.76 | |
| Moderate | 22.06 ± 1.03 | 19.36 ± 1.49 | |
| Vigorous | 16.50 ± 0.82 | 13.99 ± 1.15 | |
| Socioeconomic status (%) | 0.040 | ||
| Low | 0.83 ± 0.20 | 1.09 ± 0.39 | |
| Low-mid | 29.17 ± 1.32 | 26.92 ± 2.00 | |
| Mid-high | 47.97 ± 1.22 | 45.01 ± 1.95 | |
| High | 22.02 ± 1.04 | 26.96 ± 1.91 | |
| Education (%) | <0.001 | ||
| <High school | 22.99 ± 0.98 | 28.42 ± 1.67 | |
| High school | 38.49 ± 1.08 | 38.80 ± 1.83 | |
| College and more | 38.51 ± 1.23 | 32.76 ± 1.93 | |
| Marital status (%) | <0.001 | ||
| Single | 19.67 ± 1.05 | 14.41 ± 1.51 | |
| Married | 72.83 ± 1.10 | 74.93 ± 1.75 | |
| Divorced | 7.48 ± 0.52 | 1.06 ± 1.21 | |
| Comorbidity (%) | |||
| Hypertension | 12.67 ± 0.63 | 24.38 ± 1.54 | <0.001 |
| Diabetes mellitus | 3.82 ± 0.33 | 15.32 ± 1.19 | <0.001 |
| Hyperlipidemia | 25.01 ± 0.90 | 48.99 ± 1.79 | <0.001 |
| Concentrations (ug/L, GM ± GSE) | Total (n = 5800) | Non-NAFLD (n = 4405) | NAFLD (n = 1395) | p-Value |
|---|---|---|---|---|
| MEHHP | 2.922 ± 0.011 | 2.898 ± 0.013 | 3.000 ± 0.023 | <0.001 |
| MEOHP | 2.571 ± 0.011 | 2.558 ± 0.013 | 2.612 ± 0.023 | 0.031 |
| MECPP | 3.059 ± 0.010 | 3.039 ± 0.012 | 3.120 ± 0.021 | <0.001 |
| MnBP | 3.211 ± 0.012 | 3.212 ± 0.014 | 3.208 ± 0.024 | 1.000 |
| MBzP | 1.047 ± 0.015 | 1.033 ± 0.017 | 1.091 ± 0.031 | 0.085 |
| Phthalate Metabolites | Crude | Model 1 | Model 2 | Model 3 | ||||
|---|---|---|---|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| MEHHP | ||||||||
| Quartile 1 | 1 | <0.001 * | 1 | 0.008 * | 1 | 0.015 * | 1 | 0.019 * |
| Quartile 2 | 1.09 (0.85–1.40) | 0.482 | 1.09 (0.83–1.44) | 0.514 | 1.07 (0.81–1.42) | 0.594 | 1.05 (0.80–1.38) | 0.702 |
| Quartile 3 | 1.39 (1.14–1.71) | 0.001 | 1.40 (1.08–1.81) | 0.010 | 1.34 (1.02–1.76) | 0.030 | 1.33 (1.00–1.78) | 0.044 |
| Quartile 4 | 1.41 (1.12–1.77) | 0.003 | 1.43 (1.04–1.95) | 0.024 | 1.40 (1.02–1.93) | 0.035 | 1.39 (1.00–1.92) | 0.044 |
| MEOHP | ||||||||
| Quartile 1 | 1 | 0.069 * | 1 | 0.657 * | 1 | 0.784 * | 1 | 0.835 * |
| Quartile 2 | 1.10 (0.86–1.40) | 0.445 | 1.04 (0.80–1.35) | 0.751 | 1.03 (0.79–1.34) | 0.784 | 1.01 (0.77–1.31) | 0.929 |
| Quartile 3 | 1.12 (0.98–1.51) | 0.067 | 1.10 (0.83–1.46) | 0.480 | 1.07 (0.80–1.44) | 0.618 | 1.05 (0.77–1.43) | 0.732 |
| Quartile 4 | 1.19 (0.96–1.49) | 0.109 | 1.05 (0.78–1.42) | 0.723 | 1.03 (0.76–1.40) | 0.827 | 1.02 (0.74–1.39) | 0.888 |
| MECPP | ||||||||
