
An Integrated Approach to Hygiene, Sanitation, and Storage Practices for Improving Microbial Quality of Drinking Water Treated at Point of Use: A Case Study in Makwane Village, South Africa


Abstract
:1. Introduction
2. Materials and Methods
2.1. Description of the Study Area
2.2. Ethical Clearance
2.3. Study Survey
2.4. Water Quality Analysis
2.4.1. Genomic DNA Extraction
2.4.2. Molecular Identification of E. coli
2.4.3. Molecular Identification of Salmonella, Shigella, and V. cholerae
2.5. Statistical Analysis
3. Results
3.1. Socio-Demographic Information of the Study Area
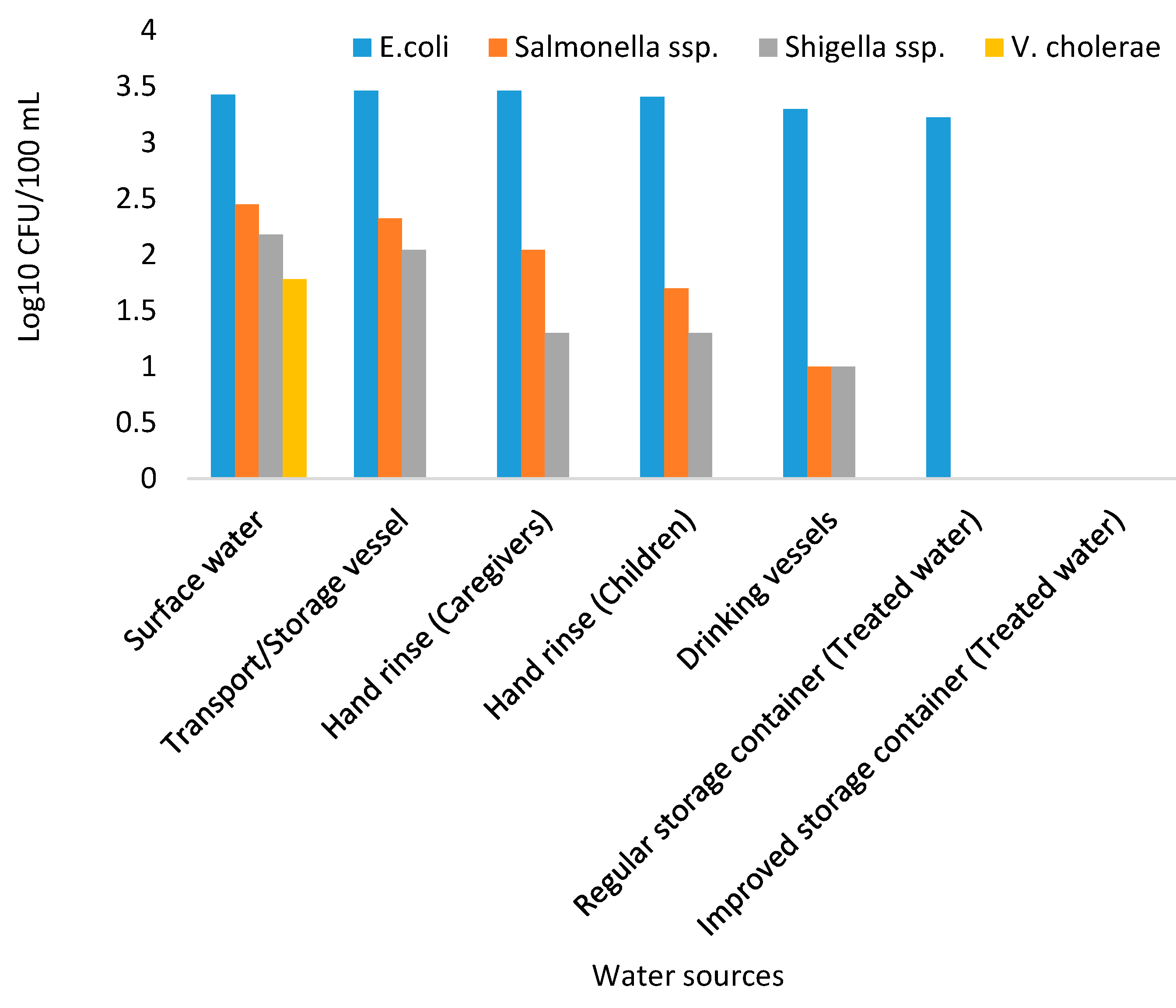
3.2. Overall Bacteriological Quality of Makwane Households’ Drinking Water
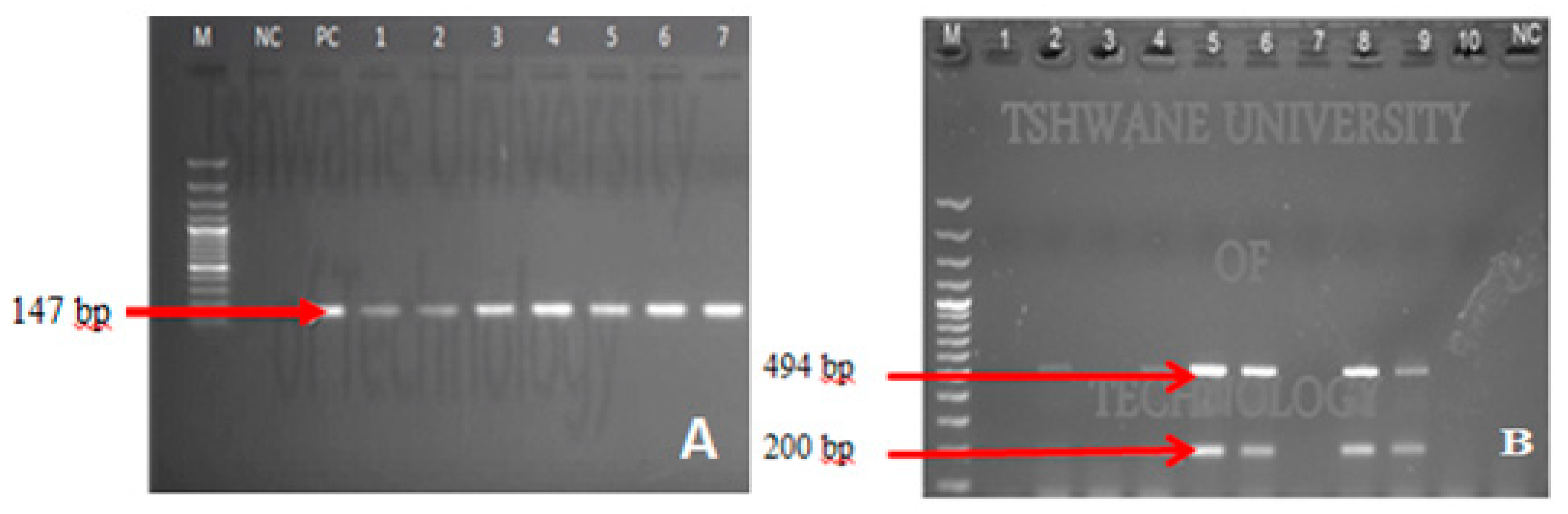
3.3. Confirmation of Enteropathogenic Bacteria by PCR
3.4. Geometric Mean Concentration of Presumptive E. coli in Treated Water Stored in Regular Containers Relative to Socio-Demographic Characteristics
3.5. Relationship between Demographic Information and Water Quality in Terms of E. coli Mean Concetration in Treated Water Stored in Regular Containers
4. Discussion
The Relevance of the Obtained Findings to the Current Situation
