
A Complementary Intervention to Promote Wellbeing and Stress Management for Early Career Teachers


Abstract
:1. Introduction
1.1. Background
Organisational Wellbeing Initiatives
1.2. Yoga and Stress Management
Yoga and the Stress Response
2. Materials and Methods
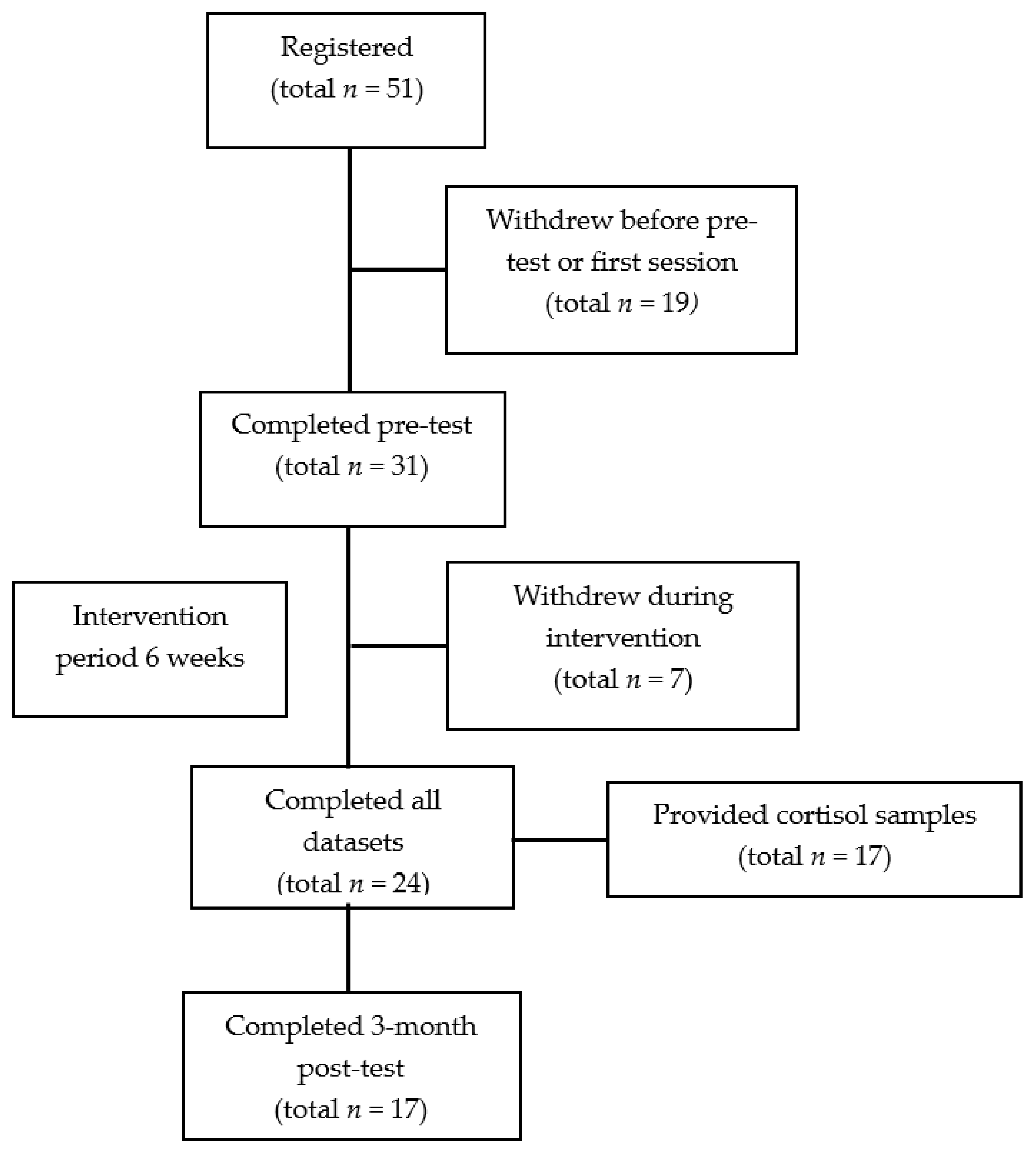
2.1. Participants
2.2. Measures
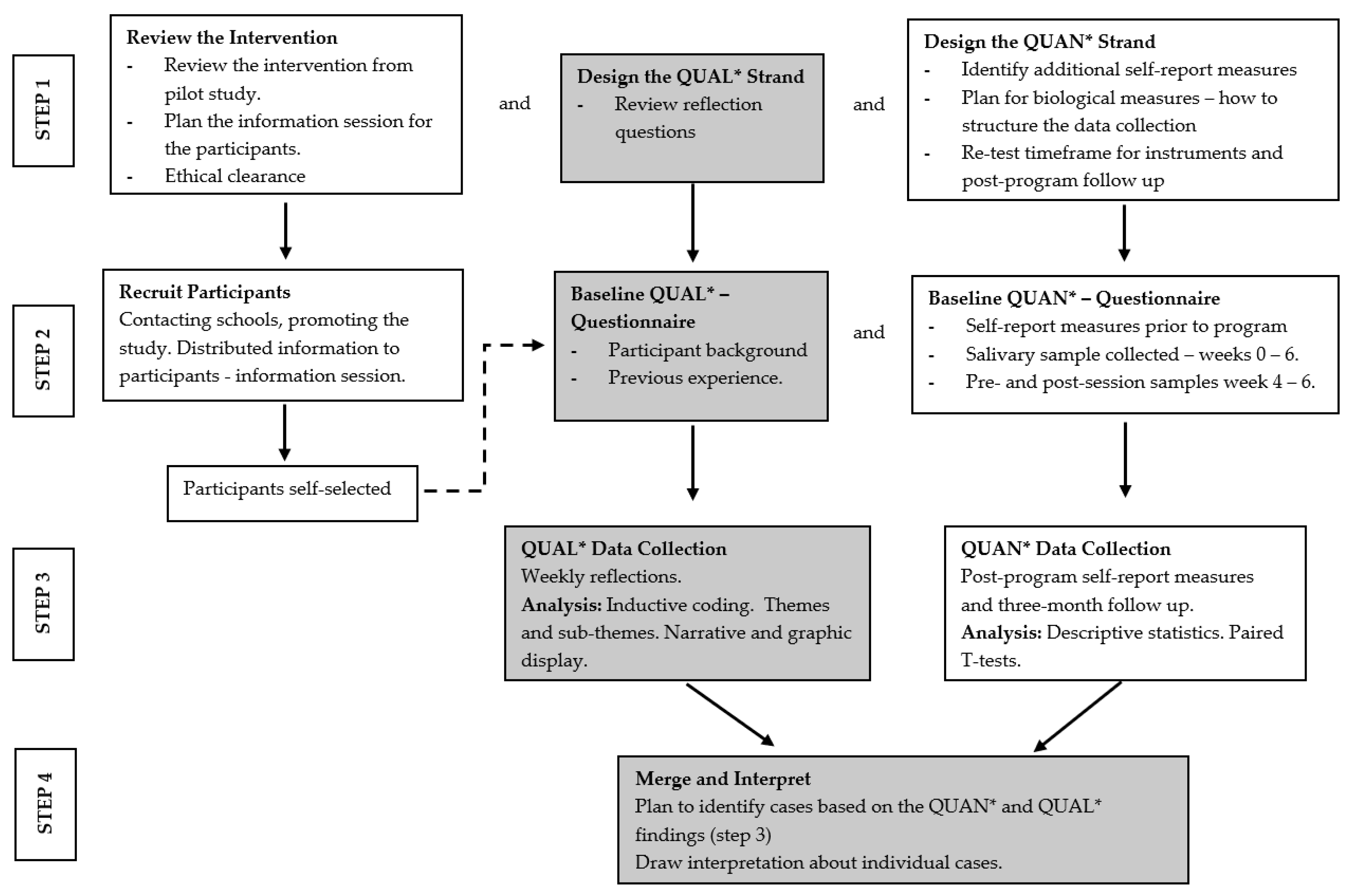
2.3. Intervention Design
2.3.1. Psychological Wellbeing: Sessions One and Two
2.3.2. Physiological Wellbeing: Sessions Two and Three
2.3.3. Interpersonal Wellbeing: Sessions Five and Six
2.3.4. Practical Component
2.3.5. Feasibility and Fidelity
2.4. Procedure
2.5. Data Preparation and Analysis
Quantitative Data
- OFC buffer bottles (containing OFC swab) were agitated for 2 minutes.
