
Lack of Informations about COVID-19 Vaccine: From Implications to Intervention for Supporting Public Health Communications in COVID-19 Pandemic

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
- Sociodemographic data of participants.
- 2.
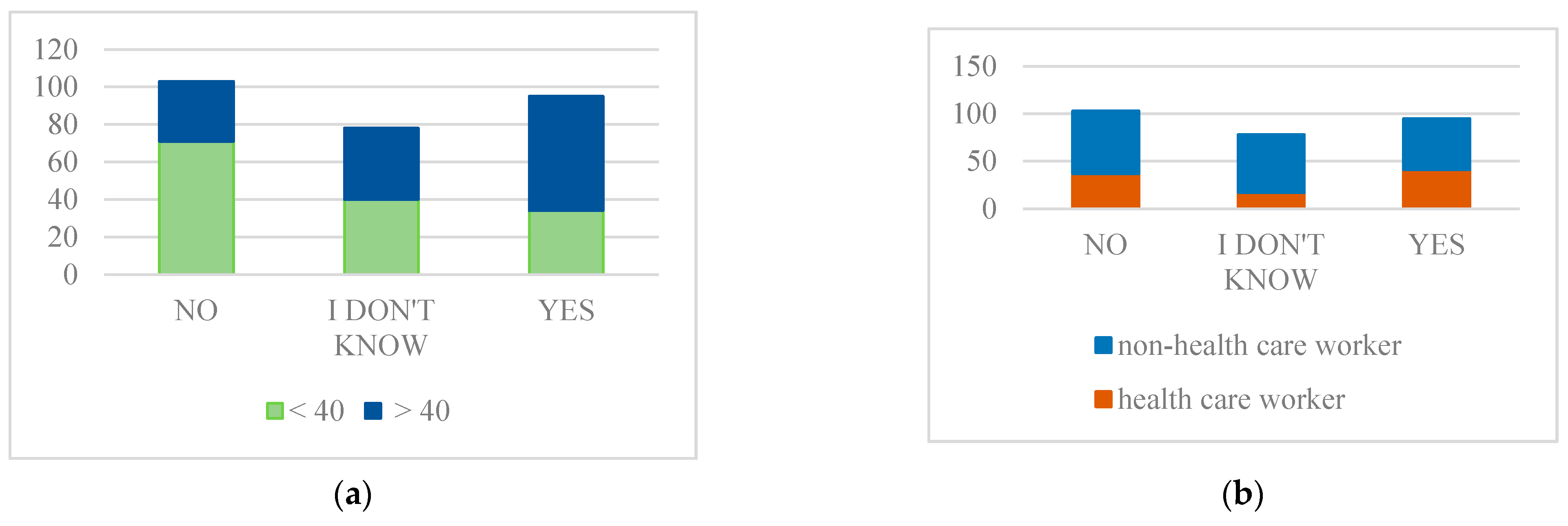
- Intention to get vaccinated
- 3.