5. Conclusions and Recommendations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- UNICEF; WHO. Progresos en Materia de Agua Potable, Saneamiento e Higiene: Atención Especial a las Desigualdades, 2000–2017; UNICEF: New York, NY, USA; WHO: Geneva, Switzerland, 2019; p. 140. [Google Scholar]
- Prüss-Ustün, A.; Wolf, J.; Bartram, J.; Clasen, T.; Cumming, O.; Freeman, M.C.; Gordon, B.; Hunter, P.R.; Medlicott, K.; Johnston, R. Burden of disease from inadequate water, sanitation and hygiene for selected adverse health outcomes: An updated analysis with a focus on low-and middle-income countries. Int. J. Hyg. Environ. Health 2019, 222, 765–777. [Google Scholar] [CrossRef] [PubMed]
- UNICEF. UNICEF Data: Monitoring the Situation of Children and Woman, UNICEF Updates, February 2017; UNICEF: Geneva, Switzerland, 2017. [Google Scholar]
- UNICEF. One Is Too Many: Ending Child Deaths from Pneumonia and Diarrhoea; ©UNICEF/UNI193975/Mackenzie: New York, NY, USA, 2016. [Google Scholar]
- Chola, L.; Michalow, J.; Tugendhaft, A.; Hofman, K. Reducing diarrhoea deaths in South Africa: Costs and effects of scaling up essential interventions to prevent and treat diarrhoea in under-five children. BMC Public Health 2015, 15, 394. [Google Scholar] [CrossRef] [Green Version]
- WHO. Cholera: Global Surveillance Summary; Weekly Epidemiological Record; 2009; Available online: http://www.who.int/wer/2010/wer8531.pdf (accessed on 21 April 2021).
