
A Mixed Methods Exploration of Surf Therapy Piloted for Youth Well-Being in Post-Conflict Sierra Leone

 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Surf Therapy in Sierra Leone; The Wave Alliance
2.2. Sample Characteristics
2.3. Mixed Methods Evaluation: Phase 1—Quantitative Analysis
2.4. Mixed Methods Evaluation: Phase 2—Qualitative Analysis
2.5. Mixed Methods Evaluation: Phase 3—Comparative Analysis
3. Results
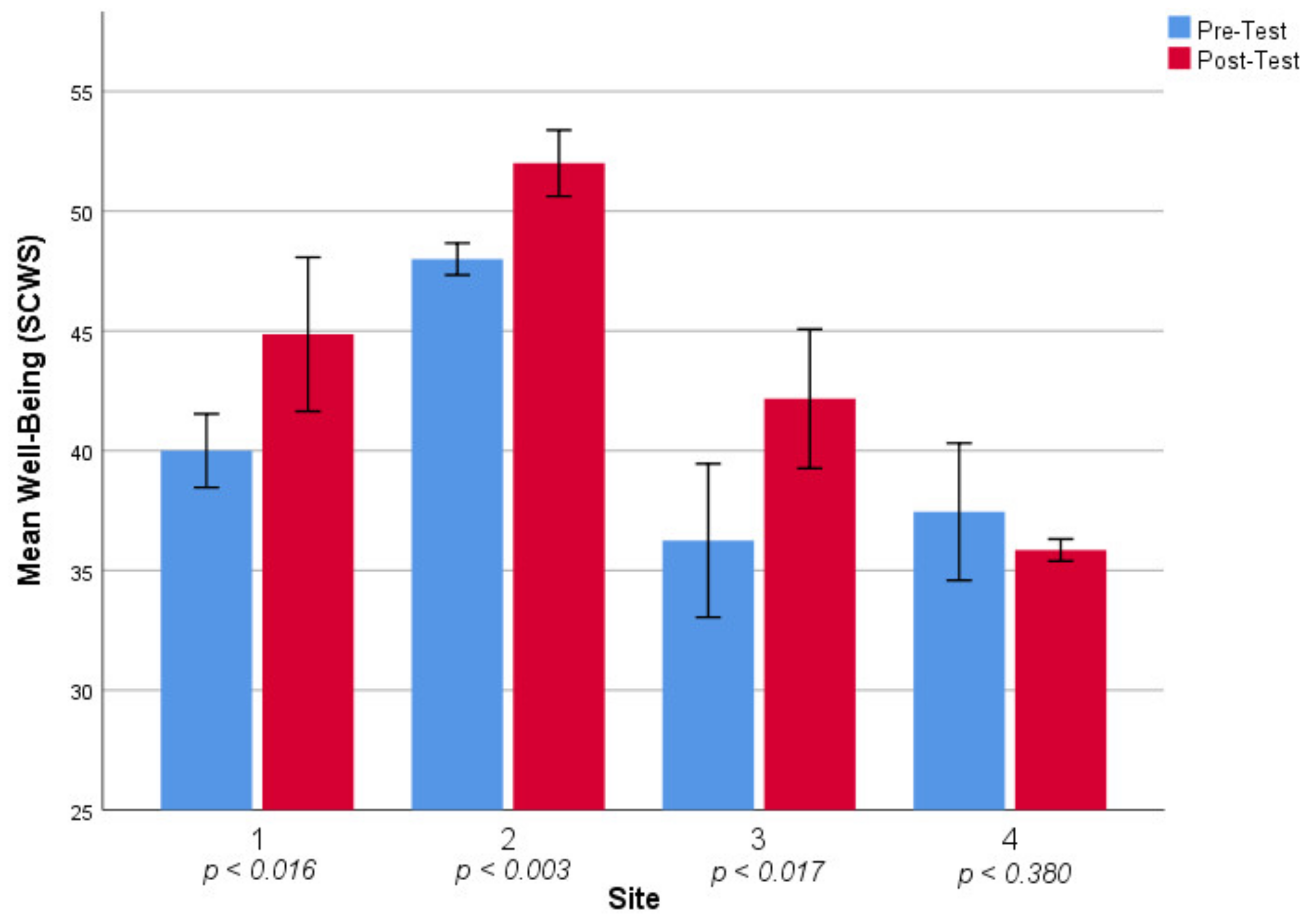
3.1. Phase 1—Statistical Analysis of Well-Being Data
3.2. Phase 2—Evaluation Synthesis
3.3. Phase 3—Comparative Analysis
4. Discussion and Implications
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Links to Surf Therapy Pilot Evaluations
References
- Attanayake, V.; McKay, R.; Joffres, M.; Singh, S.; Burkle, F., Jr.; Mills, E. Prevalence of mental disorders among children exposed to war: A systematic review of 7920 children. Med. Confl. Surviv. 2009, 25, 4–19. [Google Scholar] [CrossRef]
- Betancourt, T.S.; McBain, R.K.; Newnham, E.A.; Brennan, R.T. The intergenerational impact of war: Longitudinal relationships between caregiver and child mental health in postconflict Sierra Leone. J. Child Psychol. Psychiatry 2015, 56, 1101–1107. [Google Scholar] [CrossRef]
- Coalition to Stop the Use of Child Soldiers (CSUCS). Global Report 2008. 2008. Available online: https://reliefweb.int/sites/reliefweb.int/files/resources/67012B7F8EB991888525744F0069863A-Child%20Soldiers%20Global%20Report%202008.pdf (accessed on 2 February 2021).
