
Training Healthcare Professionals on How to Promote Physical Activity in the UK: A Scoping Review of Current Trends and Future Opportunities


Abstract
:1. Introduction
2. Materials and Methods
2.1. First Stage: Aim and Research Questions
2.2. Second Step: Relevant Studies Identified
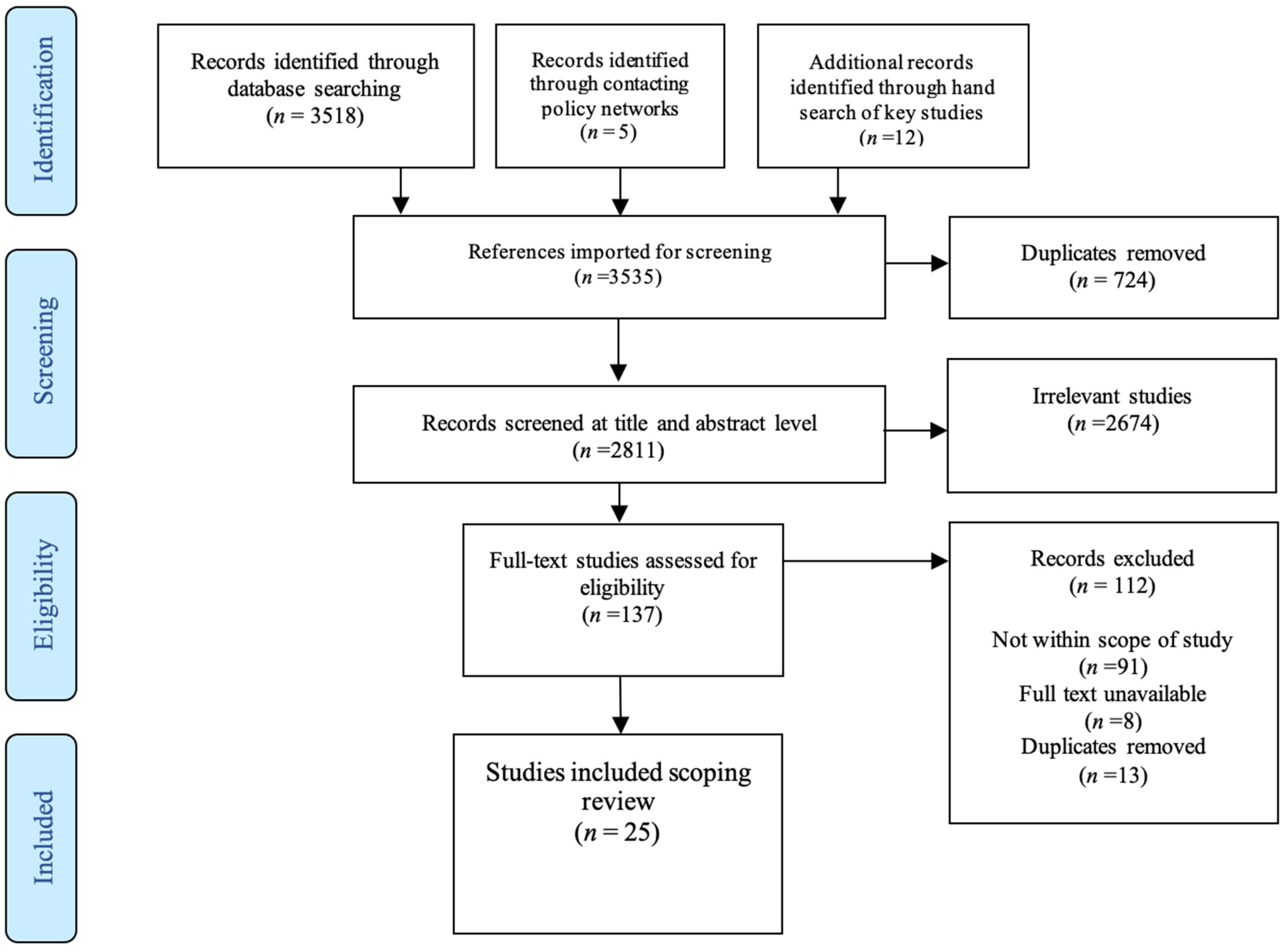
2.3. Third Step: Study Selection
2.4. Fourth Step: Charting the Data
2.5. Fifth Step: Collating, Summarising and Reporting Results
2.6. Patient and Public Involvement
3. Results
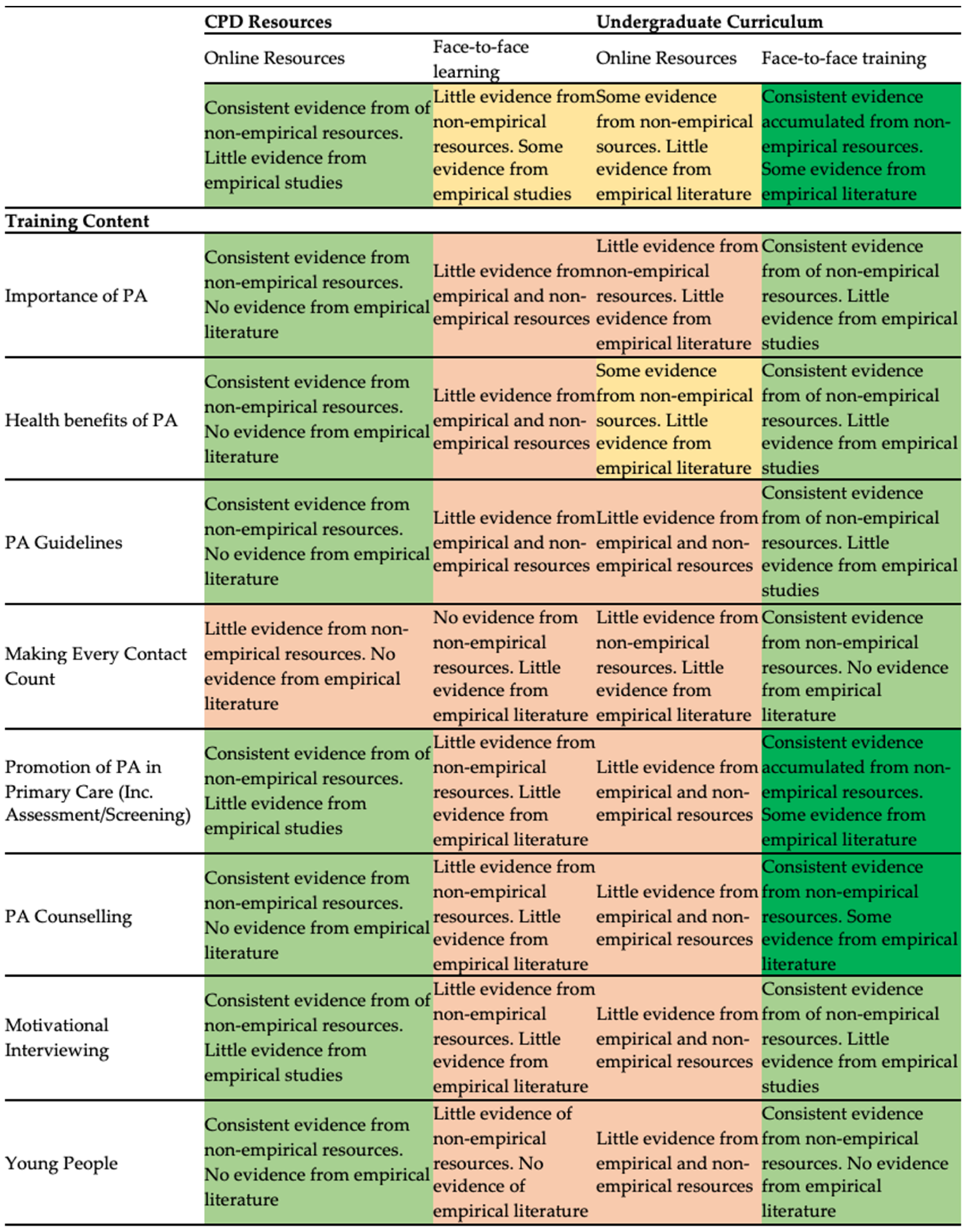
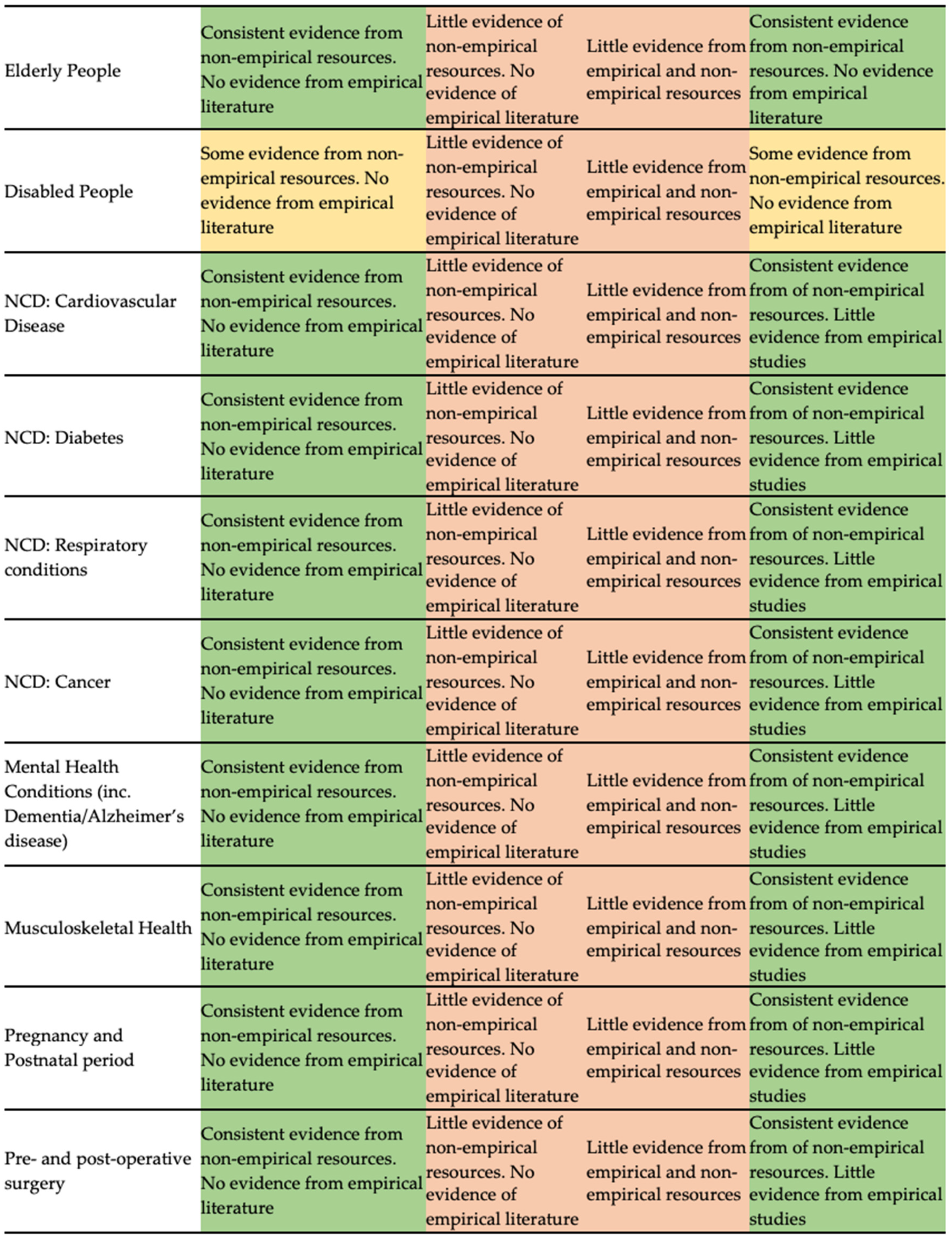
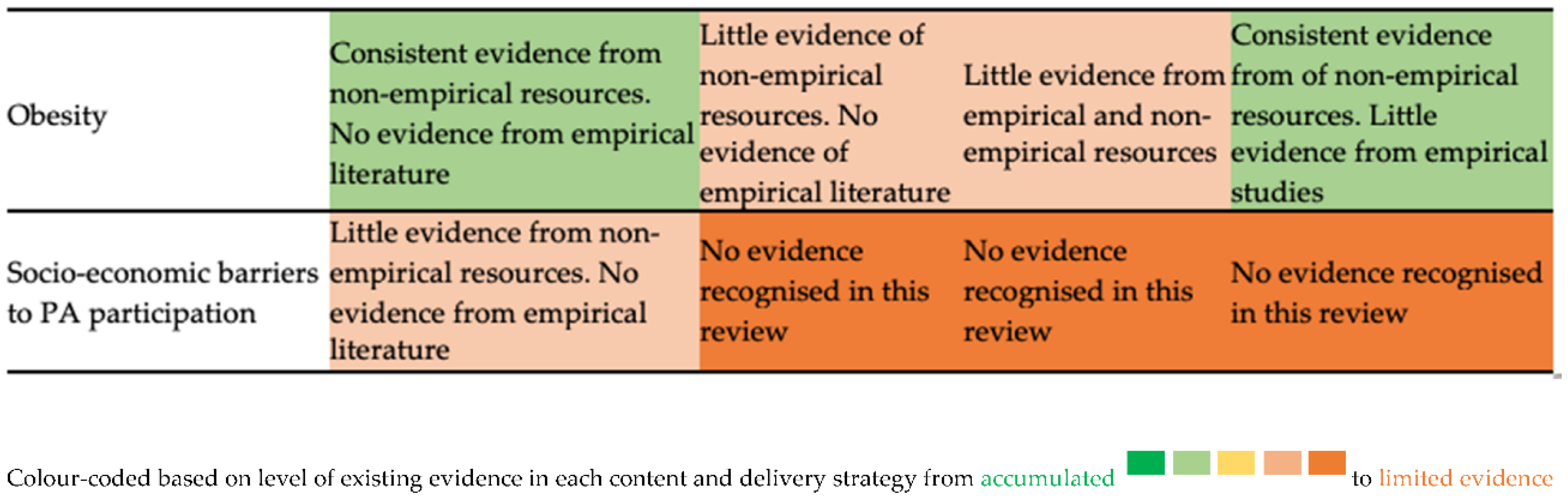
3.1. What Physical Activity Training Content do HCPs Currently Receive?
3.1.1. Health Benefits of PA
3.1.2. PA Promotion in Healthcare
3.1.3. PA and Behaviour Change
3.2. How Is PA Training Delivered to HCPs?
3.2.1. E-Learning
3.2.2. Face-To-Face Learning
4. Discussion—What Now? What Next? Discussing Results, Identifying Gaps, and Providing Directions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Global Action Plan on Physical Activity 2018–2030: More