
Burnout in Intensive Care Unit Workers during the Second Wave of the COVID-19 Pandemic: A Single Center Cross-Sectional Italian Study

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analyses
3. Results
3.1. Mental Health Outcomes
3.2. Factors Associated with Burnout
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Nurses (N = 84) | % | Physicians (N = 52) | % | Total (N = 136) | % | χ2 (p) | |
|---|---|---|---|---|---|---|---|
| Maslach burnout inventory (MBI) | |||||||
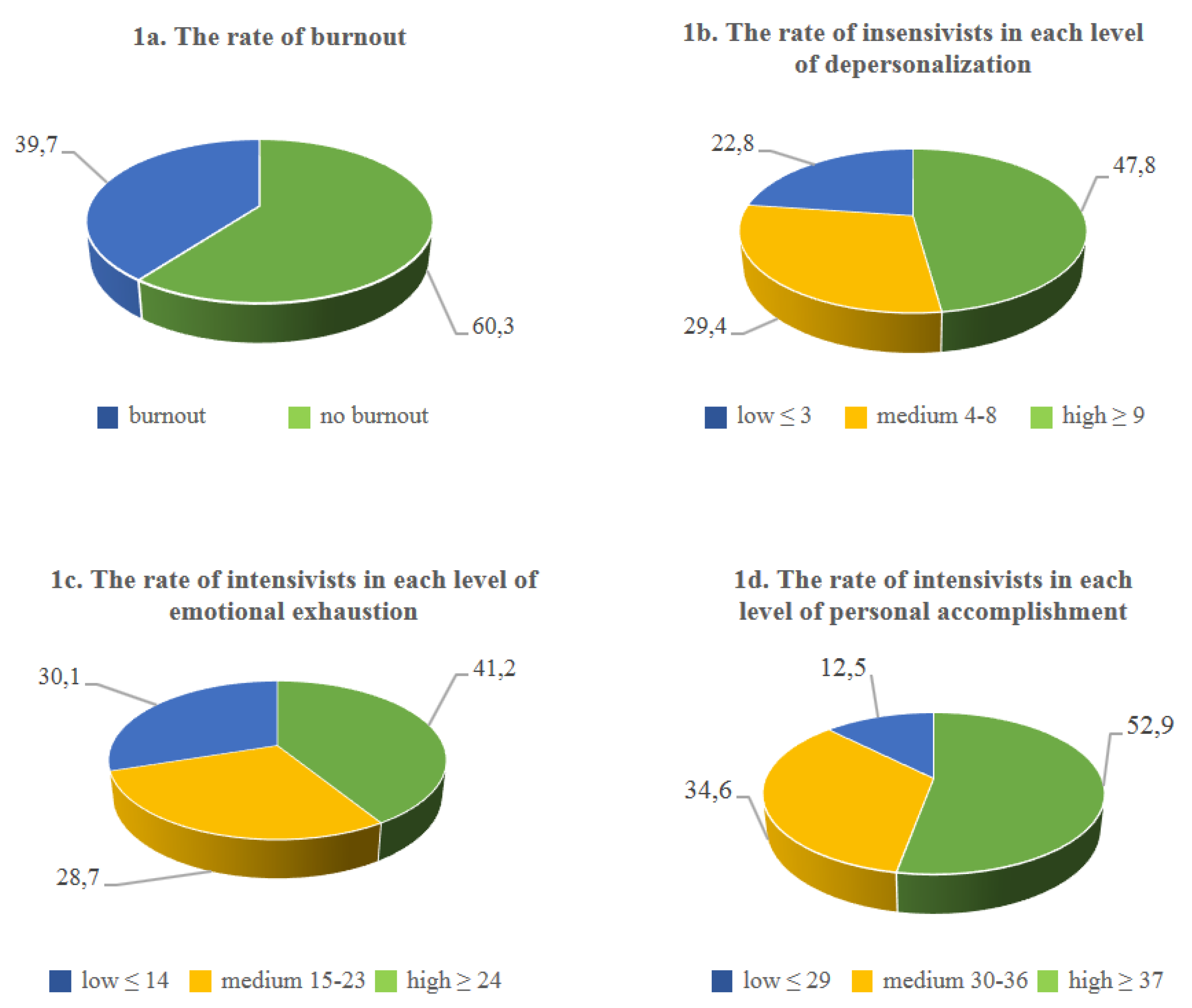
| Emotional exhaustion sub score (EE) | |||||||
| Low | 27 | 32.1 | 14 | 26.9 | 41 | 30.1 | 0.77 (0.68) |
| Medium | 22 | 26.2 | 17 | 32.7 | 39 | 28.7 | |
| High | 35 | 41.7 | 21 | 40.4 | 56 | 41.2 | |
| Total | 84 | 100.0 | 52 | 100.0 | 136 | 100.0 | |
| Depersonalization sub score (DP) | |||||||
| Low | 19 | 22.6 | 12 | 23.1 | 31 | 22.8 | 5.68 (0.06) |
| Medium | 19 | 22.6 | 21 | 40.4 | 40 | 29.4 | |
| High | 46 | 54.8 | 19 | 36.5 | 65 | 47.8 | |
| Total | 84 | 100.0 | 52 | 100.0 | 136 | 100.0 | |
| Personal accomplishment sub score (PA) | |||||||
| Low | 44 | 52.4 | 28 | 53.8 | 72 | 52.9 | 0.07 (0.96) |
| Medium | 29 | 34.5 | 18 | 34.6 | 47 | 34.6 | |
| High | 11 | 13.1 | 6 | 11.5 | 17 | 12.5 | |
| Total | 84 | 100.0 | 52 | 100.0 | 136 | 100.0 | |
| Burnout | |||||||
| Yes 1 | 52 | 61.9 | 30 | 57.7 | 82 | 60.3 | |
| No | 32 | 38.1 | 22 | 42.3 | 54 | 39.7 | |
| Total | 84 | 100.0 | 52 | 100.0 | 136 | 100.0 | |
| Burnout in EE and DP and PA 2 | 22 | 26.2 | 9 | 17.3 | 31 | 22.8 | |
| Burnout in EE or DP or PA 3 | 34 | 40.5 | 25 | 48.1 | 59 | 43.4 | |
| Low burnout in EE and DP and PA 4 | 20 | 23.8 | 10 | 19.2 | 30 | 22.1 | |
| Hospital anxiety and depression scale (HADS): | |||||||
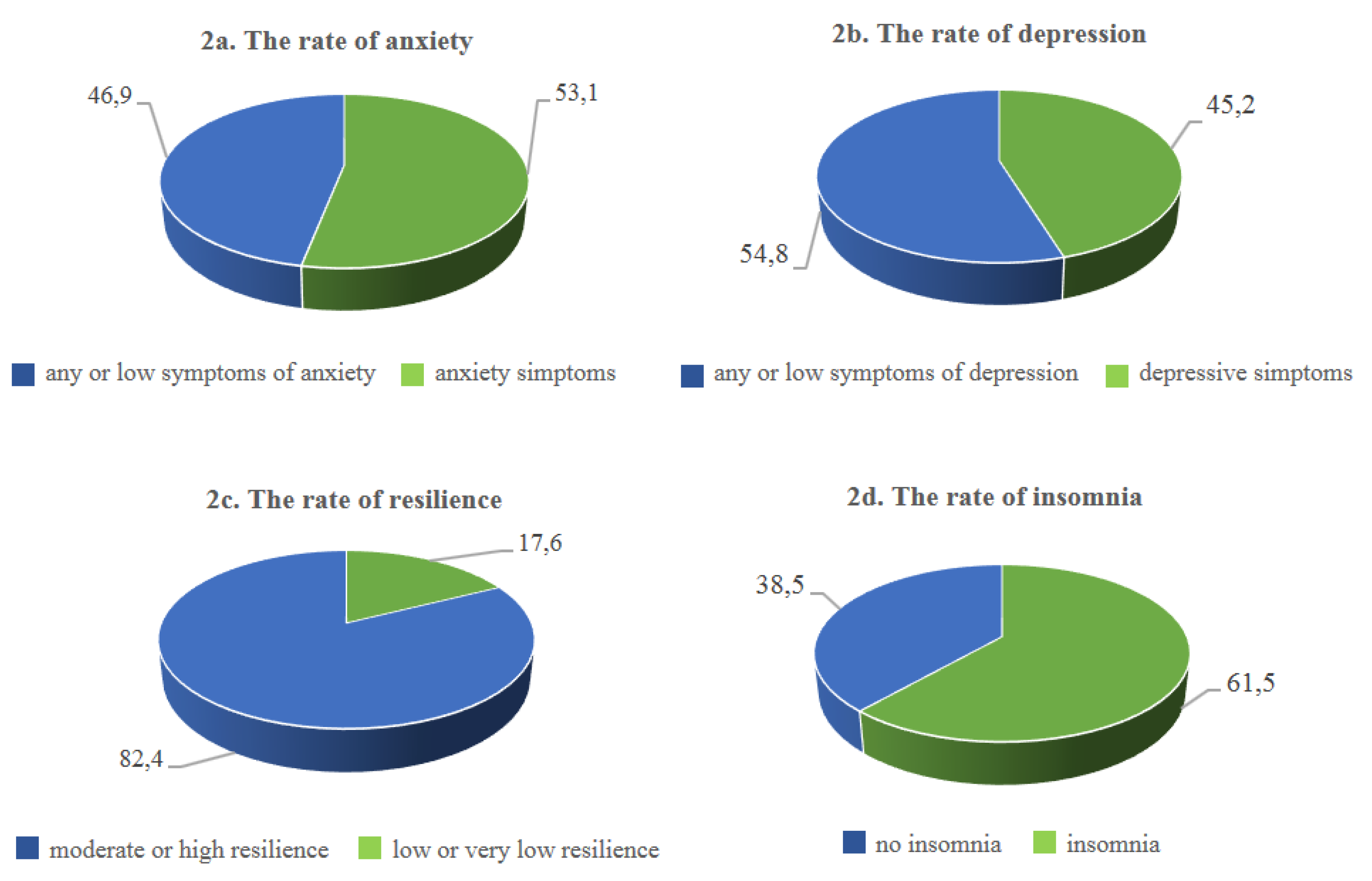
| Anxiety | |||||||
| Normal | 30 | 38.5 | 30 | 60.0 | 60 | 46.9 | 5.68 (0.02) |
| Presence of symptoms of anxiety | 48 | 61.5 | 20 | 40.0 | 68 | 53.1 | |
| Total | 78 | 100.0 | 50 | 100.0 | 128 | 100.0 | |
| Missing | 6 | 2 | 8 | ||||
| Depression | |||||||
| Normal | 40 | 51.3 | 29 | 60.4 | 69 | 54.8 | 1.00 (0.32) |
| Presence of symptoms of depression | 38 | 48.7 | 19 | 39.6 | 57 | 45.2 | |
| Total | 78 | 100.0 | 48 | 100.0 | 126 | 100.0 | |
| Missing | 6 | 4 | 10 | ||||
| Resilience | |||||||
| Low or very low | 16 | 19.0 | 8 | 15.4 | 24 | 17.6 | 0.30 (0.59) |
| Moderate or high | 68 | 81.0 | 44 | 84.6 | 112 | 82.4 | |
| Total | 84 | 100.0 | 52 | 100.0 | 136 | 100.0 | |
| Missing | - | - | - | ||||
| Insomnia | |||||||
| No clinically significant insomnia | 22 | 28.9 | 25 | 54.3 | 47 | 38.5 | 7.81 (0.005) |
| Presence of symptoms of insomnia | 54 | 71.1 | 21 | 45.7 | 75 | 61.5 | |
| Total | 76 | 100.0 | 46 | 100.0 | 122 | 100.0 | |
| Missing | 8 | 6 | 14 |
| No Burnout (N = 54) | % | Burnout (N = 82) | % | Total (N = 136) | % | OR (CI 95%) or F (p) | |
|---|---|---|---|---|---|---|---|
| Age: | |||||||
| <35 | 18 | 33.3 | 36 | 43.9 | 54 | 39.7 | 1.56 (0.77–3.20) |