- Two drops of the buffer and saliva mixture were added to the cortisol LFD.
- The IPRO Cube Reader was used to scan the LFD at exactly 10 minutes.
3. Results
3.1. Internal Consistency and Descriptive Statistics
3.2. Paired-Samples t-Tests: Pre- and Post-Intervention
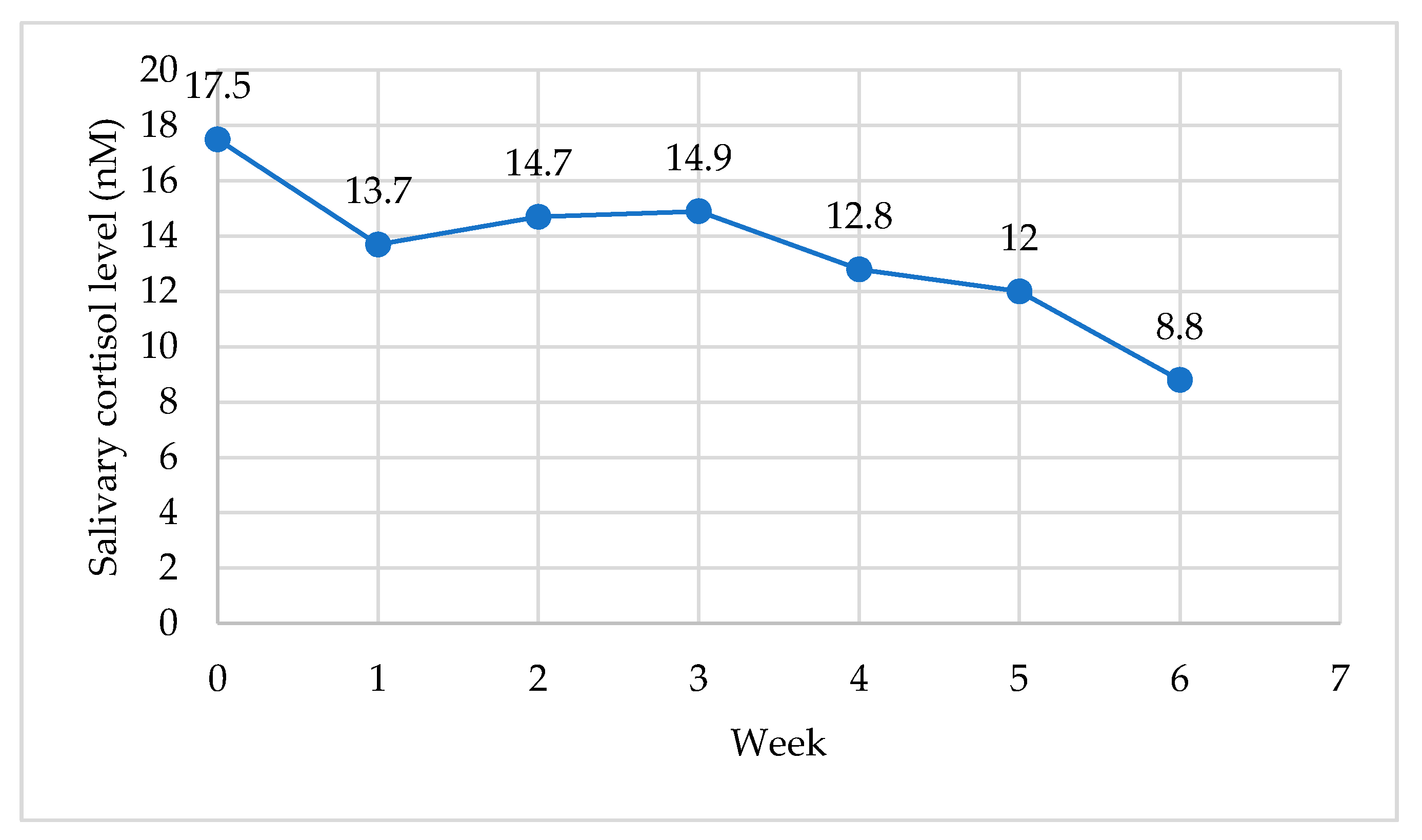
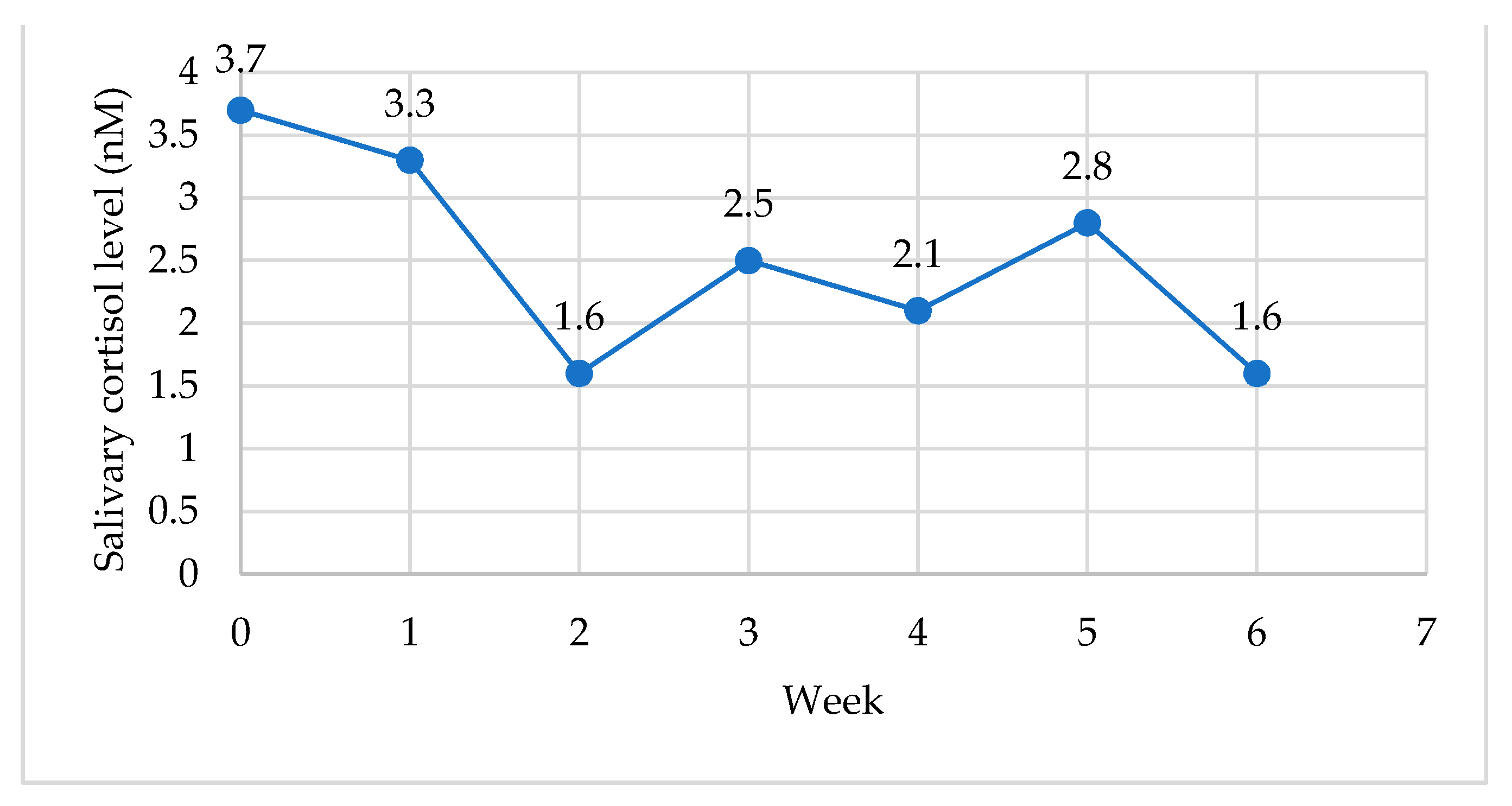
3.3. Weekly Salivary Cortisol Levels: Waking (CAR) and Resting Levels
Paired-Sample t-Tests Pre- and Post-Program
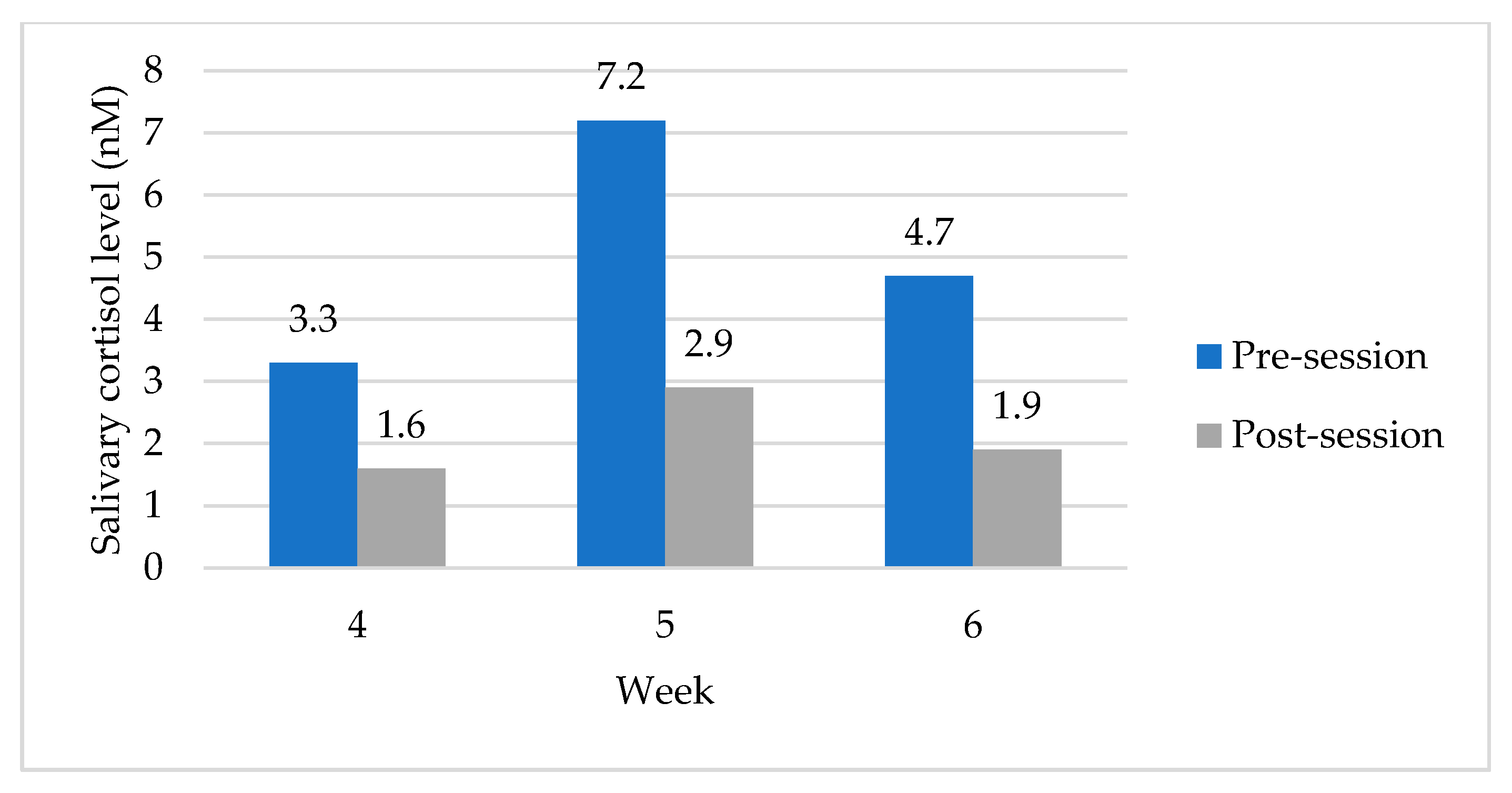
3.4. Pre- and Post-Session Salivary Cortisol Levels
Paired-Sample t-Tests Pre- and Post-Program
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Richardson, P.W.; Watt, H.M.; Devos, C. Types of Professional and Emotional Coping among Beginning Teachers. Adv. Res. Teach. 2013, 18, 229–253. [Google Scholar] [CrossRef]
- Buckworth, J. Issues in the teaching practicum. In The Challenge of Teaching through the Eyes of Pre-Service Teachers, 1st ed.; Geng, G., Smith, P., Black, P., Eds.; Springer: Singapore, 2017; pp. 9–17. [Google Scholar]
- Le Cornu, Rosie. University of South Australia. Building Early Career Teacher Resilience: The Role of Relationships. Aust. J. Teach. Educ. 2013, 38, 1. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Occupational Health Workplace Health Promotion. 2020. Available online: https://www.who.int/occupational_health/topics/workplace/en/ (accessed on 20 February 2020).