| Quartile 1 | 1 | 0.020 * | 1 | 0.214 * | 1 | 0.267 * | 1 | 0.245 * |
| Quartile 2 | 1.07 (0.85–1.36) | 0.531 | 1.04 (0.80–1.35) | 0.729 | 1.03 (0.80–1.34) | 0.773 | 1.01 (0.77–1.31) | 0.935 |
| Quartile 3 | 1.28 (1.04–1.59) | 0.020 | 1.20 (0.91–1.58) | 0.179 | 1.17 (0.88–1.55) | 0.270 | 1.14 (0.85–1.54) | 0.365 |
| Quartile 4 | 1.26 (1.00–1.60) | 0.047 | 1.18 (0.86–1.62) | 0.287 | 1.17 (0.84–1.61) | 0.337 | 1.18 (0.85–1.65) | 0.311 |
| MBzP | ||||||||
| Quartile 1 | 1 | 0.533 * | 1 | 0.664 * | 1 | 0.710 * | 1 | 0.792 * |
| Quartile 2 | 1.08 (0.86–1.37) | 0.467 | 1.02 (0.80–1.30) | 0.853 | 1.07 (0.84–1.36) | 0.573 | 1.05 (0.82–1.34) | 0.673 |
| Quartile 3 | 1.14 (0.92–1.42) | 0.220 | 1.03 (0.80–1.32) | 0.711 | 1.08 (0.84–1.38) | 0.529 | 1.06 (0.82–1.35) | 0.641 |
| Quartile 4 | 1.06 (0.84–1.34) | 0.612 | 0.93 (0.70–1.23) | 0.626 | 0.94 (0.71–1.24) | 0.678 | 0.95 (0.72–1.26) | 0.769 |
| MnBP | ||||||||
| Quartile 1 | 1 | 0.860 * | 1 | 0.191 * | 1 | 0.304 * | 1 | 0.420 * |
| Quartile 2 | 1.17 (0.95–1.44) | 0.139 | 1.05 (0.83–1.34) | 0.630 | 1.08 (0.85–1.38) | 0.492 | 1.07 (0.83–1.37) | 0.571 |
| Quartile 3 | 1.08 (0.86–1.34) | 0.481 | 0.90 (0.68–1.18) | 0.449 | 0.93 (0.71–1.22) | 0.632 | 0.94 (0.72–1.23) | 0.685 |
| Quartile 4 | 1.05 (0.82–1.33) | 0.686 | 0.83 (0.60–1.15) | 0.279 | 0.87 (0.63–1.21) | 0.424 | 0.90 (0.64–1.25) | 0.540 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, Y.-J.; Kim, T.; Hong, Y.-P. Urinary Phthalate Levels Associated with the Risk of Nonalcoholic Fatty Liver Disease in Adults: The Korean National Environmental Health Survey (KoNEHS) 2012–2014. Int. J. Environ. Res. Public Health 2021, 18, 6035. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18116035
Yang Y-J, Kim T, Hong Y-P. Urinary Phthalate Levels Associated with the Risk of Nonalcoholic Fatty Liver Disease in Adults: The Korean National Environmental Health Survey (KoNEHS) 2012–2014. International Journal of Environmental Research and Public Health. 2021; 18(11):6035. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18116035
Chicago/Turabian StyleYang, Yun-Jung, Taehyen Kim, and Yeon-Pyo Hong. 2021. "Urinary Phthalate Levels Associated with the Risk of Nonalcoholic Fatty Liver Disease in Adults: The Korean National Environmental Health Survey (KoNEHS) 2012–2014" International Journal of Environmental Research and Public Health 18, no. 11: 6035. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18116035