1. Introduction
The masticatory system is defined as a functional complex characterized by a multitude of components including bones, teeth, soft tissues, muscles, tendons, ligaments, and discs [
1]. Two temporomandibular joints enable the motion of the mandible within a range of six degrees of movements (translation along and rotation around three mutually perpendicular axes) [
1,
2]. The motion of the mandible triggers the coactivation of 16 groups of mandibular muscles, which results in cumulative force interplay within the teeth [
2]. Hypothetically, there are unlimited patterns of muscle coactivation to provide a desired occlusal load or jaw movement [
2]. In fact, repeated occlusal contacts and jaw movements remain in accordance with regular motor command paths created by the brain stem during function (central pattern generator) [
2,
3].
Dental occlusion reflects unique information contained in a center in the brain, specialized in summation and integration of neurological signaling originating from periodontal, dental, and soft tissue receptors. This complex is permanently controlled by the central nervous system (CNS) to adjust and improve mandible position and motion in accordance with peripheral inputs [
4,
5]. Within this system, there is sensorimotor neuroplasticity, which largely determines individual adaptation to occlusal and oral changes resulting from dental treatments [
5].
The relationship between dental occlusion and temporomandibular disorders (TMDs) still remains controversial, inconclusive, and not fully examined [
5,
6,
7]. Currently, etiological factors are based mainly on behavioral, psychological, and neurological components [
6]. Diagnostic Criteria for Temporomandibular Disorders (DC/TMD) provide an appropriate, valid, and reliable clinical tool to perform differential diagnosis with respect to physical and biopsychosocial condition (Axes I and II, respectively) [
5,
8,
9,
10,
11]. This protocol creates a modern approach to the etiology of TMDs. Treatment modalities for TMDs include pharmacotherapy (e.g., analgesics, non-steroidal anti-inflammatory drugs, anxiolytics, anti-depressants, Imotun, CBD), occlusal appliances, counseling, physical therapy, manual therapy, therapeutic exercises, arthroscopy, arthrocentesis, joint injections of hyaluronic acid, and muscle injections of botulinum toxin [
12,
13,
14,
15,
16,
17,
18].
The latest physiological concept considers the temporomandibular complex from the perspective of biotensegrity. According to this theory, the mandible is suspended within a tensioned network, which spreads out anatomically much further than usually assumed [
19]. Furthermore, in this biological interface, it is anatomical structures that are primarily responsible for motion control. This evolutionarily conditioned system enables a quick response to functional changes and provides a more coherent model of joint physiology [
19]. Biotensegrity interplays with elastic deformation of the bone. Under functional loading, the human mandible demonstrates flexible biomechanical behavior, which results in the flexion at the site of symphysis, entailing the reduction of the distance between left and right mandibular ramus and thus leads to a close-up of the lateral segments of the lower dental arch [
20]. It is also well known that dynamic loading implicates the bone metabolic activity. During speech, masticatory muscles trigger stress effect throughout the mandible [
21]. It is assumed that loading frequency while speaking may be from three to five times greater than that of mastication [
21]. Considering anatomical relationships and biomechanical condition of the mandible, the highest strains arising from speech activity probably occurs within the chin [
21]. This suggests that speech creates a stress pattern that triggers bone modeling, mainly in the anterior part of the mandible [
21].
Biological systems based on biotensegrity are characterized by a high level of resiliency to external disturbances. Through appropriate changes in tension/compression distribution, they maintain a balance between self-stabilization and immediate ability to respond to the load affecting them during every motion. Biotensegrity could be defined as a global balance between compressional and tensional forces—“the balance of unseen forces” [
19]. It represents internal stability of any system of forces embedded in nature [
22].
In the light of the above, it may be concluded that the condition of the temporomandibular joint as well as the entire masticatory system is presumably modulated by the variability of tension/compression distribution. Each part of the masticatory system contributes to its kinematic behavior with superior control from the nervous system. The main clinical point is that, according to the theory of biotensegrity, compressional forces are not directly transferred through the condyle, disc, and glenoid fossa. This approach remains in contrast to the classical theory of the third-class levers supported by the force-vector dependence [
23]. The standard mechanical theory follows typical linear stress-strain curves. For tensegrity and living tissues, the non-linear dynamics is assigned [
24].
These two perspectives may mirror controversies in recognizing dental occlusion as a potential risk factor in the development of TMDs and reporting research discrepancies. It is possible that changes within anatomical structures (disc perforation, erosion, degeneration) appear when a certain level of resiliency to external disturbances in biotensegrity-related systems is exceeded (cut-off point in the non-linear curve). This could suggest a direct link between occlusion and TMDs. Disturbances of self-regulation result in decompensation, i.e., loss of homeostasis. In conclusion, biotensegrity provides balance—enormous potential adaptation and compensation in one—and research findings depend on the advancement level of the captured changes.
