
Secular Trend, Seasonal Variation, Epidemiological Pattern, and Outcome of Traumatic Head Injuries Due to Road Traffic Accidents in Aseer, Saudi Arabia


Abstract
:1. Introduction
2. Materials and Methods
2.1. Type of Study
2.2. Study Area
2.3. Study Sample and Technique
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Strength and Limitations
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- James, S.L.; Lucchesi, L.R.; Bisignano, C.; Castle, C.D.; Dingels, Z.V.; Fox, J.T.; Hamilton, E.B.; Liu, Z.; McCracken, D.; Nixon, M.R.; et al. Morbidity and mortality from road injuries: Results from the Global Burden of Disease Study 2017. Inj. Prev. 2020, 26, i46–i56. [Google Scholar] [CrossRef]
- GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef]
- Global Burden of Disease Estimates. 2020. Available online: https://vizhub.healthdata.org/gbd-compare/ (accessed on 26 April 2021).
- World Health Organization. Global Status Report on Road Safety 2018; World Health Organization: Geneva, Switzerland, 2018; Available online: http://www.who.int/violence_injury_prevention/road_safety_status/2018/en/ (accessed on 26 April 2021).
- Faul, M.; Wald, M.M.; Xu, L.; Coronado, V.G. Traumatic Brain Injury in the United States: Emergency Department Visits, Hospitalizations and Deaths 2002–2006; National Center for Injury Prevention and Control, Centers for Disease Control and Prevention: Atlanta, GA, USA, 2010. [Google Scholar]
- Al-Kuwaiti, A.; Hefny, A.F.; Bellou, A.; Eid, H.O.; Abu-Zidan, F.M. Epidemiology of head injury in the United Arab Emirates. Ulus. Travma Acil Cerrahi Derg. 2012, 18, 213–218. [Google Scholar] [CrossRef] [Green Version]
- Hefny, A.F.; Barss, P.; Eid, H.O.; Abu-Zidan, F.M. Motorcycle-related injuries in the United Arab Emirates. Accid. Anal. Prev. 2012, 49, 245–248. [Google Scholar] [CrossRef]
- Alhabdan, S.; Zamakhshary, M.; AlNaimi, M.; Mandora, H.; Alhamdan, M.; Al-Bedah, K.; Al-Enazi, S.; Al-Habib, A. Epidemiology of traumatic head injury in children and adolescents in a major trauma center in Saudi Arabia: Implications for injury prevention. Ann. Saudi Med. 2013, 33, 52–56. [Google Scholar] [CrossRef] [PubMed]
- Al-Hajj, S.; Hammoud, Z.; Colnaric, J.; Ataya, M.; Macaron, M.M.; Kadi, K.; Harati, H.; Phipps, H.; Mondello, S.; Tamim, H.; et al. Characterization of traumatic brain injury research in the Middle East and North Africa Region: A systematic review. Neuroepidemiology 2021, 55, 20–31, Epub ahead of print. [Google Scholar] [CrossRef]
- General Authority for Statistics, Statistical Yearbook. 2019. Available online: http://www.gov.sa (accessed on 3 June 2021).
- Karacasu, M.; Er, A.; Bilgiç, S.; Barut, H.B. Variations in traffic accidents on seasonal, monthly, daily and hourly basis: Eskisehir Case. Procedia Soc. Behav. Sci. 2011, 20, 767–775. [Google Scholar] [CrossRef] [Green Version]
- Ministry of Municipal, Rural Affairs and Housing. Abha City Profile; Abha Tourist Dynamics; United Nations Human Settlements Programme: Nairobi, Kenya; p. 64. Available online: https://unhabitat.org/sites/default/files/2020/05/abha_en.pdf (accessed on 3 June 2021).
