
Relationship between Oral Hypofunction and Sarcopenia in Community-Dwelling Older Adults: The Otassha Study

 ,
,  , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
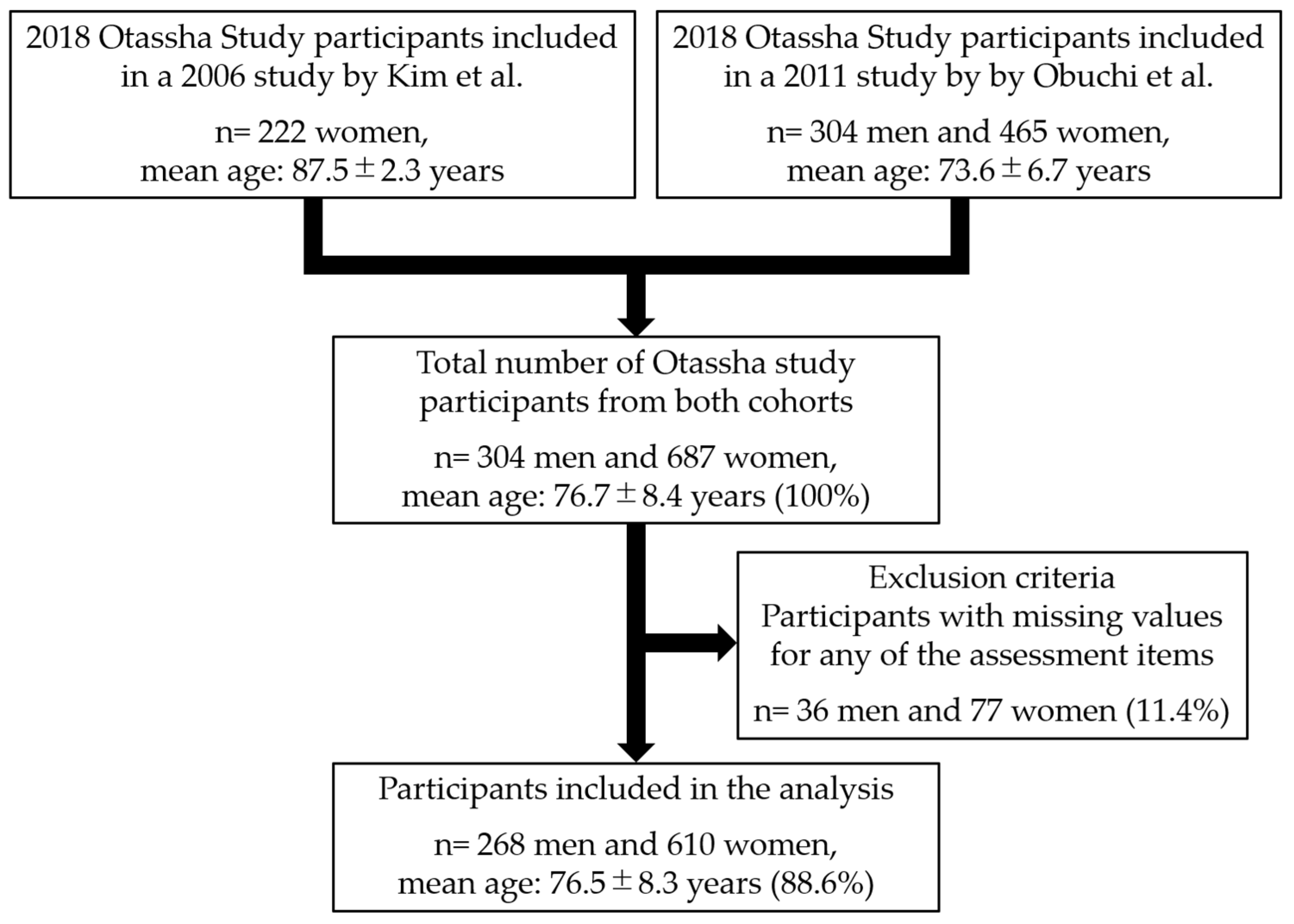
2.1. Research Design
2.2. Number of Teeth
2.3. Oral Hypofunction
2.3.1. Poor Oral Hygiene
2.3.2. Oral Dryness
2.3.3. Reduced Occlusal Force
2.3.4. Decreased Tongue–Lip Motor Function
2.3.5. Decreased Tongue Pressure
2.3.6. Decreased Masticatory Function
2.3.7. Deterioration of Swallowing Function
2.4. Sarcopenia
2.4.1. Low Muscle Strength
2.4.2. Low Physical Performance
2.4.3. Low Appendicular Skeletal Muscle Mass
2.5. Other Recorded Variables
2.6. Statistical Analysis
3. Results
3.1. Participants
3.2. Characteristics of Study Participants and between Group Comparisons
3.3. Variables Associated with Sarcopenia
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cabinet Office, Governmento of Japan. Annual Report on the Aging Society: 2020; Cabinet Office: Tokyo, Japan, 2020. [Google Scholar]
- Minakuchi, S.; Tsuga, K.; Ikebe, K.; Ueda, T.; Tamura, F.; Nagao, K.; Furuya, J.; Matsuo, K.; Yamamoto, K.; Kanazawa, M.; et al. Oral hypofunction in the older population: Position paper of the Japanese Society of Gerodontology in 2016. Gerodontology 2018, 35, 317–324. [Google Scholar] [CrossRef] [PubMed]
- Sato, Y.; Kitagawa, N.; Shichita, T.; Hatanaka, Y.; Uchida, Y. State of Implementation of Examination and Management of Oral Hypofunction Newly Covered by National Health Insurance. Ronen Shika Igaku 2020, 35, 230–232. [Google Scholar]
- Matsuo, K.; Taniguchi, H.; Nakagawa, K.; Kanazawa, M.; Furuya, J.; Tsuga, K.; Ikebe, K.; Ueda, T.; Tamura, F.; Nagao, K.; et al. Relationships between Deterioration of Oral Functions and Nutritional Status in Elderly Patients in an Acute Hospital. Ronen Shika Igaku 2016, 31, 123–133. [Google Scholar]
- Suzuki, M.; Koyama, S.; Kimura, Y.; Ishiyama, D.; Otobe, Y.; Nishio, N.; Ichikawa, T.; Kunieda, Y.; Ohji, S.; Ito, D.; et al. Relationship between characteristics of skeletal muscle and oral function in community-dwelling older women. Arch. Gerontol. Geriatr. 2018, 79, 171–175. [Google Scholar] [CrossRef] [PubMed]
- Hatta, K.; Ikebe, K. Association between oral health and sarcopenia: A literature review. J. Prosthodont. Res. 2020. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, Y.; Okada, K.; Kondo, M.; Matsushita, T.; Nakazawa, S.; Yamazaki, Y. Oral health for achieving longevity. Geriatr. Gerontol. Int. 2020, 20, 526–538. [Google Scholar] [CrossRef]
- Tanaka, T.; Takahashi, K.; Hirano, H.; Kikutani, T.; Watanabe, Y.; Ohara, Y.; Furuya, H.; Tetsuo, T.; Akishita, M.; Iijima, K. Oral Frailty as a Risk Factor for Physical Frailty and Mortality in Community-Dwelling Elderly. J. Gerontol. Ser. A 2018, 73, 1661–1667. [Google Scholar] [CrossRef]
- Hironaka, S.; Kugimiya, Y.; Watanabe, Y.; Motokawa, K.; Hirano, H.; Kawai, H.; Kera, T.; Kojima, M.; Fujiwara, Y.; Ihara, K.; et al. Association between oral, social, and physical frailty in community-dwelling older adults. Arch. Gerontol. Geriatr. 2020, 89, 104105. [Google Scholar] [CrossRef]
- Shimazaki, Y.; Nonoyama, T.; Tsushita, K.; Arai, H.; Matsushita, K.; Uchibori, N. Oral hypofunction and its association with frailty in community-dwelling older people. Geriatr. Gerontol. Int. 2020, 20, 917–926. [Google Scholar] [CrossRef] [PubMed]
