
Diarrhoea among Children Aged under Five Years and Risk Factors in Informal Settlements: A Cross-Sectional Study in Cape Town, South Africa

 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics Statement
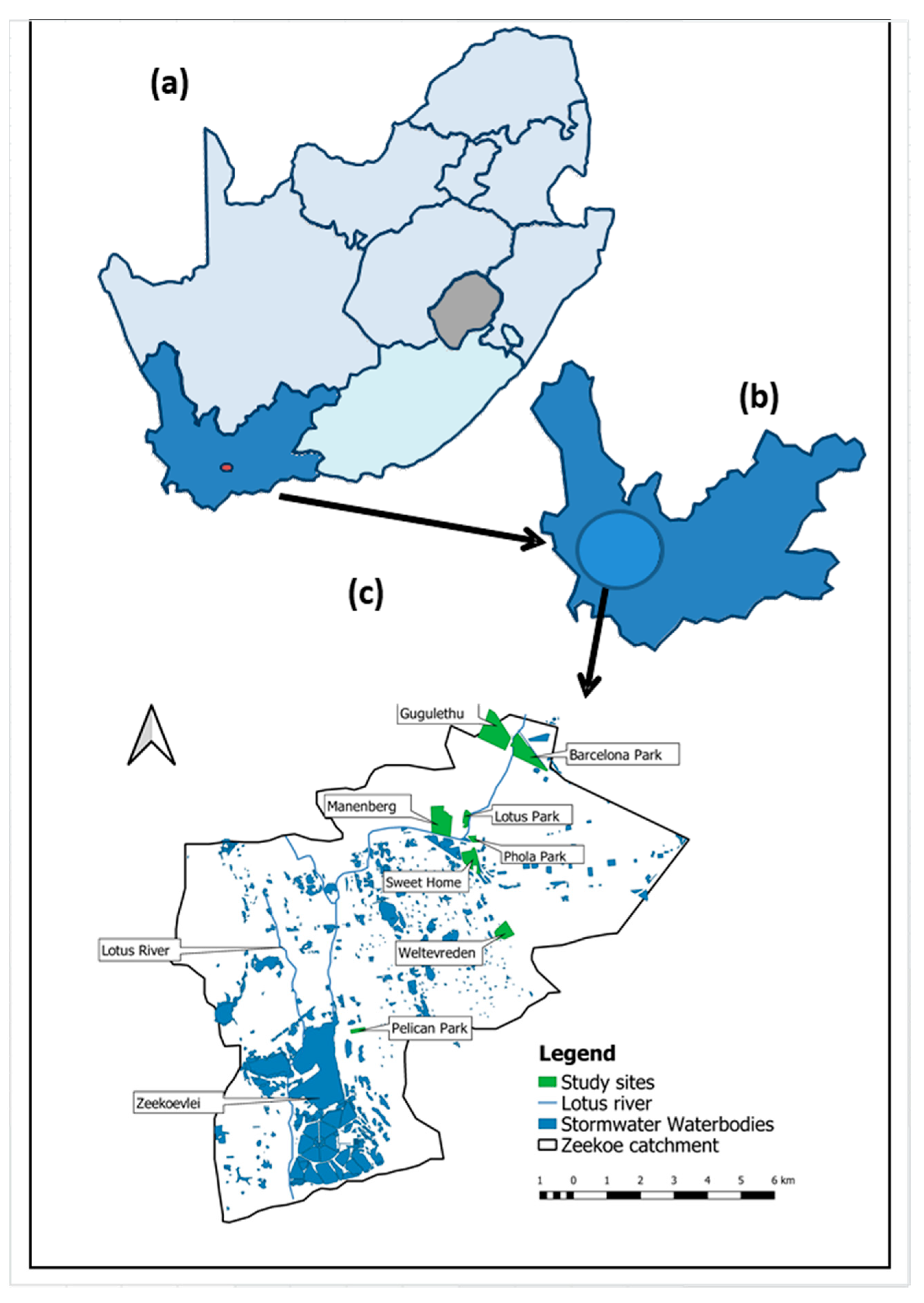
2.2. Study Location
2.3. Selection of Settlements and Study Population
2.4. Study Population
2.5. Data Collection
2.6. Statistical Analyses
3. Results
3.1. Characteristics of Studied Households
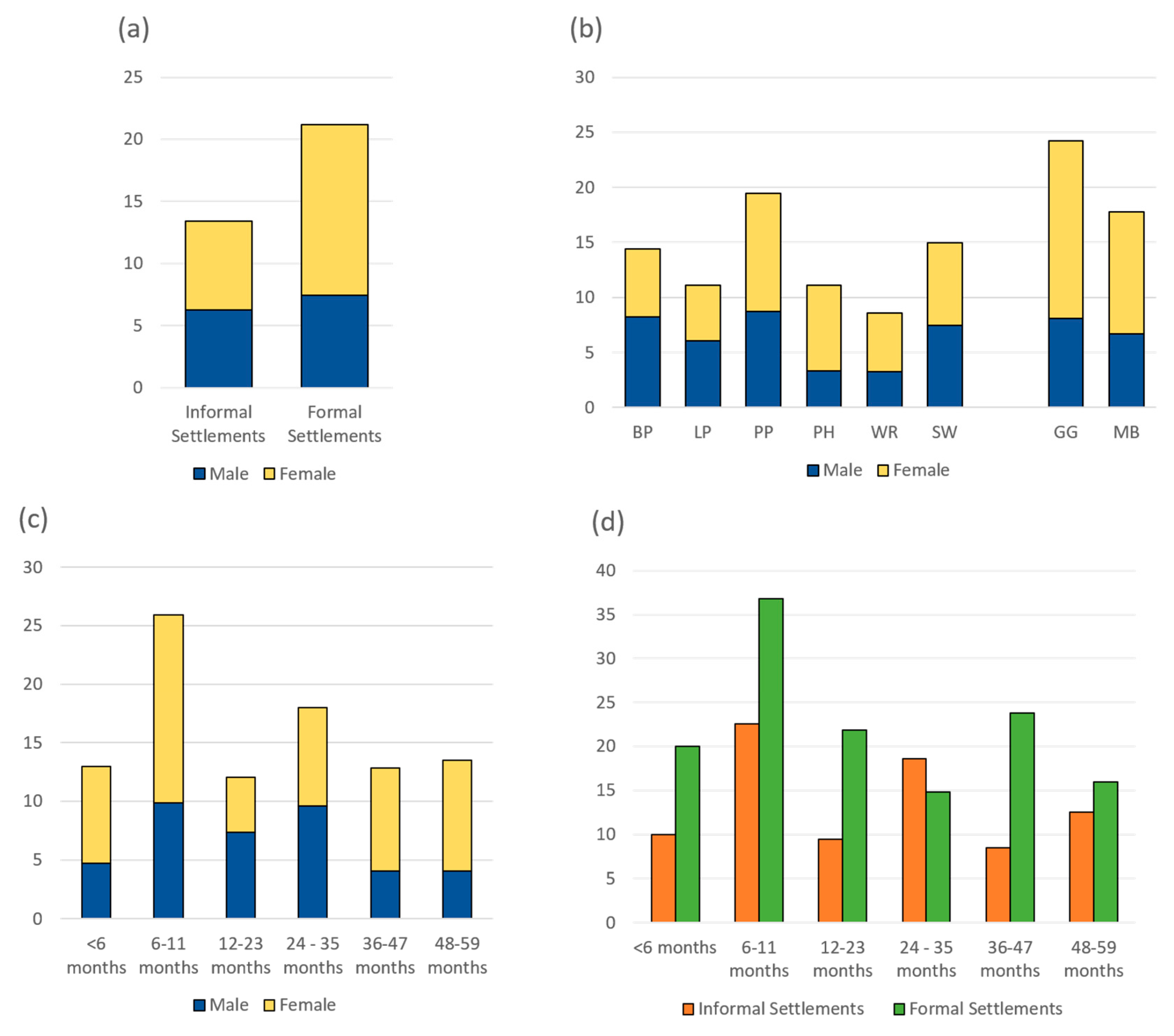
3.1.1. Demographic and Socio-Economic
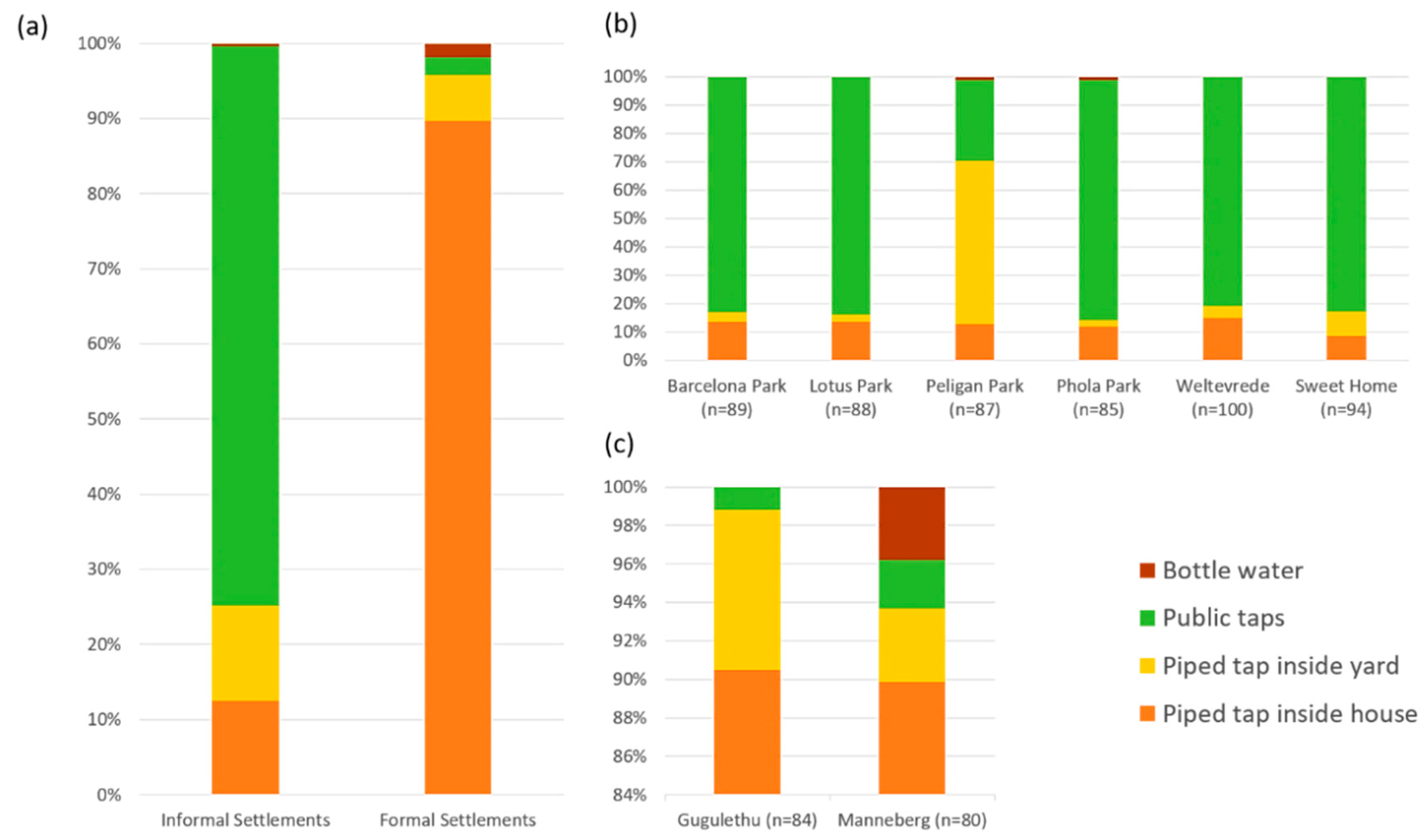
3.1.2. Water Access and Resources
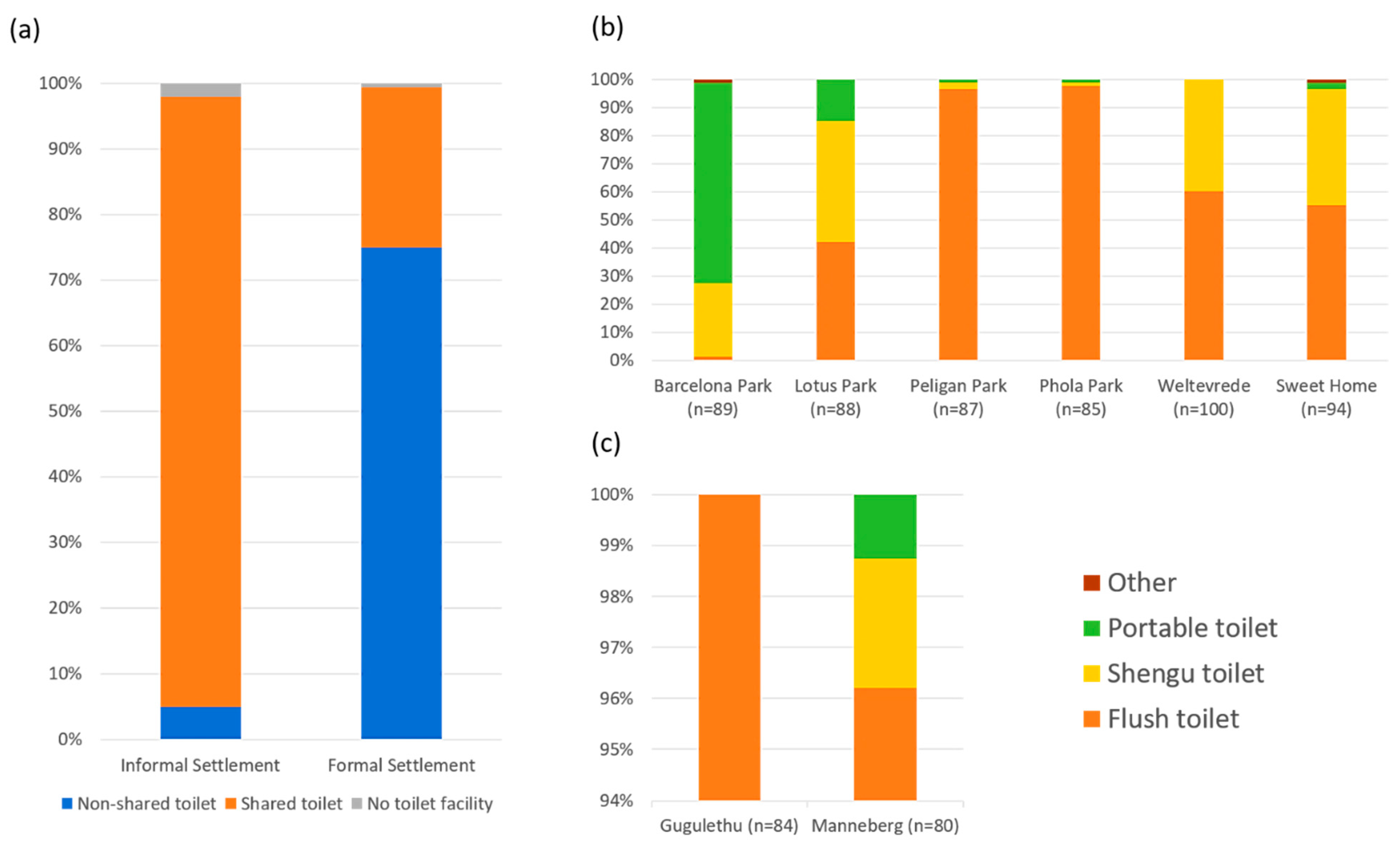
3.1.3. Sanitation