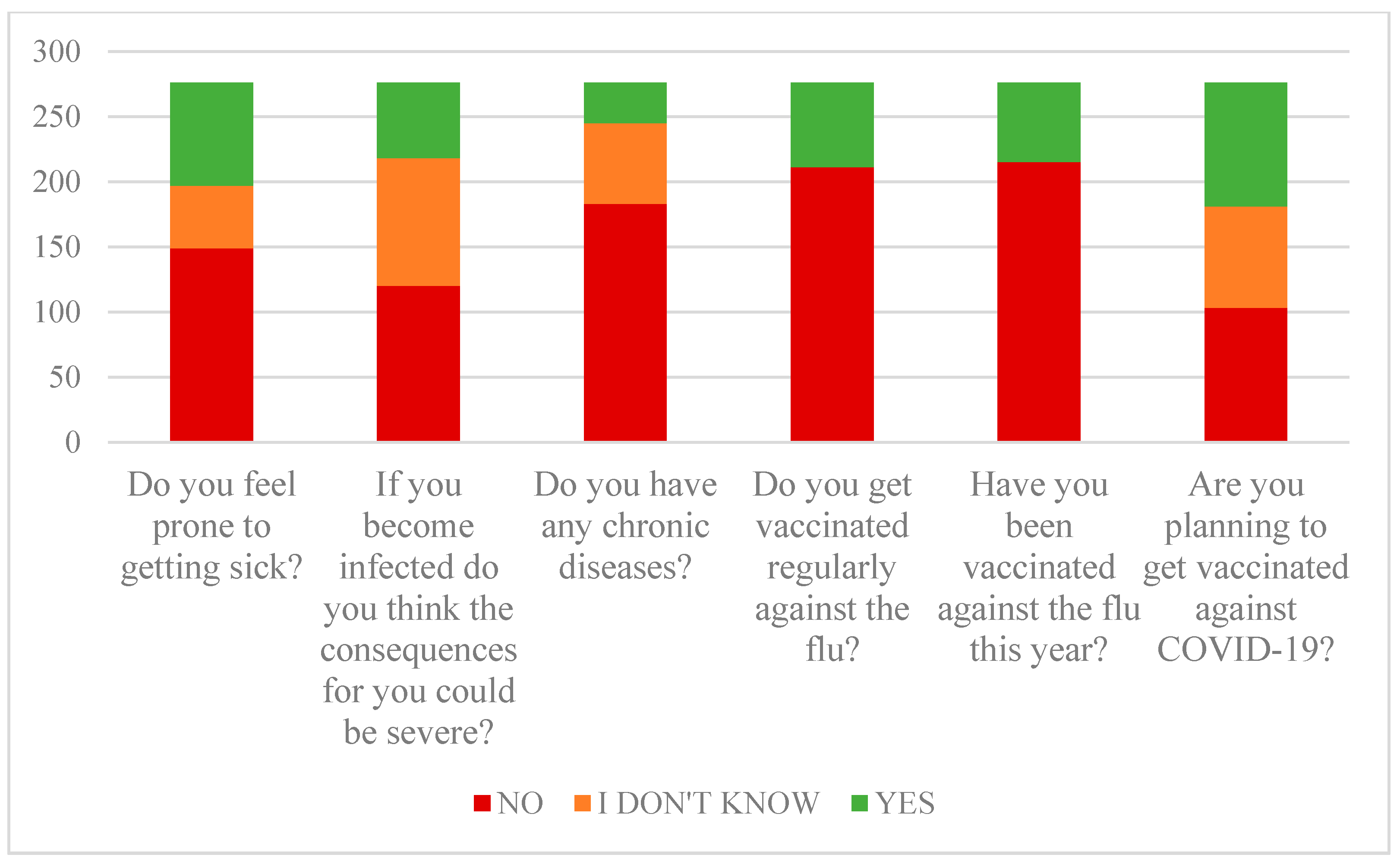
- Perception of one’s susceptibility for infection
3.1. Perception of Disease Danger
3.2. Perception of Vaccine Protective Effect and Risk Associated with Vaccine
3.3. Organisational Barriers
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lescure, F.-X.; Bouadma, L.; Nguyen, D.; Parisey, M.; Wicky, P.-H.; Behillil, S.; Gaymard, A.; Bouscambert-Duchamp, M.; Donati, F.; Le Hingrat, Q.; et al. Clinical and virological data of the first cases of COVID-19 in Europe: A case series. Lancet Infect. Dis. 2020, 20, 697–706. [Google Scholar] [CrossRef] [Green Version]
- Dubé, E.; Laberge, C.; Guay, M.; Bramadat, P.; Roy, R.; Bettinger, J.A. Vaccine hesitancy: An overview. Hum. Vaccines Immunother. 2013, 9, 1763–1773. [Google Scholar] [CrossRef] [PubMed]
- Fine, P.; Eames, K.; Heymann, D.L. “Herd Immunity”: A Rough Guide. Clin. Infect. Dis. 2011, 52, 911–916. [Google Scholar] [CrossRef]
- Puri, N.; Coomes, E.A.; Haghbayan, H.; Gunaratne, K. Social Media and Vaccine Hesitancy: New Updates for the Era of COVID-19 and Globalized Infectious Diseases. Hum. Vaccines Immunother. 2020, 16, 2586–2593. [Google Scholar] [CrossRef] [PubMed]
- Larson, H.J.; Smith, D.M.D.; Paterson, P.; Cumming, M.; Eckersberger, E.; Freifeld, C.C.; Ghinai, I.; Jarrett, C.; Paushter, L.; Brownstein, J.S.; et al. Measuring Vaccine Confidence: Analysis of Data Obtained by a Media Surveillance System Used to Analyse Public Concerns about Vaccines. Lancet Infect. Dis. 2013, 13, 606–613. [Google Scholar] [CrossRef]
- Leib, S.; Liberatos, P.; Edwards, K. Pediatricians’ Experience with and Response to Parental Vaccine Safety Concerns and Vaccine Refusals: A Survey of Connecticut Pediatricians. Public Health Rep. 2011, 126 (Suppl. S2), 13–23. [Google Scholar] [CrossRef] [Green Version]
- Black, S.; Rappuoli, R. A Crisis of Public Confidence in Vaccines. Sci. Transl. Med. 2010, 2, 61mr1. [Google Scholar] [CrossRef] [PubMed]
- Wheeler, M.; Buttenheim, A.M. Parental Vaccine Concerns, Information Source, and Choice of Alternative Immunization Schedules. Hum. Vaccines Immunother. 2013, 9, 1782–1789. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spier, R. Perception of Risk of Vaccine Adverse Events: A Historical Perspective. Vaccine 2001, 20 (Suppl. S1), S78–S84. [Google Scholar] [CrossRef]
