
Developmental Hip Dysplasia: An Epidemiological Nationwide Study in Italy from 2001 to 2016

 ,
,  , ,
, , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
Statistics
3. Results
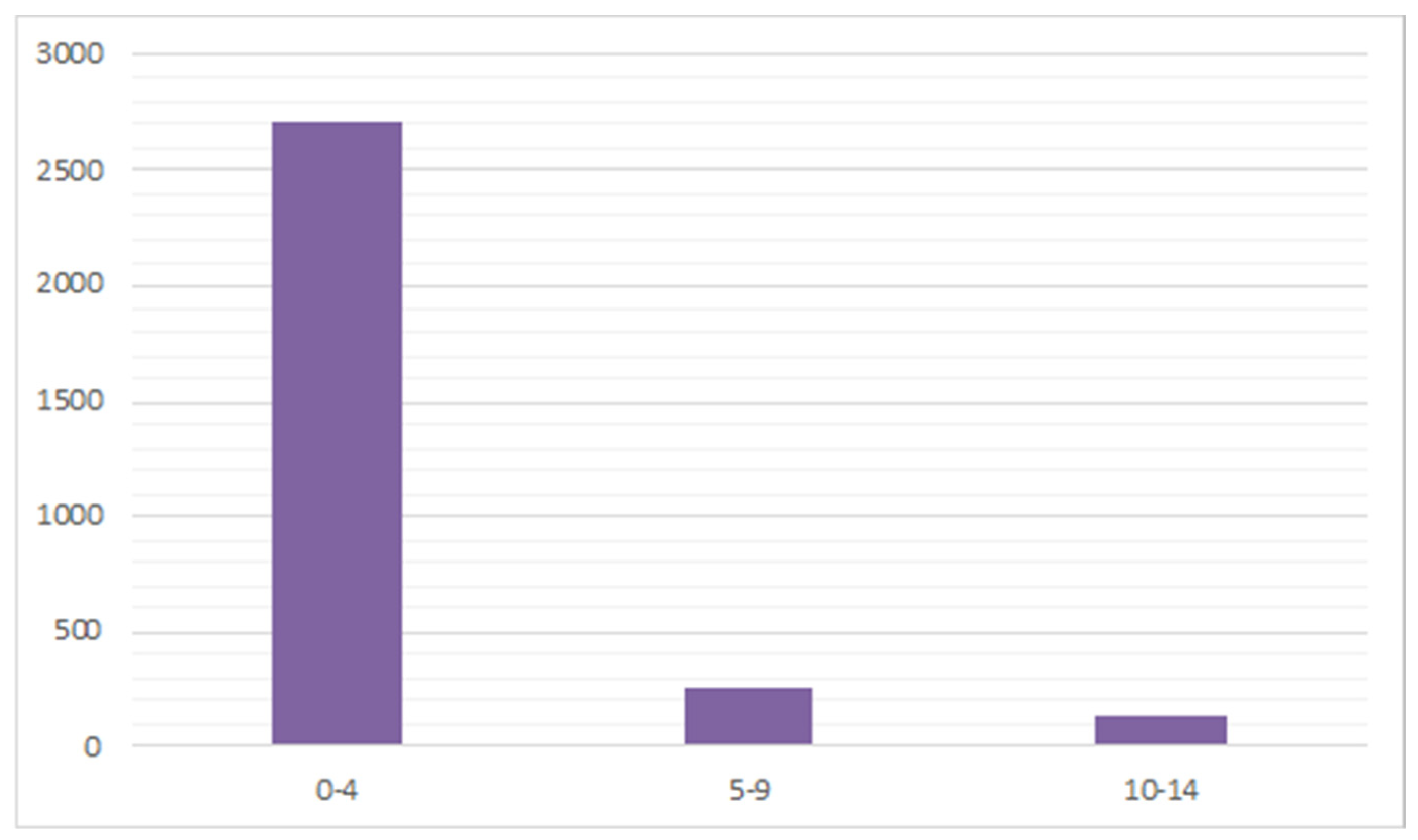
3.1. Demographics
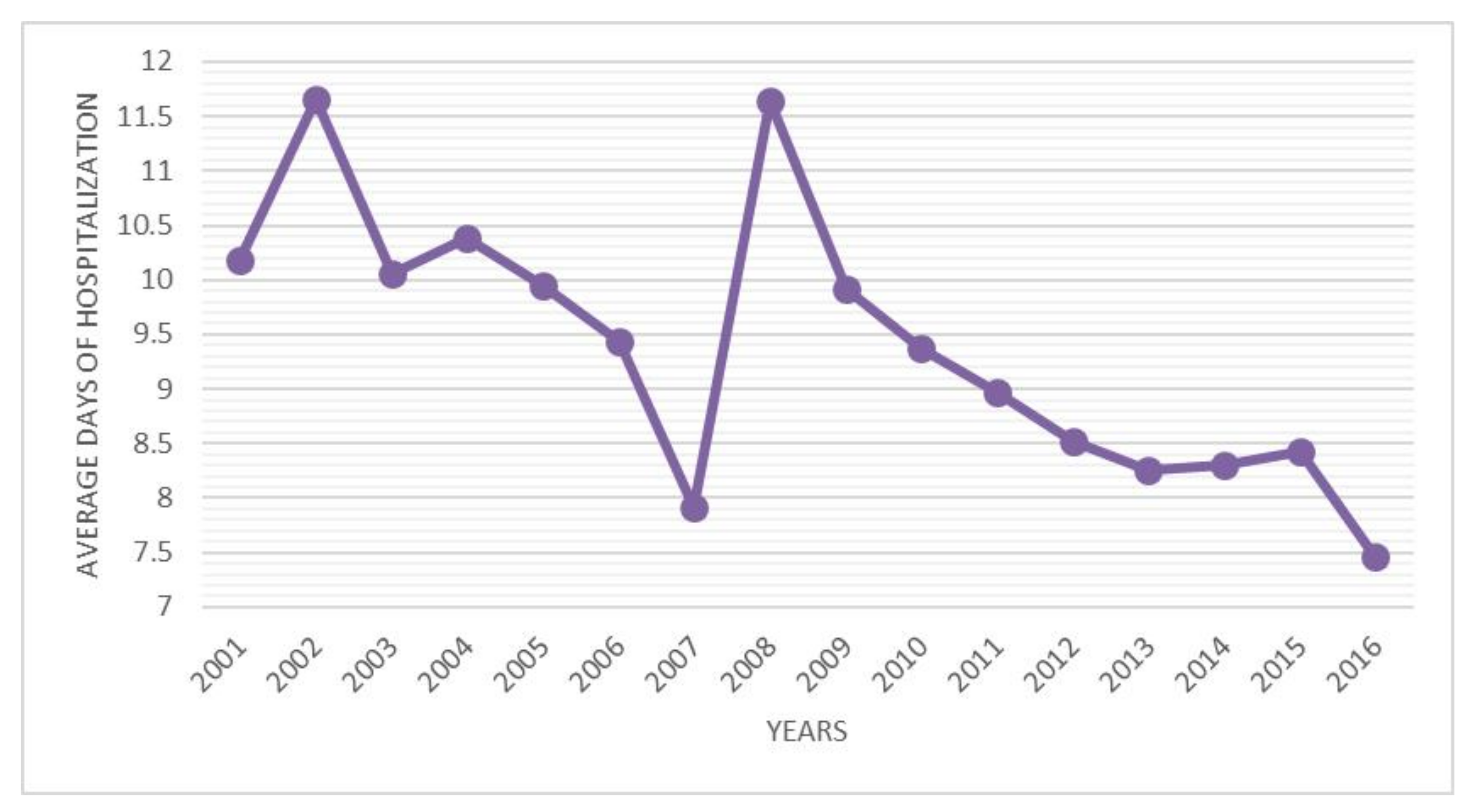
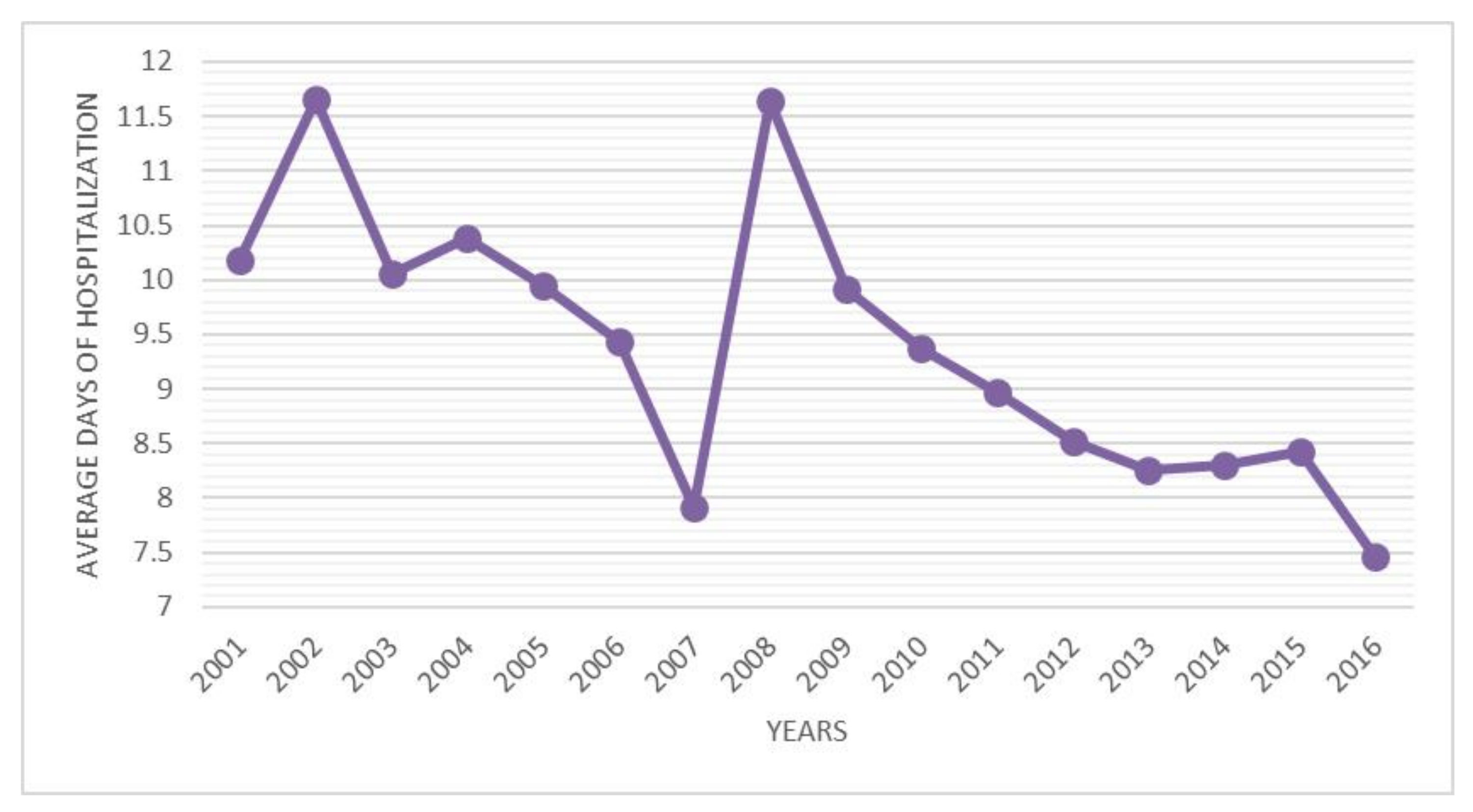
3.2. Days of Hospitalizations
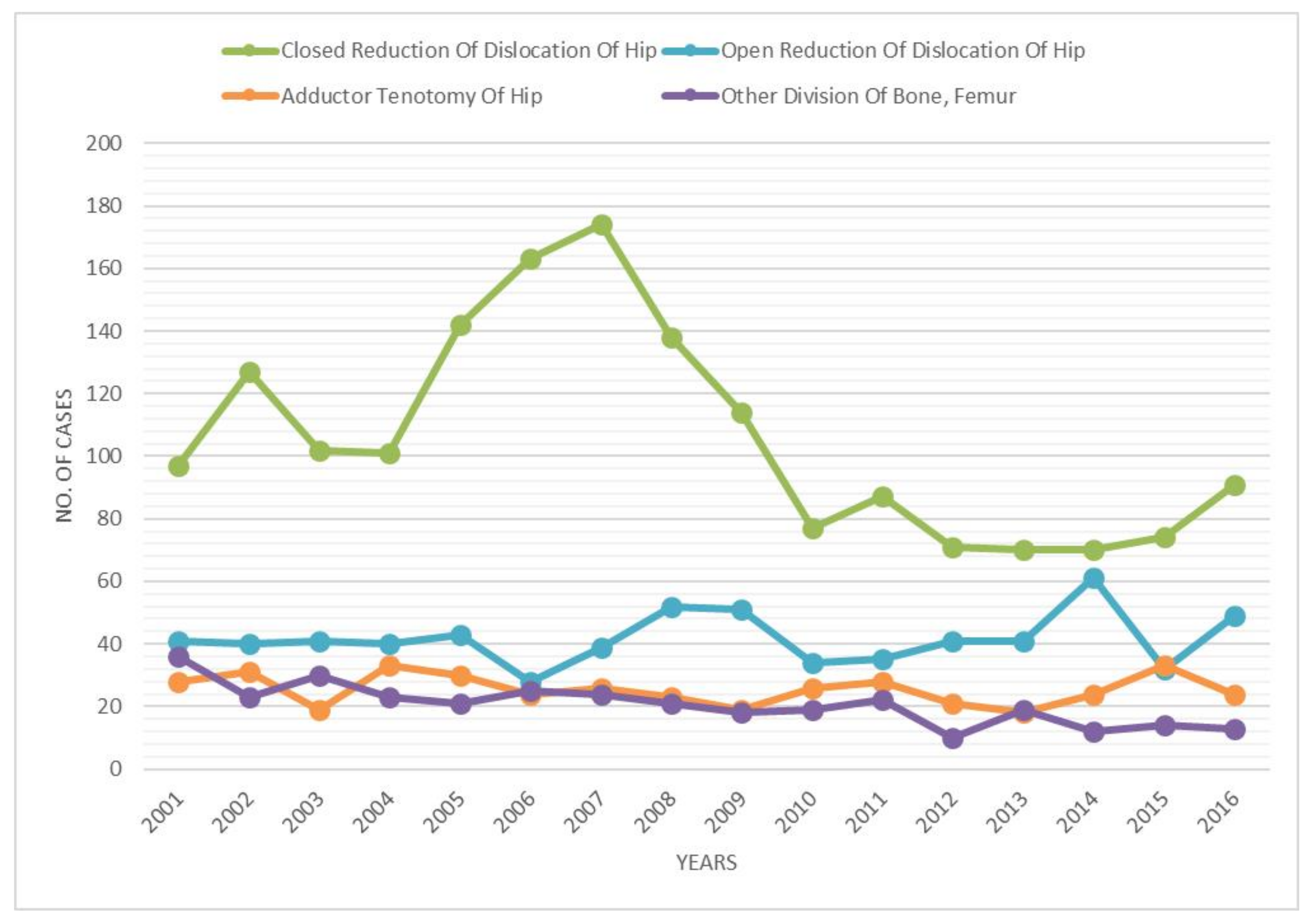
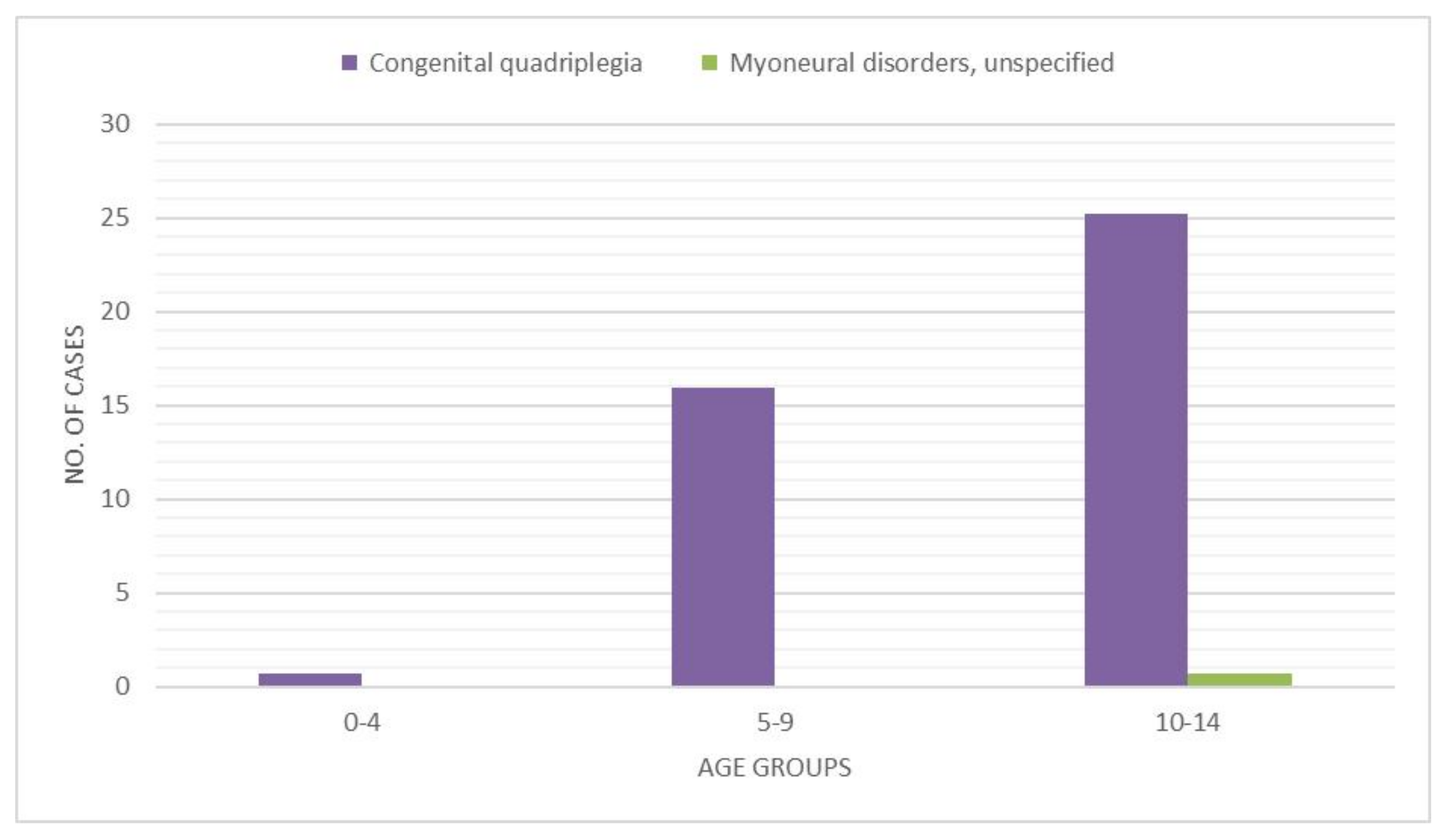
3.3. Procedure Performed and Admission Diagnosis Codes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Loder, R.; Skopelja, E. The Epidemiology and Demographics of Hip Dysplasia. ISRN Orthop. 2011, 2011, 238607. [Google Scholar] [CrossRef] [Green Version]
- Woodacre, T.; Ball, T.; Cox, P. Epidemiology of Developmental Dysplasia of the Hip within the UK: Refining the Risk Factors. J. Child. Orthop. 2016, 10, 633–642. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ortiz-Neira, C.L.; Paolucci, E.O.; Donnon, T. A Meta-Analysis of Common Risk Factors Associated with the Diagnosis of Developmental Dysplasia of the Hip in Newborns. Eur. J. Radiol. 2012, 81, e344–e351. [Google Scholar] [CrossRef] [PubMed]