| ≥35 | 36 | 66.7 | 46 | 56.1 | 82 | 60.3 | Ref |
| Total | 54 | 100.0 | 82 | 100.0 | 136 | 100.0 | |
| Age * | 54; 39.9; 38 (23–58) | 82; 38.7; 37 (23–68) | 136; 39.1; 37 (23–68) | 1.16 (0.57) | |||
| Sex: | |||||||
| Male | 24 | 46.2 | 31 | 37.8 | 55 | 41.0 | 0.71 (0.35–1.43) |
| Female | 28 | 53.8 | 51 | 62.2 | 79 | 59.0 | Ref |
| Total | 52 | 100.0 | 82 | 100.0 | 134 | 100.0 | |
| Missing | 2 | - | 2 | ||||
| Profession: | |||||||
| Nurse | 32 | 59.3 | 52 | 63.4 | 84 | 61.8 | Ref |
| Physician | 22 | 40.7 | 30 | 36.6 | 52 | 38.2 | 0.84 (0.41–1.70) |
| Total | 54 | 100.0 | 82 | 100.0 | 136 | 100.0 | |
| Missing | - | - | - | ||||
| Living alone: | |||||||
| Yes | 10 | 22.2 | 20 | 28.2 | 30 | 25.9 | 1.37 (0.57–3.28) |
| No | 35 | 77.8 | 51 | 71.8 | 86 | 74.1 | Ref |
| Total | 45 | 100.0 | 71 | 100.0 | 116 | 100.0 | |
| Missing | 9 | 11 | 20 | ||||
| Worry about transmitting the virus to the people you live with: | |||||||
| No/a little | 14 | 42.4 | 19 | 38.8 | 33 | 40.2 | 0.86 (0.35–2.11) |
| A lot | 19 | 57.6 | 30 | 61.2 | 49 | 59.8 | Ref |
| Total | 33 | 100.0 | 49 | 100.0 | 82 | 100.0 | |
| Missing | 2 | 2 | 4 | ||||
| Year of work experience | |||||||
| 46;12.4; 6 (1–34) | 68; 14.6; 13 (0–41) | 114; 13.7; 11 (0–41) | 1.25 (0.43) | ||||
| Missing | 8 | 14 | 22 | ||||
| Work area before the pandemic: | |||||||
| ICU | 30 | 57.7 | 57 | 74.0 | 87 | 67.4 | 2.09 (0.99–4.42) |
| Operating room/surgery/Other | 22 | 42.3 | 20 | 26.0 | 42 | 32.6 | Ref |
| Total | 52 | 100.0 | 77 | 100.0 | 129 | 100.0 | |
| Missing | 2 | 5 | 7 | ||||
| Difficulties in adapting to the new work environment: | |||||||
| Not at all | 27 | 52.9 | 30 | 41.1 | 57 | 46.0 | Ref |
| Yes | 24 | 47.1 | 43 | 58.9 | 67 | 54.0 | 1.61 (0.78–3.32) |
| Total | 51 | 100.0 | 73 | 100.0 | 124 | 100.0 | |
| Missing | 3 | 9 | 12 | ||||
| Compared to before the Covid emergency, the patient number/ workload has: | |||||||
| Increased | 29 | 59.2 | 44 | 57.9 | 73 | 58.4 | Ref |
| Equal/diminished | 20 | 40.8 | 32 | 42.1 | 52 | 41.6 | 1.05 (0.51–2.19) |
| Total | 49 | 100.0 | 76 | 100.0 | 125 | 100.0 | |
| Missing | 5 | 6 | 11 | ||||
| Compared to before the Covid emergency, how do you evaluate the relationship with your colleagues? | |||||||
| Improved | 30 | 60.0 | 41 | 55.4 | 71 | 57.3 | Ref |
| Equal/ Got worse | 20 | 40.0 | 33 | 44.6 | 53 | 42.7 | 1.21 (0.58–2.50) |
| Total | 50 | 100.0 | 74 | 100.0 | 124 | 100.0 | |
| Missing | 4 | 8 | 12 | ||||
| Compared to before the Covid emergency, there are opportunities to discuss important decisions in groups: | |||||||
| More frequent | 26 | 50.0 | 34 | 46.6 | 60 | 48.0 | Ref |
| Equal/Less frequent | 26 | 50.0 | 39 | 53.4 | 65 | 52.0 | 1.15 (0.56–2.34) |
| Total | 52 | 100.0 | 73 | 100.0 | 125 | 100.0 | |
| Missing | 2 | 9 | 11 | ||||
| Do you feel protected when you work? | |||||||
| No/a little bit | 17 | 32.1 | 38 | 48.7 | 55 | 42.0 | 2.01 (0.97–4.16) |
| Protected | 36 | 67.9 | 40 | 51.3 | 76 | 58.0 | Ref |
