
Association of Family History with the Development of Breast Cancer: A Cohort Study of 129,374 Women in KoGES Data


Abstract
:1. Introduction
2. Materials and Methods
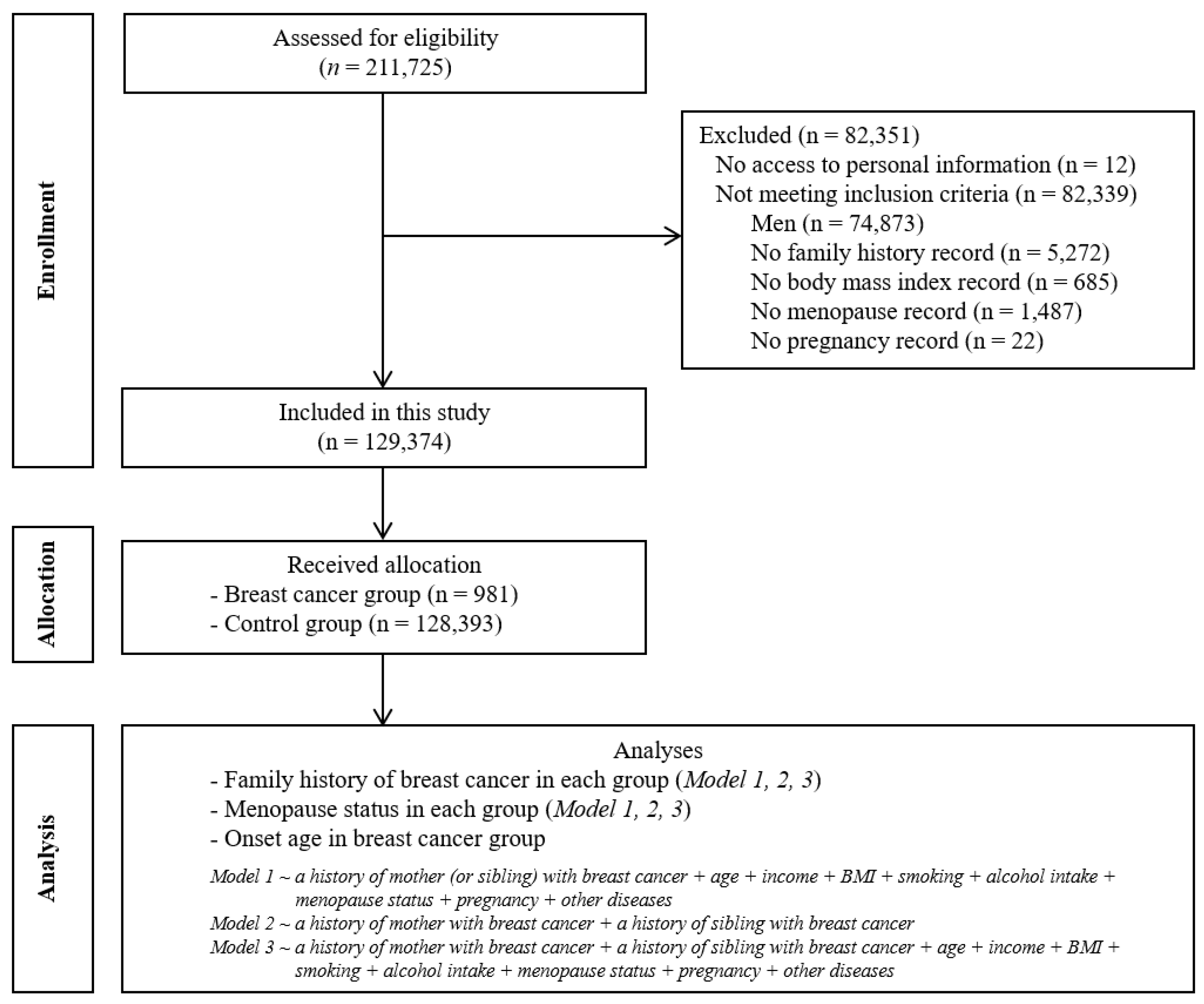
2.1. Study Design
2.2. Data Survey
2.3. Statistics
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics. CA A Cancer J. Clin. 2020, 70, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Warner, E. Breast-Cancer Screening. N. Engl. J. Med. 2011, 365, 1025–1032. [Google Scholar] [CrossRef]
- Hong, S.; Won, Y.-J.; Park, Y.R.; Jung, K.-W.; Kong, H.-J.; Lee, E.S.; Community of Population-Based Regional Cancer Registries. Cancer statistics in Korea: Incidence, mortality, survival, and prevalence in 2017. Cancer Res. Treat. 2020, 52, 335–350. [Google Scholar] [CrossRef]
- DeSantis, C.E.; Ma, J.; Gaudet, M.M.; Newman, L.A.; Mph, K.D.M.; Sauer, A.G.; Jemal, A.; Siegel, R.L. Breast cancer statistics, 2019. CA A Cancer J. Clin. 2019, 69, 438–451. [Google Scholar] [CrossRef] [PubMed]
- Dafni, U.; Tsourti, Z.; Alatsathianos, I. Breast Cancer Statistics in the European Union: Incidence and Survival across Euro-pean Countries. Breast Care 2019, 14, 344–353. [Google Scholar] [CrossRef]
- Islami, F.; Sauer, A.G.; Miller, K.D.; Siegel, R.L.; Fedewa, S.A.; Jacobs, E.J.; McCullough, M.L.; Patel, A.V.; Ma, J.; Soerjomataram, I.; et al. Proportion and number of cancer cases and deaths attributable to potentially modifiable risk factors in the United States. CA A Cancer J. Clin. 2017, 68, 31–54. [Google Scholar] [CrossRef] [PubMed]
- Tamimi, R.M.; Spiegelman, D.; Smith-Warner, S.A.; Wang, M.; Pazaris, M.; Willett, W.C.; Eliassen, A.H.; Hunter, D.J. Popu-lation Attributable Risk of Modifiable and Nonmodifiable Breast Cancer Risk Factors in Postmenopausal Breast Cancer. Am. J. Epidemiol. 2016, 184, 884–893. [Google Scholar] [CrossRef] [Green Version]
- Engmann, N.J.; Golmakani, M.K.; Miglioretti, D.L.; Sprague, B.L.; Kerlikowske, K. For the Breast Cancer Surveillance Consortium Population-Attributable Risk Proportion of Clinical Risk Factors for Breast Cancer. JAMA Oncol. 2017, 3, 1228–1236. [Google Scholar] [CrossRef]
- Whiteman, D.C.; Webb, P.M.; Green, A.C.; Neale, R.E.; Fritschi, L.; Bain, C.J.; Parkin, D.M.; Wilson, L.F.; Olsen, C.M.; Nagle, C.M.; et al. Cancers in Australia in 2010 attributable to modifiable factors: Summary and conclusions. Aust. N. Z. J. Public Heal. 2015, 39, 477–484. [Google Scholar] [CrossRef] [Green Version]