Active People for a Healthier World. World Health Organization, 2018. Available online: https://apps.who.int/iris/bitstream/handle/10665/272722/9789241514187-eng.pdf?ua=1/ (accessed on 10 December 2020).
- International Society for Physical Activity and Health (ISPAH). ISPAH’s Eight Investments That Work for Physical Activity. 2020. Available online: https://www.ispah.org/wp-content/uploads/2020/11/English-Eight-Investments-That-Work-FINAL.pdf (accessed on 10 January 2021).
- Milton, K.; Larner, J.; Hanson, S.; Jones, A. Embedding Physical Activity into the Healthcare Curriculum—A Case Study. Educ. Prim. Care 2020, 31, 176–179. [Google Scholar] [CrossRef]
- Sport England. Tackling Inactivity: An Overview of Key Work to Support Health Care Professionals, and Affiliated Roles, to Embed Physical Activity in Their Practice for Active Partnerships and Local Delivery Pilots; Sport England: London, UK, 2016. [Google Scholar]
- Orrow, G.; Kinmonth, A.L.; Sanderson, S.; Sutton, S. Effectiveness of physical activity promotion based in primary care: Systematic review and meta-analysis of randomised controlled trials. BMJ 2012, 344, e1389. [Google Scholar] [CrossRef] [Green Version]