| Total | 53 | 100.0 | 78 | 100.0 | 131 | 100.0 | |
| Missing | 1 | 3 | 4 | ||||
| Hospital anxiety and depression scale (HADS): | |||||||
| Anxiety | |||||||
| Normal | 36 | 70.6 | 24 | 31.2 | 60 | 46.9 | Ref |
| Presence of symptoms of anxiety | 15 | 29.4 | 53 | 68.8 | 68 | 53.1 | 5.3 (2.45–11.46) |
| Total | 51 | 100.0 | 77 | 100.0 | 128 | 100.0 | |
| Missing | 3 | 5 | 8 | ||||
| Depression | |||||||
| Normal | 41 | 78.8 | 28 | 37.8 | 69 | 54.8 | Ref |
| Presence of symptoms of depression | 11 | 21.2 | 46 | 62.2 | 57 | 45.2 | 6.12 (2.71–13.83) |
| Total | 52 | 100.0 | 74 | 100.0 | 126 | 100.0 | |
| Missing | 2 | 8 | 10 | ||||
| Resilience | |||||||
| Low or very low | 6 | 11.1 | 18 | 22.0 | 24 | 17.6 | 2.25 (0.83–6.10) |
| Moderate or high | 48 | 88.9 | 64 | 78.0 | 112 | 82.4 | Ref |
| Total | 54 | 100.0 | 82 | 100.0 | 136 | 100.0 | |
| Missing | |||||||
| Insomnia | |||||||
| Presence of symptoms of insomnia | 22 | 45.8 | 53 | 71.6 | 75 | 61.5 | 2.98 (1.39–6.38) |
| No clinically significant insomnia | 26 | 54.2 | 21 | 28.4 | 47 | 38.5 | Ref |
| Total | 48 | 100.0 | 74 | 100.0 | 122 | 100.0 | |
| Missing | 6 | 8 | 14 | ||||
References
- ReferencesColville, G.A.; Smith, J.G.; Brierley, J.; Citron, K.; Nguru, N.M.; Shaunak, P.D.; Tam, O.; Perkins-Porras, L. Coping with staff burnout and work-related posttraumatic stress in intensive care. Pediatr. Crit. Care Med. 2017, 18, e267–e273. [Google Scholar]
- Costa, D.K.; Moss, M. The cost of caring: Emotion, burnout, and psychological distress in critical care clinicians. Ann. Am. Thorac. Soc. 2018, 15, 787–790. [Google Scholar] [CrossRef]
- Mealer, M.; Burnham, E.L.; Goode, C.J.; Rothbaum, B.; Moss, M. The prevalence and impact of post traumatic stress disorder and burnout syndrome in nurses. Depress Anxiety 2009, 26, 1118–1126. [Google Scholar] [CrossRef] [Green Version]
- Chuang, C.H.; Tseng, P.C.; Lin, C.Y.; Lin, K.H.; Chen, Y.Y. Burnout in the intensive care unit professionals: A systematic review. Medicine 2016, 95, e5629. [Google Scholar] [CrossRef]
- Grasselli, G.; Zangrillo, A.; Zanella, A.; Antonelli, M.; Cabrini, L.; Castelli, A.; Cereda, D.; Coluccello, A.; Foti, G.; Fumagalli, R.; et al. Baseline characteristics and outcomes of 1591 patients infected with SARS-CoV-2 admitted to ICUs of the Lombardy region, italy. JAMA 2020, 323, 1574–1581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fusar-Poli, P.; Brambilla, P.; Solmi, M. Learning from COVID-19 pandemic in northern Italy: Impact on mental health and clinical care. J. Affect. Disord. 2020, 275, 78–79. [Google Scholar] [CrossRef] [PubMed]
- Lai, J.; Ma, S.; Wang, Y.; Cai, Z.; Hu, J.; Wei, N.; Wu, J.; Du, H.; Chen, T.; Li, R.; et al. Factors associated with mental health outcomes among health care workers exposed to coronavirus disease 2019. JAMA Netw. Open. 2020, 3, e203976. [Google Scholar] [CrossRef]