- Ganapathy, A.; Nieves, J.W. Nutrition and Sarcopenia-What Do We Know? Nutrients 2020, 12, 1755. [Google Scholar] [CrossRef]
- Chen, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Chou, M.Y.; Iijima, K.; Jang, H.C.; Kang, L.; Kim, M.; Kim, S.; et al. Asian Working Group for Sarcopenia: 2019 Consensus Update on Sarcopenia Diagnosis and Treatment. J. Am. Med Dir. Assoc. 2020, 21, 300–307.e2. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gotzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Lancet 2007, 370, 1453–1457. [Google Scholar] [CrossRef]
- Kugimiya, Y.; Watanabe, Y.; Shirobe, M.; Motohashi, Y.; Motokawa, K.; Edahiro, A.; Ohara, Y.; Ryu, M.; Igarashi, K.; Hoshino, D.; et al. A comparison of colorimetric and visual methods for the assessment of masticatory performance with color-changeable chewing gum in older persons. J. Dent. Sci. 2021, 16, 380–388. [Google Scholar] [CrossRef]
- Shimizu, T.; Ueda, T.; Sakurai, K. New method for evaluation of tongue-coating status. J. Oral Rehabil. 2007, 34, 442–447. [Google Scholar] [CrossRef]
- Fukushima, Y.; Yoda, T.; Araki, R.; Sakai, T.; Toya, S.; Ito, K.; Funayama, S.; Enoki, Y.; Sato, T. Evaluation of oral wetness using an improved moisture-checking device for the diagnosis of dry mouth. Oral Sci. Int. 2017, 14, 33–36. [Google Scholar] [CrossRef]
- Takano, T.; Kugimiya, Y.; Morita, K.; Tazawa, S.; Ueda, T.; Sakurai, K. Intra- and inter-investigator reliabilities of oral moisture measured using an oral moisture-checking device. J. Oral Rehabil. 2020, 47, 480–484. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, T.; Kumagai, H.; Watanabe, T.; Uchida, T.; Nagao, M. Evaluation of complete denture occlusal contacts using pressure-sensitive sheets. Int. J. Prosthodont. 1997, 10, 386–391. [Google Scholar] [PubMed]
- Hidaka, O.; Iwasaki, M.; Saito, M.; Morimoto, T. Influence of clenching intensity on bite force balance, occlusal contact area, and average bite pressure. J. Dent. Res. 1999, 78, 1336–1344. [Google Scholar] [CrossRef] [PubMed]
- Inomata, C.; Ikebe, K.; Kagawa, R.; Okubo, H.; Sasaki, S.; Okada, T.; Takeshita, H.; Tada, S.; Matsuda, K.; Kurushima, Y.; et al. Significance of occlusal force for dietary fibre and vitamin intakes in independently living 70-year-old Japanese: From SONIC Study. J. Dent. 2014, 42, 556–564. [Google Scholar] [CrossRef] [PubMed]
- Ito, K.; Yoshihara, A.; Takano, N.; Ishigami, K.; Seida, Y.; Inoue, M.; Kitahara, M.; Miyazaki, H. A Comparison of Methods for the Measurement of Oral Diadochokinesis. Ronen Shika Igaku 2009, 24, 48–54. [Google Scholar]
- Tsuga, K.; Maruyama, M.; Yoshikawa, M.; Yoshida, M.; Akagawa, Y. Manometric evaluation of oral function with a hand-held balloon probe. J. Oral Rehabil. 2011, 38, 680–685. [Google Scholar] [CrossRef] [PubMed]
- Yoshikawa, M.; Fukuoka, T.; Mori, T.; Hiraoka, A.; Higa, C.; Kuroki, A.; Takeda, C.; Maruyama, M.; Yoshida, M.; Tsuga, K. Comparison of the Iowa Oral Performance Instrument and JMS tongue pressure measurement device. J. Dent. Sci. 2021, 16, 214–219. [Google Scholar] [CrossRef] [PubMed]
- Nokubi, T.; Yoshimuta, Y.; Nokubi, F.; Yasui, S.; Kusunoki, C.; Ono, T.; Maeda, Y.; Yokota, K. Validity and reliability of a visual scoring method for masticatory ability using test gummy jelly. Gerodontology 2013, 30, 76–82. [Google Scholar] [CrossRef] [PubMed]