3.1.4. Hygiene
3.1.5. Health-Related Indicators of Children
3.2. Distribution of Diarrhoea Cases
3.3. Risk Factors Associated with Diarrhoea Using Multi-Level Multivariate Analysis
4. Discussions
4.1. Child-Health Related Factors
4.2. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Troeger, C.; Blacker, B.F.; Khalil, I.A.; Rao, P.C.; Cao, S.; Zimsen, S.R.; Albertson, S.B.; Stanaway, J.D.; Deshpande, A.; Abebe, Z.; et al. Estimates of the global, regional, and national morbidity, mortality, and aetiologies of diarrhoea in 195 countries: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Infect. Dis. 2018, 18, 1211–1228. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. GHO by Category Number of Deaths (Thousands)—Data by WHO Region. Available online: https://apps.who.int/gho/data/view.main.CM1300N?lang=en (accessed on 22 February 2021).
- Lehohla, P.; Statistics South Africa. Levels and Trends of Morbidity and Mortality among Children Aged Under-Five Years in South Africa, 2006–2010; Statistics South Africa: Pretoria, South Africa, 2012.
- City of Cape Town. Diarrhoea Statistics Prove Interventions Are Working. Available online: https://www.capetown.gov.za/Media-and-news/Diarrhoea%20statistics%20prove%20interventions%20are%20working (accessed on 22 February 2021).