- Da Silva, F.C.T.; Barbosa, C.P. The impact of the COVID-19 pandemic in an intensive care unit (ICU): Psychiatric symptoms in healthcare professionals- a systematic review. J. Psychiatr. Res. 2020; in press. [Google Scholar]
- Saracoglu, K.T.; Simsek, T.; Kahraman, S.; Bombaci, E.; Sezen, Ö.; Saracoglu, A.; Demirhan, R. The psychological impact of COVID-19 disease is more severe on intensive care unit healthcare providers: A cross-sectional study. Clin. Psychopharmacol. Neurosci. 2020, 18, 607–615. [Google Scholar] [CrossRef] [PubMed]
- Greenberg, N.; Weston, D.; Hall, C.; Caulfield, T.; Williamson, V.; Fong, K. Mental health of staff working in intensive care during COVID-19. Occup. Med. 2021, 71, 62–67. [Google Scholar] [CrossRef] [PubMed]
- Caillet, A.; Coste, C.; Sanchez, R.; Allaouchiche, B. Psychological impact of COVID-19 on ICU caregivers. Anaesth. Crit. Care Pain Med. 2020, 39, 717–722. [Google Scholar] [CrossRef]
- Dinibutun, S.R. Factors associated with burnout among physicians: An evaluation during a period of COVID-19 pandemic. J. Healthc. Leadersh. 2020, 12, 85–94. [Google Scholar] [CrossRef]
- Azoulay, E.; De Waele, J.; Ferrer, R.; Azoulay, E.; De Waele, J.; Ferrer, R.; Staudinger, T.; Borkowska, M.; Povoa, P.; Iliopoulou, K.; et al. ESICM Symptoms of burnout in intensive care unit specialists facing the COVID-19 outbreak. Ann. Intensive Care 2020, 10, 110. [Google Scholar] [CrossRef]
- Kok, N.; van Gurp, J.; Teerenstra, S.; van der Hoeven, H.; Fuchs, M.; Hoedemaekers, C.; Zegers, M. Coronavirus disease 2019 immediately increases burnout symptoms in icu professionals: A longitudinal cohort study. Crit. Care Med. 2021, 49, 419–427. [Google Scholar] [CrossRef]
- Schaufeli, W.B.; Greenglass, E.R. Introduction to special issue on burnout and health. Psychol. Health 2001, 16, 501–510. [Google Scholar] [CrossRef]
- Maslach, C.; Leiter, M.P. Understanding the burnout experience: Recent research and its implications for psychiatry. World Psychiatry 2016, 15, 103–111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arrogante, O.; Aparicio-Zaldivar, E.G. Burnout and health among critical care professionals: The mediational role of resilience. Intensive Crit. Care Nurs. 2017, 42, 110–115. [Google Scholar] [CrossRef] [PubMed]
- Hancock, J.; Witter, T.; Comber, S.; Daley, P.; Thompson, K.; Candow, S.; Follett, G.; Somers, W.; Collins, C.; White, J.; et al. Understanding burnout and moral distress to build resilience: A qualitative study of an interprofessional intensive care unit team. Can J. Anaesth. 2020, 67, 1541–1548. [Google Scholar] [CrossRef]
- Schneiderman, N.; Ironson, G.; Siegel, S.D. Stress and health: Psychological, behavioral, and biological determinants. Annu. Rev. Clin. Psychol. 2005, 1, 607–628. [Google Scholar] [CrossRef] [Green Version]
- Serrão, C.; Duarte, I.; Castro, L.; Teixeira, A. Burnout and depression in portuguese healthcare workers during the COVID-19 pandemic-the mediating role of psychological resilience. Int. J. Environ. Res. Public Health 2021, 18, 636. [Google Scholar] [CrossRef] [PubMed]