- Igarashi, K.; Watanabe, Y.; Kugimiya, Y.; Shirobe, M.; Edahiro, A.; Kaneda, K.; Hasegawa, Y.; Ito, M.; Hirano, H.; Sakurai, K.; et al. Validity of a visual scoring method using gummy jelly for evaluating chewing efficiency in a large-scale epidemiological survey. J. Oral Rehabil. 2019, 46, 409–416. [Google Scholar] [CrossRef] [PubMed]
- Belafsky, P.C.; Mouadeb, D.A.; Rees, C.J.; Pryor, J.C.; Postma, G.N.; Allen, J.; Leonard, R.J. Validity and reliability of the Eating Assessment Tool (EAT-10). Ann. Otol. Rhinol. Laryngol. 2008, 117, 919–924. [Google Scholar] [CrossRef]
- Taniguchi, Y.; Kitamura, A.; Seino, S.; Murayama, H.; Amano, H.; Nofuji, Y.; Nishi, M.; Yokoyama, Y.; Shinozaki, T.; Yokota, I.; et al. Gait Performance Trajectories and Incident Disabling Dementia Among Community-Dwelling Older Japanese. J. Am. Med. Dir. Assoc. 2017, 18, e13–e192. [Google Scholar] [CrossRef] [PubMed]
- Iwasa, H.; Masui, Y.; Inagaki, H.; Yoshida, Y.; Shimada, H.; Otsuka, R.; Kikuchi, K.; Nonaka, K.; Yoshida, H.; Yoshida, H.; et al. Assessing competence at a higher level among older adults: Development of the Japan Science and Technology Agency Index of Competence (JST-IC). Aging Clin. Exp. Res. 2018, 30, 383–393. [Google Scholar] [CrossRef] [PubMed]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Sakuma, N.; Ura, C.; Miyamae, F.; Inagaki, H.; Ito, K.; Niikawa, H.; Ijuin, M.; Okamura, T.; Sugiyama, M.; Awata, S. Distribution of Mini-Mental State Examination scores among urban community-dwelling older adults in Japan. Int. J. Geriatr. Psychiatry 2017, 32, 718–725. [Google Scholar] [CrossRef] [PubMed]
- Tamburrini, A.; Tacconi, F.; Barlattani, A.; Mineo, T.C. An update on myasthenia gravis, challenging disease for the dental profession. J. Oral Sci. 2015, 57, 161–168. [Google Scholar] [CrossRef] [Green Version]
- Palmer, P.M.; Neel, A.T.; Sprouls, G.; Morrison, L. Swallow characteristics in patients with oculopharyngeal muscular dystrophy. J. Speech Lang. Hear. Res. 2010, 53, 1567–1578. [Google Scholar] [CrossRef]
- Borgnakke, W.S.; Anderson, P.F.; Shannon, C.; Jivanescu, A. Is there a relationship between oral health and diabetic neuropathy? Curr. Diab. Rep. 2015, 15, 93. [Google Scholar] [CrossRef]
- Bergendal, B.; McAllister, A. Orofacial function and monitoring of oral care in amyotrophic lateral sclerosis. Acta Odontol. Scand. 2017, 75, 179–185. [Google Scholar] [CrossRef]
- Kouwenberg, C.V.; Voermans, N.C.; Quinlivan, R.; van den Engel-Hoek, L. Mastication and Oral Motor Function in McArdle Disease: Patient Reported Complaints. J. Neuromuscul. Dis. 2018, 5, 353–357. [Google Scholar] [CrossRef] [PubMed]
- Jeon, Y. Fibromyalgia: Practical considerations for oral health care providers. J. Dent. Anesth. Pain Med. 2020, 20, 263–269. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.A.; Suh, D.I.; Chae, J.H.; Shin, H.I. Trajectory of change in the swallowing status in spinal muscular atrophy type I. Int. J. Pediatr. Otorhinolaryngol. 2020, 130, 109818. [Google Scholar] [CrossRef]
- Printza, A.; Boziki, M.; Triaridis, S.; Kiousi, V.; Arnaoutoglou, M.; Constantinidis, J.; Grigoriadis, N. Tongue strength, dysphagia questionnaire, pharyngeal secretions and FEES findings in dysphagia management in amyotrophic lateral sclerosis. Auris Nasus Larynx 2020, 48, 672–682. [Google Scholar] [CrossRef]