- National Institute for Health and Care Excellence. Physical Activity: Brief Advice for Adults in Primary Care. NICE, 2013. Available online: https://www.nice.org.uk/guidance/ph44/resources/physical-activity-brief-advice-for-adults-in-primary-care-pdf-1996357939909 (accessed on 17 December 2020).
- Weiler, R.; Chew, S.; Coombs, N.; Hamer, M.; Stamatakis, E. Physical activity education in the undergraduate curricula of all UK medical schools. Are tomorrow’s doctors equipped to follow clinical guidelines? Br. J. Sports Med. 2012, 46, 1024–1026. [Google Scholar] [CrossRef]
- Booth, H.P.; Prevost, A.T.; Gulliford, M.C. Access to weight reduction interventions for overweight and obese patients in UK primary care: Population-based cohort study. BMJ Open 2015, 5, e006642. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chatterjee, R.; Chapman, T.; Brannan, M.G.; Varney, J. GPs’ knowledge, use, and confidence in national physical activity and health guidelines and tools: A questionnaire-based survey of general practice in England. Br. J. Gen. Pract. 2017, 67, e668–e675. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shuval, K.; Leonard, T.; Drope, J.; Katz, D.L.; Patel, A.V.; Maitin-Shepard, M.; Amir, O.; Grinstein, A. Physical activity counseling in primary care: Insights from public health and behavioral economics. CA A Cancer J. Clin. 2017, 67, 233–244. [Google Scholar] [CrossRef] [Green Version]
- Rose, S.A.; Poynter, P.S.; Anderson, J.W.; Noar, S.M.; Conigliaro, J. Physician weight loss advice and patient weight loss behavior change: A literature review and meta-analysis of survey data. Int. J. Obes. 2013, 37, 118–128. [Google Scholar] [CrossRef] [Green Version]
- Vishnubala, D.; Pringle, A. Working with healthcare professionals to promote physical activity. Perspect. Public Health 2021, 141, 111–113. [Google Scholar] [CrossRef]
- Sport England. Moving Healthcare Professionals. Sport England, 2021. Available online: https://www.sportengland.org/campaigns-and-our-work/moving-healthcare-professionals (accessed on 20 January 2021).