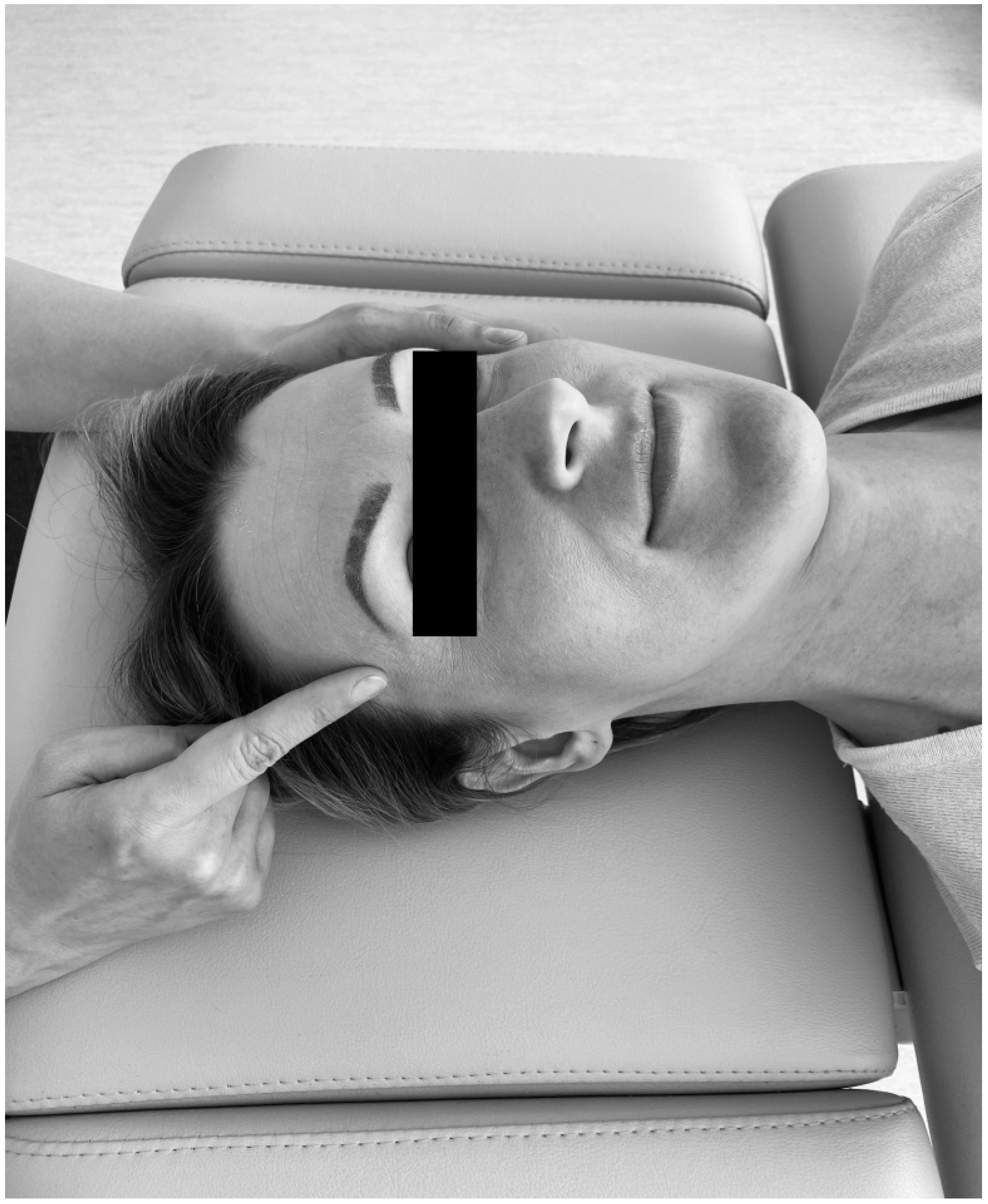
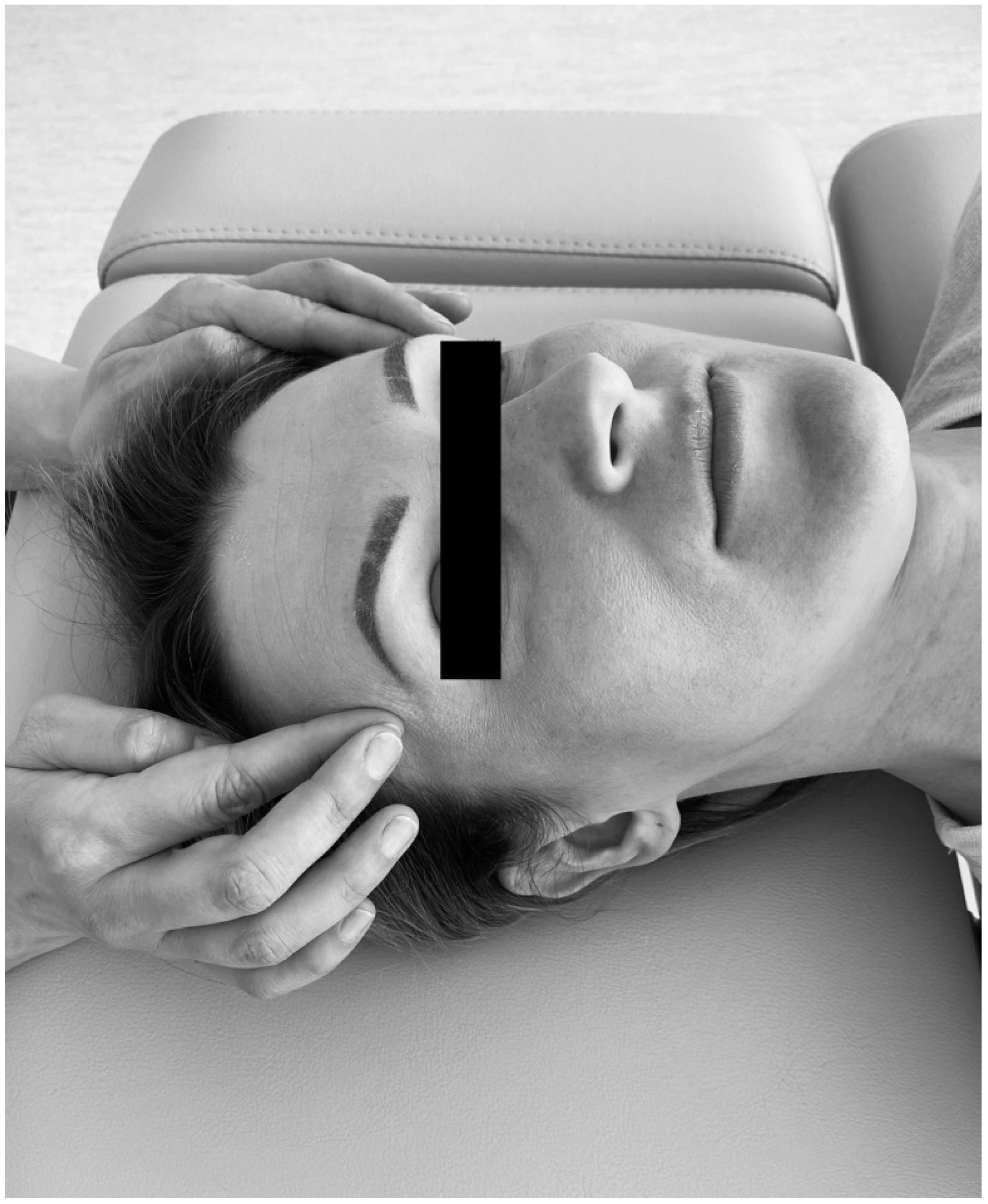
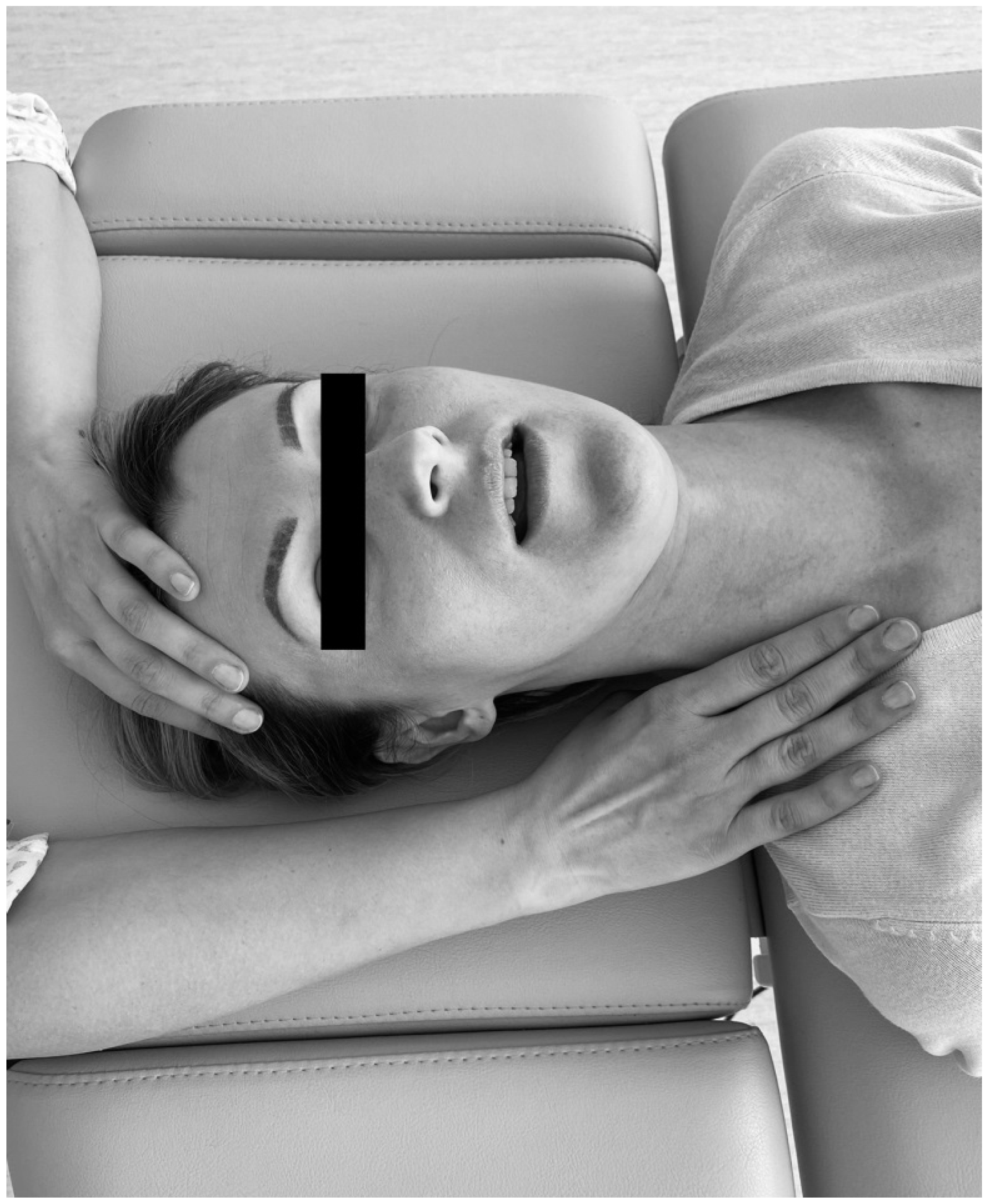
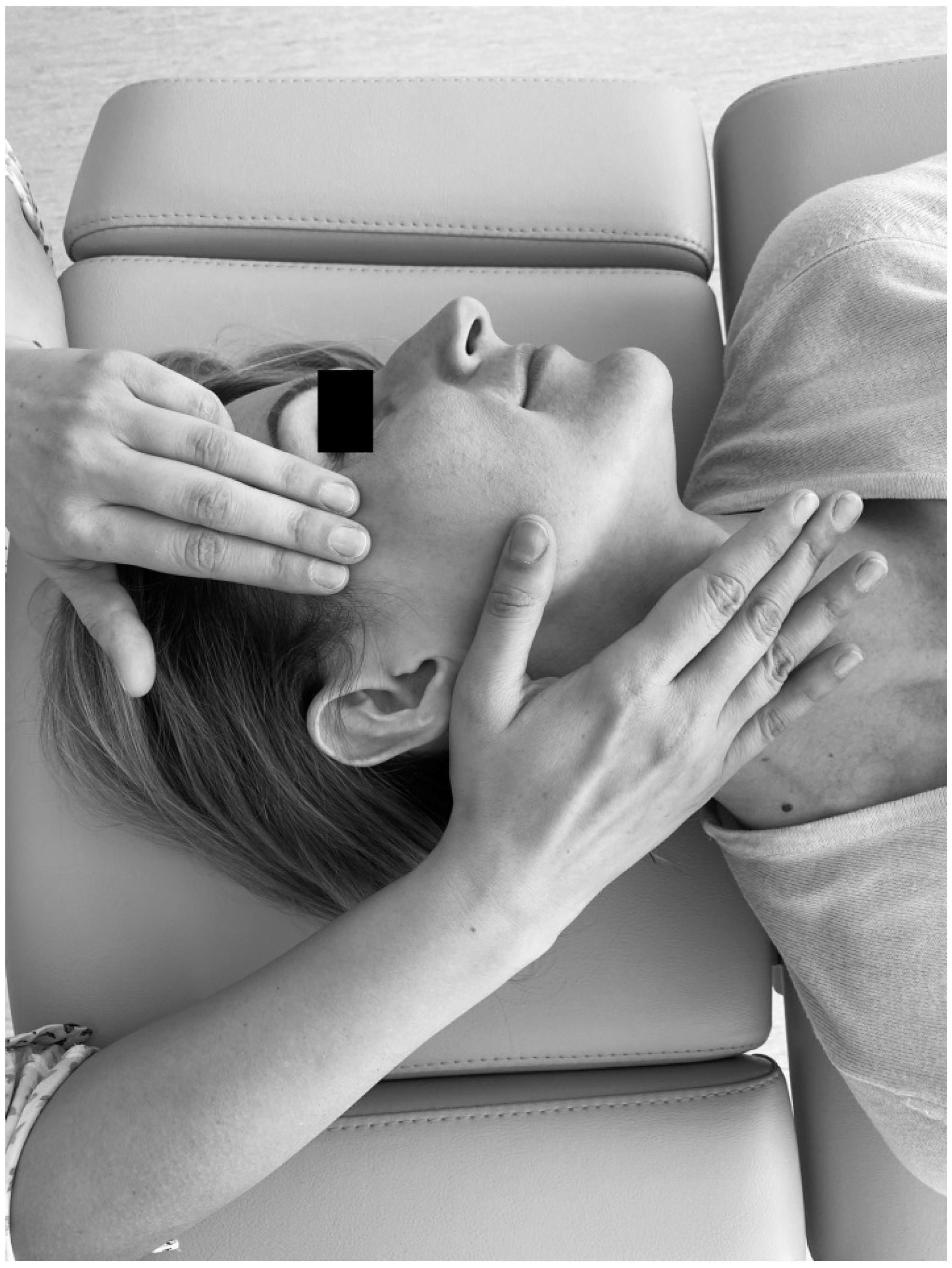
Considering that soft tissue mobilization is a kind of external load, which leads to the release of tension and stress of myofascial components, achievement of new balance between tensional and compressional forces and changes in myofascial force distribution in a non-invasive manner, and remembering that soft tissue mobilization is closely linked to biotensegrity, it was hypothesized that there is at least one significant difference between pre- and post-treatment values of occlusal parameters in patients with temporomandibular disorder—myofascial pain with referral. As a dysfunction of multifactorial nature, myofascial pain with referral is always related with trigger points of the head and neck. This condition reflects a combination of sensory experiences, motor reactions, and autonomic symptoms, including local and referred pain [
25,
26,
27].
The primary aim of the study was to evaluate occlusal parameters as cofactors of the existing TMDs in patients with myofascial pain with referral.