- Nakamura, M.; Hamada, T.; Tanaka, A.; Nishi, K.; Kume, K.; Goto, Y.; Beppu, M.; Hijioka, H.; Higashi, Y.; Tabata, H.; et al. Association of Oral Hypofunction with Frailty, Sarcopenia, and Mild Cognitive Impairment: A Cross-Sectional Study of Community-Dwelling Japanese Older Adults. J. Clin. Med. 2021, 10, 1626. [Google Scholar] [CrossRef] [PubMed]
- Kugimiya, Y.; Watanabe, Y.; Ueda, T.; Motokawa, K.; Shirobe, M.; Igarashi, K.; Hoshino, D.; Takano, T.; Sakurai, K.; Taniguchi, Y.; et al. Rate of oral frailty and oral hypofunction in rural community-dwelling older Japanese individuals. Gerodontology 2020, 37, 342–352. [Google Scholar] [CrossRef]
- Matsuo, K.; Kito, N.; Ogawa, K.; Izumi, A.; Kishima, M.; Itoda, M.; Masuda, Y. Improvement of oral hypofunction by a comprehensive oral and physical exercise programme including textured lunch gatherings. J. Oral Rehabil. 2020, 48, 411–421. [Google Scholar] [CrossRef]
- Liu, X.; Hou, L.; Zhao, W.; Xia, X.; Hu, F.; Zhang, G.; Hao, Q.; Zhou, L.; Liu, Y.; Ge, M.; et al. The Comparison of Sarcopenia Diagnostic Criteria using AWGS 2019 with the Other Five Criteria in West China. Gerontology 2021, 67, 290–300. [Google Scholar]
- Huang, J.; He, F.; Gu, X.; Chen, S.; Tong, Z.; Zhong, S. Estimation of sarcopenia prevalence in individuals at different ages from Zheijang province in China. Aging 2021, 13, 6066. [Google Scholar] [CrossRef] [PubMed]
- Kitamura, A.; Seino, S.; Abe, T.; Nofuji, Y.; Yokoyama, Y.; Amano, H.; Nishi, M.; Taniguchi, Y.; Narita, M.; Fujiwara, Y.; et al. Sarcopenia: Prevalence, associated factors, and the risk of mortality and disability in Japanese older adults. J. Cachexia Sarcopenia Muscle 2021, 12, 30–38. [Google Scholar] [CrossRef] [PubMed]
- Can, B.; Kara, O.; Kizilarslanoglu, M.C.; Arik, G.; Aycicek, G.S.; Sumer, F.; Civelek, R.; Demirtas, C.; Ulger, Z. Serum markers of inflammation and oxidative stress in sarcopenia. Aging Clin. Exp. Res. 2017, 29, 745–752. [Google Scholar] [CrossRef] [PubMed]
- Fukuoka, Y.; Narita, T.; Fujita, H.; Morii, T.; Sato, T.; Sassa, M.H.; Yamada, Y. Importance of physical evaluation using skeletal muscle mass index and body fat percentage to prevent sarcopenia in elderly Japanese diabetes patients. J. Diabetes Investig. 2019, 10, 322–330. [Google Scholar] [CrossRef] [PubMed]
- Tanimoto, Y.; Watanabe, M.; Sun, W.; Sugiura, Y.; Tsuda, Y.; Kimura, M.; Hayashida, I.; Kusabiraki, T.; Kono, K. Association between sarcopenia and higher-level functional capacity in daily living in community-dwelling elderly subjects in Japan. Arch. Gerontol. Geriatr. 2012, 55, e9–e13. [Google Scholar] [CrossRef]
- Wang, D.X.M.; Yao, J.; Zirek, Y.; Reijnierse, E.M.; Maier, A.B. Muscle mass, strength, and physical performance predicting activities of daily living: A meta-analysis. J. Cachexia Sarcopenia Muscle 2020, 11, 3–25. [Google Scholar] [CrossRef] [Green Version]
- Iwasaki, M.; Motokawa, K.; Watanabe, Y.; Shirobe, M.; Inagaki, H.; Edahiro, A.; Ohara, Y.; Hirano, H.; Shinkai, S.; Awata, S. A Two-Year Longitudinal Study of the Association between Oral Frailty and Deteriorating Nutritional Status among Community-Dwelling Older Adults. Int. J. Environ. Res. Public Health 2020, 18, 213. [Google Scholar] [CrossRef]