- Alghnam, S.; Alkelya, M.; Alfraidy, M.; Al-Bedah, K.; Albabtain, I.T.; Alshenqeety, O. Outcomes of road traffic injuries before and after the implementation of a camera ticketing system: A retrospective study from a large trauma center in Saudi Arabia. Ann. Saudi. Med. 2017, 3, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Dahim, M.A.H. Impact of vision 2030 on traffic safety in Saudi Arabia. Int. J. Pediatr. Adolesc. Med. 2018, 5, 103–109. [Google Scholar] [CrossRef]
- Barrimah, I.; Midhet, F.; Sharaf, F. Epidemiology of road traffic injuries in Qassim Region, Saudi Arabia: Consistency of police and health data. Int. J. Health Sci. 2012, 6, 31–41. [Google Scholar] [CrossRef] [PubMed]
- Matsui, Y.; Oikawa, S.; Ando, K. Risks of pedestrian serious injuries and fatalities associated with impact velocities of cars in car-versus-pedestrian accidents in Japan. STAPP Car Crash J. 2013, 57, 201–217. [Google Scholar]
- Kudryavtsev, A.V.; Nilssen, O.; Lund, J.; Grjibovski, A.M.; Ytterstad, B. Road traffic crashes with fatal and non-fatal injuries in Arkhangelsk, Russia in 2005–2010. Int. J. Inj. Control Saf. Promot. 2013, 20, 349–357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kisser, J.; Waldstein, S.R.; Evans, M.K.; Zonderman, A.B. Lifetime prevalence of traumatic brain injury in a demographically diverse community sample. Brain Inj. 2017, 31, 620–623. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Habib, A.; A-shail, A.; Alaqeel, A.; Zamakhshary, M.; Al-Bedah, K.; AlQunai, M.; Al-Enazi, S. Causes and patterns of adult traumatic head injuries in Saudi Arabia: Implications for injury prevention. Ann. Saudi Med. 2013, 33, 351–355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alnaami, I.; Alshehri, S.; Alghamdi, S.; Ogran, M.; Qasem, A.; Medawi, A.; Medawi, A.; Alshahrani, S.; Sarhan, L. Patterns, types, and outcomes of head injury in Aseer Region, Kingdom of Saudi Arabia. Neuroscience 2019, 2019, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taylor, M.S.; Zelinkova, V.; Plancikova, D.; Melichova, J.; Sivco, P.; Rusnak, M.; Majdan, M. Seasonal patterns of traumatic brain injury deaths due to traffic-related incidents in the Slovak Republic. Traffic Inj. Prev. 2020, 21, 55–59. [Google Scholar] [CrossRef]
- Livingston, K.S.; Miller, P.E.; Lierhaus, A.; Matheney, T.H.; Mahan, S.T. Does weather matter? The effect of weather patterns and temporal factors on pediatric orthopedic trauma volume. Open Orthop. J. 2016, 10, 550–558. [Google Scholar] [CrossRef] [Green Version]