The second objective was to assess the influence of soft tissue mobilization on occlusion time, disclusion time, and occlusal loads.
3. Results
Before the first treatment, the average occlusion time (OT) in the entire study group (
n = 50) was 0.191 s (
Table 1). The values of the right and left disclusion times (TDR, TDL) were comparable and amounted to 0.209 s and 0.214 s, respectively. After the first mobilization, the OT dropped to 0.151 s. A similar decreasing tendency was observed after the second and third therapy (
Table 1). The first soft tissue mobilization shortened TDR and TDL to 0.181 s and 0.185 s, respectively. After the third treatment, the mean occlusion time in the entire study group was 0.119 s. In the case of TDR and TDL, the values were similar and amounted to 0.159 s and 0.165 s, respectively (
Table 1).
The Friedman test for the entire study group indicated that soft tissue mobilization altered the occlusion time (OT) and both disclusion times (TDR, TDL) (
p < 0.05) (
Table 1). The value of Kendall’s W coefficient was at least 0.12. For the occlusion time, this parameter oscillated around 0.28.
The Dunn–Bonferroni test revealed that in the occlusion time, there were statistically significant differences before and after the first treatment, before the first and after the second therapy, as well as before the first and after the third soft tissue mobilization (
p < 0.05 adjusted to the Bonferroni correction) (
Table 1). In the case of the right disclusion time, statistically significant differences were observed before the first and after the second mobilization as well as before the first and after the third soft tissue mobilization (
p < 0.05 adjusted to the Bonferroni correction). The left disclusion time differed only in comparison with the first and third treatment (
Table 1).
In the group of women (
n = 37), the average occlusion time was 0.182 s before the first treatment (
Table 2). The values of the right and left disclusion times (TDR and TDL, respectively) were similar and amounted to 0.200 s and 0.206 s, respectively. After the first soft tissue mobilization, the OT was reduced to 0.152 s. An analogous decreasing tendency was observed after the second and third therapy (
Table 2). The first soft tissue mobilization reduced TDR and TDL to 0.186 s and 0.187 s, respectively. After the third treatment, the mean occlusion time in the entire study group was 0.115 s. In the case of TDR and TDL, the values amounted to 0.152 s and 0.161 s, respectively (
Table 2).
The Friedman test revealed statistically significant differences among the mean ranks of the occlusion time (OT) and both disclusion times (TDR, TDL) (
p < 0.05) (
Table 2).
The Dunn–Bonferroni test revealed that in the occlusion time, there were statistically significant differences before and after the first treatment, before the first and after the second therapy, as well as before the first and after the third soft tissue mobilization (
p < 0.05 adjusted to the Bonferroni correction) (
Table 2). In the case of the right disclusion time, statistically significant differences were reported before the first and after the second mobilization as well as before the first and after the third soft tissue mobilization (
p < 0.05 adjusted to the Bonferroni correction). With respect to the left disclusion time, there were no statistically significant differences observed before the first and after the first, second and third soft tissue mobilizations, respectively (
p > 0.05) (
Table 2).