- Hussain, A.; Ali, S.; Ahmed, M.; Hussain, S. The Anti-Vaccination Movement: A Regression in Modern Medicine. Cureus 2018, 10, e2919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Camargo, K.R., Jr. Here we go again: The reemergence of anti-vaccine activism on the Internet. Cad. Saúde Pública 2020, 36, e00037620. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.; Wong, E.L.Y.; Ho, K.-F.; Cheung, A.W.L.; Yau, P.S.Y.; Dong, D.; Wong, S.Y.S.; Yeoh, E.-K. Change of willingness to accept COVID-19 vaccine and reasons of vaccine hesitancy of working people at different waves of local epidemic in Hong Kong, China: Repeated cross-sectional surveys. Vaccines 2021, 9, 62. [Google Scholar] [CrossRef] [PubMed]
- Kata, A. Anti-vaccine activists, Web 2.0, and the postmodern paradigm—an overview of tactics and tropes used online by the anti-vaccination movement. Vaccine 2012, 30, 3778–3789. [Google Scholar] [CrossRef]
- Ward, J.K.; Peretti-Watel, P.; Verger, P. Vaccine criticism on the Internet: Propositions for future research. Hum. Vaccines Immunother. 2016, 12, 1924–1929. [Google Scholar] [CrossRef] [Green Version]
- Davies, P.; Chapman, S.; Leask, J. Antivaccination Activists on the World Wide Web. Arch. Dis. Child. 2002, 87, 22–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ward, J.K.; Peretti-Watel, P.; Larson, H.J.; Raude, J.; Verger, P. Vaccine-Criticism on the Internet: New Insights Based on French-Speaking Websites. Vaccine 2015, 33, 1063–1070. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fu, L.Y.; Zook, K.; Spoehr-Labutta, Z.; Hu, P.; Joseph, J.G. Search Engine Ranking, Quality, and Content of Web Pages That Are Critical Versus Noncritical of Human Papillomavirus Vaccine. J. Adolesc. Health 2016, 58, 33–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fadda, M.; Allam, A.; Schulz, P.J. Arguments and Sources on Italian Online Forums on Childhood Vaccinations: Results of a Content Analysis. Vaccine 2015, 33, 7152–7159. [Google Scholar] [CrossRef] [PubMed]