- Walker, C.L.F.; Black, R.E. Diarrhoea morbidity and mortality in older children, adolescents, and adults. Epidemiol. Infect. 2010, 138, 1215–1226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reiner, R.C.; Graetz, N.; Casey, D.C.; Troeger, C.; Garcia, G.M.; Mosser, J.; Deshpande, A.; Swartz, S.J.; Ray, S.E.; Blacker, B.F.; et al. Variation in Childhood Diarrheal Morbidity and Mortality in Africa, 2000–2015. N. Engl. J. Med. 2018, 379, 1128–1138. [Google Scholar] [CrossRef]
- Thiam, S.; Diène, A.N.; Fuhrimann, S.; Winkler, M.S.; Sy, I.; Ndione, J.A.; Schindler, C.; Vounatsou, P.; Utzinger, J.; Faye, O.; et al. Prevalence of diarrhoea and risk factors among children under five years old in Mbour, Senegal: A cross-sectional study. Infect. Dis. Poverty 2017, 6, 109. [Google Scholar] [CrossRef] [Green Version]
- Prüss-Üstün, A.; Wolf, J.; Corvalán, C.; Bos, R.; Neira, M. Preventing Disease through Healthy Environments: A Global Assessment of the Burden of Disease from Environmental Risks, 2nd ed.; World Health Organization: Geneva, Switzerland, 2016; p. 147. [Google Scholar]
- World Health Organization. Inheriting a Sustainable World: Atlas on Children’s Health and the Environment [Internet]. Available online: http://www.who.int/ceh/publications/inheriting-a-sustainable-world/en/ (accessed on 26 February 2021).
- UN-Habitat. World Cities Report 2016. Urbanization and Development: Emerging Futures [Internet]. Available online: https://wcr.unhabitat.org/wp-content/uploads/sites/16/2016/05/WCR-%20Full-Report-2016.pdf (accessed on 26 February 2021).
- Smit, W. The challenge of COVID-19 in African cities: An urgent call for informal settlement upgrading. Cities Health 2020, 1–3. [Google Scholar] [CrossRef]
- Gibson, L.; Rush, D. Novel Coronavirus in Cape Town Informal Settlements: Feasibility of Using Informal Dwelling Outlines to Identify High Risk Areas for COVID-19 Transmission from A Social Distancing Perspective. JMIR Public Health Surveill. 2020, 6, e18844. [Google Scholar] [CrossRef]
- OECD, Sahel and West Africa Club. Africa’s Urbanisation Dynamics 2020: Africapolis, Mapping a New Urban Geography [Internet]. 2020. (West African Studies). Available online: https://0-www-oecd--ilibrary-org.brum.beds.ac.uk/development/africa-s-urbanisation-dynamics-2020_b6bccb81-en (accessed on 26 February 2021).
- Kellerman, A. Globalization and Spatial Mobilities: Commodities and People, Capital, Information and Technology; Edward Elgar Pubishing: Cheltenham, UK; Northampton, MA, USA, 2020; p. 198. [Google Scholar]
- City of Cape Town. Diarrhoea Trends Suggest that More Hard Work is Required [Internet]. Available online: https://www.capetown.gov.za/media-and-news/Diarrhoea%20trends%20suggest%20that%20more%20hard%20work%20is%20required (accessed on 16 February 2021).
- Nesre, R. Water Quality and Diarrhoeal Diseases in Children in the Lotus River Catchment Area in Cape Town, South Africa; University of Basel: Basel, Switzerland, 2017. [Google Scholar]
- Chola, L.; Michalow, J.; Tugendhaft, A.; Hofman, K. Reducing diarrhoea deaths in South Africa: Costs and effects of scaling up essential interventions to prevent and treat diarrhoea in under-five children. BMC Public Health 2015, 15, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Dorrington, R.; Bradshaw, D.; Laubscher, R.; Nannan, N. Rapid Mortality Surveillance Report 2016; South African Medical Research Council: Cape Town, South Africa, 2018. [Google Scholar]
- Grobicki, A.M. Urban catchment management in a developing country: The Lotus River project, Cape Town, South Africa. Water Sci. Technol. 2001, 44, 313–319. [Google Scholar] [CrossRef]
- Sommet, N.; Morselli, D. Keep Calm and Learn Multilevel Logistic Modeling: A Simplified Three-Step Procedure Using Stata, R, Mplus, and SPSS. Int. Rev. Soc. Psychol. 2017, 30, 203–218. [Google Scholar] [CrossRef] [Green Version]
- Hashizume, M.; Armstrong, B.; Hajat, S.; Wagatsuma, Y.; Faruque, A.S.G.; Hayashi, T.; Sack, D.A. Association between climate variability and hospital visits for non-cholera diarrhoea in Bangladesh: Effects and vulnerable groups. Int. J. Epidemiol. 2007, 36, 1030–1037. [Google Scholar] [CrossRef] [PubMed]
- Azage, M.; Kumie, A.; Worku, A.; Bagtzoglou, A.; Anagnostou, E. Effect of climatic variability on childhood diarrhea and its high risk periods in northwestern parts of Ethiopia. PLoS ONE 2017, 12, e0186933. [Google Scholar] [CrossRef] [Green Version]
- Wu, J.; Yunus, M.; Streatfield, P.K.; Emch, M. Association of climate variability and childhood diarrhoeal disease in rural Bangladesh, 2000–2006. Epidemiol. Infect. 2013, 142, 1859–1868. [Google Scholar] [CrossRef] [PubMed]
- Musengimana, G.; Mukinda, F.K.; Machekano, R.; Mahomed, H. Temperature Variability and Occurrence of Diarrhoea in Children under Five-Years-Old in Cape Town Metropolitan Sub-Districts. Int. J. Environ. Res. Public Health 2016, 13, 859. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pmc/articles/PMC5036692 (accessed on 26 February 2021). [CrossRef] [PubMed]
- Azage, M.; Kumie, A.; Worku, A.; Bagtzoglou, A.C. Childhood diarrhea in high and low hotspot districts of Amhara Region, northwest Ethiopia: A multilevel modeling. J. Health Popul. Nutr. 2016, 35, 13. [Google Scholar] [CrossRef] [Green Version]
- Alexander, K.A.; Carzolio, M.; Goodin, D.; Vance, E. Climate Change is Likely to Worsen the Public Health Threat of Diarrheal Disease in Botswana. Int. J. Environ. Res. Public Health 2013, 10, 1202–1230. [Google Scholar] [CrossRef]
- Aguilar-León, P.; Solano-Zapata, F. Heatwaves and health: Reflections on the El Niño phenomenon in Piura, Peru. Cadernos de Saúde Pública 2016, 32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thompson, A.A.; Matamale, L.; Kharidza, S.D. Impact of Climate Change on Children’s Health in Limpopo Province, South Africa. Int. J. Environ. Res. Public Health 2012, 9, 831–854. [Google Scholar] [CrossRef] [PubMed]
- Kapwata, T.; Mathee, A.; Le Roux, W.J.; Wright, C.Y. Diarrhoeal Disease in Relation to Possible Household Risk Factors in South African Villages. Int. J. Environ. Res. Public Health 2018, 15, 1665. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pmc/articles/PMC6121382/ (accessed on 26 February 2021). [CrossRef] [Green Version]
- UNICEF. Progress for Children: A Report Card on Water and Sanitation; UNICEF: New York, NY, USA, 2006.