- Lalloo, F.; Evans, D.G. Familial Breast Cancer. Clin. Genet. 2012, 82, 105–114. [Google Scholar] [CrossRef]
- Pharoah, P.D.; Antoniou, A.C.; Easton, D.F.; Ponder, B.A. Polygenes, risk prediction, and targeted prevention of breast cancer. N. Engl. J. Med. 2008, 358, 2796–2803. [Google Scholar] [CrossRef]
- Lu, K.H.; Wood, M.E.; Daniels, M.; Burke, C.; Ford, J.; Kauff, N.D.; Kohlmann, W.; Lindor, N.M.; Mulvey, T.M.; Robinson, L.; et al. American society of clinical oncology expert statement: Collection and use of a cancer family history for oncology providers. J. Clin. Oncol. 2014, 32, 833–840. [Google Scholar] [CrossRef] [PubMed]
- Baumgart, L.A.; Postula, K.J.V.; Knaus, W.A. Initial clinical validation of Health Heritage, a patient-facing tool for personal and family history collection and cancer risk assessment. Fam. Cancer 2015, 15, 331–339. [Google Scholar] [CrossRef] [PubMed]
- Daly, M.B.; Pilarski, R.; Yurgelun, M.B.; Berry, M.P.; Buys, S.S.; Dickson, P.; Domchek, S.M.; Elkhanany, A.; Friedman, S.; Garber, J.E.; et al. NCCN Guidelines Insights: Genetic/Familial High-Risk Assessment: Breast, Ovarian, and Pancreatic, Version 1.2020. J. Natl. Compr. Cancer Netw. 2020, 18, 380–391. [Google Scholar] [CrossRef] [PubMed]
- Scott, D.; Friedman, S.; Telli, M.L.; Kurian, A.W. Decision Making About Genetic Testing Among Women With a Personal and Family History of Breast Cancer. JCO Oncol. Pract. 2020, 16, e37–e55. [Google Scholar] [CrossRef]
- Owens, D.K.; Davidson, K.W.; Krist, A.H.; Barry, M.J.; Cabana, M.; Caughey, A.B.; Doubeni, C.A.; Epling, J.W., Jr.; Kubik, M.; Landefeld, C.S.; et al. Risk assessment, genetic counseling, and genetic testing for BRCA-related cancer: US preventive ser-vices task force recommendation statement. JAMA 2019, 322, 652–665. [Google Scholar]
- Gail, M.H.; Brinton, L.A.; Byar, D.P.; Corle, D.K.; Green, S.B.; Schairer, C.; Mulvihill, J.J. Projecting individualized probabili-ties of developing breast cancer for white females who are being examined annually. J. Natl. Cancer Inst. 1989, 81, 1879–1886. [Google Scholar] [CrossRef]
- Wood, M.E.; Rehman, H.T.; Bedrosian, I. Importance of family history and indications for genetic testing. Breast J. 2020, 26, 100–104. [Google Scholar] [CrossRef] [PubMed]
- Mukama, T.; Kharazmi, E.; Sundquist, K.; Sundquist, J.; Brenner, H.; Fallah, M. Familial risk of breast cancer by dynamic, accumulative, and static definitions of family history. Cancer 2020, 126, 2837–2848. [Google Scholar] [CrossRef] [Green Version]