- Uscinski, J.E.; Enders, A.M.; Klofstad, C.; Seelig, M.; Funchion, J.; Everett, C.; Wuchty, S.; Premaratne, K.; Murthi, M. Why Do People Believe COVID-19 Conspiracy Theories? Harvard Kennedy School Misinformation Review: Cambridge, MA, USA, 2020; Volume 1, pp. 1–12. [Google Scholar]
- Conner, M.; Norman, P. Predicting Health Behaviour; McGraw-Hill Education: London, UK, 2005. [Google Scholar]
- Maiman, L.A.; Becker, M.H. The health belief model: Origins and correlates in psychological theory. Health Educ. Monogr. 1974, 2, 336–353. [Google Scholar] [CrossRef]
- Donadiki, E.; Garcia, R.J.; Hernández-Barrera, V.; Sourtzi, P.; Carrasco-Garrido, P.; Lopez-De-Andres, A.; Jimenez-Trujillo, I.; Velonakis, E. Health Belief Model Applied to Non-Compliance with HPV Vaccine Among Female University Students. Public Health 2014, 128, 268–273. [Google Scholar] [CrossRef] [PubMed]
- Coe, A.B.; Gatewood, S.B.; Moczygemba, L.R. The use of the health belief model to assess predictors of intent to receive the novel (2009) H1N1 influenza vaccine. Innov. Pharm. 2012, 3, 1. [Google Scholar] [CrossRef] [PubMed]
- Cheney, M.K.; John, R. Underutilization of influenza vaccine: A test of the health belief model. Sage Open 2013, 3. [Google Scholar] [CrossRef] [Green Version]
- Palamenghi, L.; Barello, S.; Boccia, S.; Graffigna, G. Mistrust in Biomedical Research and Vaccine Hesitancy: The Forefront Challenge in the Battle against COVID-19 in Italy. Eur. J. Epidemiol. 2020, 35, 785–788. [Google Scholar] [CrossRef] [PubMed]
- Sanche, S.; Lin, Y.T.; Xu, C.; Romero-Severson, E.; Hengartner, N.; Ke, R. High Contagiousness and Rapid Spread of Severe Acute Respiratory Syndrome Coronavirus 2. Emerg. Infect. Dis. 2020, 26, 1470–1477. [Google Scholar] [CrossRef] [PubMed]
- Provenzi, L.; Barello, S. The science of the future: Establishing a citizen-scientist collaborative agenda after Covid-19. Front. Public Health 2020, 8, 6–8. [Google Scholar] [CrossRef]
- Expectations for a COVID-19 Vaccine. Associated Press-NORC Center for Public Affairs. May 2020. Available online: https://apnorc.org/projects/expectations-for-a-covid-19-vaccine/ (accessed on 30 July 2020).