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Levac, D.; Colquhoun, H.; O’Brien, K.K. Scoping studies: Advancing the methodology. Implement. Sci. 2010, 5, 69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peters, M.D.J.; Marnie, C.; Tricco, A.C.; Pollock, D.; Munn, Z.; Alexander, L.; McInerney, P.; Godfrey, C.M.; Khalil, H. Updated methodological guidance for the conduct of scoping reviews. JBI Evid. Synth. 2020, 18, 2119–2126. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matters, G. A Practical Tool for Searching Health-Related Grey Literature. CADTH, 2018. Available online: https:www.cadth.ca/resources/finding-evidence (accessed on 17 December 2020).
- Bird, W. Physical Activity in the Treatment of Long Term Health Conditions. BMJ, 2014. Available online: https://0-learning-bmj-com.brum.beds.ac.uk/learning/course-intro/physical-activity.html?courseId=10051913 (accessed on 10 December 2020).
- E-Learning for Healthcare. Physical Activity and Health. E-Learning for Healthcare. Available online: https://www.e-lfh.org.uk/programmes/physical-activity-and-health/ (accessed on 10 December 2020).
- Gates, A.B.; Swainson, M.G.; Isba, R.; Wheatley, R.G.; Curtis, F.A. Movement for Movement: A practical insight into embedding physical activity into the undergraduate medical curriculum exemplified by Lancaster Medical School. Br. J. Sports Med. 2019, 53, 609–610. [Google Scholar] [CrossRef] [PubMed]
- Waterall, J. New tools to help boost your prevention impact. Pract. Nurs. 2019, 30, 244–245. [Google Scholar] [CrossRef]
- Gates, A.B. Training tomorrow’s doctors, in exercise medicine, for tomorrow’ patients. Br. J. Sports Med. 2015, 49, 207–208. [Google Scholar] [CrossRef]
- Gates, A.B.; Ritchie, I.K. Embedding Physical Activity in the Undergraduate Curriculum; Public Health England (PHE), Sport England: London, UK, 2018. [Google Scholar]
- Gates, A.B.; Ritchie, I.K. Appendices: Embedding Physical Activity in the Undergraduate Curriculum; Public Health England (PHE), Sport England: London, UK, 2018. [Google Scholar]
- Pugh, G.; O’Halloran, P.; Blakey, L.; Leaver, H.; Angioi, M. Integrating physical activity promotion into UK medical school curricula: Testing the feasibility of an educational tool developed by the Faculty of Sports and Exercise Medicine. BMJ Open Sport Exerc. Med. 2020, 6, e000679. [Google Scholar] [CrossRef]
- Gates, A. How to Use the “Movement for Movement” Resources. Movement for Movement, 2017. Available online: https://councilofdeans.org.uk/wp-content/uploads/2017/11/2017-VERSION-HOW-TO-USE-THE-MOVEMENT-FOR-MOVEMENT-RESOURCES-GUIDE.pdf (accessed on 24 December 2020).
- Gates, A. How to Use the ‘Movement for Movement’ Resources Erasmus+ 2020–2025 Update. Movement for Movement, 2020. Available online: https://councilofdeans.org.uk/wp-content/uploads/2020/11/ERASMUS-How-to-use-the-resources-in-medical-and-health-education-1.pdf (accessed on 24 December 2020).
- Motivate2Move. 2020. Available online: https://gpcpd.heiw.wales/clinical/motivate-2-move/ (accessed on 10 December 2020).
- Moving Medicine. Find the Right Consultation. Moving Medicine. Available online: https://movingmedicine.ac.uk/ (accessed on 1 December 2020).
- Public Health Scotland. Encouraging and Enabling Physical Activity. Public Health Scotland. Available online: https://elearning.healthscotland.com/course/view.php?id=581 (accessed on 10 December 2020).