- Liaw, Y.Y.; Loong, F.S.; Tan, S.; On, S.Y.; Khaw, E.; Chiew, Y.; Nordin, R.; Mat, T.N.; Arulanantham, S.; Gandhi, A. A retrospective study on breast cancer presentation, risk factors, and protective factors in patients with a positive family history of breast cancer. Breast J. 2019, 26, 469–473. [Google Scholar] [CrossRef]
- Ramsey, S.D.; Yoon, P.; Moonesinghe, R.; Khoury, M.J. Population-based study of the prevalence of family history of cancer: Implications for cancer screening and prevention. Genet. Med. 2006, 8, 571–575. [Google Scholar] [CrossRef] [Green Version]
- Collaborative Group on Hormonal Factors in Breast Cancer. Familial breast cancer: Collaborative reanalysis of individual data from 52 epidemiological studies including 58,209 women with breast cancer and 101,986 women without the disease. Lancet 2001, 358, 1389–1399. [Google Scholar] [CrossRef]
- Chen, S.; Parmigiani, G. Meta-Analysis of BRCA1 and BRCA2 Penetrance. J. Clin. Oncol. 2007, 25, 1329–1333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, J.-Y.; Lee, K.-M.; Park, S.K.; Noh, D.-Y.; Ahn, S.-H.; Yoo, K.-Y.; Kang, D. Association of paternal age at birth and the risk of breast cancer in offspring: A case control study. BMC Cancer 2005, 5, 143. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.; Han, B.-G.; KoGES Group. Cohort profile: The Korean Genome and Epidemiology Study (KoGES) Consortium. Int. J. Epidemiol. 2017, 46, e20. [Google Scholar] [CrossRef]
- Brewer, H.R.; Jones, M.E.; Schoemaker, M.J.; Ashworth, A.; Swerdlow, A.J. Family history and risk of breast cancer: An anal-ysis accounting for family structure. Breast Cancer Res. Treat. 2017, 165, 193–200. [Google Scholar] [CrossRef] [Green Version]
- Shah, M.; Zhu, K.; Palmer, R.C.; Jatoi, I.; Shriver, C.; Wu, H. Breast, colorectal, and skin cancer screening practices and family history of cancer in U.S. women. J. Womens Health 2007, 16, 526–534. [Google Scholar] [CrossRef]
- Braithwaite, D.; Miglioretti, D.L.; Zhu, W.; Demb, J.; Trentham-Dietz, A.; Sprague, B.; Tice, J.; Onega, T.; Henderson, L.M.; Buist, D.S.M.; et al. Family History and Breast Cancer Risk Among Older Women in the Breast Cancer Surveillance Consortium Cohort. JAMA Intern. Med. 2018, 178, 494–501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kang, E.; Seong, M.-W.; Park, S.K.; Lee, J.W.; Lee, J.; Kim, L.S.; Lee, J.E.; Kim, S.Y.; Jeong, J.; Han, S.A.; et al. The prevalence and spectrum of BRCA1 and BRCA2 mutations in Korean population: Recent update of the Korean Hereditary Breast Cancer (KOHBRA) study. Breast Cancer Res. Treat. 2015, 151, 157–168. [Google Scholar] [CrossRef] [PubMed]