- Desteli, E.E.; Pişkin, A.; Gülman, A.B.; Kaymaz, F.; Köksal, B.; Erdoǧan, M. Estrogen Receptors in Hip Joint Capsule and Ligamentum Capitis Femoris of Babies with Developmental Dysplasia of the Hip. Acta Orthop. Traumatol. Turc. 2013, 47, 158–161. [Google Scholar] [CrossRef]
- Schwend, R.M.; Shaw, B.A.; Segal, L.S. Evaluation and Treatment of Developmental Hip Dysplasia in the Newborn and Infant. Pediatr. Clin. N. Am. 2014, 61, 1095–1107. [Google Scholar] [CrossRef]
- Lipton, G.E.; Guille, J.T.; Altiok, H.; Bowen, J.R.; Harcke, H.T. A Reappraisal of the Ortolani Examination in Children with Developmental Dysplasia of the Hip. J. Pediatr. Orthop. 2007, 27, 27–31. [Google Scholar] [CrossRef] [PubMed]
- Shaw, B.A.; Segal, L.S.; SECTION ON ORTHOPAEDICS. Evaluation and Referral for Developmental Dysplasia of the Hip in Infants. Pediatrics 2016, 138. [Google Scholar] [CrossRef] [Green Version]
- Noordin, S.; Umer, M.; Hafeez, K.; Nawaz, H. Developmental Dysplasia of the Hip. Orthop. Rev. 2010, 2, e19. [Google Scholar] [CrossRef] [Green Version]