- Gates, A.B.; Ritchie, I.K.; Moffatt, F.; Breda, J. Leadership in physical activity: Is this the currency of change in the student healthcare curriculum? Br. J. Sports Med. 2018, 52, 1484–1485. [Google Scholar] [CrossRef]
- Jones, P.R.; Brooks, J.H.M.; Wylie, A. Realising the potential for an Olympic legacy; teaching medical students about sport and exercise medicine and exercise prescribing. Br. J. Sports Med. 2013, 47, 1090–1094. [Google Scholar] [CrossRef] [Green Version]
- Copeland, R.J.; Quirk, H.; Crank, H.; Broom, D.; Goldsmith, S. Evaluation of the Public Health England and Sport England Funded Sport and Exercise Medicine Pilot in Secondary Care; Sheffield Hallam University: Sheffield, UK, 2020. [Google Scholar] [CrossRef]
- Copeland, R.J.; Quirk, H.; Crank, H.; Broom, D.; Goldsmith, S. Evaluation of the Public Health England and Sport England Funded Physical Activity Clinical Advice Pad Pilot in Primary Care; Sheffield Hallam University: Sheffield, UK, 2020. [Google Scholar] [CrossRef]
- Carlin, E.; Musson, H.; Adams, E.J. Evaluation of the Clinical Champions’ Physical Activity Training Programme (Moving Healthcare Professionals Phase 1); National Centre for Sport and Exercise Medicine, School of Sport, Exercise and Health Sciences, Loughborough University: Loughborough, UK, 2019. [Google Scholar]
- Gates, A.B. Making every contact count for physical activity—for tomorrow’s patients: The launch of the interdisciplinary, undergraduate, resources on exercise medicine and health in the UK. Br. J. Sports Med. 2016, 50, 322–323. [Google Scholar] [CrossRef]
- Sport England. We Are Undefeatable. Sport England, 2021. Available online: https://weareundefeatable.co.uk/ (accessed on 3 February 2021).
- World Health Organization Social Determinants of Health. World Health Organization, 2014. Available online: https://www.who.int/health-topics/social-determinants-of-health#tab=tab_1 (accessed on 2 February 2021).
- Ruiz, J.G.; Mintzer, M.J.; Leipzig, R.M. The impact of E-learning in medical education. Acad. Med. 2006, 81, 207–212. [Google Scholar] [CrossRef]
- Brannan, M.; Bernardotto, M.; Clarke, N.; Varney, J. Moving healthcare professionals—A whole system approach to embed physical activity in clinical practice. BMC Med Educ. 2019, 19. [Google Scholar] [CrossRef] [Green Version]
- Lowe, A.; Gates, A.; Callaghan, P. Special interest report: Making every contact count for physical activity: Equipping tomorrow’s physiotherapists to deliver high quality physical activity interventions. Physiotherapy 2016, 102, e45–e46. [Google Scholar] [CrossRef] [Green Version]
- Osborne, S.A.; Adams, J.M.; Fawkner, S.; Kelly, P.; Murray, A.D.; Oliver, C.W. Tomorrow’s doctors want more teaching and training on physical activity for health. Br. J. Sports Med. 2017, 51, 624. [Google Scholar] [CrossRef] [Green Version]
- Carroll, N. E-learning—the McDonaldization of education. Eur. J. High. Educ. 2013, 3, 342–356. [Google Scholar] [CrossRef]
- Kirk, D. Curriculum work in physical education: Beyond the objectives approach? J. Teach. Phys. Educ. 1993, 244–265. [Google Scholar] [CrossRef]
- Bleakley, A. Embracing ambiguity: Curriculum design and activity theory. Med. Teach. 2021, 43, 14–18. [Google Scholar] [CrossRef] [PubMed]
- Dishman, R.K.; Heath, G.; Schmidt, M.D.; Lee, I.-M. Physical Activity Epidemiology; Human Kinetics: Champaign, IL, USA, 2021. [Google Scholar]
- Agiovlasitis, S.; Yun, J.; Jin, J.; McCubbin, J.A.; Motl, R.W. Physical Activity Promotion for Persons Experiencing Disability: The Importance of Interdisciplinary Research and Practice. Adapt. Phys. Activ. Q. 2018, 35, 437–457. [Google Scholar] [CrossRef]
- Radonjic, A.; Evans, E.L. Should the Medical Humanities Be Vital to Curricula? Acad. Med. 2020, 95, 819. [Google Scholar] [CrossRef] [PubMed]
- Wald, H.S.; McFarland, J.; Markovina, I. Medical humanities in medical education and practice. Med. Teach. 2018, 41, 492–496. [Google Scholar] [CrossRef] [PubMed]
- Warnecke, E.; Pearson, S. Medical students’ perceptions of using e-learning to enhance the acquisition of consulting skills. Australas. Med. J. 2011, 4, 300–307. [Google Scholar] [CrossRef] [PubMed]
- Hew, K.F.; Lo, C.K. Flipped classroom improves student learning in health professions education: A meta-analysis. BMC Med. Educ. 2018, 18. [Google Scholar] [CrossRef] [Green Version]