- World Health Organization. Preventing Diarrhoea through Better Water, Sanitaiton and Hygiene Exposures and Impacts in Low- and Middle-Income Countries. [Internet]; World Health Organization: Geneva, Switzerland, 2014; Available online: https://0-ebookcentral-proquest-com.brum.beds.ac.uk/lib/uvic/detail.action?docID=1975014 (accessed on 26 February 2021).
- Schilling, K.A.; Omore, R.; Derado, G.; Ayers, T.; Ochieng, J.B.; Farag, T.H.; Nasrin, D.; Panchalingam, S.; Nataro, J.P.; Kotloff, K.L.; et al. Factors Associated with the Duration of Moderate-to-Severe Diarrhea among Children in Rural Western Kenya Enrolled in the Global Enteric Multicenter Study, 2008–2012. Am. J. Trop. Med. Hyg. 2017, 97, 248–258. [Google Scholar] [CrossRef]
- Nygren, B.L.; O’Reilly, C.E.; Rajasingham, A.; Omore, R.; Ombok, M.; Awuor, A.O.; Jaron, P.; Moke, F.; Vulule, J.; Laserson, K.; et al. The Relationship between Distance to Water Source and Moderate-to-Severe Diarrhea in the Global Enterics Multi-Center Study in Kenya, 2008–2011. Am. J. Trop. Med. Hyg. 2016, 94, 1143–1149. [Google Scholar] [CrossRef]
- Baker, K.K.; Sow, S.O.; Kotloff, K.L.; Nataro, J.P.; Farag, T.H.; Tamboura, B.; Doumbia, M.; Sanogo, D.; Diarra, D.; O’Reilly, C.E.; et al. Quality of piped and stored water in households with children under five years of age enrolled in the Mali site of the Global Enteric Multi-Center Study (GEMS). Am. J. Trop. Med. Hyg. 2013, 89, 214–222. [Google Scholar] [CrossRef] [PubMed]
- Alegbeleye, O.O.; Sant’Ana, A.S. Manure-borne pathogens as an important source of water contamination: An update on the dynamics of pathogen survival/transport as well as practical risk mitigation strategies. Int. J. Hyg. Environ. Health 2020, 227, 113524. [Google Scholar] [CrossRef] [PubMed]
- Troeger, C.; Forouzanfar, M.; Rao, P.C.; Khalil, I.; Brown, A.; Reiner, R.C.; Fullman, N.; Thompson, R.L.; Abajobir, A.; Ahmed, M.; et al. Estimates of global, regional, and national morbidity, mortality, and aetiologies of diarrhoeal diseases: A systematic analysis for the Global Burden of Disease Study 2015. Lancet Infect. Dis. 2017, 17, 909–948. [Google Scholar] [CrossRef] [Green Version]
- Rheingans, R.; Kukla, M.; Adegbola, R.A.; Saha, D.; Omore, R.; Breiman, R.F.; Sow, S.O.; Onwuchekwa, U.; Nasrin, D.; Farag, T.H.; et al. Exploring Household Economic Impacts of Childhood Diarrheal Illnesses in 3 African Settings. Clin. Infect. Dis. 2012, 55, S317–S326. [Google Scholar] [CrossRef] [Green Version]
- Govender, T.; Barnes, J.M.; Pieper, C.H. Contribution of Water Pollution from Inadequate Sanitation and Housing Quality to Diarrheal Disease in Low-Cost Housing Settlements of Cape Town, South Africa. Am. J. Public Health 2011, 101, e4–e9. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization; UNICEF. Progress on Drinking Water, Sanitation and Hygiene: 2017 Update and SDG Baselines; World Health Organization: Geneva, Switzerland; UNICEF: New York, NY, USA, 2017.
- Baker, K.K.; O’Reilly, C.E.; Levine, M.M.; Kotloff, K.L.; Nataro, J.P.; Ayers, T.L.; Farag, T.H.; Nasrin, D.; Blackwelder, W.C.; Wu, Y.; et al. Sanitation and Hygiene-Specific Risk Factors for Moderate-to-Severe Diarrhea in Young Children in the Global Enteric Multicenter Study, 2007–2011: Case-Control Study. PLoS Med. 2016, 13, e1002010. [Google Scholar] [CrossRef]
- Kwiringira, J.; Atekyereza, P.; Niwagaba, C.; Günther, I. Descending the sanitation ladder in urban Uganda: Evidence from Kampala Slums. BMC Public Health 2014, 14, 624. [Google Scholar] [CrossRef] [Green Version]
- Nelson, K.B.; Karver, J.; Kullman, C.; Graham, J.P. User Perceptions of Shared Sanitation among Rural Households in Indonesia and Bangladesh. PLoS ONE 2014, 9, e103886. [Google Scholar] [CrossRef]
- Simiyu, S.; Swilling, M.; Cairncross, S.; Rheingans, R. Determinants of quality of shared sanitation facilities in informal settlements: Case study of Kisumu, Kenya. BMC Public Health 2017, 17, 68. [Google Scholar] [CrossRef] [Green Version]
- Bain, R.; Cronk, R.; Hossain, R.; Bonjour, S.; Onda, K.; Wright, J.; Yang, H.; Slaymaker, T.; Hunter, P.; Prüss--Ustün, A.; et al. Global assessment of exposure to faecal contamination through drinking water based on a systematic review. Trop. Med. Int. Health 2014, 19, 917–927. [Google Scholar] [CrossRef] [Green Version]
- Bain, R.; Cronk, R.; Wright, J.; Yang, H.; Slaymaker, T.; Bartram, J. Fecal Contamination of Drinking-Water in Low- and Middle-Income Countries: A Systematic Review and Meta-Analysis. PLoS Med. 2014, 11, e1001644. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pmc/articles/PMC4011876 (accessed on 26 February 2021). [CrossRef] [Green Version]
- U.S. Environmental Protection Agency (US EPA). Health Effects Support Document for Perfluorooctanoic Acid (PFOA); US EPA: Washington, DC, USA, 2016; p. 322.