- Han, S.-A.; Kim, S.-W.; Kang, E.; Park, S.K.; Ahn, S.-H.; Lee, M.H.; Nam, S.-J.; Han, W.; Bae, Y.T.; Kim, H.-A.; et al. The prevalence of BRCA mutations among familial breast cancer patients in Korea: Results of the Korean Hereditary Breast Cancer study. Fam. Cancer 2013, 12, 75–81. [Google Scholar] [CrossRef]
- Claus, E.B.; Risch, N.; Thompson, W.D. Autosomal dominant inheritance of early-onset breast cancer. Implications for risk prediction. Cancer 1994, 73, 643–651. [Google Scholar] [CrossRef]
- Lord, C.J.; Ashworth, A. The DNA damage response and cancer therapy. Nat. Cell Biol. 2012, 481, 287–294. [Google Scholar] [CrossRef] [PubMed]
- Oeffinger, K.C.; Fontham, E.T.; Etzioni, R.; Herzig, A.; Michaelson, J.S.; Shih, Y.-C.T.; Water, L.C.; Church, T.R.; Flowers, C.R.; LaMonte, S.J.; et al. Breast cancer screening for women at average risk: 2015 guideline update from the American Cancer Society. JAMA 2015, 314, 1599–1614. [Google Scholar] [CrossRef]
- Bevers, T.B.; Ward, J.H.; Arun, B.K.; Colditz, G.A.; Cowan, K.H.; Daly, M.B.; Garber, J.E.; Gemignani, M.L.; Gradishar, W.J.; Jordan, J.A.; et al. Breast Cancer Risk Reduction, Version 2.2015. J. Natl. Compr. Cancer Netw. 2015, 13, 880–915. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- White, M.C.; Soman, A.; Weinberg, C.R.; Rodriguez, J.L.; Sabatino, S.A.; Peipins, L.A.; DeRoo, L.; Nichols, H.B.; Hodgson, M.E.; Sandler, D.P. Factors associated with breast MRI use among women with a family history of breast cancer. Breast J. 2018, 24, 764–771. [Google Scholar] [CrossRef]
- Piccinin, C.; Panchal, S.; Watkins, N.; Kim, R.H. An update on genetic risk assessment and prevention: The role of genetic testing panels in breast cancer. Expert Rev. Anticancer. Ther. 2019, 19, 787–801. [Google Scholar] [CrossRef] [PubMed]
- Bevers, T.B.; Helvie, M.; Bonaccio, E.; Calhoun, K.E.; Camp, M.; Daly, M.B.; Lehman, C.D.; Farrar, W.B.; Garber, J.E.; Gray, R.; et al. Breast Cancer Screening and Diagnosis, Version 1. 2019. Available online: https://www.nccn.org/professionals/physician_gls/pdf/breast-screening.pdf (accessed on 6 April 2020).