- Miles, D.K.; Heald, A.H.; Stedman, M. How fast should social restrictions be eased in England as COVID-19 vaccinations are rolled out? Int. J. Clin. Pract. 2021, e14191. [Google Scholar] [CrossRef]
- Smith, G. Does Gender Influence Online Survey Participation? A Record-Linkage Analysis of University Faculty Online Survey Response Behavior; ERIC Document Reproduction Service No. ED 501717; San Jose State University: San Jose, CA, USA, 2008. [Google Scholar]
- Hawkins, J.; Kieffer, E.C.; Sinco, B.; Spencer, M.; Anderson, M.; Rosland, A.M. Does gender influence participation? Predictors of participation in a community health worker diabetes management intervention with African American and Latino adults. Diabetes Educ. 2013, 39, 647–654. [Google Scholar] [CrossRef] [Green Version]
- Canning, H.S.; Phillips, J.; Allsup, S. Health care worker beliefs about influenzavaccine and reasons for non-vaccination—A cross-sectional survey. J. Clin. Nurs. 2005, 14, 922–925. [Google Scholar] [CrossRef]
- Song, J.Y.; Park, C.W.; Jeong, H.W.; Cheong, H.J.; Kim, W.J.; Kim, S.R. Effect of a hospital campaign for influenza vaccination of healthcare workers. Infect. Control Hosp. Epidemiol. 2006, 27, 612–617. [Google Scholar] [CrossRef]
- Zimmerman, R.K.; Nowalk, M.P.; Lin, C.J.; Raymund, M.; Fox, D.E.; Harper, J.D.; Tanis, M.D.; Willis, B.C. Factorial design for improving influenza vaccination among employees of a large health system. Infect. Control Hosp. Epidemiol. 2009, 30, 691. [Google Scholar] [CrossRef]
- Polgreen, P.M.; Polgreen, L.A.; Evans, T.; Helms, C. A Statewide System for Improving Influenza Vaccination Rates in Hospital Employees. Infect. Control Hosp. Epidemiol. 2009, 30, 474–478. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dror, A.A.; Eisenbach, N.; Taiber, S.; Morozov, N.G.; Mizrachi, M.; Zigron, A.; Srouji, S.; Sela, E. Vaccine Hesitancy: The Next Challenge in the Fight Against COVID-19. Eur. J. Epidemiol. 2020, 35, 775–779. [Google Scholar] [CrossRef]
- Schmitt, H.-J.; Booy, R.; Aston, R.; Van Damme, P.; Schumacher, R.F.; Campins, M.; Rodrigo, C.; Heikkinen, T.; Weil-Olivier, C.; Finn, A.; et al. How to Optimise the Coverage Rate of Infant and Adult Immunisations in Europe. BMC Med. 2007, 5, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silva, G.; Majnarić Ljiljana, T.; Salha, T. Is virtual communication enough to save employed people young people from feeling of social isolation and loneliness? CPQ Neurol. Psychol. 2020, 3, 4. [Google Scholar]
- Kim, J.H.; Marks, F.; Clemens, J.D. Looking Beyond COVID-19 Vaccine Phase 3 Trials. Nat. Med. 2021, 27, 205–211. [Google Scholar] [CrossRef]
- Verbeke, R.; Lentacker, I.; De Smedt, S.C.; Dewitte, H. The Dawn of MRNA Vaccines: The COVID-19 Case. J. Control Release 2021, 333, 511–520. [Google Scholar] [CrossRef] [PubMed]
- Forni, G.; Mantovani, A. COVID-19 Vaccines: Where We Stand and Challenges Ahead. Cell Death Differ. 2021, 28, 626–639. [Google Scholar] [CrossRef] [PubMed]
- Mallapaty, S. China COVID vaccine reports mixed results - what does that mean for the pandemic? Nature 2021. [Google Scholar] [CrossRef]