- Jones, D.M.; Anderson Crow, D. How can we use the ‘science of stories’ to produce persuasive scientific stories? Palgrave Commun. 2017, 3. [Google Scholar] [CrossRef] [Green Version]
- Casper, A.M.A.; Balgopal, M.M. How guest experts tell stories about environmental socio-scientific issues in an undergraduate class. Int. J. Sci. Educ. 2020, 42, 1568–1584. [Google Scholar] [CrossRef]
- Smith, B.; Tomasone, J.R.; Latimer-Cheung, A.E.; Martin Ginis, K.A. Narrative as a knowledge translation tool for facilitating impact: Translating physical activity knowledge to disabled people and health professionals. Health Psychol. 2015, 34, 303–313. [Google Scholar] [CrossRef] [PubMed]
- Din, N.U.; Moore, G.F.; Murphy, S.; Wilkinson, C.; Williams, N.H. Health professionals’ perspectives on exercise referral and physical activity promotion in primary care: Findings from a process evaluation of the National Exercise Referral Scheme in Wales. Health Educ. J. 2015, 74, 743–757. [Google Scholar] [CrossRef] [Green Version]
- Kime, N.; Pringle, A.; Zwolinsky, S.; Vishnubala, D. How prepared are healthcare professionals for delivering physical activity guidance to those with diabetes? A formative evaluation. BMC Health Serv. Res. 2020, 20, 1–12. [Google Scholar] [CrossRef]
- Albert, F.A.; Crowe, M.J.; Malau-Aduli, A.E.; Malau-Aduli, B.S. Physical activity promotion: A systematic review of the perceptions of healthcare professionals. Int. J. Environ. Res. Public Health 2020, 17, 4358. [Google Scholar] [CrossRef]
- Williamson, C.; Baker, G.; Mutrie, N.; Niven, A.; Kelly, P. Get the message? A scoping review of physical activity messaging. Int. J. Behav. Nutr. Phys. Act. 2020, 17. [Google Scholar] [CrossRef]
- Smith, B.; Wightman, L. Promoting physical activity to disabled people: Messengers, messages, guidelines and communication formats. Disabil. Rehabil. 2019, 1–5. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| UK-based research articles | Abstracts without full text |
| Research conducted in any student or HCP populations | Articles focusing on the behaviour change of the participant not within the scope of this review (e.g., investigating the PA behaviours of medical students) |
| Articles published in peer-reviewed or Grey literature | Articles that did not include the concept of what PA training was included within participant training |
| Articles published in English | Articles that did not include the context of how PA training was delivered to participants |
| Research designs including, but not limited to; qualitative, natural experiment with pre-post measures, content analysis, systematic or non-systematic reviews, commentary, theory, summary, policy, or practice papers | Non-UK based research articles |
| Articles stating the context and concept of the applied training delivered to the relevant participant | Articles not in English language |
| Training resources highlighted within literature |
| Curricula Content | BMJ E-Learning (MHPP) [20] | E-Learning for Healthcare (MHPP) [19] | Movementfor Movement (Based on ERASMUS How-to Guide) [28] | Motivate2Move [29] | Moving Medicine [30] | Public Health Scotland [31] |
|---|---|---|---|---|---|---|
| Importance of PA | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Health benefits of PA | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| PA Guidelines | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Promotion of PA in Primary Care | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| PA Counselling | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Motivational Interviewing | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Young People | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Elderly People | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Disabled People | ✓ * | ✓ * | ✓ | ✓ | ✓ | ✓ |
| NCD: Cardiovascular Disease | ✓ | ✓ | ✓ | ✓ | ✓ | ✕ |
| NCD: Diabetes | ✓ | ✓ | ✓ | ✓ | ✓ | ✕ |
| NCD: Cancer | ✓ | ✓ | ✓ | ✓ | ✓ | ✕ |
| Mental Health Conditions (inc. Dementia/Alzheimer’s disease) | ✓ | ✓ | ✓ | ✓ | ✓ | ✕ |
| Musculoskeletal Health | ✓ | ✓ | ✓ | ✓ | ✓ | ✕ |
| Pregnancy and Postnatal period | ✕ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Socio-economic barriers to PA participation | ✕ | ✕ | _ ** | ✕ | ✓ | ✓ |