- Ogunyemi, O.; Onigbogi, O. Effect of Storage Containers on Quality of Household Drinking Water in Urban Communities in Ibadan, Nigeria. Int. J. Public Health Sci. 2014, 3. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention (CDC). Safe water systems for the developing world: A handbook for implementing household-based water treatment and safe storage projects. In Safe Water Systems for the Developing World: A Handbook for Implementing Household-Based Water Treatment and Safe Storage Projects; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2001. Available online: http://www.cdc.gov/safewater/manual/swsmanual.pdf (accessed on 21 April 2021).
- UNICEF. Promotion of Household Water Treatment and Safe Storage in UNICEF WASH Programmes; UNICEF: New York, NY, USA, 2008. [Google Scholar]
- Subbaraman, R.; Shitole, S.; Shitole, T.; Sawant, K.; O’brien, J.; Bloom, D.E.; Patil-Deshmukh, A. The social ecology of water in a Mumbai slum: Failures in water quality, quantity, and reliability. BMC Public Health 2013, 13, 173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, J.M.; Proum, S.; Sobsey, M.D. Escherichia coli in household drinking water and diarrhoeal disease risk: Evidence from Cambodia. Water Sci. Technol. 2008, 58, 757–763. [Google Scholar] [CrossRef]
- Levy, K.; Nelson, K.L.; Hubbard, A.; Eisenberg, J.N.S. Following the water: A controlled study of drinking water storage in northern coastal Ecuador. Environ. Health Perspect. 2008, 116, 1533–1540. [Google Scholar] [CrossRef] [PubMed]
- Sobsey, M.D.; Stauber, C.E.; Casanova, L.M.; Brown, J.M.; Elliott, M.A. Point of use household drinking water filtration: A practical, effective solution for providing sustained access to safe drinking water in the developing world. Environ. Sci. Technol. 2008, 42, 4261–4267. [Google Scholar] [CrossRef] [PubMed]
- Pickering, A.J.; Julian, T.R.; Mamuya, S.; Boehm, A.B.; Davis, J. Bacterial hand contamination among Tanzanian mothers varies temporally and following household activities. Trop. Med. Int. Health 2011, 16, 233–239. [Google Scholar] [CrossRef]
- Potgieter, N.; Becker, P.J.; Ehlers, M.M. Evaluation of the CDC safe water-storage intervention to improve the microbiological quality of point-of-use drinking water in rural communities in South Africa. Water SA 2009, 35. [Google Scholar] [CrossRef] [Green Version]
- VanDerslice, J.; Briscoe, J. Environmental interventions in developing countries: Interactions and their implications. Am. J. Epidemiol. 1995, 141, 135–144. [Google Scholar] [CrossRef]
- Curtis, V.; Cairncross, S. Effect of washing hands with soap on diarrhoea risk in the community: A systematic review. Lancet Infect. Dis. 2003, 3, 275–281. [Google Scholar] [CrossRef]
- Luby, S.P.; Agboatwalla, M.; Painter, J.; Altaf, A.; Billhimer, W.L.; Hoekstra, R.M. Effect of intensive handwashing promotion on childhood diarrhoea in high-risk communities in Pakistan: A randomized controlled trial. JAMA 2004, 291, 2547–2554. [Google Scholar] [CrossRef] [PubMed]
- Cairncross, S.; Shordt, K.; Zacharia, S.; Govindan, B.K. What causes sustainable changes in hygiene behaviour? A cross-sectional study from Kerala, India. Soc. Sci. Med. 2005, 61, 2212–2220. [Google Scholar] [CrossRef]
- Moropeng, R.; Budeli, P.; Mpenyana-Monyatsi, L.; Momba, M. Dramatic Reduction in Diarrhoeal Diseases through Implementation of Cost-Effective Household Drinking Water Treatment Systems in Makwane Village, Limpopo Province, South Africa. Int. J. Environ. Res. Public Health 2018, 15, 410. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsai, Y.-L.; Palmer, C.J.; Sangermano, L.R. Detection of Escherichia coli in sewage and sludge by polymerase chain reaction. Appl. Environ. Microbiol. 1993, 59, 353–357. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Cao, B.; Liu, B.; Liu, D.; Gao, Q.; Peng, X.; Wu, J.; Bastin, D.A.; Feng, L.; Wang, L. Molecular detection of all 34 distinct O-antigen forms of Shigella. J. Med. Microbiol. 2009, 58, 69–81. [Google Scholar] [CrossRef]