- Moore, J.P.; Offit, P.A. SARS-CoV-2 vaccines and the growing threat of viral variants. JAMA 2021, 325, 821–822. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Schmidt, F.; Weisblum, Y.; Muecksch, F.; Barnes, C.O.; Finkin, S.; Schaefer-Babajew, D.; Cipolla, M.; Gaebler, C.; Lieberman, J.A.; et al. mRNA vaccine-elicited antibodies to SARS-CoV-2 and circulating variants. bioRxiv 2021, preprint. [Google Scholar]
- Ngiam, J.N.; Chew, N.; Tham, S.M.; Beh, D.L.-L.; Lim, Z.Y.; Li, T.Y.; Cen, S.; Tambyah, P.A.; Santosa, A.; Sia, C.-H.; et al. Demographic Shift in COVID-19 Patients in Singapore from an Aged, at-Risk Population to Young Migrant Workers with Reduced Risk of Severe Disease. Int. J. Infect. Dis. 2021, 103, 329–335. [Google Scholar] [CrossRef]
- Mitchell, W.B.; Davila, J.; Keenan, J.; Jackson, J.; Tal, A.; Morrone, K.A.; Silver, E.J.; O’Brien, S.; Manwani, D. Children and Young Adults Hospitalized for Severe COVID-19 Exhibit Thrombotic Coagulopathy. Pediatr. Blood Cancer 2021, 68, e28975. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Huang, Z.; Wang, M.; Tang, K.; Wang, S.; Gao, P.; Xie, J.; Wang, T.; Zhao, J. Clinical Characteristics and Predictors of Mortality in Young Adults with Severe COVID-19: A Retrospective Observational Study. Ann. Clin. Microbiol. Antimicrob. 2021, 20, 1–9. [Google Scholar] [CrossRef]
- Bhavsar, S.M.; Clouser, K.N.; Gadhavi, J.; Anene, O.; Kaur, R.; Lewis, R.; Naganathan, S.; Michalak, Z.; Chen, C.Q.; Shah, P.; et al. COVID-19 in Pediatrics: Characteristics of Hospitalized Children in New Jersey. Hosp. Pediatr. 2021, 11, 79–87. [Google Scholar] [CrossRef]
- Sallam, M. COVID-19 Vaccine Hesitancy Worldwide: A Concise Systematic Review of Vaccine Acceptance Rates. Vaccines 2021, 9, 160. [Google Scholar] [CrossRef] [PubMed]
- Sarasty, O.; Carpio, C.E.; Hudson, D.; Guerrero-Ochoa, P.A.; Borja, I. The Demand for a COVID-19 Vaccine in Ecuador. Vaccine 2020, 38, 8090–8098. [Google Scholar] [CrossRef]
- Wong, L.P.; Alias, H.; Wong, P.F.; Lee, H.Y.; AbuBakar, S. The use of the health belief model to assess predictors of intent to receive the COVID-19 vaccine and willingness to pay. Hum. Vaccines Immunother. 2020, 16, 2204–2214. [Google Scholar] [CrossRef]
- Harapan, H.; Wagner, A.L.; Yufika, A.; Winardi, W.; Anwar, S.; Gan, A.K.; Setiawan, A.M.; Rajamoorthy, Y.; Sofyan, H.; Mudatsir, M. Acceptance of a COVID-19 Vaccine in Southeast Asia: A Cross-Sectional Study in Indonesia. Front. Public Health 2020, 8, 381. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Jing, R.; Lai, X.; Zhang, H.; Lyu, Y.; Knoll, M.D.; Fang, H. Acceptance of COVID-19 Vaccination During the COVID-19 Pandemic in China. Vaccines 2020, 8, 482. [Google Scholar] [CrossRef] [PubMed]
- Sallam, M.; Dababseh, D.; Eid, H.; Al-Mahzoum, K.; Al-Haidar, A.; Taim, D.; Yaseen, A.; Ababneh, N.A.; Bakri, F.G.; Mahafzah, A. High Rates of COVID-19 Vaccine Hesitancy and Its Association with Conspiracy Beliefs: A Study in Jordan and Kuwait Among Other Arab Countries. Vaccines 2021, 9, 42. [Google Scholar] [CrossRef] [PubMed]
- La Vecchia, C.; Negri, E.; Alicandro, G.; Scarpino, V. Attitudes towards Influenza Vaccine and a Potential COVID-19 Vaccine in Italy and Differences across Occupational Groups, September 2020. Med. Lav. 2020, 111, 445–448. [Google Scholar] [PubMed]
- Lazarus, J.V.; Ratzan, S.C.; Palayew, A.; Gostin, L.O.; Larson, H.J.; Rabin, K.; Kimball, S.; El-Mohandes, A. A global survey of potential acceptance of a COVID-19 vaccine. Nat. Med. 2020, 27, 225–228. [Google Scholar] [CrossRef]