- Bonati, M.; Campi, R.; Zanetti, M.; Cartabia, M.; Scarpellini, F.; Clavenna, A.; Segre, G. Psychological distress among Italians during the 2019 coronavirus disease (COVID-19) quarantine. BMC Psychiatry 2021, 21, 20. [Google Scholar] [CrossRef]
- Ciprandi, R.; Bonati, M.; Campi, R.; Pescini, R.; Castellani, C. Psychological distress in adults with and without cystic fibrosis during the COVID-19 lockdown. J. Cyst. Fibros. 2021, 20, 198–204. [Google Scholar] [CrossRef]
- Maslach, C.; Jackson, S.E.; Leiter, M.P. Maslach Burnout Inventory, 3rd ed.; Zalaquett, C.P., Wood, R.J., Eds.; Evaluating Stress: A Book of Resources; Scarecrow Education: Lanham, Maryland, 1986; pp. 191–218. [Google Scholar]
- Dyrbye, L.N.; West, C.P.; Shanafelt, T.D. Defining burnout as a dichotomous variable. J. Gen. Intern. Med. 2009, 24, 440–441. [Google Scholar] [CrossRef]
- Sirigatti, S.; Stefanile, C.; Menoni, E. Per un adattamento italiano del Maslach Burnout Inventory (MBI). Boll. Di Psicol. Appl. 1998, 187–188, 33–39. [Google Scholar]
- Naldi, A.; Vallelonga, F.; Di Liberto, A.; Cavallo, R.; Agnesone, M.; Gonella, M.; Sauta, M.D.; Lochner, P.; Tondo, G.; Bragazzi, N.L.; et al. COVID-19 pandemic-related anxiety, distress and burnout: Prevalence and associated factors in healthcare workers of North-West Italy. B. J. Psych. Open 2021, 7, e27. [Google Scholar] [CrossRef]
- Aylard, P.R.; Gooding, J.H.; McKenna, P.J.; Snaith, R.P. A validation study of three anxiety and depression self-assessment scales. J. Psychosom. Res. 1987, 31, 261–268. [Google Scholar] [CrossRef]
- Bjelland, I.; Dahl, A.A.; Haug, T.T.; Neckelmann, D. The validity of the Hospital Anxiety and Depression Scale. An updated literature review. J. Psychosom. Res. 2002, 52, 69–77. [Google Scholar] [CrossRef]
- Friborg, O.; Hjemdal, O.; Rosenvinge, J.H.; Martinussen, M. A new rating scale for adult resilience: What are the central protective resources behind healthy adjustment? Int. J. Methods Psychiatr. Res. 2003, 12, 65–76. [Google Scholar] [CrossRef] [PubMed]
- Callegari, C.; Bertù, L.; Lucano, M.; Ielmini, M.; Braggio, E.; Vender, S. Reliability and validity of the Italian version of the 14-item Resilience Scale. Psychol. Res. Behav. Manag. 2016, 9, 277–284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Busch, I.M.; Moretti, F.; Mazzi, M.; Wu, A.W.; Rimondini, M. What we have learned from two decades of epidemics and pandemics: A systematic review and meta-analysis of the psychological burden of frontline healthcare workers. Psychother Psychosom. 2021, 90, 178–190. [Google Scholar] [CrossRef] [PubMed]
- Chor, W.; Ng, W.M.; Cheng, L.; Situ, W.; Chong, J.W.; Ng, L.; Mok, P.L.; Yau, Y.W.; Lin, Z. Burnout amongst emergency healthcare workers during the COVID-19 pandemic: A multi-center study. Am. J. Emerg. Med. 2020. [Google Scholar] [CrossRef]