- Eom, K.S. The time-related trends in the presenting of traumatic head injury in a single institution. Korean J. Neurotrauma 2020, 16, 28–37. [Google Scholar] [CrossRef] [Green Version]
- Aldawood, A.S.; Alsultan, M.; Haddad, S.; Alqahtani, S.M.; Tamim, H.; Arabi, Y.M. Trauma profile at a tertiary intensive care unit in Saudi Arabia. Ann. Saudi Med. 2012, 32, 498–501. [Google Scholar] [CrossRef] [Green Version]
- Haghparast-Bidgoli, H.; Saadat, S.; Bogg, L.; Yarmohammadian, M.H.; Hasselberg, M. Factors affecting hospital length of stay and hospital charges associated with road traffic-related injuries in Iran. BMC Health Serv. Res. 2013, 13, 281. [Google Scholar] [CrossRef] [Green Version]
- Khan, M.A.B.; Grivna, M.; Nauman, J.; Soteriades, E.S.; Cevik, A.A.; Hashim, M.J.; Govender, R.; Al Azeezi, S.R. Global incidence and mortality patterns of pedestrian road traffic injuries by sociodemographic index, with forecasting: Findings from the Global Burden of Diseases, Injuries, and Risk Factors 2017 Study. Int. J. Environ. Res. Public Health 2020, 17, 2135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pape-Köhler, C.I.; Simanski, C.; Nienaber, U.; Lefering, R. External factors and the incidence of severe trauma: Time, date, season and moon. Injury 2014, 45, S93–S99. [Google Scholar] [CrossRef] [PubMed]
- Ostermann, R.C.; Joestl, J.; Tiefenboeck, T.M.; Lang, N.; Platzer, P.; Hofbauer, M. Risk factors predicting prognosis and outcome of elderly patients with isolated traumatic brain injury. J. Orthop. Surg. Res. 2018, 13, 277. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Variable | Male n = 1114 (%) | Female n = 121 (%) | Total n = 1235 (%) | OR [CI 95%] | p Value |
|---|---|---|---|---|---|
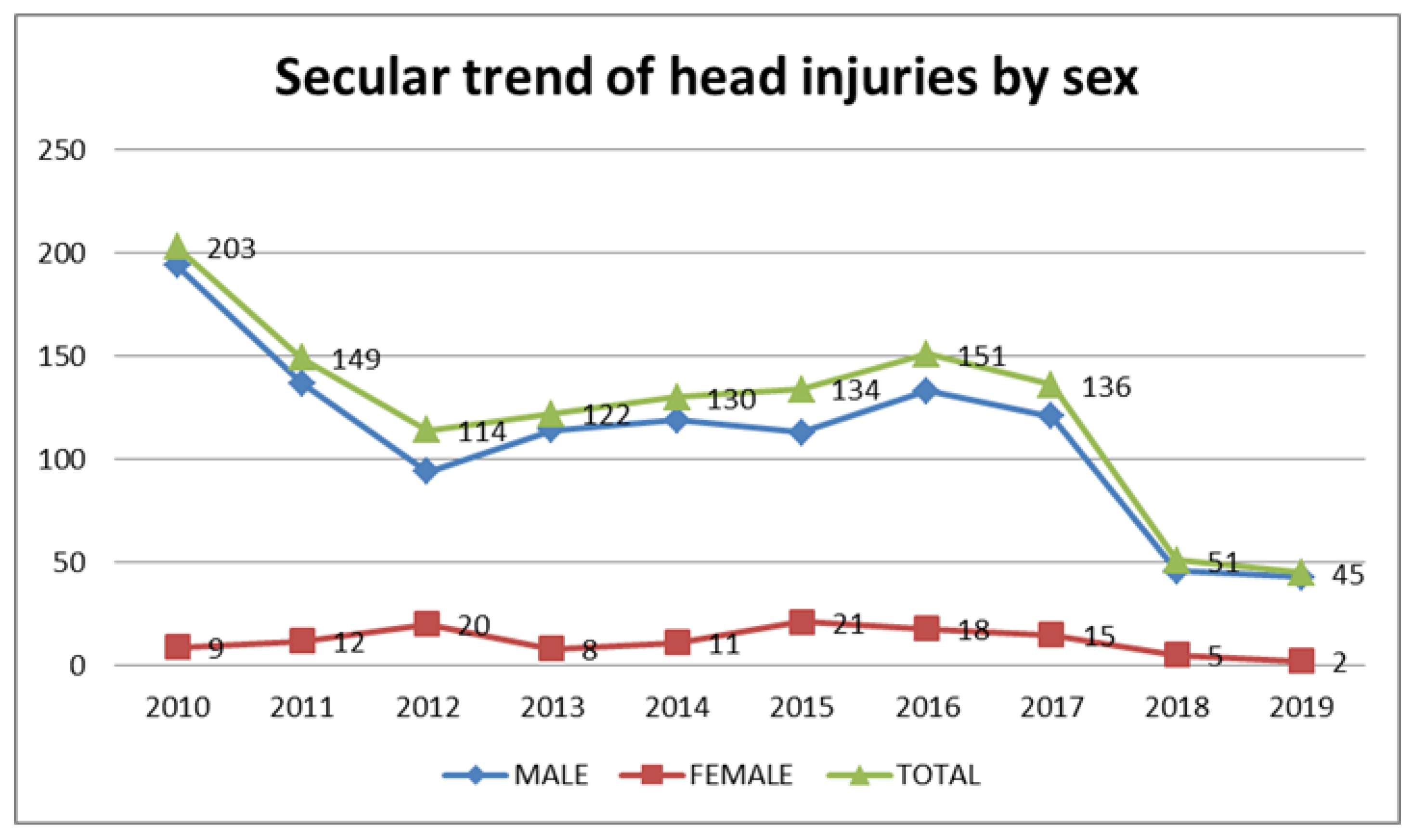
| Year | |||||
| 2010 * standard residual | 194 (17.4) | 9 (7.4) −2.4 | 203 (16.4) | --------- | 0.004 |
| 2011 | 137 (12.3) | 12 (9.9) | 149 (12.1) | ||
| 2012 * standard residual | 94 (8.4) | 20 (16.5) 2.6 | 114 (9.2) | ||
| 2013 | 114 (10.2) | 8 (6.6) | 122 (9.9) | ||
| 2014 | 119 (10.7) | 11 (9.1) | 130 (10.5) | ||
| 2015 * standard residual | 113 (10.1) | 21 (17.4) 2.2 | 134 (10.9) | ||
| 2016 | 133 (11.9) | 18 (14.9) | 151 (12.2) | ||
| 2017 | 121 (10.9) | 15 (12.4) | 136 (11.0) | ||
| 2018 | 46 (4.1) | 5 (4.1) | 51 (4.1) | ||
| 2019 | 43 (3.9) | 2 (1.7) | 45 (3.6) | ||
| Month | |||||
| January | 94 (8.4) | 6 (5) | 100 (8.1) | 0.017 | |
| February * standard residual | 87 (7.8) | 3 (2.5) * −2 | 90 (7.3) | ||
| March | 98 (8.8) | 6 (5) | 104 (8.4) | ||
| April | 78 (7.0) | 13 (10.7) | 91 (7.4) | ||
| May | 79 (7.1) | 14 (11.6) | 93 (7.5) | ||
| June | 108 (9.7) | 7 (5.8) | 115 (9.3) | ||