| Resource | Movement for Movement [28] | BMJ Learning [19] | E-Learning for Healthcare [20] | Motivate2Move [29] | Public Health Scotland [31] | Moving Medicine [30] |
|---|---|---|---|---|---|---|
| Who does this training target? | Undergraduate curriculum | CPD training | CPD training | CPD training | CPD training | CPD training |
| How training is disseminated? | Slide-set resources to be embedded in Undergraduate education | E-learning | E-Learning | Online resources and factsheets | E-learning | Online consultation guide |
| Training content chapters | Leadership on PA in health and wellbeing | The importance of PA | Introduction to PA | UK PA guidelines | What is PA? | PA and patient age type |
| World Health Organization (WHO) and UK PA guidelines and recommendations | How does PA produce health benefits? | Promoting PA in primary care | All-cause mortality (longevity) | UK Chief Medical Officers’ (CMO) guidelines | PA and stroke | |
| MECC | The health benefits of PA: cancer | Children and young people: Being active | Cancer | How active are we? | PA and amputee | |
| Brief interventions and making every influence matter | The health benefits of PA: Diabetes | Older adults: Being active | PA and cardiovascular health | Benefits of PA | PA and cancer | |
| Cancer and exercise | The health benefits of PA: osteoarthritis and lower back pain | Cardiovascular conditions: Being active | Chronic kidney disease | Key Messages | PA and Chronic Obstructive Pulmonary Disease (COPD) | |
| CVD, exercise and cardiac rehabilitation | The health benefits of PA: cardiovascular disease | Type 2 Diabetes: Being active | PA & mental health | National PA pathway | PA and Dementia | |
| T2 Diabetes and exercise | The health benefits of PA: respiratory disease | Cancer conditions: Being active | Neurological disorders | Raising PA | PA and Depression | |
| Mental health and exercise | The health benefits of PA: depression, anxiety, sleep, and dementia | Mental health: Being active | Obesity | Screening for activity | PA and inflammatory rheumatic disease | |
| Osteoporosis, sarcopenia and exercise | The health benefits of PA: promoting PA in primary care | Musculoskeletal health: Being active | PA and pregnancy | Delivering PA advice | PA and ischaemic heart disease | |
| Fall and exercise | Pregnancy and postnatal period: Being active | PA and respiratory disease | Signposting and referral | PA and musculoskeletal pain | ||
| COPD, exercise and pulmonary rehabilitation | Motivational Interviewing video | Sedentary behaviour | Follow up and review | PA and primary prevention | ||
| Surgery and exercise | Supporting people to change their health behaviour | Key resources | PA and type 2 Diabetes | |||
| Hypertension and exercise | Starting to exercise | PA and pregnancy | ||||
| Stroke, exercise and rehabilitation | Resources for primary care | Support and local activities | ||||
| Deconditioning and exercise | Why movement matters | |||||
| Obesity and exercise | Consensus statement | |||||
| Rheumatoid arthritis and exercise | Case studies ‘We Are Undefeatable’ | |||||
| Pregnancy pre/post and exercise | ||||||
| Chronic kidney disease and exercise | ||||||
| Environment, health and PA | ||||||
| Intellectual disability and PA | ||||||
| School for change agency and leadership | ||||||
| Leadership on PA in health and wellbeing |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Netherway, J.; Smith, B.; Monforte, J. Training Healthcare Professionals on How to Promote Physical Activity in the UK: A Scoping Review of Current Trends and Future Opportunities. Int. J. Environ. Res. Public Health 2021, 18, 6701. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18136701
Netherway J, Smith B, Monforte J. Training Healthcare Professionals on How to Promote Physical Activity in the UK: A Scoping Review of Current Trends and Future Opportunities. International Journal of Environmental Research and Public Health. 2021; 18(13):6701. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18136701
Chicago/Turabian StyleNetherway, Jake, Brett Smith, and Javier Monforte. 2021. "Training Healthcare Professionals on How to Promote Physical Activity in the UK: A Scoping Review of Current Trends and Future Opportunities" International Journal of Environmental Research and Public Health 18, no. 13: 6701. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18136701