- Acheson, L.S. Recording, interpreting, and updating the family history of cancer: Implications for cancer prevention. JAMA 2011, 306, 208–210. [Google Scholar] [CrossRef] [PubMed]
- Nindrea, R.D.; Aryandono, T.; Lazuardi, L.; Dwiprahasto, I. Family History of Breast Cancer and Breast Cancer Risk between Malays Ethnicity in Malaysia and Indonesia: A Meta-Analysis. Iran. J. Public Heal. 2019, 48, 198–205. [Google Scholar] [CrossRef]
- Ziogas, A.; Horick, N.K.; Kinney, A.; Lowery, J.T.; Domchek, S.M.; Isaacs, C.; Griffin, C.A.; Moorman, P.G.; Edwards, K.L.; Hill, D.A.; et al. Clinically Relevant Changes in Family History of Cancer Over Time. JAMA 2011, 306, 172–178. [Google Scholar] [CrossRef] [Green Version]
- Saslow, D.; Boetes, C.; Burke, W.; Harms, S.; Leach, M.O.; Lehman, C.D.; Morris, E.; Pisano, E.; Schnall, M.; Sener, S.; et al. American Cancer Society Guidelines for Breast Screening with MRI as an Adjunct to Mammography. CA A Cancer J. Clin. 2007, 57, 75–89. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Variable | Total Participants | p | |
|---|---|---|---|
| Breast Cancer | Control | ||
| Total Number (n, %) | 981 (100.0) | 128,393 (100.0) | |
| Age (year) | 54.2 ± 7.5 | 53.4 ± 8.5 | n.s |
| Income (n, %) | <0.001 † | ||
| No information | 145 (14.8) | 26,826 (20.9) | |
| Lowest | 227 (23.1) | 28,348 (22.1) | |
| Middle | 289 (29.5) | 32,927 (25.6) | |
| Highest | 320 (32.6) | 40,292 (31.4) | |
| Hypertension (n, %) | n.s | ||
| Yes | 165 (16.8) | 24,417 (19.0) | |
| No | 816 (83.2) | 103,976 (81.0) | |
| Diabetes (n, %) | n.s | ||
| Yes | 67 (6.8) | 7379 (5.7) | |
| No | 914 (93.2) | 121,014 (94.3) | |
| Dyslipidemia (n, %) | n.s | ||
| Yes | 100 (10.2) | 11,011 (8.6) | |
| No | 881 (89.8) | 117,382 (91.4) | |
| Pregnancy (n, %) | 0.001 † | ||
| Yes | 934 (95.2) | 124,613 (97.1) | |
| No | 47 (4.8) | 3780 (2.9) | |
| Menopause (n, %) | <0.001 † | ||
| Yes | 835 (85.1) | 79,748 (62.1) | |
| No | 146 (14.9) | 48,645 (37.9) | |
| BMI (kg/m2) | 23.5 ± 2.9 | 23.8 ± 3.0 | n.s |
| Smoking (pack-year) | 0.22 ± 2.12 | 0.56 ± 3.57 | <0.001 * |
| Alcohol (g/day) | 0.66 ± 3.71 | 1.81 ± 7.75 | <0.001 * |
| Family history of mother (n, %) | <0.001 † | ||
| Breast cancer | 12 (1.2) | 546 (0.4) | |
| No breast cancer | 969 (98.8) | 127,847 (99.6) | |
| Family history of sibling (n, %) | <0.001 † | ||
| Breast cancer | 33 (3.4) | 1519 (1.2) | |
| No breast cancer | 948 (96.6) | 126,874 (98.8) | |
| Variable | Odds Ratio of Breast Cancer | |||||||
|---|---|---|---|---|---|---|---|---|
| Crude | p | Model 1 | p | Model 2 | p | Model 3 | p | |
| Family History of a Mother with Breast Cancer | ||||||||
| Breast cancer | 2.90 (1.63–5.16) | <0.001 * | 3.21 (1.80–5.74) | <0.001 * | 2.78 (1.56–4.94) | 0.001 * | 3.12 (1.75–5.59) | <0.001 * |
| Control | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| Family history of a sibling with breast cancer | ||||||||
| Breast cancer | 2.91 (2.05–4.13) | <0.001 * | 2.66 (1.87–3.78) | <0.001 * | 2.86 (2.02–4.07) | <0.001 * | 2.63 (1.85–3.74) | <0.001 * |