- Hoshino, D.; Hirano, H.; Edahiro, A.; Motokawa, K.; Shirobe, M.; Watanabe, Y.; Motohashi, Y.; Ohara, Y.; Iwasaki, M.; Maruoka, Y.; et al. Association between Oral Frailty and Dietary Variety among Community-Dwelling Older Persons: A Cross-Sectional Study. J. Nutr. Health Aging 2021, 25, 361–368. [Google Scholar] [CrossRef]
- Amagai, N.; Komagamine, Y.; Kanazawa, M.; Iwaki, M.; Jo, A.; Suzuki, H.; Minakuchi, S. The effect of prosthetic rehabilitation and simple dietary counseling on food intake and oral health related quality of life among the edentulous individuals: A randomized controlled trial. J. Dent. 2017, 65, 89–94. [Google Scholar] [CrossRef]
- Suzuki, H.; Kanazawa, M.; Komagamine, Y.; Iwaki, M.; Jo, A.; Amagai, N.; Minakuchi, S. The effect of new complete denture fabrication and simplified dietary advice on nutrient intake and masticatory function of edentulous elderly: A randomized-controlled trial. Clin. Nutr. 2018, 37, 1441–1447. [Google Scholar] [CrossRef] [PubMed]
- Kanazawa, M.; Suzuki, H.; Komagamine, Y.; Iwaki, M.; Amagai, N.; Minakuchi, S. Combined effects of new complete denture fabrication and simplified dietary advice on nutrient intake in edentulous elderly patients for 6 months. Clin. Oral Investig. 2019, 23, 2245–2252. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Overall | Women | Men | Robust | Sarcopenia | Robust | Oral Hypofunction | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| (n = 878) | (n = 610) | (n = 268) | (n = 715) | (n = 163) | (n = 435) | (n = 443) | ||||
| Continuous Variables | Median, (Q1, Q3) | Median, (Q1, Q3) | Median, (Q1, Q3) | p-Value | Median, (Q1, Q3) | Median, (Q1, Q3) | p-Value | Median, (Q1, Q3) | Median, (Q1, Q3) | p-Value |
| Variables of oral hypofunction | ||||||||||
| Tongue coating index (%) | 22.2, (11.1, 50.0) | 22.2, (11.1, 50.0) | 33.3, (16.7, 61.1) | <0.001 | 22.2, (11.1, 50.0) | 22.2, (11.1, 38.9) | 0.047 | 16.7, (11.1, 38.9) | 33.3, (11.1, 55.6) | <0.001 |
| Oral moisture | 27.1, (24.9, 28.8) | 26.9, (24.8, 28.6) | 27.4, (25.2, 29.3) | 0.008 | 27.2, (25.0, 28.9) | 26.6, (24.4, 28.6) | 0.096 | 27.8, (26.3, 29.3) | 26.1, (24.3, 28.0) | <0.001 |
| Occlusal force (N) | 257.1, (121.0, 417.8) | 213.8, (101.8, 366.4) | 367.7, (221.3, 559.3) | <0.001 | 293.2, (140.4, 435.9) | 163, (72.8, 288.7) | <0.001 | 352.2, (240.0, 517.4) | 155.5, (79.6, 301.2) | <0.001 |
| Oral diadochokinesis/pa/ (time/s) | 6.4, (5.8, 6.8) | 6.2, (5.8, 6.8) | 6.4, (6.0, 6.8) | 0.002 | 6.4, (6.0, 6.8) | 6.0, (5.4, 6.6) | <0.001 | 6.6, (6.2, 7.0) | 6.2, (5.6, 6.6) | <0.001 |
| Oral diadochokinesis/ta/ (time/s) | 6.4, (5.8, 6.8) | 6.2, (5.8, 6.8) | 6.4, (6.0, 6.8) | 0.004 | 6.4, (5.8, 6.8) | 6.0, (5.4, 6.4) | <0.001 | 6.6, (6.2, 7.0) | 6, (5.6, 6.4) | <0.001 |
| Oral diadochokinesis/ka/ (time/s) | 5.8, (5.4, 6.4) | 5.8, (5.4, 6.4) | 6.0, (5.2, 6.4) | 0.917 | 6.0, (5.4, 6.4) | 5.6, (5.0, 6.0) | <0.001 | 6.2, (5.8, 6.6) | 5.6, (5.0, 6.0) | <0.001 |
| Tongue pressure (kPa) | 31.8, (26.3, 36.9) | 31.3, (25.8, 35.7) | 33.4, (27.8, 39) | <0.001 | 32.9, (27.8, 37.8) | 27.2, (20.6, 31.8) | <0.001 | 34.6, (30.8, 39.2) | 28.3, (23.5, 33.2) | <0.001 |
| Gummy jelly score | 5, (3, 6) | 5, (2, 6) | 6, (5, 7) | <0.001 | 5, (4, 6) | 4, (1, 6) | <0.001 | 6, (5, 6) | 4, (1, 6) | <0.001 |
| EAT-10 score | 1, (0, 3) | 1, (0, 3) | 1, (0, 4) | 0.516 | 1, (0, 3) | 1, (0, 5) | 0.004 | 0, (0, 2) | 2, (0, 5) | <0.001 |