- Sá, I.; Semedo, M.; Cunha, M.E. Kidney Cancer. Heavy Metals as a Risk Factor. Porto Biomed. J. 2016, 1, 25–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, G.; Ye, S.; Yuan, H.; Ding, X.; Wang, J. Surface sediment properties and heavy metal pollution assessment in the Pearl River Estuary, China. Environ. Sci. Pollut. Res. 2017, 24, 2966–2979. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karri, V.; Schuhmacher, M.; Kumar, V. Heavy metals (Pb, Cd, As and MeHg) as risk factors for cognitive dysfunction: A general review of metal mixture mechanism in brain. Environ. Toxicol. Pharmacol. 2016, 48, 203–213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mazumder, D.N.G. Arsenic and non-malignant lung disease. J. Environ. Sci. Health Part A 2007, 42, 1859–1867. [Google Scholar] [CrossRef]
- Von Ehrenstein, O.S.; Guha Mazumder, D.N.; Hira-Smith, M.; Ghosh, N.; Yuan, Y.; Windham, G.; Ghosh, A.; Haque, R.; Lahiri, S.; Kalman, D.; et al. Pregnancy outcomes, infant mortality, and arsenic in drinking water in West Bengal, India. Am. J. Epidemiol. 2006, 163, 662–669. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sites | Overall (N = 778) | Informal Settlements (IS) | Formal Settlements (FS) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Overall IS (n = 589) | Barcelona (n = 97) | Lotus Park (n = 99) | Pelican Park (n = 103) | Phola Park (n = 90) | Weltevrede (n = 93) | Sweet Home (n = 107) | Overall FS (n = 189) | Gugulethu (n = 99) | Manenberg (n = 90) | ||
| Gender | |||||||||||
| Male | 374 (48.1%) | 295 (50.1%) | 54 (55.7%) | 54 (54.6%) | 50 (48.5%) | 41 (45.6%) | 47 (50.5%) | 49 (45.8%) | 79 (41.8%) | 40 (40.4%) | 39 (43.3%) |
| Female | 404 (51.9%) | 294 (49.9%) | 43 (44.3%) | 45 (45.4%) | 53 (51.5%) | 49 (54.4%) | 46 (49.5%) | 58 (54.2%) | 110 (58.2%) | 59 (59.6%) | 51 (56.7%) |
| Age group (6 months intervals) | |||||||||||
| <6 | 85 (10.9%) | 60 (10.2%) | 6 (6.2%) | 7 (7.1%) | 10 (9.7%) | 5 (5.6%) | 18 (19.4%) | 14 (13.1%) | 25 (13.2%) | 15 (15.2%) | 10 (11.1%) |
| 6–11 | 81 (10.4%) | 62 (10.5%) | 9 (9.3%) | 8 (8.1%) | 14 (13.6%) | 6 (6.7%) | 9 (9.7%) | 16 (15%) | 19 (10.1%) | 13 (13.1%) | 6 (6.7%) |
| 12–23 | 149 (19.2%) | 117 (19.8%) | 12 (12.4%) | 25 (25.3%) | 18 (17.5%) | 23 (25.6%) | 17 (18.3%) | 22 (20.6%) | 32 (16.9%) | 17 (17.2%) | 15 (16.7%) |
| 24–35 | 167 (21.5%) | 140 (23.8%) | 23 (23.7%) | 26 (26.3%) | 32 (31.1%) | 22 (24.4%) | 16 (17.2%) | 21 (19.6%) | 27 (14.3%) | 12 (12.1%) | 15 (16.7%) |
| 36–47 | 148 (19%) | 106 (18%) | 26 (26.8%) | 17 (17.2%) | 18 (17.5%) | 12 (13.3%) | 18 (19.4%) | 15 (14%) | 42 (22.2%) | 22 (22.2%) | 20 (22.2%) |
| 48–59 | 148 (19%) | 104 (17.7%) | 21 (21.7%) | 16 (16.2%) | 11 (10.7%) | 22 (24.4%) | 15 (16.1%) | 19 (17.8%) | 44 (23.3%) | 20 (20.2%) | 24 (26.7%) |
| Vaccination for child | |||||||||||
| HepA | 329 (42.3%) | 265 (45%) | 37 (38.1%) | 57 (57.6%) | 55 (53.4%) | 45 (50%) | 28 (30.1%) | 43 (40.2%) | 64 (33.9%) | 45 (45.5%) | 19 (21.1%) |
| Hep B | 522 (67.1%) | 378 (64.2%) | 53 (54.6%) | 59 (59.6%) | 93 (90.3%) | 70 (77.8%) | 43 (46.2%) | 60 (56.1%) | 144 (76.2%) | 69 (67.7%) | 75 (83.3%) |
| Rotavirus | 440 (56.6%) | 300 (50.9%) | 59 (60.8%) | 41 (41.4%) | 62 (60.2%) | 54 (60%) | 45 (48.4%) | 39 (36.5%) | 140 (74.1%) | 62 (62.6%) | 78 (86.7%) |
| Breastfeeding in the first 06 months | |||||||||||
| No breastfeeding | 594 (76.4%) | 445 (75.6%) | 77 (79.4%) | 76 (76.8%) | 62 (60.2%) | 76 (84.4%) | 72 (77.4%) | 82 (76.6%) | 149 (78.8%) | 82 (82.8%) | 67 (74.4%) |
| Partial | 88 (11.3%) | 73 (12.4%) | 11 (11.3%) | 13 (13.1%) | 23 (22.3%) | 8 (8.9%) | 8 (8.6%) | 10 (9.4%) | 15 (7.9%) | 9 (9.1%) | 6 (6.7%) |
| Inclusive | 96 (12.3%) | 71 (12.1%) | 9 (9.3%) | 10 (10.1%) | 18 (17.5%) | 6 (6.7%) | 13 (14%) | 15 (14%) | 25 (13.2%) | 8 (8.1%) | 17 (18.9%) |