| Control | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| Variable | Odds Ratio of Breast Cancer | p |
|---|---|---|
| Model 4 | ||
| Family history of maternal breast cancer | 2.56 (1.36–4.79) | 0.003 * |
| Family history of sibling breast cancer | 2.78 (1.94–4.00) | <0.001 * |
| Family history of maternal and sibling breast cancer | 1.99 (0.39–10.13) | 0.406 |
| Variable | Odds Ratio of Breast Cancer | |||||||
|---|---|---|---|---|---|---|---|---|
| Crude | p | Model 1 | p | Model 2 | p | Model 3 | p | |
| Menopause (n = 80,583) | ||||||||
| Family history of a mother with breast cancer | ||||||||
| Breast cancer | 2.86 (1.35–6.09) | 0.006 * | 2.56 (1.20–5.47) | 0.015 * | 2.78 (1.30–5.91) | 0.008 * | 2.50 (1.17–5.35) | 0.018 * |
| Control | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| Family history of a sibling with breast cancer | ||||||||
| Breast cancer | 2.68 (1.83–3.93) | <0.001 * | 2.54 (1.73–3.73) | <0.001 * | 2.66 (1.82–3.90) | <0.001 * | 2.53 (1.72–3.71) | <0.001 * |
| Control | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| No menopause (n = 48,791) | ||||||||
| Family history of a mother with breast cancer | ||||||||
| Breast cancer | 5.51 (2.24–13.54) | <0.001 * | 5.23 (2.12–12.89) | <0.001 * | 5.18 (2.10–12.78) | <0.001 * | 4.93 (1.99–12.20) | 0.001 * |
| Control | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| Family history of a sibling with breast cancer | ||||||||
| Breast cancer | 3.42 (1.39–8.37) | 0.007 * | 3.36 (1.37–8.23) | 0.008 * | 3.17 (1.29–7.81) | 0.012 * | 3.13 (1.27–7.72) | 0.013 * |
| Control | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| Variable | Onset of Breast Cancer | p | |
|---|---|---|---|
| <50 years | ≥50 years | ||
| Family history of a mother with breast cancer (n, %) | |||
| Yes | 8 (1.4) | 4 (1.0) | 0.771 * |
| No | 573 (98.6) | 387 (99.0) | |
| Family history of a sibling with breast cancer (n, %) | |||
| Yes | 19 (3.3) | 14 (3.6) | 0.793 † |
| No | 562 (96.7) | 377 (96.4) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, H.G.; Park, J.H.; Choi, Y.J.; Suh, Y.J. Association of Family History with the Development of Breast Cancer: A Cohort Study of 129,374 Women in KoGES Data. Int. J. Environ. Res. Public Health 2021, 18, 6409. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18126409
Choi HG, Park JH, Choi YJ, Suh YJ. Association of Family History with the Development of Breast Cancer: A Cohort Study of 129,374 Women in KoGES Data. International Journal of Environmental Research and Public Health. 2021; 18(12):6409. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18126409
Chicago/Turabian StyleChoi, Hyo Geun, Jung Ho Park, Yeon Ju Choi, and Yong Joon Suh. 2021. "Association of Family History with the Development of Breast Cancer: A Cohort Study of 129,374 Women in KoGES Data" International Journal of Environmental Research and Public Health 18, no. 12: 6409. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18126409