- Quick, J.C. Preventive Stress Management in Organizations; American Psychological Association: Washington, DC, USA, 1997. [Google Scholar]
- Jacobson, E. Progressive Relaxation: A Physiological and Clinical Investigation of Muscular States and Their Significance in Psy-Chology and Medical Practice, 2nd ed.; University of Chicago Press: Chicago, IL, USA, 1938. [Google Scholar]
- Le Fevre, M.; Kolt, G.; Matheny, J. Eustress, distress and their interpretation in primary and secondary occupational stress management interventions: Which way first? J. Manag. Psychol. 2006, 21, 547–565. [Google Scholar] [CrossRef]
- Australian Institute for Teaching and School Leadership. Australian Professional Standards for Teachers; Education Services Australia: Canberra, Australia, 2011; Available online: https://www.aitsl.edu.au/teach/standards (accessed on 31 March 2020).
- Parker, P.D.; Martin, A.J. Coping and buoyancy in the workplace: Understanding their effects on teachers’ work-related well-being and engagement. Teach. Teach. Educ. 2009, 25, 68–75. [Google Scholar] [CrossRef]
- Cooper, C.L.; Dewe, P.; O’Driscoll, M.P. Organizational interventions. In Organizational Stress a Review and Critique of Theory, Research, and Applications; Cooper, C.L., Dewe, P., O’Driscoll, M.P., Eds.; SAGE: London, UK, 2001; pp. 187–210. [Google Scholar]
- Hwang, Y.-S.; Bartlett, B.; Greben, M.; Hand, K. A systematic review of mindfulness interventions for in-service teachers: A tool to enhance teacher wellbeing and performance. Teach. Teach. Educ. 2017, 64, 26–42. [Google Scholar] [CrossRef]
- Skinner, E.; Beers, J. Mindfulness and teachers’ coping in the classroom: A developmental model of teacher stress, coping, and everyday resilience. In Mindfulness in Behavioral Health: Handbook of Mindfulness in Education: Integrating Theory and Research into Practice; Schonert-Reichl, K.A., Roeser, R.W., Eds.; Springer: New York, NY, USA, 2016; pp. 99–118. [Google Scholar]
- Kemeny, M.E.; Foltz, C.; Cavanagh, J.F.; Cullen, M.; Giese-Davis, J.; Jennings, P.; Rosenberg, E.L.; Gillath, O.; Shaver, P.R.; Wallace, B.A.; et al. Contemplative/emotion training reduces negative emotional behavior and promotes prosocial responses. Emotion 2012, 12, 338–350. [Google Scholar] [CrossRef]
- Jennings, P.A.; Brown, J.L.; Frank, J.L.; Doyle, S.; Oh, Y.; Davis, R.; Rasheed, D.; Deweese, A.; DeMauro, A.A.; Cham, H.; et al. Impacts of the CARE for Teachers program on teachers’ social and emotional competence and classroom interactions. J. Educ. Psychol. 2017, 109, 1010–1028. [Google Scholar] [CrossRef]
- Kabat-Zinn, J. Full Catastrophe Living: Using the Wisdom of Your Body and Mind to Face Stress, Pain, and Illness; Dell Publishing: New York, NY, USA, 1991. [Google Scholar]
- Beshai, S.; McAlpine, L.; Weare, K.; Kuyken, W. A Non-Randomised Feasibility Trial Assessing the Efficacy of a Mindfulness-Based Intervention for Teachers to Reduce Stress and Improve Well-Being. Mindfulness 2016, 7, 198–208. [Google Scholar] [CrossRef]
- Gold, E.; Smith, A.; Hopper, I.; Herne, D.; Tansey, G.; Hulland, C. Mindfulness-Based Stress Reduction (MBSR) for Primary School Teachers. J. Child Fam. Stud. 2010, 19, 184–189. [Google Scholar] [CrossRef]
- Flook, L.; Goldberg, S.; Pinger, L.; Bonus, K.; Davidson, R.J. Mindfulness for Teachers: A Pilot Study to Assess Effects on Stress, Burnout, and Teaching Efficacy. Mind Brain Educ. 2013, 7, 182–195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frank, J.L.; Reibel, D.; Broderick, P.; Cantrell, T.; Metz, S. The Effectiveness of Mindfulness-Based Stress Reduction on Educator Stress and Well-Being: Results from a Pilot Study. Mindfulness 2013, 6, 208–216. [Google Scholar] [CrossRef]
- Hwang, Y.-S.; Goldstein, H.; Medvedev, O.N.; Singh, N.N.; Noh, J.-E.; Hand, K. Mindfulness-Based Intervention for Educators: Effects of a School-Based Cluster Randomized Controlled Study. Mindfulness 2019, 10, 1417–1436. [Google Scholar] [CrossRef]
- Taylor, N.Z.; Millear, P.M.R. The contribution of mindfulness to predicting burnout in the workplace. Pers. Individ. Differ. 2016, 89, 123–128. [Google Scholar] [CrossRef]
- Franco, C.; Mañas, I.; Cangas, A.J.; Moreno, E.; Gallego, J. Reducing Teachers’ Psychological Distress through a Mindfulness Training Program. Span. J. Psychol. 2010, 13, 655–666. [Google Scholar] [CrossRef] [Green Version]
- Napoli, M. Mindfulness Training for Teachers: A Pilot Program. Complement. Health Pract. Rev. 2004, 9, 31–42. [Google Scholar] [CrossRef]
- Bernay, R.S. Mindfulness and the Beginning Teacher. Aust. J. Teach. Educ. 2014, 39, 4. [Google Scholar] [CrossRef] [Green Version]
- Schussler, D.L.; Jennings, P.A.; Sharp, J.E.; Frank, J.L. Improving Teacher Awareness and Well-Being through CARE: A Qualitative Analysis of the Underlying Mechanisms. Mindfulness 2016, 7, 130–142. [Google Scholar] [CrossRef]
- Jennings, P.A.; Frank, J.L.; Snowberg, K.E.; Coccia, M.A.; Greenberg, M.T. Improving classroom learning environments by Cultivating Awareness and Resilience in Education (CARE): Results of a randomized controlled trial. Sch. Psychol. Q. 2013, 28, 374–390. [Google Scholar] [CrossRef] [Green Version]
- Sharp, J.E.; Jennings, P.A. Strengthening Teacher Presence through Mindfulness: What Educators Say About the Cultivating Awareness and Resilience in Education (CARE) Program. Mindfulness 2016, 7, 209–218. [Google Scholar] [CrossRef]
- Jennings, P.A. Promoting teachers’ social and emotional competencies to support performance and reduce burnout. In Breaking the Mold of Preservice and Inservice Teacher Education; Cohan, A., Honigsfeld, A., Eds.; R&L Education: Lanham, MA, USA, 2011; pp. 105–113. [Google Scholar]
- Roeser, R.W.; Schonert-Reichl, K.A.; Jha, A.; Cullen, M.; Wallace, L.; Wilensky, R.; Oberle, E.; Thomson, K.; Taylor, C.; Harrison, J. Mindfulness training and reductions in teacher stress and burnout: Results from two randomized, waitlist-control field trials. J. Educ. Psychol. 2013, 105, 787–804. [Google Scholar] [CrossRef] [Green Version]