- Wang, J.; Hu, B.; Peng, Z.; Song, H.; Cai, S.; Rao, X.; Li, L.; Li, J. Prevalence of burnout among intensivists in mainland China: A nationwide cross-sectional survey. Crit. Care 2021, 25, 8. [Google Scholar] [CrossRef] [PubMed]
- Barello, S.; Palamenghi, L.; Graffigna, G. Burnout and somatic symptoms among frontline healthcare professionals at the peak of the Italian COVID-19 pandemic. Psychiatry Res. 2020, 290, 113129. [Google Scholar] [CrossRef] [PubMed]
- Agostinelli, A.; La Torre, G.; Bevilacqua, F.; Chiaradia, G.; Specchia, M.L.; Ricciardi, W. Il burnout nel personale sanitario ospedaliero: Risultati di uno studio trasversale condotto in un policlinico universitario a Roma [Burnout in healthcare workers of a university teaching hospital in Rome, Italy: A cross-sectional study]. Ig. Sanita Pubbl. 2008, 64, 41–52. [Google Scholar] [PubMed]
- Jose, S.; Dhandapani, M.; Cyriac, M.C. Burnout and resilience among frontline nurses during COVID-19 pandemic: A cross-sectional study in the emergency department of a tertiary care center, North India. Indian J. Crit. Care Med. 2020, 24, 1081–1088. [Google Scholar]
- West, C.P.; Dyrbye, L.N.; Shanafelt, T.D. Physician burnout: Contributors, consequences and solutions. J. Intern. Med. 2018, 283, 516–529. [Google Scholar] [CrossRef] [Green Version]
- Lasalvia, A.; Bonetto, C.; Porru, S.; Carta, A.; Tardivo, S.; Bovo, C.; Ruggeri, M.; Amaddeo, F. Psychological impact of COVID-19 pandemic on healthcare workers in a highly burdened area of north-east Italy. Epidemiol. Psychiatr. Sci. 2020, 30, e1. [Google Scholar] [CrossRef]
- Dykes, N.; Johnson, O.; Bamford, P. Assessing the psychological impact of COVID-19 on intensive care workers: A single-centre cross-sectional UK-based study. J. Intensive Care Soc. 2021. [Google Scholar] [CrossRef]
- Shen, X.; Zou, X.; Zhong, X.; Yan, J.; Li, L. Psychological stress of ICU nurses in the time of COVID-19. Crit. Care 2020, 24, 200. [Google Scholar] [CrossRef]
- Moradi, Y.; Baghaei, R.; Hosseingholipour, K.; Mollazadeh, F. Challenges experienced by ICU nurses throughout the provision of care for COVID-19 patients: A qualitative study. J. Nurs. Manag. 2021, 22. [Google Scholar] [CrossRef]
- Zhang, H.; Ye, Z.; Tang, L.; Zou, P.; Du, C.; Shao, J.; Wang, X.; Chen, D.; Qiao, G.; Mu, S.Y. Anxiety symptoms and burnout among Chinese medical staff of intensive care unit: The moderating effect of social support. BMC Psychiatry 2020, 20, 197. [Google Scholar] [CrossRef]
- Secosan, I.; Virga, D.; Crainiceanu, Z.P.; Bratu, L.M.; Bratu, T. Infodemia: Another Enemy for Romanian Frontline Healthcare Workers to Fight during the COVID-19 Outbreak. Medicina 2020, 56, 679. [Google Scholar] [CrossRef]
- Bai, Y.; Lin, C.C.; Lin, C.Y.; Chen, J.Y.; Chue, C.M.; Chou, P. Survey of stress reactions among health care workers involved with the SARS outbreak. Psychiatr. Serv. 2004, 55, 1055–1057. [Google Scholar] [CrossRef] [PubMed]