- Shipman, S.A.; Helfand, M.; Moyer, V.A.; Yawn, B.P. Screening for Developmental Dysplasia of the Hip: A Systematic Literature Review for the US Preventive Services Task Force. Pediatrics 2006, 117, e557–e576. [Google Scholar] [CrossRef] [Green Version]
- Graf, R. The Diagnosis of Congenital Hip-Joint Dislocation by the Ultrasonic Combound Treatment. Arch. Orthop. Trauma. Surg. 1980, 97, 117–133. [Google Scholar] [CrossRef]
- Fogarty, E.E.; Accardo, N.J.J. Incidence of Avascular Necrosis of the Femoral Head in Congenital Hip Dislocation Related to the Degree of Abduction During Preliminary Traction. J. Pediatr. Orthop. 1981, 1, 307–311. [Google Scholar] [CrossRef]
- Wicart, P.; Bocquet, A.; Gelbert, N.; Beley, G.; Proslier, R.; Pracos-Deffrenne, P.; Vie le Sage, F.; Assathiany, R.; Chapuis, M.; Fron, D.; et al. Congenital Dislocation of the Hip: Optimal Screening Strategies in 2014. Orthop. Traumatol. Surg. Res. OTSR 2014, 100, S339–S347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Biedermann, R.; Eastwood, D.M. Universal or Selective Ultrasound Screening for Developmental Dysplasia of the Hip? A Discussion of the Key Issues. J. Child. Orthop. 