| Oral hypofunction score | 3, (2, 4) | 3, (2, 4) | 2, (1, 3) | <0.001 | 2, (1, 3) | 4, (2, 5) | <0.001 | 2, (1, 2) | 4, (3, 4) | <0.001 |
| Variables of sarcopenia | ||||||||||
| Handgrip strength (kg) | 24.0, (18.0, 31.0) | 21.0, (17.0, 25.0) | 35.0, (30.3, 40.0) | <0.001 | 25.0, (21.0, 33.0) | 16, (14, 19) | <0.001 | 26, (21, 35) | 21, (16, 27) | <0.001 |
| Gait speed (m/s) | 1.32, (1.11, 1.52) | 1.32, (1.09, 1.47) | 1.39, (1.22, 1.55) | <0.001 | 1.39, (1.19, 1.52) | 1.09, (0.91, 1.32) | <0.001 | 1.39, (1.22, 1.56) | 1.25, (1.04, 1.43) | <0.001 |
| Skeletal muscle mass index (kg/m2) | 6.1, (5.6, 7.0) | 5.8, (5.3, 6.2) | 7.5, (7.0, 7.9) | <0.001 | 6.3, (5.8, 7.3) | 5.3, (4.9, 5.6) | <0.001 | 6.3, (5.7, 7.4) | 5.9, (5.4, 6.7) | <0.001 |
| Other recorded variables | ||||||||||
| Age (years) | 76, (68, 85) | 78, (70, 86) | 71, (68, 78.8) | <0.001 | 74, (68, 81) | 86, (80, 89) | <0.001 | 72, (67, 79) | 81, (72, 86) | <0.001 |
| Number of present teeth | 23, (14, 27) | 22, (12, 26) | 25, (20, 28) | <0.001 | 24, (17, 27) | 20, (7, 25) | <0.001 | 26, (21, 28) | 19, (8, 25) | <0.001 |
| Number of functional teeth | 28, (27, 28) | 28, (27, 28) | 28, (27, 28) | 0.081 | 28, (27, 28) | 28, (27, 28) | 0.046 | 28, (27, 28) | 28, (27, 28) | 0.028 |
| Body mass index (kg/m2) | 22.5, (20.6, 24.7) | 22.0, (20.2, 24.3) | 23.4, (21.7, 25.2) | <0.001 | 22.8, (20.8, 24.9) | 21.1, (18.8, 22.9) | <0.001 | 22.8, (20.8, 24.8) | 22.3, (20.3, 24.5) | 0.056 |
| Education (years) | 12, (12, 16) | 12, (11, 14) | 16, (12, 16) | <0.001 | 12, (12, 16) | 12, (10, 12) | <0.001 | 12, (12, 16) | 12, (10, 14) | <0.001 |
| JST-IC score | 12, (9, 14) | 12, (9, 14) | 12, (10, 14) | 0.009 | 12, (10, 14) | 9, (7, 12) | <0.001 | 13, (11, 14) | 11, (8, 13) | <0.001 |
| MMSE-J score | 29, (28, 30) | 29, (28, 30) | 29, (28, 30) | 0.138 | 29, (28, 30) | 29, (27, 29) | <0.001 | 29, (28, 30) | 29, (27, 30) | <0.001 |
| Serum albumin (g/dL) | 4.2, (4.1, 4.4) | 4.3, (4.1, 4.4) | 4.2, (4.1, 4.4) | 0.073 | 4.3, (4.1, 4.4) | 4.2, (4.0, 4.4) | 0.001 | 4.3, (4.1, 4.4) | 4.2, (4.1, 4.4) | 0.008 |
| Hemoglobin A1c (%) | 5.7, (5.5, 6.0) | 5.7, (5.5, 6.0) | 5.6, (5.4, 6.0) | 0.282 | 5.7, (5.5, 6.0) | 5.6, (5.4, 6.0) | 0.493 | 5.7, (5.5, 6.0) | 5.7, (5.4, 6.0) | 0.635 |
| Overall | Women | Men | Robust | Sarcopenia | Robust | Oral Hypofunction | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| (n = 878) | (n = 610) | (n = 268) | (n = 715) | (n = 163) | (n = 435) | (n = 443) | |||||
| Category Variables | N, (%) | N, (%) | N, (%) | p-Value | N, (%) | N, (%) | p-Value | N, (%) | N, (%) | p-Value | |
| Variables of oral hypofunction | |||||||||||
| Poor oral hygiene | 254, (28.9) | 154, (25.2) | 100, (37.3) | <0.001 | 217, (30.3) | 37, (22.7) | 0.052 | 87, (20.0) | 167, (37.7) | <0.001 | |
| Oral dryness | 414, (47.2) | 307, (50.3) | 107, (39.9) | 0.004 | 327, (45.7) | 87, (53.4) | 0.078 | 130, (29.9) | 284, (64.1) | <0.001 | |
| Reduced occlusal force | 352, (40.1) | 291, (47.7) | 61, (22.8) | <0.001 | 256, (35.8) | 96, (58.9) | <0.001 | 72, (16.6) | 280, (63.2) | <0.001 | |
| Decreased tongue–lip motor function | 485, (55.2) | 343, (56.2) | 142, (53.0) | 0.373 | 363, (50.8) | 122, (74.8) | <0.001 | 147, (33.8) | 338, (76.3) | <0.001 | |
| Oral diadochokinesis/pa/ | <6 times/s | 236, (26.9) | 179, (29.3) | 57, (21.3) | 0.013 | 167, (23.4) | 69, (42.3) | <0.001 | 65, (14.9) | 171, (38.6) | <0.001 |