| July | 112 (10.1) | 11 (9.1) | 123 (10.0) | ||
| August * standard residual | 109 (9.8) | 21 (17.4) * 2.3 | 130 (10.5) | ||
| September | 97 (8.7) | 8 (6.6) | 105 (8.5) | ||
| October | 89 (8.0) | 13 (10.7) | 102 (8.3) | ||
| November | 94 (8.4) | 13 (10.7) | 107 (8.7) | ||
| December | 69 (6.2) | 6 (5) | 75 (6.1) | ||
| Season | ----------- | 0.071 | |||
| Winter | 250 (22.4) | 15 (12.4) | 265 (21.5) | ||
| Spring | 176 (15.8) | 19 (15.7) | 195 (15.8) | ||
| Summer | 408 (36.6) | 53 (43.8) | 461 (37.3) | ||
| Autumn | 280 (25.1) | 34 (28.1) | 314 (25.4) | ||
| Day of week | |||||
| Weekday | 795 (71.4) | 80 (66.1) | 875 (70.9) | 0.78 [0.52,1.16] | 0.228 |
| Weekend | 319 (28.6) | 41 (33.9) | 360 (29.1) | ||
| Vision 2030 | |||||
| Before | 771 (69.2) | 81 (66.9) | 852 (69) | 0.901 [0.604,1.34] | 0.608 |
| After | 343 (30.8) | 40 (33.1) | 383 (31) | ||
| Variable | Male n (%) | Female n (%) | Total n (%) | OR [CI 95%] | p Value |
|---|---|---|---|---|---|
| Head injury | |||||
| Multiple lesions | 360 (32.3) | 37 (30.6) | 397 (32.1) | --------- | 0.029 |
| Concussion | 94 (8.4) | 14 (11.6) | 108 (8.7) | ||
| Contusion | 146 (13.1) | 14 (11.6) | 160 (12.9) | ||
| SDH * Standard residual | 116 (10.4) | 2 (1.7) * −2.8 | 118 (9.6) | ||
| EDH | 98 (8.8) | 10 (8.3) | 108 (8.7) | ||
| SAH | 36 (3.2) | 5 (4.1) | 41 (3.3) | ||
| Skull fracture | 118 (10.6) | 20 (16.5) | 138 (11.2) | ||
| Superficial injury | 36 (3.2) | 6 (5) | 42 (3.4) | ||
| Unspecified injury | 75 (6.7) | 12 (9.9) | 87 (7.0) | ||
| Other (DAI, IVH, ICH) | 35 (3.1) | 1 (0.8) | 36 (2.9) | ||
| Associated injury | |||||
| No | 534 (47.9) | 51 (42.1) | 585 (47.4) | 0.79 [0.541,1.157] | 0.226 |
| Yes | 580 (52.1) | 70 (57.9) | 650 (52.6) | ||
| ICU admission | |||||
| No | 902 (81) | 100 (82.6) | 1002 (81.1) | 1.11 [0.683,1.834] | 0.651 |
| Yes | 212 (19) | 21 (17.4) | 233 (18.9) | ||
| LOS | ------ | 0.483 | |||
| Less than 1 week | 433 (38.9) | 44 (36.4) | 477 (38.6) | ||
| 1–2 weeks | 281 (25.2) | 36 (29.8) | 317 (25.7) | ||
| 15–30 days | 188 (16.9) | 19 (15.7) | 207 (16.8) | ||
| 30–180 days | 191 (17.1) | 22 (18.2) | 213 (17.2) | ||
| >180 days | 21 (1.9) | 0 (0) | 21 (1.7) | ||
| Outcome | ------ | 0.674 | |||
| Discharge to home | 910 (81.7) | 95 (78.5) | 1005 (81.4) | ||
| Transfer | 43 (3.9) | 6 (5.0) | 49 (4.0) | ||
| Death | 161 (14.5) | 20 (16.5) | 181 (14.7) | ||
| Variable | 0–17 Years n (%) | 18–34 Years n (%) | 35–59 Years n (%) | 60 Years and above n (%) | Total n (%) | p Value |
|---|---|---|---|---|---|---|
| Year | ||||||
| 2010 | 49 (14.6) | 124 (18.6) | 18 (12.9) | 12 (13.0) | 203 (16.4) | 0.499 |