- Harris, A.R.; Jennings, P.A.; Katz, D.A.; Abenavoli, R.M.; Greenberg, M.T. Promoting Stress Management and Wellbeing in Educators: Feasibility and Efficacy of a School-Based Yoga and Mindfulness Intervention. Mindfulness 2016, 7, 143–154. [Google Scholar] [CrossRef]
- Soloway, G. Preparing teacher candidates for the present: Investigating the value of mindfulness-training in teacher education. In Mindfulness in Behavioral Health: Handbook of Mindfulness in Education: Integrating Theory and Research into Practice; Schonert-Reichl, K.A., Roeser, R.W., Eds.; Springer: New York, NY, USA, 2016; pp. 191–205. [Google Scholar]
- Pradhan, B. Yoga and Mindfulness Based Cognitive Therapy: A Clinical Guide; Springer International Publishing: New York, NY, USA, 2014. [Google Scholar]
- Swami, S. The Yoga Sutras of Patanjali; Integral Yoga Publications: Yogaville, VA, USA, 1978. [Google Scholar]
- Sovik, R.; Bhavanani, A. History, philosophy, and practice of yoga. In The Principles and Practice of Yoga in Health Care; Khalsa, S.B., Cohen, L., McCall, T., Telles, S., Eds.; Handspring Publishing Limited: London, UK, 2016; pp. 17–29. [Google Scholar]
- Saraswati, S.S. Yoga Nidra; Yoga Publications Trust: Bihar, India, 1976. [Google Scholar]
- Kamei, T.; Toriumi, Y.; Kimura, H.; Kumano, H.; Ohno, S.; Kimura, K. Decrease in Serum Cortisol during Yoga Exercise is Correlated with Alpha Wave Activation. Percept. Mot. Skills 2000, 90, 1027–1032. [Google Scholar] [CrossRef]
- Devi, S.K.; Chansauria, J.P.N.; Udupa, K. Mental depression and kundalini yoga. Anc. Sci. Life 1986, 6, 112–118. [Google Scholar] [PubMed]
- Uebelacker, L.; Lavretsky, H.; Tremont, G. Yoga therapy for depression. In The Principles and Practice of Yoga in Health Care; Khalsa, S.B., Cohen, L., McCall, T., Telles, S., Eds.; Handspring Publishing Limited: London, UK, 2016; pp. 73–94. [Google Scholar]
- Smith, J.A.; Greer, T.; Sheets, T.; Watson, S. Is there more to yoga than exercise? Altern. Ther. Health Med. 2011, 17, 22–29. [Google Scholar] [PubMed]
- Sullivan, M.; Carberry, A.; Evans, E.S.; Hall, E.E.; Nepocatych, S. The effects of power and stretch yoga on affect and salivary cortisol in women. J. Health Psychol. 2017, 24, 1658–1667. [Google Scholar] [CrossRef]
- West, J.; Otte, C.; Geher, K.; Johnson, J.; Mohr, D.C. Effects of hatha yoga and african dance on perceived stress, affect, and salivary cortisol. Ann. Behav. Med. 2004, 28, 114–118. [Google Scholar] [CrossRef] [PubMed]
- Berthoud, H.-R.; Neuhuber, W.L. Functional and chemical anatomy of the afferent vagal system. Auton. Neurosci. 2000, 85, 1–17. [Google Scholar] [CrossRef]
- Porges, S.W. The polyvagal perspective. Biol. Psychol. 2007, 74, 116–143. [Google Scholar] [CrossRef]
- Brown, R.P.; Gerbarg, P.L. Sudarshan Kriya Yogic Breathing in the Treatment of Stress, Anxiety, and Depression: Part II—Clinical Applications and Guidelines. J. Altern. Complement. Med. 2005, 11, 711–717. [Google Scholar] [CrossRef] [Green Version]
- Schmalzl, L.; Streeter, C.; Khalsa, S. Research on the psychophysiology of yoga. In The Principles and Practice of Yoga in Health Care; Khalsa, S.B., Cohen, L., McCall, T., Telles, S., Eds.; Handspring Publishing Limited: London, UK, 2016; pp. 49–68. [Google Scholar]
- Woolery, A.; Myers, H.; Sternlieb, B.; Zeltzer, L. A yoga intervention for young adults with elevated symptoms of depression. Altern. Ther. Health Med. 2004, 10, 60. [Google Scholar]
- Khattab, K.; Khattab, A.A.; Ortak, J.; Richardt, G.; Bonnemeier, H. Iyengar Yoga Increases Cardiac Parasympathetic Nervous Modulation among Healthy Yoga Practitioners. Evid. Based Complement. Altern. Med. 2007, 4, 511–517. [Google Scholar] [CrossRef] [PubMed]
- Streeter, C.; Gerbarg, P.; Saper, R.; Ciraulo, D.; Brown, R. Effects of yoga on the autonomic nervous system, gamma-aminobutyric-acid, and allostasis in epilepsy, depression, and post-traumatic stress disorder. Med. Hypotheses 2012, 78, 571–579. [Google Scholar] [CrossRef]
- Brown, R.P.; Gerbarg, P.L. Sudarshan Kriya Yogic Breathing in the Treatment of Stress, Anxiety, and Depression: Part I—Neurophysiologic Model. J. Altern. Complement. Med. 2005, 11, 189–201. [Google Scholar] [CrossRef] [PubMed]
- Streeter, C.C.; Whitfield, T.H.; Owen, L.; Rein, T.; Karri, S.K.; Yakhkind, A.; Perlmutter, R.; Prescot, A.; Renshaw, P.F.; Ciraulo, D.A.; et al. Effects of Yoga Versus Walking on Mood, Anxiety, and Brain GABA Levels: A Randomized Controlled MRS Study. J. Altern. Complement. Med. 2010, 16, 1145–1152. [Google Scholar] [CrossRef]
- Brown, R.P.; Gerbarg, P.L.; Muench, F. Breathing Practices for Treatment of Psychiatric and Stress-Related Medical Conditions. Psychiatr. Clin. N. Am. 2013, 36, 121–140. [Google Scholar] [CrossRef] [PubMed]
- Gard, T.; Noggle, J.J.; Park, C.L.; Vago, D.R.; Ewilson, A. Potential self-regulatory mechanisms of yoga for psychological health. Front. Hum. Neurosci. 2014, 8, 770. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCall, T.B. Yoga as Medicine: The Yogic Prescription for Health and Healing; Bantam Books: New York, NY, USA, 2007. [Google Scholar]
- Pilkington, K.; Gerbarg, P.L.; Brown, R.P. Yoga therapy for anxiety. In The Principles and Practice of Yoga in Health Care; Khalsa, S.B., Cohen, L., McCall, T., Telles, S., Eds.; Handspring Publishing Limited: London, UK, 2016; pp. 95–116. [Google Scholar]
- Vago, D.R.P.; Silbersweig, D.A. Self-awareness, self-regulation, and self-transcendence (S-ART): A framework for understanding the neurobiological mechanisms of mindfulness. Front. Hum. Neurosci. 2012, 6, 296. [Google Scholar] [CrossRef] [Green Version]
- Lovallo, W.R. Stress and Health: Biological and Psychological Interactions, 3rd ed.; Sage Publications: Thousand Oaks, CA, USA, 2016. [Google Scholar]
- Mulholland, R.; McKinlay, A.; Sproule, J. Teachers in need of space: The content and changing context of work. Educ. Rev. 2016, 69, 1–20. [Google Scholar] [CrossRef] [Green Version]
- Queensland College of Teachers. Queensland Teachers Annual Report 2019. Queensland College of Teachers, 2019. Available online: https://www.qct.edu.au/about/corporate-publications (accessed on 30 March 2020).