Before the first treatment, in the group of men (
n = 13), the average occlusion time was 0.216 s (
Table 3). The right and left disclusion times (TDR, TDL) were comparable and amounted to 0.236 s and 0.239 s, respectively. After the first soft tissue mobilization, the OT decreased to 0.145 s. A similar decreasing tendency was observed after the second and third therapy (
Table 3). The first treatment reduced TDR and TDL to 0.165 s and 0.182 s, respectively. After the third soft tissue mobilization, the mean occlusion time in the male group was 0.129 s. In the case of TDR and TDL, the values amounted to 0.180 s and 0.177 s, respectively (
Table 3).
The Friedman test revealed statistically significant differences among the mean ranks of the occlusion time (OT) and left disclusion time (TDL) (
p < 0.05) (
Table 3).
The Dunn–Bonferroni test demonstrated that only in the occlusion time, there were statistically significant differences before and after the first treatment, before the first and after the second therapy, as well as before the first and after the third soft tissue mobilization (
p < 0.05 adjusted to the Bonferroni correction) (
Table 3). With respect to the right and left disclusion times, there were no statistically significant differences before the first and after the first, second, and third soft tissue mobilizations, respectively (
p > 0.05) (
Table 3).
There were no statistically significant differences between females and males in terms of TO, TDR, and TDL at every stage of the research (
p > 0.05) (
Table 4).
Before the first soft tissue mobilization, the average occlusal load on the left side of both dental arches in the entire study group was 52.8%, and on the right side it was 47.2%. After the first, second, and third therapy, the distribution of the load was comparable to the initially registered values (
Table 5). There was no statistically significant influence of soft tissue mobilization on the occlusal load distribution (
p > 0.05) (
Table 5). Similar trends were observed in the case of both the group of women and men (
Table 6 and
Table 7).
There were no statistically significant differences between females and males in terms of occlusal load distribution (%) in maximal intercuspation at every stage of the research (
p > 0.05) (
Table 8).
4. Discussion
Supporting systems in animal and vegetal bodies tend to receive and create forces (with external or internal origin) which cancel each other out, with the result equal to zero. It allows to restore the original anatomical structure [
22]. This phenomenon reflects excellent force distribution based on the theory of biotensegrity [
22]. Within this concept, the possibility of returning to original shape after being subject to force loading is determined by structural and functional balance. Changes introduced to the structure under the influence of forces result in a new design, new balance of forces, and thus new tensegrity [
22].
Dental tensegrity can be evaluated from numerous perspectives—of one tooth, certain groups of teeth, a dental arch, or across the face [
22]. The tensegrity of the dental arch is provided by interproximal surfaces, proper occlusion, biological forces including the occlusal load, activity of the cheeks, lips and other soft tissues, adaptive and functional bone remodeling, and age-related growth vectors originating from functional and esthetic adaptations [
22].
Soft tissue mobilization offers a kind of an external load, which can lead to transient disturbances of myofascial components and tensegrity in one. As a consequence of myofascial release, changes in dental force distribution as well as improvement in movements of the mandible can be expected. This type of physiotherapeutic treatment may enable specialists to reach new balance between compressional and tensional forces.
In the presented study, soft tissue mobilization contributed to the reduction of the occlusion time (TO) as well as the right and left disclusion times (TDR, TDL) (
Table 1,
Table 2 and
Table 3). Both before and after the treatment, occlusal parameters oscillated within the reference values (OT < 0.2 s, TDR < 0.4 s, TDL < 0.4 s) (
Table 1,
Table 2 and
Table 3).
Changes of the occlusal parameters, induced by soft tissues mobilization, are probably triggered by relieving the tension and stress of the associated masticatory muscles and fascia [
32]. As a consequence, the freedom and quality of motion as well as the range of eccentric movements of the mandible may improve. Moreover, the aspect of neuromuscular facilitation attributed to the repeated registrations of T-scan III cannot be excluded. Coordinated, regular movements of the mandible could influence the resetting and restoration of compressional and tensional forces within the myofascial system with all occlusal consequences. This phenomenon appears to be analogous to deprogramming and creating new muscle engrams [
33,
34]. T-scan III might prove useful in clinical procedures as an occlusal biofeedback [
35,
36]. This may be of great importance in the case of people who, due to occlusal reasons, have consciously changed their chewing pattern (one-sided chewing, bypassing selected anatomical units in the chewing cycle) and, consequently, overload the structures of the masticatory system. In some cases, occlusal equilibration may be necessary [
37,
38,
39].