| Having diarrhea during 07 days prior to the survey | |||||||||||
| Yes | 119 (15.3%) | 79 (15.3%) | 14 (14.4%) | 11 (11.1%) | 20 (19.4%) | 10 (11.1%) | 8 (8.6%) | 16 (15%) | 40 (21.2%) | 24 (24.2%) | 16 (17.8%) |
| Sites | Overall N = 707 | Informal Settlements (IS) | Formal Settlements (FS) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Overall IS (n = 543) | Barcelona (n = 89) | Lotus Park (n = 88) | Pelican Park (n = 87) | Phola Park (n = 85) | Weltevrede (n = 100) | Sweet Home (n = 94) | Overall FS (n = 164) | Gugulethu (n = 84) | Manenberg (n = 80) | ||
| Access to water resources | 99.4% | 99.3% | 97.8% | 100% | 100% | 100% | 98% | 100% | 100% | 100% | 100% |
| Drinking water resources | |||||||||||
| Piped tap inside house | 30.4% | 12.5% | 13.5% | 13.6% | 12.6% | 11.8% | 15% | 8.5% | 89.6% | 89.4% | 89.9% |
| Piped tap inside yard | 11.2% | 12.7% | 3.4% | 2.3% | 57.5% | 2.4% | 4% | 8.5% | 6.1% | 8.3% | 3.8% |
| Public taps | 57.7% | 74.4% | 83.2% | 84.1% | 28.7% | 84.7% | 81% | 83% | 2.4% | 2.4% | 2.5% |
| Use of bottled water | 0.7% | 0.4% | 0 | 0 | 1.2% | 1.2% | 0 | 0 | 1.8% | 0 | 3.8% |
| Distance to water resource | |||||||||||
| Within 500 m | 95.5% | 94.1% | 89.9% | 96.6% | 100% | 100% | 92% | 87.2% | 100% | 100% | 100% |
| >500 m | 4.5% | 5.9% | 10.1% | 3.4% | 0 | 0 | 8% | 12.8% | 0 | 0 | 0 |
| Time spent to fletch water | |||||||||||
| Within 30 min | 99.4% | 99.3% | 97.8% | 100% | 100% | 100% | 98% | 100% | 100% | 100% | 100% |
| >30 min | 0.6% | 0.7% | 2.2% | 0 | 0 | 0 | 2% | 0 | 0 | 0 | 0 |
| Storing water <12 h | 87.8% | 91.3% | 88.8% | 100% | 86.2% | 89.4% | 93% | 90.4% | 76.2% | 87.1% | 64.6% |
| Water cut-off in the last 30 days | 19.4% | 20.1% | 36% | 16% | 6.9% | 5.9% | 42% | 10.6% | 17.1% | 10.6% | 24.1% |
| Treating water before drinking | 46.5% | 42.7% | 28.1% | 53.4% | 57.5% | 36.5% | 50% | 30.9% | 59.2% | 45.9% | 73.2% |
| Type of water-storing container | |||||||||||
| Plastic bucket/bottles | 96.3 | 98.3% | 100% | 98.9% | 98.8% | 97.6% | 97% | 98.9% | 89.6% | 85.7% | 93.8% |
| Other | 3.7% | 1.7% | 0 | 1.1% | 1.2% | 2.4% | 3% | 1.1% | 10.4% | 14.3% | 4.2% |
| Cleaning frequency of water-storing container | |||||||||||
| Daily | 79.5% | 82% | 69.7% | 90.9% | 90.8% | 789.4% | 75% | 77.7% | 71.3% | 77.7% | 64.6% |
| <1 time/day | 120.5% | 18% | 40.3% | 9.1% | 9.2% | 10.6% | 25% | 22.3% | 29.7% | 22.3% | 35.4% |
| Overall (N = 707) | Informal Settlements (IS) | Formal Settlements (FS) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Overall IS (n = 543) | Barcelona (n = 89) | Lotus Park (n = 88) | Pelican Park (n = 87) | Phola Park (n = 85) | Weltevrede (n = 100) | Sweet Home (n = 94) | Overall FS (n = 164) | Gugulethu (n = 84) | Manenberg (n = 80) | ||
| Respondent’s hand-washing practices | |||||||||||
| Before eating | 96.6% | 96.9% | 97.8% | 90.9% | 100% | 100% | 96% | 96.8% | 95.7% | 94.1% | 97.5% |
| After eating | 59.8% | 61.1% | 57.3% | 53.4% | 82.8% | 77.7% | 51% | 47.9% | 55.5% | 63.5% | 46.8% |
| After defecation | 48% | 51.2% | 39.3% | 53.4% | 66.7% | 61.2% | 42% | 46.8% | 37.2% | 50.6% | 22.8% |
| After latrine use | 62% | 62.6% | 58.4% | 59.1% | 83.9% | 72.9% | 50% | 54.3% | 59.8% | 64.7% | 54.4% |
| Before feeding child | 61.7% | 61.9% | 55.1% | 56.8% | 80.5% | 53.2% | 51% | 77.7% | 61% | 63.5% | 58.2% |
| After handling rubbish | 54.5% | 58% | 50.6% | 55.7% | 67.8% | 75.3% | 51% | 50% | 42.7% | 58.8% | 25.3% |
| After handling baby diaper/feces | 48.5% | 52.9% | 41.6% | 50% | 69% | 68.2% | 46% | 44.7% | 34.2% | 52.9% | 13.9% |
| Before food reparation | 60.3% | 58.9% | 49.4% | 59.8% | 87.4% | 64.7% | 48% | 50% | 64.6% | 57.7% | 72.2% |
| After touching animals | 12.5% | 12.5% | 9% | 8% | 23% | 24.7% | 3% | 9.6% | 12.2% | 18.8% | 5% |
| Observed availability of soap | 28% | 28.5% | 31.5% | 51.1% | 24.1% | 15.3% | 15% | 35.1% | 26.2% | 42.1% | 12.5 |