- Brown, K.W.; Ryan, R.M. The benefits of being present: Mindfulness and its role in psychological well-being. J. Pers. Soc. Psychol. 2003, 84, 822–848. [Google Scholar] [CrossRef] [Green Version]
- Brown, R. The Perceived Impact of Mindfulness Instruction on Pre-Service Elementary Teachers. Child. Educ. 2017, 93, 136–146. [Google Scholar] [CrossRef]
- Hue, M.-T.; Lau, N.-S. Promoting well-being and preventing burnout in teacher education: A pilot study of a mindfulness-based programme for pre-service teachers in Hong Kong. Teach. Dev. 2015, 19, 381–401. [Google Scholar] [CrossRef]
- Kostanski, M. The role of mindfulness in reducing stress for pre-service students. In Proceedings of the Australian Association for Research in Education Conference, Fremantle, Australia, 25 November 2007; Available online: http://www.aare.edu.au/data/publications/2007/kos07569.pdf (accessed on 27 April 2017).
- Cummins, R.A.; McCabe, M.P.; Romeo, Y.; Gullone, E. Validity Studies the Comprehensive Quality of Life Scale (Comqol): Instrument Development and Psychometric Evaluation on College Staff and Students. Educ. Psychol. Meas. 1994, 54, 372–382. [Google Scholar] [CrossRef]
- Cummins, R. The domains of life satisfaction: An attempt to order chaos. Soc. Indic. Res. 1996, 38, 303–328. [Google Scholar] [CrossRef]
- International Wellbeing Group. Personal Wellbeing Index, 5th ed.; Australian Centre of Quality of Life: Melbourne, Australia, 2013; Available online: http://www.deakin.edu.au/research/acqol/instruments/wellbeing-index/index.php (accessed on 10 March 2017).
- Tomyn, A.J.; Tyszkiewicz, M.D.F.; Cummins, R.A. The Personal Wellbeing Index: Psychometric Equivalence for Adults and School Children. Soc. Indic. Res. 2011, 110, 913–924. [Google Scholar] [CrossRef]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S. The Perceived Stress Scale; Mind Garden Inc.: Menlo Park, CA, USA, 1994; pp. 1–5. Available online: http://www.mindgarden.com/documents/PerceivedStressScale.pdf (accessed on 6 July 2018).
- Hester, N. Yoga and Teacher Stress: An Examination of a Workplace-Based Yoga Practice on the Perceived Stress of Elementary School Teachers. Ph.D. Thesis, ProQuest Dissertations Publishing, Morrisvillem, NC, USA, 2017. Available online: https://0-search-proquest-com.brum.beds.ac.uk/docview/1969169426 (accessed on 26 July 2018).
- Katz, D.A.; Greenberg, M.T.; Jennings, P.A.; Klein, L.C. Associations between the awakening responses of salivary α-amylase and cortisol with self-report indicators of health and wellbeing among educators. Teach. Teach. Educ. 2016, 54, 98–106. [Google Scholar] [CrossRef]
- Kerr, S.L.; Lucas, L.J.; DiDomenico, G.E.; Mishra, V.; Stanton, B.J.; Shivde, G.; Pero, A.N.; Runyen, M.E.; Terry, G.M. Is mindfulness training useful for pre-service teachers? An exploratory investigation. Teach. Educ. 2017, 28, 349–359. [Google Scholar] [CrossRef]
- Geng, G.; Midford, R.; Buckworth, J. Investigating the Stress Levels of Early Childhood, Primary and Secondary Pre-service Teachers during Teaching Practicum. J. Teach. Educ. Sustain. 2015, 17, 35–47. [Google Scholar] [CrossRef] [Green Version]
- Hopkins, W.S.; Hoffman, S.Q.; Moss, V.D. Professional Development Schools and Preservice Teacher Stress. Action Teach. Educ. 1997, 18, 36–46. [Google Scholar] [CrossRef]
- Martin, N.K.; Sass, D.A.; Schmitt, T.A. Teacher efficacy in student engagement, instructional management, student stressors, and burnout: A theoretical model using in-class variables to predict teachers’ intent-to-leave. Teach. Teach. Educ. 2012, 28, 546–559. [Google Scholar] [CrossRef]
- Maslach, C.; Jackson, S.E.; Leiter, M.P. Maslach Burnout Inventory Manual, 3rd ed.; Consulting Psychologists Press: Palo Alto, CA, USA, 1996. [Google Scholar]
- Van Katwyk, P.T.; Fox, S.; Spector, P.E.; Kelloway, E.K. Using the Job-Related Affective Well-Being Scale (JAWS) to investigate affective responses to work stressors. J. Occup. Health Psychol. 2000, 5, 219–230. [Google Scholar] [CrossRef] [PubMed]
- Travers, C. Current knowledge on the nature, prevalence, sources and potential impact of teacher stress. In Educator Stress: An Occupational Health Perspective; McIntyre, T.M., McIntyre, S.E., Francis, D.J., Eds.; Springer International Publishing: Cham, Switzerland, 2017; pp. 347–368. [Google Scholar]
- Bruk-Lee, V.; Spector, P.E. The social stressors-counterproductive work behaviors link: Are conflicts with supervisors and coworkers the same? J. Occup. Health Psychol. 2006, 11, 145–156. [Google Scholar] [CrossRef]
- Cole, M.S.; Walter, F.; Bruch, H. Affective mechanisms linking dysfunctional behavior to performance in work teams: A moderated mediation study. J. Appl. Psychol. 2008, 93, 945–958. [Google Scholar] [CrossRef]
- Machin, M.A.; Hoare, P.N. The role of workload and driver coping styles in predicting bus drivers’ need for recovery, positive and negative affect, and physical symptoms. Anxiety Stress Coping 2008, 21, 359–375. [Google Scholar] [CrossRef] [Green Version]
- Greer, J.G.; Greer, B.B. Stopping Burnout Before it Starts: Prevention Measures at the Preservice Level. Teach. Educ. Spec. Educ. J. Teach. Educ. Div. Counc. Except. Child. 1992, 15, 168–174. [Google Scholar] [CrossRef]
- Hemmings, B.; Hockley, T. Student teacher stress and coping mechanisms. Educ. Rural Aust. 2002, 12, 25–35. [Google Scholar]
- Turner, S.; Zanker, N.; Braine, M. An investigation into teacher wellbeing during the teacher training year. Des. Technol. Educ. 2012, 17, 21–34. [Google Scholar]
- Mental Health Foundation. Food for Thought: Mental Health and Nutrition Briefing. 2016. Available online: https://www.mentalhealth.org.uk/sites/default/files/food-for-thought-mental-health-nutrition-briefing-march-2017.pdf (accessed on 21 March 2019).