- World Health Organization. Ebola Situation Report—20 January 2016. 2016. Available online: https://apps.who.int/ebola/current-situation/ebola-situation-report-20-january-2016 (accessed on 5 February 2021).
- Bah, A.J.; James, P.B.; Bah, N.; Sesay, A.B.; Sevalie, S.; Kanu, J.S. Prevalence of anxiety, depression and post-traumatic stress disorder among Ebola survivors in northern Sierra Leone: A cross-sectional study. BMC Public Health 2020, 20, 1391. [Google Scholar] [CrossRef]
- Betancourt, T.S.; Newnham, E.A.; Hann, K.; McBain, R.K.; Akinsulure-Smith, A.M.; Weisz, J.; Lilienthal, G.M.; Hansen, N. Addressing the Consequences of Violence and Adversity: The Development of a Group Mental Health Intervention for War-Affected Youth in Sierra Leone. 2014. Available online: https://academicworks.cuny.edu/cgi/viewcontent.cgi?article=1420&context=cc_pubs (accessed on 5 February 2021).
- Whitley, M.A.; Massey, W.V.; Camiré, M.; Blom, L.C.; Chawansky, M.; Forde, S.; Boutet, M.; Borbee, A.; Darnell, S.C. A systematic review of sport for development interventions across six global cities. Sport Manag. Rev. 2019, 22, 181–193. [Google Scholar] [CrossRef]
- Whitley, M.A.; Massey, W.V.; Camiré, M.; Boutet, M.; Borbee, A. Sport-based youth development interventions in the United States: A systematic review. BMC Public Health 2019, 19, 89. [Google Scholar] [CrossRef]
- Hamilton, A.; Foster, C.; Richards, J. A systematic review of the mental health impacts of sport and physical activity programmes for adolescents in post-conflict settings. J. Sport Dev. 2016, 4, 44–59. [Google Scholar]
- Benninger, E.; Curtis, C.; Sarkisian, G.V.; Rogers, C.M.; Bender, K.; Comer, M. Surf therapy: A scoping review of the qualitative and quantitative research evidence. Glob. J. Community Psychol. Pract. 2020, 11, 1–26. [Google Scholar]
- Marshall, J.; Ferrier, B.; Ward, P.B.; Martindale, R. I feel happy when I surf because it takes stress from my mind: An Initial Exploration of Program Theory within Waves for Change Surf Therapy in Post-Conflict Liberia. J. Sport Dev. 2020, 9, 1–17. [Google Scholar]
- Marshall, J.; Kelly, P.; Niven, A. When I Go There, I Feel Like I Can Be Myself. Exploring Programme Theory within the Wave Project Surf Therapy Intervention. Int. J. Environ. Res. Public Health 2019, 16, 2159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liddle, I.; Carter, G.F. Emotional and psychological well-being in children: The development and validation of the Stirling Children’s Well-being Scale. Educ. Psychol. Pract. 2015, 31, 174–185. [Google Scholar] [CrossRef]
- Begley, C.M. Using triangulation in nursing research. J. Adv. Nurs. 1996, 24, 122–128. [Google Scholar] [CrossRef]
- Evans, D. Systematic reviews of interpretive research: Interpretive data synthesis of processed data. Aust. J. Adv. Nurs. 2002, 20, 22–26. [Google Scholar] [PubMed]
- Hill, A.B. The Environment and Disease: Association or Causation? Proc. R. Soc. Med. 1965, 58, 295–300. [Google Scholar] [CrossRef] [Green Version]
- Richards, J.; Jiang, X.; Kelly, P.; Chau, J.; Bauman, A.; Ding, D. Don’t worry, be happy: Cross-sectional associations between physical activity and happiness in 15 European countries. BMC Public Health 2015, 15, 53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hansen, D.M.; Larson, R.W. Amplifiers of developmental and negative experiences in organized activities: Dosage, motivation, lead roles, and adult-youth ratios. J. Appl. Dev. Psychol. 2007, 28, 360–374. [Google Scholar] [CrossRef]
- Borgonovo-Santos, M.; Zacca, R.; Fernandes, R.J.; Vilas-Boas, J.P. The impact of a single surfing paddling cycle on fatigue and energy cost. Sci. Rep. 2021, 11, 4566. [Google Scholar] [CrossRef] [PubMed]
- Miller, L.; Alele, F.O.; Emeto, T.I.; Franklin, R.C. Epidemiology, risk factors and measures for preventing drowning in Africa: A systematic review. Medicina 2019, 55, 637. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whitley, M.A.; Farrell, K.; Wolff, E.A.; Hillyer, S.J. Sport for development and peace: Surveying actors in the field. J. Sport Dev. 2019, 7, 1–15. [Google Scholar]