- Kong, R.Y.C.; Lee, S.K.Y.; Law, T.W.F.; Law, S.H.W.; Wu, R.S.S. Rapid detection of six types of bacterial pathogens in marine waters by multiplex PCR. Water Res. 2002, 36, 2802–2812. [Google Scholar] [CrossRef]
- Hossain, M.T.; Kim, E.; Kim, Y.; Kim, D.; Kong, I. Development of a groEL gene–based species-specific multiplex polymerase chain reaction assay for simultaneous detection of Vibrio cholerae, Vibrio parahaemolyticus and Vibrio vulnificus. J. Appl. Microbiol. 2013, 114, 448–456. [Google Scholar] [CrossRef]
- WHO; UNICEF; JMP. Joint Monitoring Programme (JMP) for Water Supply and Sanitation 2015. Progress on Sanitation and Drinking Water—2015 Update and MDG Assessment; UNICEF: New York, NY, USA; WHO: Geneva, Switzerland, 2015. [Google Scholar]
- Liu, L.; Johnson, H.L.; Cousens, S.; Perin, J.; Scott, S.; Lawn, J.E.; Rudan, I.; Campbell, H.; Cibulskis, R.; Li, M. Global, regional, and national causes of child mortality: An updated systematic analysis for 2010 with time trends since 2000. Lancet 2012, 379, 2151–2161. [Google Scholar] [CrossRef]
- WHO. Guidelines for Drinking-Water Quality, 4th ed.; WHO: Geneva, Switzerland, 2012. [Google Scholar]
- DWAF. Water and Sanitation Coverage in South Africa. Pretoria, South Africa: Government Printer; DWAF: Pretoria, South Africa, 2008. [Google Scholar]
- Singh, U.; Lutchmanariyan, R.; Wright, J.; Knight, S.; Jackson, S.; Langmark, J.; Vosloo, D.; Rodda, N. Microbial quality of drinking water from groundtanks and tankers at source and point-of-use in eThekwini Municipality, South Africa, and its relationship to health outcomes. Water SA 2013, 39, 663–674. [Google Scholar] [CrossRef] [Green Version]
- Deb, B.C.; Sircar, B.K.; Sengupta, P.G.; De, S.P.; Mondal, S.K.; Gupta, D.N.; Saha, N.C.; Ghosh, S.; Mitra, U.; Pal, S.C. Studies on interventions to prevent eltor cholera transmission in urban slums. Bull. World Health Organ. 1986, 64, 127. [Google Scholar] [PubMed]
- Qadri, M.H.; Al-Ghamdi, M.A.; Musharaf, A.Y.; Haq, M.I. A study on diarrhoeal diseases in children under five years of age. Ann. Saudi Med. 1992, 12, 459–462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trevett, A.F.; Carter, R.C.; Tyrrel, S.F. Water quality deterioration: A study of household drinking water quality in rural Honduras. Int. J. Environ. Health Res. 2004, 14, 273–283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fewtrell, L.; Kaufmann, R.B.; Kay, D.; Enanoria, W.; Haller, L.; Colford, J.M., Jr. Water, sanitation, and hygiene interventions to reduce diarrhoea in less developed countries: A systematic review and meta-analysis. Lancet Infect. Dis. 2005, 5, 42–52. [Google Scholar] [CrossRef]
- Trevett, A.F.; Carter, R.C.; Tyrrel, S.F. The importance of domestic water quality management in the context of faecal–oral disease transmission. J. Water Health 2005, 3, 259–270. [Google Scholar] [CrossRef]
- Roberts, L.; Chartier, Y.; Chartier, O.; Malenga, G.; Toole, M.; Rodka, H. Keeping clean water clean in a Malawi refugee camp: A randomized intervention trial. Bull. World Health Organ. 2001, 79, 280–287. [Google Scholar]
- WHO; UNICEF. Progress on Sanitation and Drinking Water—2015 Update and MDG Assessment. In UNICEF and World Health Organization; WHO Press: Geneva, Switzerland, 2015. [Google Scholar]