| 2011 | 39 (11.6) | 87 (13.0) | 16 (11.5) | 7 (7.6) | 149 (12.1) | |
| 2012 | 39 (11.6) | 50 (7.5) | 12 (8.6) | 13 (14.1) | 114 (9.2) | |
| 2013 | 36 (10.7) | 64 (9.6) | 12 (8.6) | 10 (10.9) | 122 (9.9) | |
| 2014 | 37 (11.0) | 64 (9.6) | 18 (12.9) | 11 (12.0) | 130 (10.5) | |
| 2015 | 41 (12.2) | 69 (10.3) | 15 (10.8) | 9 (9.8) | 134 (10.9) | |
| 2016 | 40 (11.9) | 76 (11.4) | 23 (16.5) | 12 (13.0) | 151 (12.2) | |
| 2017 | 35 (10.4) | 78 (11.7) | 11 (7.9) | 12 (13.0) | 136 (11.0) | |
| 2018 | 12 (3.6) | 30 (4.5) | 5 (3.6) | 4 (4.3) | 51 (4.1) | |
| 2019 | 8 (2.4) | 26 (3.9) | 9 (6.5) | 2 (2.2) | 45 (3.6) | |
| Month | 0.402 | |||||
| January | 26 (7.7) | 62 (9.3) | 8 (5.8) | 4 (4.3) | 100 (8.1) | |
| February | 23 (6.8) | 52 (7.8) | 9 (6.5) | 6 (6.5) | 90 (7.3) | |
| March | 22 (6.5) | 64 (9.6) | 13 (9.4) | 5 (5.4) | 104 (8.4) | |
| April | 29 (8.6) | 48 (7.2) | 7 (5.0) | 7 (7.6) | 91 (7.4) | |
| May | 30 (8.9) | 42 (6.3) | 10 (7.2) | 11 (12.0) | 93 (7.5) | |
| June | 31 (9.2) | 58 (8.7) | 15 (10.8) | 11 (12.0) | 115 (9.3) | |
| July | 35 (10.4) | 63 (9.4) | 16 (11.5) | 9 (9.8) | 123 (10.0) | |
| August | 42 (12.5) | 70 (10.5) | 10 (7.2) | 8 (8.7) | 130 (10.5) | |
| September | 26 (7.7) | 54 (8.1) | 17 (12.2) | 8 (8.7) | 105 (8.5) | |
| October | 28 (8.3) | 47 (7.0) | 19 (13.7) | 8 (8.7) | 102 (8.3) | |
| November | 25 (7.4) | 65 (9.7) | 6 (4.3) | 11 (12.0) | 107 (8.7) | |
| December | 19 (5.7) | 43 (6.4) | 9 (6.5) | 4 (4.3) | 75 (6.1) | |
| Season | 0.338 | |||||
| Winter | 68 (20.2) | 157 (23.5) | 26 (18.7) | 14 (15.2) | 265 (21.5) | |
| Spring | 51 (15.2) | 112 (16.8) | 20 (14.4) | 12 (13) | 195 (15.8) | |
| Summer | 138 (41.1) | 233 (34.9) | 51 (36.7) | 39 (42.4) | 461 (37.3) | |
| Autumn | 79 (23.5) | 166 (24.9) | 42 (30.2) | 27 (29.3) | 314 (25.4) | |
| Day of week | 0.400 | |||||
| Workdays | 239 (71.1) | 471 (70.5) | 105 (75.5) | 60 (65.2) | 875 (70.9) | |
| Weekend | 97 (28.9) | 197 (29.5) | 34 (24.5) | 32 (34.8) | 360 (29.1) | |
| Vision 2030 | ||||||
| Before | 241 (71.7) | 458 (68.6) | 91 (65.5) | 62 (67.4) | 852 (69) | 0.542 |
| After | 95 (28.3) | 210 (31.4) | 48 (34.5) | 30 (32.6) | 383 (31) |
| Variable | 0–17 Years n (%) | 18–34 Years n (%) | 35–59 Years n (%) | ≥60 Years n (%) | Total n (%) | p Value |
|---|---|---|---|---|---|---|
| Head injury | <0.001 | |||||
| Multiple lesions | 115 (34.2) | 213 (31.9) | 43 (30.9) | 26 (28.3) | 397 (32.1) | |
| Concussion | 30 (8.9) | 64 (9.6) | 10 (7.2) | 4 (4.3) | 108 (8.7) | |
| Contusion | 41 (12.2) | 96 (14.4) | 12 (8.6) | 11 (12) | 160 (13) | |