| Oral diadochokinesis/ta/ | <6 times/s | 250, (28.5) | 186, (30.5) | 64, (23.9) | 0.046 | 180, (25.2) | 70, (42.9) | <0.001 | 68, (15.6) | 182, (41.1) | <0.001 |
| Oral diadochokinesis/ka/ | <6 times/s | 440, (50.1) | 309, (50.7) | 131, (48.9) | 0.628 | 327, (45.7) | 113, (69.3) | <0.001 | 134, (30.8) | 306, (69.1) | <0.001 |
| Decreased tongue pressure | 285, (32.5) | 216, (35.4) | 69, (25.7) | 0.005 | 193, (27.0) | 92, (56.4) | <0.001 | 62, (14.3) | 223, (50.3) | <0.001 | |
| Decreased masticatory function | 191, (21.8) | 164, (26.9) | 27, (10.1) | <0.001 | 123, (17.2) | 68, (41.7) | <0.001 | 16, (3.7) | 175, (39.5) | <0.001 | |
| Deterioration of swallowing function | 256, (29.2) | 174, (28.5) | 82, (30.6) | 0.534 | 197, (27.6) | 59, (36.2) | 0.028 | 65, (14.9) | 191, (43.1) | <0.001 | |
| Oral hypofunction | 443, (50.5) | 335, (54.9) | 108, (40.3) | <0.001 | 324, (45.3) | 119, (73.0) | <0.001 | - | - | ||
| Variables of sarcopenia | |||||||||||
| Low muscle strength | 215, (24.5) | 174, (28.5) | 41, (15.3) | <0.001 | 77, (10.8) | 138, (84.7) | <0.001 | 64, (14.7) | 151, (34.1) | <0.001 | |
| Low physical performance | 114, (13.0) | 97, (15.9) | 17, (6.3) | <0.001 | 52, (7.3) | 62, (38.0) | <0.001 | 24, (5.5) | 90, (20.3) | <0.001 | |
| Low appendicular skeletal muscle mass | 348, (39.6) | 279, (45.7) | 69, (25.7) | <0.001 | 185, (25.9) | 163, (100.0) | <0.001 | 141, (32.4) | 207, (46.7) | <0.001 | |
| Sarcopenia | Robust | 715, (81.4) | 473, (77.5) | 242, (90.3) | <0.001 | 715, (100.0) | 0, (0) | <0.001 | 391, (89.9) | 324, (73.1) | <0.001 |
| Sarcopenia | 126, (14.4) | 106, (17.4) | 20, (7.5) | 0, (0) | 126, (77.3) | 42, (9.7) | 84, (19.0) | ||||
| Severe sarcopenia | 37, (4.2) | 31, (5.1) | 6, (2.2) | 0, (0) | 37, (22.7) | 2, (0.5) | 35, (7.9) | ||||
| Other recorded variables | |||||||||||
| Sex | Women | 610, (69.5) | - | - | 473, (66.2) | 137, (84.0) | <0.001 | 275, (63.2) | 335, (75.6) | <0.001 | |
| Body mass index | <18.5 | 85, (9.7) | 72, (11.8) | 13, (4.9) | 0.001 | 51, (7.1) | 34, (20.9) | <0.001 | 37, (8.5) | 48, (10.8) | 0.243 |
| Daily drinking habits | 139, (15.8) | 47, (7.7) | 92, (34.3) | <0.001 | 122, (17.1) | 17, (10.4) | 0.036 | 81, (18.6) | 58, (13.1) | 0.025 | |
| Smoking habit | Never smoked | 617, (70.3) | 528, (86.6) | 89, (33.2) | <0.001 | 483, (67.6) | 134, (82.2) | 0.001 | 282, (64.8) | 335, (75.6) | 0.002 |
| Used to smoke | 209, (23.8) | 60, (9.8) | 149, (55.6) | 186, (26.0) | 23, (14.1) | 121, (27.8) | 88, (19.9) | ||||
| Smoking | 52, (5.9) | 22, (3.6) | 30, (11.2) | 46, (6.4) | 6, (3.7) | 32, (7.4) | 20, (4.5) | ||||
| Living situation | Living alone | 266, (30.3) | 224, (36.7) | 42, (15.7) | <0.001 | 202, (28.3) | 64, (39.3) | 0.006 | 119, (27.4) | 147, (33.2) | 0.060 |
| Depression | 159, (18.1) | 124, (20.3) | 35, (13.1) | 0.010 | 111, (15.5) | 48, (29.4) | <0.001 | 49, (11.3) | 110, (24.8) | <0.001 | |
| Stroke | 46, (5.2) | 24, (3.9) | 22, (8.2) | 0.009 | 42, (5.9) | 4, (2.5) | 0.077 | 17, (3.9) | 29, (6.5) | 0.079 | |
| Heart disease | 143, (16.3) | 97, (15.9) | 46, (17.2) | 0.641 | 110, (15.4) | 33, (20.2) | 0.129 | 67, (15.4) | 76, (17.2) | 0.482 | |
| Diabetes | 98, (11.2) | 62, (10.2) | 36, (13.4) | 0.157 | 80, (11.2) | 18, (11.0) | 0.957 | 49, (11.3) | 49, (11.1) | 0.924 | |