- Fisher, K.A.; Bloomstone, S.J.; Walder, J.; Crawford, S.; Fouayzi, H.; Mazor, K.M. Attitudes toward a potential SARS-CoV-2 vaccine: A survey of US adults. Ann. Intern. Med. 2020, 173, 964–973. [Google Scholar] [CrossRef]
- Loomba, S.; de Figueiredo, A.; Piatek, S.J.; de Graaf, K.; Larson, H.J. Measuring the impact of COVID-19 vaccine misinformation on vaccination intent in the UK and USA. Nat. Hum. Behav. 2021, 5, 337–348. [Google Scholar] [CrossRef] [PubMed]
- Nzaji, M.K.; Ngombe, L.K.; Mwamba, G.N.; Ndala, D.B.B.; Miema, J.M.; Luhata Lungoyo, C.; Lora Mwimba, B.; Cikomola Mwana Bene, A.; Mukamba Musenga, E. Acceptability of Vaccination Against COVID-19 Among Healthcare Workers in the Democratic Republic of the Congo. Pragmatic Obs. Res. 2020, 11, 103. [Google Scholar] [CrossRef]
- Fu, C.; Wei, Z.; Pei, S.; Li, S.; Sun, X.; Liu, P. Acceptance and preference for COVID-19 vaccination in health-care workers (HCWs). medRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Hertwig, R.; Grüne-Yanoff, T. Nudging and Boosting: Steering or Empowering Good Decisions. Perspect. Psychol. Sci. 2017, 12, 973–986. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lurie, N.; Saville, M.; Hatchett, R.; Halton, J. Developing Covid-19 Vaccines at Pandemic Speed. N. Engl. J. Med. 2020, 382, 1969–1973. [Google Scholar] [CrossRef] [PubMed]
- Danchin, M.; Biezen, R.; Manski-Nankervis, J.-A.; Kaufman, J.; Leask, J. Preparing the Public for COVID-19 Vaccines: How Can General Practitioners Build Vaccine Confidence and Optimise Uptake for Themselves and Their Patients? Aust. J. Gen. Pr. 2020, 49, 625–629. [Google Scholar] [CrossRef]
- World Health Organisation (WHO). Coronavirus Disease (COVID-19). COVID-19 Vaccine. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/covid-19-vaccines (accessed on 25 May 2021).
- Jeanrenaud, L.; Mariniello, M.; Wolff, G.B. What Do Vaccination Passports Mean for Europe? Bruegel-Blogs. Available online: https://www.bruegel.org/2021/01/what-do-vaccination-passports-mean-for-europe/ (accessed on 25 May 2021).




{kind=link}
{kind=link}
{kind=link}
| Frequency | Percentage (%) | |
|---|---|---|
| Age: | ||
| 20–40 | 145 | 52.5 |
| 40–60 | 62 | 22.5 |
| >60 | 69 | 25.0 |
| Sex: | ||
| Male | 56 | 20.3 |
| Female | 220 | 79.7 |
| Employment status: | ||
| Health care worker | 95 | 34.4 |
| Non-health care worker | 111 | 40.2 |
| Unemployed | 28 | 10.1 |
| Retired | 42 | 15.2 |
| Household status: | ||
| Living alone | 81 | 29.3 |
| With a partner, no children | 68 | 24.6 |
| With a partner and minor children | 85 | 30.8 |
| With a partner and adult children | 31 | 11.2 |
| With children, no partner | 11 | 4.0 |
| Group | z-Value | OR * | p-Value † | CI ‡ | |
|---|---|---|---|---|---|
| 5% | 95% | ||||
| <40 years of age | 3.977 | 2.845 | <0.001 | 1.7 | 4.763 |
| >40 years of age | 3.977 | 0.352 | <0.001 | 0.21 | 0.588 |
| Healthcare worker | 2.202 | 0.560 | 0.028 | 0.334 | 0.938 |
| Non-healthcare worker | 2.202 | 1.786 | 0.028 | 1.066 | 2.992 |
| Male < 40 years of age | 0.957 | 1.7460 | 0.3387 | 0.558 | 5.469 |
| Male > 40 years of age | 0.957 | 0.5727 | 0.3387 | 0.183 | 1.794 |
| Female < 40 years of age | 3.98 | 3.241 | <0.001 | 3.98 | 5.782 |