2018, 12, 296–301. [Google Scholar] [CrossRef]
- Treiber, M.; Korpar, B.; Sirše, M.; Merc, M. Early Neonatal Universal Ultrasound Screening for Developmental Dysplasia of the Hip: A Single Institution Observational Study. Int. Orthop. 2021, 45, 991–995. [Google Scholar] [CrossRef]
- Husum, H.-C.; Møller-Madsen, B.; Thomsen, J.L.; Maimburg, R.D.; Rahbek, O. Screening of dysplasia of the hip in Denmark. Ugeskr. Laeger 2021, 183, V05200371. [Google Scholar]
- O’Beirne, J.G.; Chlapoutakis, K.; Alshryda, S.; Aydingoz, U.; Baumann, T.; Casini, C.; de Pellegrin, M.; Domos, G.; Dubs, B.; Hemmadi, S.; et al. International Interdisciplinary Consensus Meeting on the Evaluation of Developmental Dysplasia of the Hip. Ultraschall Med. 2019, 40, 454–464. [Google Scholar] [CrossRef] [Green Version]
- Longo, U.G.; Papalia, R.; De Salvatore, S.; Ruzzini, L.; Piergentili, I.; Oggiano, L.; Costici, P.F.; Denaro, V. Trends in Hospitalisation of Subtalar Joint Arthroereisis in Italy from 2009 to 2016. Foot Ankle Surg. 2021, in press. [Google Scholar] [CrossRef]