- West, C.P.; Dyrbye, L.N.; Sinsky, C.; Trockel, M.; Tutty, M.; Nedelec, L.; Shanafelt, T.D. Resilience and burnout among physicians and the general US working population. JAMA Netw. Open 2020, 3, e209385. [Google Scholar] [CrossRef] [PubMed]


| Nurses (N = 84) | % | Physicians (N = 52) | % | Total (N = 136) | % | χ or F | p-Value | |
|---|---|---|---|---|---|---|---|---|
| Age: | ||||||||
| <35 | 37 | 44.0 | 17 | 32.7 | 54 | 39.7 | χ2 = 1.7299 | 0.1884 |
| ≥35 | 47 | 56.0 | 35 | 67.3 | 82 | 60.3 | ||
| Total | 84 | 100.0 | 52 | 100.0 | 136 | 100.0 | ||
| Age * | 38.5; 36.5 (23–58) | 40.1; 38 (28–68) | 39.1; 37 (23–68) | F = 1.42 | 0.1770 | |||
| Sex: | ||||||||
| Male | 30 | 36.6 | 25 | 48.1 | 55 | 41.0 | χ2 = 1.7366 | 0.1876 |
| Female | 52 | 63.4 | 27 | 51.9 | 79 | 59.0 | ||
| Total | 82 | 100.0 | 52 | 100.0 | 134 | 100.0 | ||
| Missing | 2 | - | 2 | |||||
| Living alone: | ||||||||
| Yes | 20 | 27.4 | 10 | 23.3 | 30 | 25.9 | χ2 = 0.2421 | 0.6227 |
| No | 53 | 72.6 | 33 | 76.7 | 86 | 74.1 | ||
| Total | 73 | 100.0 | 43 | 100.0 | 116 | 100.0 | ||
| Missing | 11 | 9 | 20 | |||||
| Worry about transmitting the virus to the people you live with: | ||||||||
| No/a little | 16 | 30.8 | 17 | 56.7 | 33 | 40.2 | χ2 = 5.3057 | 0.0213 |
| A lot | 36 | 69.2 | 13 | 43.3 | 49 | 59.8 | ||
| Total | 52 | 100.0 | 30 | 100.0 | 82 | 100.0 | ||
| Missing | 1 | 3 | 4 | |||||
| Year of work experience | ||||||||
| 71; 15.9; 15 (0–36) | 43; 10.2; 6 (0–41) | 114; 13.7; 11 (0–41) | F = 1.45 | 0.1955 | ||||
| Missing | 13 | 9 | 22 | |||||
| Work area before the pandemic: | ||||||||
| ICU | 49 | 62.0 | 38 | 76.0 | 87 | 67.4 | χ2 = 2.7233 | 0.0989 |
| Operating room/surgery/Other | 30 | 38.0 | 12 | 24.0 | 42 | 32.6 | ||
| Total | 79 | 100.0 | 50 | 100.0 | 129 | 100.0 | ||
| Missing | 5 | 2 | 7 | |||||
| Difficulties in adapting to the new work environment: | ||||||||
| Not at all | 31 | 40.3 | 26 | 55.3 | 57 | 46.0 | χ2 = 2.6649 | 0.1026 |
| Yes | 46 | 59.7 | 21 | 44.7 | 67 | 54.0 | ||
| Total | 77 | 100.0 | 47 | 100.0 | 124 | 100.0 | ||
| Missing | 7 | 5 | 12 | |||||
| Compared to before the Covid emergency the patient number/ workload has: | ||||||||
| Increased | 40 | 51.9 | 33 | 68.8 | 73 | 58.4 | χ2 = 3.4359 | 0.0638 |
| Equal/diminished | 37 | 48.1 | 15 | 31.3 | 52 | 41.6 | ||
| Total | 77 | 100.0 | 48 | 100.0 | 125 | 100.0 | ||
| Missing | 7 | 4 | 11 | |||||
| Compared to before the Covid emergency, how do you evaluate the relationship with your colleagues? | ||||||||
| Improved | 41 | 55.4 | 30 | 60.0 | 71 | 57.3 | χ2 = 0.2574 | 0.6119 |
| Equal/Got worse | 33 | 44.6 | 20 | 40.0 | 53 | 42.7 | ||
| Total | 74 | 100.0 | 50 | 100.0 | 124 | 100.0 | ||
| Missing | 10 | 2 | 12 | |||||
| Compared to before the Covid emergency, there are opportunities to discuss important decisions in groups: | ||||||||
| More frequent | 33 | 42.9 | 27 | 56.3 | 60 | 48.0 | χ2 = 2.1248 | 0.1449 |
| Equal/Less frequent | 44 | 57.1 | 21 | 43.8 | 65 | 52.0 | ||
| Total | 77 | 100.0 | 48 | 100.0 | 125 | 100.0 | ||
| Missing | 7 | 4 | 11 | |||||