- Pierce, S.; Gould, D.; Camiré, M. Definition and model of life skills transfer. Int. Rev. Sport Exerc. Psychol. 2017, 10, 186–211. [Google Scholar] [CrossRef]
- Britton, E.; Kindermann, G.; Domegan, C.; Carlin, C. Blue care: A systematic review of blue space interventions for health and wellbeing. Health Promot. Int. 2020, 35, 50–69. [Google Scholar] [CrossRef] [Green Version]
- Hollifield, M.; Warner, T.D.; Lian, N.; Krakow, B.; Jenkins, J.H.; Kesler, J.; Stevenson, J.; Westermeyer, J. Measuring trauma and health status in refugees: A critical review. JAMA 2002, 288, 611–621. [Google Scholar] [CrossRef] [PubMed]
- Betancourt, T.S.; Bass, J.; Borisova, I.; Neugebauer, R.; Speelman, L.; Onyango, G.; Bolton, P. Assessing local instrument reliability and validity: A field-based example from northern Uganda. Soc. Psychiatry Psychiatr. Epidemiol. 2009, 44, 685–692. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Site Number | Organization | n | Average Age | Age Range | Average Attendance | Male | Female |
|---|---|---|---|---|---|---|---|
| na | Pooled National Data | 58 | 12.9 | 7–22 | 57.20% | 35 | 23 |
| 1 | Moseray Fadika Trust | 14 | 13.3 | 9–20 | 89.30% | 2 | 10 |
| 2 | Young Leaders Sierra Leone | 12 | 15.1 | 11–18 | 59.50% | 12 | 0 |
| 3 | United Sierra Leone | 12 | 12.3 | 7–16 | 58.30% | 11 | 3 |
| 4 | Pipul Pikin Foundation | 20 | 11.7 | 8–22 | 37.20% | 10 | 10 |
| Site | Z | Asymp. Sig (p) | Effect Size (r) |
|---|---|---|---|
| 1 | −2.415 | 0.016 | 0.65 |
| 2 | −2.944 | 0.003 | 0.84 |
| 3 | −2.395 | 0.017 | 0.69 |
| 4 | −0.877 | 0.380 | −0.22 |
| Intervention Site | Reported Qualitative Impact | Plausible Mechanisms Reported | Challenges Reported |
|---|---|---|---|
| 1 | Feeling calmer, Improved socializing | New positive relationships, Respite from stress, Alternative to negative activities | Perceptions around water safety, Need for food within program, Lack of disability access, Transport to program |
| 2 | Improved academic attendance, Behavioral improvements | Peer support from other surfers, Positive social relationships | Perceptions around water safety, Need for food within program, Lack of female participation, Transport to program |
| 3 | Improved socializing, Reduction in bad behaviors, Academic performance | Peer support from coaches, Safe space, Coping skills | Perceptions around water safety, Need for food within program, Accessibility to younger (<8) participants |
| 4 | Improved mindset, Improved academic effort | Coping skills, Safe Space | Consistency of delivery, Low attendance, Change of location, Change of lead coaches, Perceptions around water safety, Need for food within program |
| 5 | Improved socializing, Reduction in bad behaviors | Respite, Peer support from coaches, Increased physical activity | Evaluation confusion, Perceptions around program aims |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marshall, J.; Kamuskay, S.; Samai, M.M.; Marah, I.; Tonkara, F.; Conteh, J.; Keita, S.; Jalloh, O.; Missalie, M.; Bangura, M.; et al. A Mixed Methods Exploration of Surf Therapy Piloted for Youth Well-Being in Post-Conflict Sierra Leone. Int. J. Environ. Res. Public Health 2021, 18, 6267. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18126267
Marshall J, Kamuskay S, Samai MM, Marah I, Tonkara F, Conteh J, Keita S, Jalloh O, Missalie M, Bangura M, et al. A Mixed Methods Exploration of Surf Therapy Piloted for Youth Well-Being in Post-Conflict Sierra Leone. International Journal of Environmental Research and Public Health. 2021; 18(12):6267. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18126267
Chicago/Turabian StyleMarshall, Jamie, Sallu Kamuskay, Michaella Margaedah Samai, Isha Marah, Fanta Tonkara, Josephine Conteh, Sullayman Keita, Oullematu Jalloh, Mohamed Missalie, Mohamed Bangura, and et al. 2021. "A Mixed Methods Exploration of Surf Therapy Piloted for Youth Well-Being in Post-Conflict Sierra Leone" International Journal of Environmental Research and Public Health 18, no. 12: 6267. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18126267