- Mayer, E. The Mind-Gut Connection: How the Hidden Conversation within Our Bodies Impacts Our Mood, Our Choices, and Our Overall Health; HarperCollins Publishers: New York, NY, USA, 2018. [Google Scholar]
- Mosley, M. The Clever Guts Diet—How to Revolutionise Your Body from the Inside Out; Short Books: London, UK, 2017. [Google Scholar]
- Koch, L. Core Awareness—Enhancing Yoga, Pilates, Exercise and Dance; North Atlantic Books: Berkeley, CA, USA, 2012. [Google Scholar]
- Langevin, H.M.; Nedergaard, M.; Howe, A.K. Cellular control of connective tissue matrix tension. J. Cell. Biochem. 2013, 114, 1714–1719. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Long, R. The Key Poses of Yoga; Bandha Yoga Publications: Chaplain, NY, USA, 2008; Volume 2. [Google Scholar]
- Lou, H.C.; Kjaer, T.W.; Friberg, L.; Wildschiodtz, G.; Holm, S.; Norwak, M. A 15O-H2O PET study of meditation and the resting state of normal consciousness. Hum. Brain Mapp. 1990, 7, 98–105. [Google Scholar] [CrossRef]
- Kjaer, T.W.; Bertelsen, C.; Piccini, P.; Brooks, D.; Alving, J.; Lou, H.C. Increased dopamine tone during meditation-induced change of consciousness. Cogn. Brain Res. 2002, 13, 255–259. [Google Scholar] [CrossRef]
- Salmon, P.; Lush, E.; Jablonski, M.; Sephton, S. Yoga and Mindfulness: Clinical Aspects of an Ancient Mind/Body Practice. Cogn. Behav. Pract. 2009, 16, 59–72. [Google Scholar] [CrossRef]
- Australian Research Council and Universities. National Statement on Ethical Conduct in Human Research 2007; National Health and Medical Research Council: Canberra, Australia, 2018. Available online: www.nhmrc.gov.au/guidelines/publications/e72 (accessed on 24 April 2019).
- Jehanli, A.; Dunbar, J.; Skelhorn, S. Development and validation of an oral fluid collection device and its use in the immuno-assay of salivary steroids and immunoglobulins in sports persons. In Proceedings of the International Society of Exercise Immu-nology Symposium, Wallingford, UK, 11–13 July 2011. [Google Scholar]
- Dunbar, J.; Hazell, G.; Jehanli, A. Evaluation of a new point of care quantitative cube reader for salivary analysis in premier league soccer clubs. In Proceedings of the International Sports Science and Sports Medicine Conference, Newcastle Upon Tyne, UK, 8–10 September 2015. [Google Scholar]
- Evans, J. Straight forward Statistics for the Behavioral Sciences; Brooks/Cole Publishing: Pacific Grove, CA, USA, 1996. [Google Scholar]
- Hepburn, S.-J. Integrated Wellbeing for Teachers: A Mixed-Methods Study Investigating Attention Awareness, Perceived Stress and Subjective Wellbeing and a Complementary Intervention for Pre-service and Early Career Teachers. Ph.D. Thesis, The University of Queensland, Brisbane, Australia, 2020. [Google Scholar] [CrossRef]
- Moir, E. The Stages of a Teacher’s First Year. A Better Beginning, Supporting and Mentoring New Teachers; Association for Supervision and Curriculum Development: Alexandria, VA, USA, 1999. [Google Scholar]
- Baer, R.A.; Smith, G.T.; Hopkins, J.; Krietemeyer, J.; Toney, L. Using Self-Report Assessment Methods to Explore Facets of Mindfulness. Assessment 2006, 13, 27–45. [Google Scholar] [CrossRef] [Green Version]
- Jennings, P.A.; Greenberg, M.T. The Prosocial Classroom: Teacher Social and Emotional Competence in Relation to Student and Classroom Outcomes. Rev. Educ. Res. 2009, 79, 491–525. [Google Scholar] [CrossRef]
- Tennant, R.; Hiller, L.; Fishwick, R.; Platt, S.; Joseph, S.; Weich, S.; Parkinson, J.; Secker, J.; Stewart-Brown, S. The Warwick-Edinburgh Mental Well-being Scale (WEMWBS): Development and UK validation. Health Qual. Life Outcomes 2007, 5, 63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. WHO (Five) Well-Being Index; Frederiksborg General Hospital Hillerød WHO Collaborating Center for Mental Health: Hillerød, Danmark, 1998; Available online: https://www.psykiatri-regionh.dk/who-5/about-the-who-5/Pages/default.aspx (accessed on 15 April 2019).
- Huppert, F.A. Psychological Well-being: Evidence Regarding its Causes and Consequences. Appl. Psychol. Health Well-Being 2009, 1, 137–164. [Google Scholar] [CrossRef]
- McEwen, B.S. Physiology and Neurobiology of Stress and Adaptation: Central Role of the Brain. Physiol. Rev. 2007, 87, 873–904. [Google Scholar] [CrossRef] [Green Version]
- Kemeny, M.E.; Schedlowski, M. Understanding the interaction between psychosocial stress and immune-related diseases: A stepwise progression. Brain Behav. Immun. 2007, 21, 1009–1018. [Google Scholar] [CrossRef]
- Bellingrath, S.; Kudielka, B.M. Biological pathways to stress-related disease vulnerability in educators. In Educator Stress: An Occupational Health Perspective; McIntyre, T.M., McIntyre, S.E., Francis, D.J., Eds.; Springer: Cham, Switzerland, 2017; pp. 77–100. [Google Scholar]
- Nater, U.; Maloney, E.; Boneva, R.S.; Gurbaxani, B.M.; Lin, J.-M.; Jones, J.F.; Reeves, W.C.; Heim, C. Attenuated Morning Salivary Cortisol Concentrations in a Population-Based Study of Persons with Chronic Fatigue Syndrome and Well Controls. J. Clin. Endocrinol. Metab. 2008, 93, 703–709. [Google Scholar] [CrossRef] [Green Version]
- de Kloet, E.R.; Karst, H.; Joels, M. Corticosteroid hormones in the central stress response: Quick-and-slow. Front. Neuroendocr. 2008, 29, 268–272. [Google Scholar] [CrossRef]
- Pruessner, J.C.; Hellhammer, D.H.; Kirschbaum, C. Burnout, perceived stress, and cortisol responses to awakening. Psychosom. Med. 1999, 61, 197–204. [Google Scholar] [CrossRef]