| Do you feel protected when you work? | ||||||||
| No/a little bit | 33 | 41.3 | 22 | 43.1 | 55 | 42.0 | χ2 = 0.0455 | 0.8310 |
| Yes | 47 | 58.8 | 29 | 56.9 | 76 | 58.0 | ||
| Total | 80 | 100.0 | 51 | 100.0 | 131 | 100.0 | ||
| Missing | 4 | 1 | 5 | |||||
| OR 1 | CI 95% | p-Value | |
|---|---|---|---|
| Age | |||
| <35 vs. ≥35 | 1.15 | 0.42–3.15 | 0.7851 |
| Sex: | |||
| Male vs. Female | 0.86 | 0.32–2.33 | 0.7684 |
| Profession | |||
| Physicians vs. Nurses | 1.19 | 0.45–3.11 | 0.7277 |
| Living alone | |||
| Yes vs. No | 0.97 | 0.30–3.13 | 0.9619 |
| Work area before the pandemic | |||
| ICU vs. Operating room/Surgery/Other | 3.02 | 1.06–8.58 | 0.0384 |
| Difficulties in adapting to the new work environment: | |||
| Yes vs. Not at all | 1.55 | 0.59–4.10 | 0.3772 |
| Compared to before the Covid-19 emergency, the patient number/workload has | |||
| Equal/diminished vs. Increased | 1.50 | 0.53–4.28 | 0.4443 |
| Compared to before the Covid-19 emergency, how do you evaluate the relationship with your colleagues? | |||
| Equal/Got worse vs. Improved | 1.91 | 0.63–5.85 | 0.2555 |
| Compared to before the Covid-19 emergency, there are opportunities to discuss decisions in groups | |||
| Equal/Less frequent vs. More frequent | 0.56 | 0.18–1.69 | 0.3003 |
| Do you feel protected when you work? | |||
| No/a little bit vs. Yes | 1.35 | 0.49–3.69 | 0.5641 |
| Anxiety | |||
| Symptoms vs. Normal | 2.39 | 0.81–7.05 | 0.1146 |
| Depression | |||
| Symptoms vs. Normal | 4.88 | 1.54–15.48 | 0.0071 |
| Resilience | |||
| Moderate/High vs. Low or very low | 0.76 | 0.20–3.00 | 0.7004 |
| Insomnia | |||
| Presence of symptoms of insomnia vs. No clinically significant insomnia | 2.33 | 0.82–6.65 | 0.1129 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stocchetti, N.; Segre, G.; Zanier, E.R.; Zanetti, M.; Campi, R.; Scarpellini, F.; Clavenna, A.; Bonati, M. Burnout in Intensive Care Unit Workers during the Second Wave of the COVID-19 Pandemic: A Single Center Cross-Sectional Italian Study. Int. J. Environ. Res. Public Health 2021, 18, 6102. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18116102
Stocchetti N, Segre G, Zanier ER, Zanetti M, Campi R, Scarpellini F, Clavenna A, Bonati M. Burnout in Intensive Care Unit Workers during the Second Wave of the COVID-19 Pandemic: A Single Center Cross-Sectional Italian Study. International Journal of Environmental Research and Public Health. 2021; 18(11):6102. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18116102
Chicago/Turabian StyleStocchetti, Nino, Giulia Segre, Elisa R. Zanier, Michele Zanetti, Rita Campi, Francesca Scarpellini, Antonio Clavenna, and Maurizio Bonati. 2021. "Burnout in Intensive Care Unit Workers during the Second Wave of the COVID-19 Pandemic: A Single Center Cross-Sectional Italian Study" International Journal of Environmental Research and Public Health 18, no. 11: 6102. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18116102