| SDH * Standard residual | 20 (6.0) −2.1 | 56 (8.4) | 13 (9.4) | 29 (31.5) 6.8 | 118 (9.6) | |
| EDH * Standard residual | 28 (8.3) | 67 (10) | 11 (7.9) | 2 (2.2) −2.1 | 108 (8.7) | |
| SAH * Standard residual | 4 (1.2) 2.2 | 16 (2.4) | 15 (10.8) −2 | 6 (6.5) | 41 (3.3) | |
| Skull Fracture * Standard residual | 51 (15.2) −2.1 | 72 (10.8) | 11 (7.9) | 4 (4.3) 4.8 | 138 (11.2) | |
| Superficial injury | 14 (4.2) | 18 (2.7) | 8 (5.8) | 2 (2.2) | 42 (3.4) | |
| Unspecified injury | 24 (7.1) | 45 (6.7) | 12 (8.6) | 6 (6.5) | 87 (7) | |
| Other (DAI, IVH, ICH) | 9 (2.7) | 21 (3.1) | 4 (2.9) | 2 (2.2) | 36 (2.9) | |
| Associated injury | ||||||
| No | 174 (51.8) | 302 (45.2) | 59 (42.4) | 50 (54.3) | 585 (47.4) | 0.071 |
| Yes | 162 (48.2) | 366 (54.8) | 80 (57.6) | 42 (45.7) | 650 (52.6) | |
| ICU admission | ||||||
| No | 276 (82.1) | 537 (80.4) | 109 (78.4) | 80 (87) | 1002 (811) | 0.366 |
| Yes | 60 (17.9) | 131 (19.6) | 30 (21.6) | 12 (13) | 233 (18.9) | |
| LOS | 0.124 | |||||
| Up to 1 week | 133 (39.6) | 259 (38.8) | 51 (36.7) | 34 (37) | 477 (38.6) | |
| 1–2 weeks | 101 (30.1) | 162 (24.3) | 29 (20.9) | 25 (27.2) | 317 (25.7) | |
| 15–30 days | 53 (15.8) | 112 (16.8) | 29 (20.9) | 13 (14.1) | 207 (16.8) | |
| 30–180 days | 46 (13.7) | 118 (17.7) | 29 (20.9) | 20 (21.7) | 213 (17.2) | |
| >180 days | 3 (0.9) | 17 (2.5) | 1 (0.7) | 0 (0) | 21 (1.7) | |
| Outcome | 0.416 | |||||
| Discharge to home | 278 (82.7) | 539 (80.7) | 109 (78.4) | 79 (85.9) | 1005 (81.4) | |
| Transfer | 14 (4.2) | 30 (4.5) | 03 (2.2) | 02 (2.2) | 49 (4.0) | |
| Death | 44 (13.1) | 99 (14.8) | 27 (19.4) | 11 (12) | 181 (14.7) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Algahtany, M.A. Secular Trend, Seasonal Variation, Epidemiological Pattern, and Outcome of Traumatic Head Injuries Due to Road Traffic Accidents in Aseer, Saudi Arabia. Int. J. Environ. Res. Public Health 2021, 18, 6623. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18126623
Algahtany MA. Secular Trend, Seasonal Variation, Epidemiological Pattern, and Outcome of Traumatic Head Injuries Due to Road Traffic Accidents in Aseer, Saudi Arabia. International Journal of Environmental Research and Public Health. 2021; 18(12):6623. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18126623
Chicago/Turabian StyleAlgahtany, Mubarak Ali. 2021. "Secular Trend, Seasonal Variation, Epidemiological Pattern, and Outcome of Traumatic Head Injuries Due to Road Traffic Accidents in Aseer, Saudi Arabia" International Journal of Environmental Research and Public Health 18, no. 12: 6623. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18126623