Peck et al. highlighted that in patients with acute inflammation and pain of the temporomandibular joint, attention should be paid to reducing jaw function rather than changing the occlusal scheme [
2]. Furthermore, these authors stressed that the compression of the temporomandibular joint is the norm, which will not be altered by modification of the occlusal scheme [
2]. Such an approach might stem from a hidden nature of biotensegrity. The above-mentioned soft tissue mobilization and occlusal biofeedback may be implemented as an alternative in some TMDs and pain management, leading to the establishment of new compressional/tensional force distribution and muscle engrams. This could possibly alleviate the patients’ symptoms and signs.
Other considerations indicate that remodeling capacity within the masticatory system facilitates adaptation to most occlusal functions and dysfunctions [
6]. It seems to mirror the non-linear dynamics of a stress/strain curve, which is dedicated to tensegrity and living tissues [
24]. Currently, there is insufficient evidence that occlusal adjustments may help to prevent or control TMDs. It is possible that there is no justification for occlusal corrections for the management or prevention of TMD [
40]. This suggestion could be confirmed by the results of our research, in which, despite the existing TMDs–myofascial pain with referral, the obtained results for occlusal parameters remained at the level of reference values. It should be emphasized that the occlusion time is strongly associated with maximum intercuspation defined as the highest number of occlusal contacts. This position provides the most suitable occlusal load transfer, i.e., through the long axis of the teeth [
41]. During the clenching, maximal intercuspation enables the most favorable dissipation of occlusal forces [
41]. It is in line with the theory of biotensegrity [
22] and imitates load dispersion similar to the Newton’s cradle steel balance. In the presented study, soft tissue mobilization seems to have optimized the activation timing of the muscles responsible for mandibular movements, thereby affecting the occlusion time in closure and disclusion time in lateral excursions. It is probable that the activation timing of individual muscle groups directly reflects the balance between compressional and tensional forces, indicating possible shifts in biotensegrity.
Sierpińska et al. reported that in patients with advanced tooth wear, prosthetic rehabilitation—including multipoint contacts and increased cuspal morphology—resulted in stability of the occlusal conditions [
41]. The high degree of force equality per arch half seems to play a crucial role. These authors indicated that changes of the vertical occlusal dimension lead to the improvement of the occlusion time and a lack of significant changes in the case of disclusion time [
41]. Furthermore, it has been evidenced that the activity of the masseter muscles is strongly positively associated with occlusal point contacts as compared to the flattener surface [
41,
42].
The lack of statistically significant differences in some TDR and TDL after first, second, or third mobilizations at certain stages of the study may indicate the lateralization of both occlusal and muscular disorders, clearly suggesting the direction of morphologically or/and functionally anchored dysfunction (
p > 0.05) (
Table 1,
Table 2 and
Table 3). Additional evaluation of the activity of the masticatory muscles responsible for lateral movements of the mandible might be necessary. This lateralization-related asymmetry passively distributes tension through muscle-fascial chains in the entire body. It could affect the human posture and reflect a general lack of equilibrium in individuals [
43].
The absence of statistically significant differences with respect to gender confirmed the homogeneity of the study group, as well as the coherent nature of neuromuscular dependence determined by occlusal conditions (
Table 4). The above-mentioned lateralization issues could be evidenced by the results concerning the occlusal load distribution (
Table 5,
Table 6 and
Table 7). In the entire study group as well as in the group of females and group of males, a greater concentration of occlusal forces was observed on the left side of clenched dental arches (
Table 5,
Table 6 and
Table 7). No statistically significant differences were observed with regard to gender (
Table 8). The asymmetry of occlusal force distribution may indicate that the source of dysfunction might be either a one-sided chewing pattern or one of disorders closely related to the lateralization of the so-called descending or ascending cranio-mandibular, homo- or heterolateral dysfunction [
44]. In such cases, T-scan III could be used as an occlusal biofeedback employed to facilitate engrams involved in bite dynamics. In this aspect, further research should be conducted on the possibilities of preserving the occlusal force center, force development, and movement of the center of force as well as the center of gravity [
45].