| Female > 40 years of age | 3.98 | 0.309 | <0.001 | 0.173 | 0.551 |
| Coefficient | Standard Error | t-Test | p-Value * | R2 | |
|---|---|---|---|---|---|
| Constant | 1.167 | 0.039 | 29.730 | <0.001 | |
| Do you feel prone to getting sick? | 0.078 | 0.034 | 2.296 | 0.022 | 0.060 |
| If you become infected, do you think consequences could be severe? | 0.118 | 0.043 | 2.720 | 0.007 | 0.068 |
| Do you have any chronic diseases? | −0.154 | 0.051 | −3.047 | 0.003 | 0.013 |
| Do you get vaccinated against flu regularly? | 0.125 | 0.096 | 1.300 | 0.195 | 0.089 |
| Did you get this year’s flu vaccine? | 0.301 | 0.099 | 3.052 | 0.002 | 0.109 |
| Coefficient | Standard Error | t-Test | p-Value * | R2 | |
|---|---|---|---|---|---|
| Constant | 0.480 | 0.140 | 3.415 | 0.001 | |
| I don’t think I’m going to get sick even if I don’t get vaccinated. | 0.031 | 0.036 | 0.857 | 0.392 | 0.117 |
| I was already COVID-19 positive, so I will definitely not be positive again. | 0.018 | 0.038 | 0.490 | 0.624 | 0.037 |
| When the vaccine stops the pandemic, I won’t need to be vaccinated. | 0.079 | 0.039 | 2.041 | 0.042 | 0.130 |
| I don’t expect severe symptoms so there is no need to get the vaccine. | 0.131 | 0.039 | 3.321 | 0.001 | 0.203 |
| I don’t want to waste time on vaccination, I have more important worries. | −0.007 | 0.040 | −0.176 | 0.861 | 0.085 |
| I don’t care if I get sick. | −0.079 | 0.051 | −1.547 | 0.123 | 0.026 |
| I will not be vaccinated—it will be as it must be. | 0.208 | 0.036 | 5.749 | <0.001 | 0.262 |
| Coefficient | Standard Error | t-Test | p-Value * | R2 | |
|---|---|---|---|---|---|
| Constant | 1.784 | 0.115 | 15.524 | <0.001 | |
| I believe in the effectiveness of the vaccine. | −0.034 | 0.041 | −0.811 | 0.418 | 0.214 |
| I am afraid of the side effects of the vaccine. | 0.048 | 0.029 | 1.684 | 0.093 | 0.077 |
| I think the vaccine will protect me from getting sick. | −0.132 | 0.041 | −3.220 | 0.001 | 0.247 |
| I am not sufficiently informed about the vaccine. | 0.089 | 0.028 | 3.190 | 0.002 | 0.104 |
| I think COVID−19 vaccine is safe. | −0.171 | 0.039 | −4.358 | <0.001 | 0.288 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guljaš, S.; Bosnić, Z.; Salha, T.; Berecki, M.; Krivdić Dupan, Z.; Rudan, S.; Majnarić Trtica, L. Lack of Informations about COVID-19 Vaccine: From Implications to Intervention for Supporting Public Health Communications in COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 6141. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18116141
Guljaš S, Bosnić Z, Salha T, Berecki M, Krivdić Dupan Z, Rudan S, Majnarić Trtica L. Lack of Informations about COVID-19 Vaccine: From Implications to Intervention for Supporting Public Health Communications in COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2021; 18(11):6141. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18116141
Chicago/Turabian StyleGuljaš, Silva, Zvonimir Bosnić, Tamer Salha, Monika Berecki, Zdravka Krivdić Dupan, Stjepan Rudan, and Ljiljana Majnarić Trtica. 2021. "Lack of Informations about COVID-19 Vaccine: From Implications to Intervention for Supporting Public Health Communications in COVID-19 Pandemic" International Journal of Environmental Research and Public Health 18, no. 11: 6141. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18116141