- Longo, U.G.; Salvatore, G.; Rizzello, G.; Berton, A.; Ciuffreda, M.; Candela, V.; Denaro, V. The Burden of Rotator Cuff Surgery in Italy: A Nationwide Registry Study. Arch. Orthop. Trauma Surg. 2017, 137, 217–224. [Google Scholar] [CrossRef]
- Longo, U.G.; Salvatore, G.; Locher, J.; Ruzzini, L.; Candela, V.; Berton, A.; Stelitano, G.; Schena, E.; Denaro, V. Epidemiology of Paediatric Shoulder Dislocation: A Nationwide Study in Italy from 2001 to 2014. Int. J. Environ. Res. Public. Health 2020, 17, 2834. [Google Scholar] [CrossRef] [Green Version]
- Pollet, V.; Percy, V.; Prior, H.J. Relative Risk and Incidence for Developmental Dysplasia of the Hip. J. Pediatr. 2017, 181, 202–207. [Google Scholar] [CrossRef]
- Neonatal Detection of Developmental Dysplasia of the Hip (DDH)-PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/9853482/ (accessed on 26 August 2020).
- Williams, N. Improving Early Detection of Developmental Dysplasia of the Hip through General Practitioner Assessment and Surveillance. Aust. J. Gen. Pract. 2018, 47, 619–623. [Google Scholar] [CrossRef]
- Feeley, I.H.; Green, C.J.; Rowan, F.E.; Moore, D.P. International Variance in the Treatment of Developmental Dysplasia of the Hip. J. Child. Orthop. 2014, 8, 381–386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, C.L.; Weller, S.; Roberts, L.; Reading, I.; Cook, A.; Little, L.; Wood, W.; Stanton, L.; Roposch, A.; Clarke, N.M. Timing of Surgical Intervention for Developmental Dysplasia of the Hip: A Randomised Controlled Trial (Hip ’Op). Health Technol. Assess. Winch. Engl. 2017, 21, 1–84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kyung, B.S.; Lee, S.H.; Jeong, W.K.; Park, S.Y. Disparity between Clinical and Ultrasound Examinations in Neonatal Hip Screening. Clin. Orthop. Surg. 2016, 8, 203–209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- French, L.M.; Dietz, F.R. Screening for Developmental Dysplasia of the Hip. Am. Fam. Physician 1999, 60, 177–184, 187–188. [Google Scholar] [PubMed]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Longo, U.G.; Papalia, R.; De Salvatore, S.; Ruzzini, L.; Piergentili, I.; Oggiano, L.; Costici, P.F.; Denaro, V. Developmental Hip Dysplasia: An Epidemiological Nationwide Study in Italy from 2001 to 2016. Int. J. Environ. Res. Public Health 2021, 18, 6589. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18126589
Longo UG, Papalia R, De Salvatore S, Ruzzini L, Piergentili I, Oggiano L, Costici PF, Denaro V. Developmental Hip Dysplasia: An Epidemiological Nationwide Study in Italy from 2001 to 2016. International Journal of Environmental Research and Public Health. 2021; 18(12):6589. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18126589
Chicago/Turabian StyleLongo, Umile Giuseppe, Rocco Papalia, Sergio De Salvatore, Laura Ruzzini, Ilaria Piergentili, Leonardo Oggiano, Pier Francesco Costici, and Vincenzo Denaro. 2021. "Developmental Hip Dysplasia: An Epidemiological Nationwide Study in Italy from 2001 to 2016" International Journal of Environmental Research and Public Health 18, no. 12: 6589. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18126589