Proper dental occlusion facilitates chewing performance and adequate stimulation of the nervous system. Occlusion enables mastication, and mastication, in turn, determines sensory amplification. In the latest research, a direct link between mastication and cognitive function is strongly highlighted. This dependence is defined as the brain-stomatognathic axis [
46]. As a physiological process, mastication reflects a complex movement of a neuronal network, which affects some regions of the brain, including the prefrontal cortex [
47,
48,
49]. Typically, increased cortical blood flow is observed within the somatosensory and motor region, insular cortex, thalamus, corpus striatum, cerebellum, and hippocampus [
47]. Studies on animal models indicated that mastication can alter neuronal metabolism. In rats, molar dysfunction results in progressive loss of memory and learning ability, which suggests deficits in cognitive decline [
50,
51]. After multiple tooth loss, the subsequent rewiring, remapping, and rebuilding of the sensorimotor details in accordance with the originally determined neuromuscular pathways are impaired [
52,
53]. Occlusal disharmony leads to hippocampal morphological and functional disturbances [
46]. The activity of the hippocampus is conditioned by the noradrenergic, serotonergic, and dopaminergic innervation. Therefore, changes caused by occlusal disharmony may affect the function of the hippocampus. Some authors indicated that an increase in vertical occlusal dimension with acrylic by 0.1 mm results in changes within the central nervous system, which can accelerate involutional changes associated with the hippocampus-related cognitive function [
46]. According to recent considerations, food properties can also influence the afferent input signal in the central nervous system. A type of food determines chewing forces, vertical and lateral movements of the mandible, rate of masticatory cycles, and frequency of mastication [
54]. Organoleptic characteristics of the food are monitored by the brainstem. Food properties significantly affect the subjective perception and the so-called mouthfeel. A significant role is attributed to mechanical properties (elasticity, hardness, cohesiveness, breaking resistance), wetness (moisture, absorption, release of liquid), structure (granularity, softness, viscosity, graininess), chewing sensation (chewability, adhesion, stickiness, slipperiness, roughness, heaviness), and chewing experience (uniformity of the bite, uniformity of chewing, texture, overall uniformity, dryness) [
54]. The enormity of the related stimuli determines somatosensory amplification. Furthermore, the latest research revealed that the overall oral tactile acuity is increased in patients with painful TMD, which could suggest elevated vulnerability to occlusal alterations [
55]. Bucci et al. demonstrated that increased oral tactile acuity is treated as a risk factor connected with occlusal dysaesthesia under occlusal hypervigilance conditions which, in turn, are insufficient to trigger TMDs alone. These authors stressed that self-assessment by the patient is more important than the degree of somatosensation—“occlusal scanning” [
55].
Occlusally determined mastication might be a preventive factor against neurodegenerative disorders [
56]. It has been evidenced that tooth loss increases the risk of senile dementia or Alzheimer disorder [
46]. In an animal model of Alzheimer’s disease (rats), prolonged soft food diet resulted in decreased neuronal proliferation determined by the hippocampus as well as impaired memory and learning capacity [
46].
Bearing in mind the aforementioned dependencies and the fact that occlusion is currently perceived as a broader neurophysiological concept, prosthetic rehabilitation—as a global impact on the functioning of the human body—should involve anterior guidance, stable bilateral tooth contacts in maximum intercuspation and centric relation, proper distribution of contacts in maximum intercuspation, adequate axially directed occlusal forces, freedom of contact movements oscillating from maximum intercuspation, and lack of damaging intermaxillary contacts during lateral and protrusive movements [
2]. In the era of new clinical challenges, developing our knowledge about the neurophysiological model of mastication, constant evaluation of bite dynamics, as well as consideration of the masticatory organ in the context of biotensegrity seem to be issues of the utmost importance.
Strengths and Limitations of the Study
The presented research and other clinical studies based on DC/TMD will enable the selection of a homogeneous group of patients with respect to strictly defined research criteria. This, in turn, promotes a better understanding between scientists working on similar topics.
This is probably the first study on biotensegrity in the context of soft tissue mobilization in patients with temporomandibular joint disorders—myofascial pain with referral as well as the first research identifying the role and effect of soft tissue mobilization and tensegrity on occlusal parameters.
The applied clinical procedure has confirmed the possibility of using instrumental analysis in connection with a new independent research axis with respect to the DC/TMD. It should be highlighted that Axis III of the DC/TMD was designed for relevant biomarkers (quantitative sensory measures and genomic or molecular profiles), and axis IV was developed for the classification of the patients into clinically meaningful categories [
10].
The main advantage of the T-scan III system is the fact that it is a widely used, reproducible, and non-invasive method. The precision of each single registration includes the coverage factor 1.96 (measurement error). The overall accuracy (repeatability, reproducibility) of the subsequent measurements involves factor 2.77. In the case of the maximum total force measured, the error amounts to 1%, reliability is 2.8%, and accuracy reaches 2% [
57,
58].
Although in the presented study the tested occlusal parameters oscillated within reference values, there is a clinical need to perform another research in the future aimed at analyzing the individual biting dynamics for each case. It may demonstrate that the diagnosed myofascial pain with referral is closely correlated with the presence of even premature occlusal contact.
T-scan III does not consider biodynamics of mastication which—as shown above—is an important factor in the brain-stomatognathic system axis. Apart from occlusal parameters, patients should be tested for their chewing efficiency, mastication time, occlusal forces involved in chewing, and the time of contact between both dental arches. Perhaps a possibility of 24 h evaluation of the bite dynamics would enable us to assess the degree of somatosensation and somatosensory amplification.
Another limitation is the fact that there is no objective tool that would allow for direct monitoring of the changes in biotensegrity.








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}