- Taylor, A.G.; Goehler, L.E.; Galper, D.I.; Innes, K.E.; Bourguignon, C. Top-Down and Bottom-Up Mechanisms in Mind-Body Medicine: Development of an Integrative Framework for Psychophysiological Research. Explore 2010, 6, 29–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Field, T. Yoga clinical research review. Complement. Ther. Clin. Pract. 2011, 17, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Rapaport, M.H.; Schettler, P.; Bresee, C. A Preliminary Study of the Effects of Repeated Massage on Hypothalamic–Pituitary–Adrenal and Immune Function in Healthy Individuals: A Study of Mechanisms of Action and Dosage. J. Altern. Complement. Med. 2012, 18, 789–797. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Creswell, J. Educational Research: Planning, Conducting and Evaluating Quantitative and Qualitative Research, 4th ed.; Pearson: Harlow, UK, 2014. [Google Scholar]
- Teddlie, C.; Tashakkori, A. Foundations of Mixed Methods Research: Integrating Quantitative and Qualitative Approaches in the Social and Behavioral Sciences; Sage Publications: Thousand Oaks, CA, USA, 2009. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Technique | Mechanism | Layers of Tension | Output | |
|---|---|---|---|---|
| Decrease | Increase | |||
| Meditation Practices (Samyama) | Attentional stability Response inhibition Meta-awareness | Mental | Habitual maladaptive tendencies. | Executive monitoring systems. |
| Ethical Principles (Yama, Niyama) | Introspection Non-reactive awareness | Emotional | Rumination Emotional reactions. | Prosocial behaviour. |
| Postures (Asana) Breathing Practice (Pranayama) | Interoceptive and proprioceptive awareness. Vagal tone. | Physical | Cortisol Inflammation Tension HPA-axis activation | PSN activation. |
| Characteristic | All Participants % | n |
|---|---|---|
| Female (%) | 91.7 | 22 |
| Male (%) | 8.3 | 2 |
| Fulltime (%) | 75 | 18 |
| Part-time (%) | 25 | 6 |
| First career (%) | 37.5 | 9 |
| Industry experience prior to teaching (%) | 62.5 | 15 |
| Dependents: Yes (%) | 10 | 41.7 |
| Dependents: No (%) | 14 | 58.3 |
| First year teaching (%) | 45.8 | 11 |
| Second year teaching (%) | 12.5 | 3 |
| Three to five years’ teaching (%) | 41.6 | 10 |
| Lower Primary: Prep–Grade 2 (%) | 26.1 | 6 |
| Upper Primary: Grade 3–6 (%) | 56.5 | 13 |
| Secondary: Grade 7–9 (%) | 17.4 | 4 |
| Secondary: Grade 10–12 (%) | 0 | 0 |
| Secondary: Grade 7–12 (%) | 4.2 | 1 |
| Topic | Week | Theoretical Content | Physical Practice (Minutes) | Activities |
|---|---|---|---|---|
| Psychological Wellbeing | 1 | The impact of stress | 20–25 | Instant relaxation techniques: breathing practices, visualisation Restorative poses and sequences. Supported inversions. Guided meditation: Yoga Nidra, Compassion meditation, positive experiences. Gentle stretching (postures). Reflection activities Group discussion |
| 2 | The benefits of relaxation | 30 | ||
| Physiological Wellbeing | 3 | The importance of exercise | 30–45 | |
| 4 | Diet and stress | 60 | ||
| Social Wellbeing | 5 | Self-compassion | 60 | |
| 6 | Professional relationships | 60 | ||
| Home practice: 3–20-min guided meditation (pre-recorded audio track) 10–20-min yoga sequence (pre-recorded track) Breathing practices (practice length determined by the individual) | ||||
| Scale | Cronbach’s Alpha A | |
|---|---|---|
| Pre-Program | Post-Program | |
| Mindful Attention Awareness (MAAS) | 0.89 | 0.89 |
| Perceived Stress (PSS) | 0.92 | 0.80 |
| Personal Wellbeing Index (PWI) | 0.86 | 0.89 |
| Maslach Burnout Inventory (MBI-ES) Emotional Exhaustion Depersonalisation Personal Accomplishment | 0.91 | 0.75 |
| 0.90 | 0.59 | |
| 0.73 | 0.90 | |
| Job-related Affective Wellbeing (JAWS) Positive emotions | 0.86 | 0.90 |
| Negative emotions | 0.89 | 0.88 |
| Pre-Program | Post-Program | Paired t-Test | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Scale | Mean | SD | Mean | SD | sd | t | p-Value | ||
| MAAS | 3.55 | 0.79 | 4.0 | 0.67 | −0.44 | 0.61 | −0.72 | −3.54 | 0.002 |
| PSS | 21.13 | 7.07 | 16.63 | 4.5 | 4.5 | 5.48 | 0.82 | 4.01 | 0.001 |
| PWI | 52 | 9.3 | 57.4 | 11.53 | −5.4 | 8.6 | −0.62 | −3.05 | 0.006 |
| MBI-ES Emotional Exhaustion | 27.63 | 11.08 | 24.92 | 10.14 | 2.7 | 9.38 | 0.28 | 1.4 | 0.17 |
| MBI-ES Depersonalisation | 7.13 | 8.20 | 6.50 | 5.46 | 0.62 | 5.32 | 0.11 | 0.57 | 0.57 |
| MBI-ES Personal Accomplishment | 36.21 | 5.16 | 35.29 | 7.03 | 0.91 | 6.7 | 0.13 | 0.66 | 0.51 |
| JAWS—Positive | 28.33 | 5.69 | 29.63 | 6.02 | −1.29 | 4.5 | −0.26 | −1.38 | 0.18 |
| JAWS—Negative | 24.58 | 6.32 | 23.17 | 6.12 | 1.4 | 5.08 | 0.27 | 1.36 | 0.18 |
| Time One | Time Two | Paired t-Test | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | sd | t | p-Value | |||
| Waking cortisol level | 17.26 | 4.22 | 9.12 | 4.27 | 8.14 | 4.97 | 1.66 | 6.34 | 0.001 |
| Resting cortisol level | 3.48 | 1.56 | 1.98 | 1.16 | 1.5 | 1.76 | 0.85 | 3.29 | 0.005 |
| Session Four | 3.44 | 1.36 | 1.56 | 0.65 | 1.88 | 1.14 | 1.64 | 6.37 | 0.001 |
| Session Five | 7.18 | 4.81 | 2.72 | 2.45 | 4.46 | 3.94 | 1.13 | 4.38 | 0.001 |
| Session Six | 4.44 | 2.62 | 1.84 | 0.66 | 2.6 | 2.54 | 1.02 | 4.2 | 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hepburn, S.-J.; Carroll, A.; McCuaig-Holcroft, L. A Complementary Intervention to Promote Wellbeing and Stress Management for Early Career Teachers. Int. J. Environ. Res. Public Health 2021, 18, 6320. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18126320
Hepburn S-J, Carroll A, McCuaig-Holcroft L. A Complementary Intervention to Promote Wellbeing and Stress Management for Early Career Teachers. International Journal of Environmental Research and Public Health. 2021; 18(12):6320. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18126320
Chicago/Turabian StyleHepburn, Stevie-Jae, Annemaree Carroll, and Louise McCuaig-Holcroft. 2021. "A Complementary Intervention to Promote Wellbeing and Stress Management for Early Career Teachers" International Journal of Environmental Research and Public Health 18, no. 12: 6320. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18126320