| Hand-washing index (mean) | −2.30 × 10−8 | 0.04 | −0.14 | −0.05 | 0.5 | 0.4 | −0.16 | −0.2 | −0.14 | 0.06 | −0.36 |
| Pest invasion | |||||||||||
| Rat | 77.4% | 86.9% | 92.1% | 94.3% | 61% | 80% | 94% | 97.9% | 45.7% | 72.9% | 16.5% |
| Cockroaches | 70.9% | 71.8% | 78.7% | 83% | 60.9% | 57.7% | 81% | 68.1% | 67.7% | 58.8% | 77.2% |
| Using pesticides during the last 2 weeks | |||||||||||
| Inside house | 47.4% | 44.4% | 53.4% | 26.4% | 50.6% | 41.2% | 54.6% | 39.4% | 57.3% | 37.7% | 78.5% |
| Outside house | 21.6% | 21.7% | 22.5% | 18.2% | 25.3% | 12.9% | 26.3% | 23.9% | 21.3% | 28.3% | 13.9% |
| Waste water disposal | |||||||||||
| To open ground near house | 12.2% | 10.9% | 14.6% | 3.4% | 4.6% | 33.5% | 17% | 20.2% | 16.5% | 2.4% | 31.7% |
| To open ground far away from house | 44.8% | 52.9% | 58.4% | 52.3% | 18.4% | 69.4% | 61% | 56.4% | 18.3% | 31.8% | 3.8% |
| To toilet/ lavabo | 33.7% | 28.4% | 22.5% | 42.1% | 62.1% | 17.7% | 9% | 20.2% | 51.2% | 57.7% | 44.3% |
| To water storm drains | 9.3% | 7.9% | 4.5% | 2.3% | 14.9% | 9.4% | 13% | 3.2% | 14% | 8.2% | 20.3% |
| Risk Factors | OR | 95% CI | p-Value |
|---|---|---|---|
| Caretaker’s education level | 1.59 | 1.06–2.40 | 0.03 |
| Having >2 U5-children | 0.67 | 0.38–1.17 | 0.16 |
| Drinking water sources | |||
| Private piped taps on premises | Ref | - | - |
| Piped taps inside yard | 1.94 | 0.84–4.47 | 0.12 |
| Communal public tap | 0.59 | 0.14–2.54 | 0.48 |
| Storing water >12 h | 1.9 | 1.02–3.79 | 0.05 |
| Using water treatment | 0.57 | 0.34–0.97 | 0.04 |
| Water interruption during 07 days prior the survey | 1.21 | 0.69–2.09 | 0.50 |
| Toilet access and sharing | |||
| Private toilet facility | Ref | - | - |
| Shared with 1–3 households | 0.76 | 0.34–1.64 | 0.49 |
| Shared with ≥4 households | 0.35 | 0.15–0.85 | 0.02 |
| No toilet facility | 0.44 | 0.07–2.77 | 0.39 |
| Reported problems with toilet facility | 1.88 | 1.00–3.55 | 0.05 |
| Feces disposal | 1.18 | 0.75–1.84 | 0.47 |
| Using pesticide inside house during 07 days prior the survey | 0.49 | 0.30–0.84 | 0.01 |
| Hand-washing index | 0.59 | 0.42–0.82 | 0.02 |
| Child’s age (in months) | 0.99 | 0.98–1.01 | 0.23 |
| Child’s gender | |||
| Male | Ref | - | - |
| Female | 1.32 | 0.83–2.09 | 0.23 |
| Duration of breast feeding | 1.11 | 1.00–1.23 | 0.07 |
| Had Hepatitis A vaccine | 0.51 | 0.28–0.9 | 0.02 |
| Had Rotavirus vaccine | 1.62 | 0.86–3.08 | 0.14 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nguyen, T.Y.C.; Fagbayigbo, B.O.; Cissé, G.; Redi, N.; Fuhrimann, S.; Okedi, J.; Schindler, C.; Röösli, M.; Armitage, N.P.; Carden, K.; et al. Diarrhoea among Children Aged under Five Years and Risk Factors in Informal Settlements: A Cross-Sectional Study in Cape Town, South Africa. Int. J. Environ. Res. Public Health 2021, 18, 6043. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18116043
Nguyen TYC, Fagbayigbo BO, Cissé G, Redi N, Fuhrimann S, Okedi J, Schindler C, Röösli M, Armitage NP, Carden K, et al. Diarrhoea among Children Aged under Five Years and Risk Factors in Informal Settlements: A Cross-Sectional Study in Cape Town, South Africa. International Journal of Environmental Research and Public Health. 2021; 18(11):6043. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18116043
Chicago/Turabian StyleNguyen, Thi Yen Chi, Bamidele Oladapo Fagbayigbo, Guéladio Cissé, Nesre Redi, Samuel Fuhrimann, John Okedi, Christian Schindler, Martin Röösli, Neil Philip Armitage, Kirsty Carden, and et al. 2021. "Diarrhoea among Children Aged under Five Years and Risk Factors in Informal Settlements: A Cross-Sectional Study in Cape Town, South Africa" International Journal of Environmental Research and Public Health 18, no. 11: 6043. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18116043