| Cancer | 128, (14.6) | 91, (14.9) | 37, (13.8) | 0.667 | 102, (14.3) | 26, (16.0) | 0.582 | 67, (15.4) | 61, (13.8) | 0.493 | |
| Serum albumin | <4.0 g/dL | 94, (10.7) | 66, (10.8) | 28, (10.4) | 0.870 | 60, (8.4) | 34, (20.9) | <0.001 | 38, (8.7) | 56, (12.6) | 0.061 |
| Hemoglobin A1c | <6.0% | 644, (73.3) | 446, (73.1) | 198, (73.9) | 0.069 | 524, (73.3) | 120, (73.6) | 0.958 | 319, (73.3) | 325, (73.4) | 0.959 |
| 6.0–6.4% | 137, (15.6) | 104, (17.0) | 33, (12.3) | 111, (15.5) | 26, (16.0) | 69, (15.9) | 68, (15.3) | ||||
| 6.5%≤ | 97, (11.0) | 60, (9.8) | 37, (13.8) | 80, (11.2) | 17, (10.4) | 47, (10.8) | 50, (11.3) |
| 95% Confidence Intervals | |||||
|---|---|---|---|---|---|
| Independent Variables | p-Value | Odds Ratio | Lower Limit | Upper Limit | |
| Oral hypofunction | 0:No, 1:Yes | 0.041 | 1.585 | 1.019 | 2.465 |
| Age | 1-year increments | <0.001 | 1.111 | 1.075 | 1.148 |
| Sex | 0:Women, 1:Men | 0.967 | 0.987 | 0.519 | 1.876 |
| Body mass index | 0:18.5≤, 1:<18.5 | <0.001 | 4.036 | 2.248 | 7.246 |
| Daily drinking habits | 0:No, 1:Yes | 0.746 | 1.114 | 0.579 | 2.146 |
| Smoking habit | 0:Never smoked | 0.732 | reference | ||
| 1:Used to smoke | 0.478 | 0.793 | 0.418 | 1.506 | |
| 2:Smoking | 0.639 | 0.774 | 0.265 | 2.258 | |
| Living situation | 0:Living with someone1:Living alone | 0.733 | 1.078 | 0.701 | 1.658 |
| Depression | 0:No, 1:Yes | 0.653 | 0.894 | 0.550 | 1.455 |
| Education | 1-year increments | 0.083 | 0.933 | 0.863 | 1.009 |
| JST-IC score | 1-score increments | 0.004 | 0.900 | 0.838 | 0.967 |
| MMSE-J score | 1-score increments | 0.567 | 0.975 | 0.893 | 1.064 |
| Stroke | 0:No, 1:Yes | 0.126 | 0.409 | 0.130 | 1.285 |
| Heart disease | 0:No, 1:Yes | 0.493 | 1.196 | 0.716 | 1.998 |
| Diabetes | 0:No, 1:Yes | 0.868 | 1.067 | 0.493 | 2.310 |
| Cancer | 0:No, 1:Yes | 0.873 | 1.045 | 0.607 | 1.801 |
| Serum albumin | 0:4.0 g/dL≤, 1:<4.0 g/dL | 0.013 | 1.995 | 1.157 | 3.439 |
| Hemoglobin A1c | 0:<6.0% | 0.333 | reference | ||
| 1:6.0–6.4% | 0.138 | 0.650 | 0.368 | 1.148 | |
| 2:6.5%≤ | 0.656 | 0.834 | 0.375 | 1.855 | |
| Constant | <0.001 | 0.001 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kugimiya, Y.; Iwasaki, M.; Ohara, Y.; Motokawa, K.; Edahiro, A.; Shirobe, M.; Watanabe, Y.; Obuchi, S.; Kawai, H.; Fujiwara, Y.; et al. Relationship between Oral Hypofunction and Sarcopenia in Community-Dwelling Older Adults: The Otassha Study. Int. J. Environ. Res. Public Health 2021, 18, 6666. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18126666
Kugimiya Y, Iwasaki M, Ohara Y, Motokawa K, Edahiro A, Shirobe M, Watanabe Y, Obuchi S, Kawai H, Fujiwara Y, et al. Relationship between Oral Hypofunction and Sarcopenia in Community-Dwelling Older Adults: The Otassha Study. International Journal of Environmental Research and Public Health. 2021; 18(12):6666. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18126666
Chicago/Turabian StyleKugimiya, Yoshihiro, Masanori Iwasaki, Yuki Ohara, Keiko Motokawa, Ayako Edahiro, Maki Shirobe, Yutaka Watanabe, Shuichi Obuchi, Hisashi Kawai, Yoshinori Fujiwara, and et al. 2021. "Relationship between Oral Hypofunction and Sarcopenia in Community-Dwelling Older Adults: The Otassha Study" International Journal of Environmental Research and Public Health 18, no. 12: 6666. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18126666