- Momba, M.N.B.; Kaleni, P. Regrowth and survival of indicator microorganisms on the surfaces of household containers used for the storage of drinking water in rural communities of South Africa. Water Res. 2002, 36, 3023–3028. [Google Scholar] [CrossRef]
- Jagals, P.; Jagals, C.; Bokako, T.C. The effect of container-biofilm on the microbiological quality of water used from plastic household containers. J. Water Health 2003, 1, 101–108. [Google Scholar] [CrossRef] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pathogen | Gene Targeted/Oligonucleotide Name | Sequence (5′-3′) | Gene Size (bp) | Ref. |
|---|---|---|---|---|
| E. coli | uidA-F | -AAAACGGCAAGAAAAAGCAG- | 147 | [21] |
| uidA-R | -ACGCGTGGTTAACAGTCTTGCG- | |||
| Shigella | ipaH-F | -GTTACCTGTACTCCCTGCTT-R CTAGCCTTCCTTGTGCAA | 200 | [22] |
| ipaH-R | -CTAGCCTTCCTTGTGCAA- | |||
| Salmonella | ipaB-F | -GGACTTTTTAAAAGCGGCGG- | 494 | [23] |
| ipaB-R | -GCCTCTCCCAGAGCCGTCTGG- | |||
| Vibrio | sodB-F | -AAGACCTCAACTGGCGGTA- | 248 | [24] |
| sodB-R | -GAAGTGTTAGTGATCGCCAGAGT- |
| Characteristics | Frequency N = 58 | Percentage % |
|---|---|---|
| Caregivers per age group | ||
| 17–21 | 3 | 5.2 |
| 22–26 | 16 | 27.6 |
| 27–31 | 14 | 24.1 |
| 32–36 | 18 | 31 |
| ≥37 | 7 | 12.1 |
| Number of children < 5 years | ||
| 1 | 15 | 25.9 |
| 2 | 17 | 29.3 |
| 3 | 22 | 37.9 |
| 4 | 4 | 6.9 |
| Number of household members | ||
| 2–4 | 19 | 32.8 |
| 5–7 | 25 | 43.1 |
| 8–9 | 12 | 20.7 |
| ≥10 | 2 | 3.4 |
| Sanitation facilities | ||
| Open pit latrines | 30 | 51.7 |
| Open field defecation | 25 | 43.1 |
| Defecate in streams | 3 | 5.2 |
| Water sources | ||
| Surface water | 42 | 72.4 |
| Spring water | 4 | 6.9 |
| Borehole water | 12 | 20.7 |
| Hygiene | ||
| Wash hands after using toilet | ||
| With soap | 0 | 0 |
| Without soap | 14 | 6.9 |
| Never wash hands after using toilet | 44 | 93.1 |
| Demographic Characteristics | E. coli Counts (<1 Log10 CFU/100 mL) | E. coli Counts (≥1 Log10 CFU/100 mL) | OR (95% CI) | p-Value | |
|---|---|---|---|---|---|
| Age groups of caregivers | 17–31 | 14 (42.4%) | 19 (57.6%) | 8.47 (0.15–3.35) | <0.05 |
| ≥32 | 2 (8%) | 23 (92%) | |||
| Number of children < 5 years per household | ≤2 | 20 (62.5) | 12 (37.5) | 9.17 (0.18–3.02) | <0.05 |
| ≥3 | 4 (11.5) | 22 (88.5) | |||
| Sanitation facility | Open pit latrines | 8 (26.7) | 22 (73.3) | 0.91 (−0.97–0.88) | >0.5 |
| Open defecation | 8 (28.6) | 20 (71.4) | |||
| Hygiene practice | Wash hands | 12 (85.7) | 2 (14.3) | 16.00 (0.68–3.95) | <0.05 |
| Do not wash hands (with/without soap) | 12 (27.3) | 32 (72.7) | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moropeng, R.C.; Budeli, P.; Momba, M.N.B. An Integrated Approach to Hygiene, Sanitation, and Storage Practices for Improving Microbial Quality of Drinking Water Treated at Point of Use: A Case Study in Makwane Village, South Africa. Int. J. Environ. Res. Public Health 2021, 18, 6313. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18126313
Moropeng RC, Budeli P, Momba MNB. An Integrated Approach to Hygiene, Sanitation, and Storage Practices for Improving Microbial Quality of Drinking Water Treated at Point of Use: A Case Study in Makwane Village, South Africa. International Journal of Environmental Research and Public Health. 2021; 18(12):6313. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18126313
Chicago/Turabian StyleMoropeng, Resoketswe Charlotte, Phumudzo Budeli, and Maggy Ndombo Benteke Momba. 2021. "An Integrated Approach to Hygiene, Sanitation, and Storage Practices for Improving Microbial Quality of Drinking Water Treated at Point of Use: A Case Study in Makwane Village, South Africa" International Journal of Environmental Research and Public Health 18, no. 12: 6313. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18126313