
Prevalence of Depression during Pregnancy in Spanish Women: Trajectory and Risk Factors in Each Trimester

Abstract
:1. Introduction
- Is the trajectory of depression throughout pregnancy the same regardless of its severity?
- Do the same variables predict the presence of probable depression and of major depression?
- Which variables are the most closely associated with depression in each trimester? Are they the same, or are there trimester-specific predictors?
2. Materials and Methods
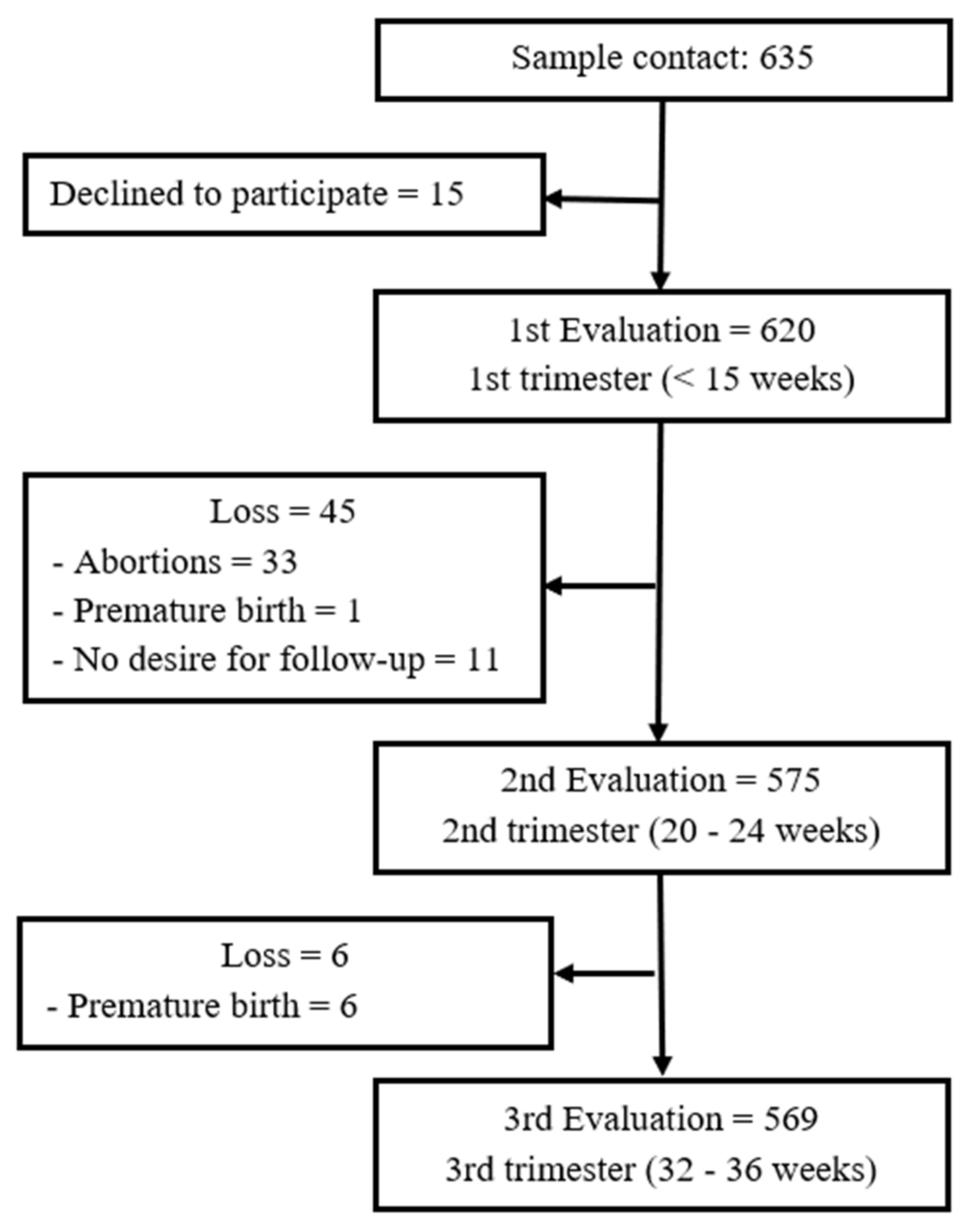
2.1. Procedure and Participants
2.2. Measures
2.2.1. Socio-Demographic and Pregnancy Information
2.2.2. Depression
2.2.3. Stress
2.2.4. Anxiety
2.3. Data Analysis
3. Results
3.1. Characteristics of the Sample
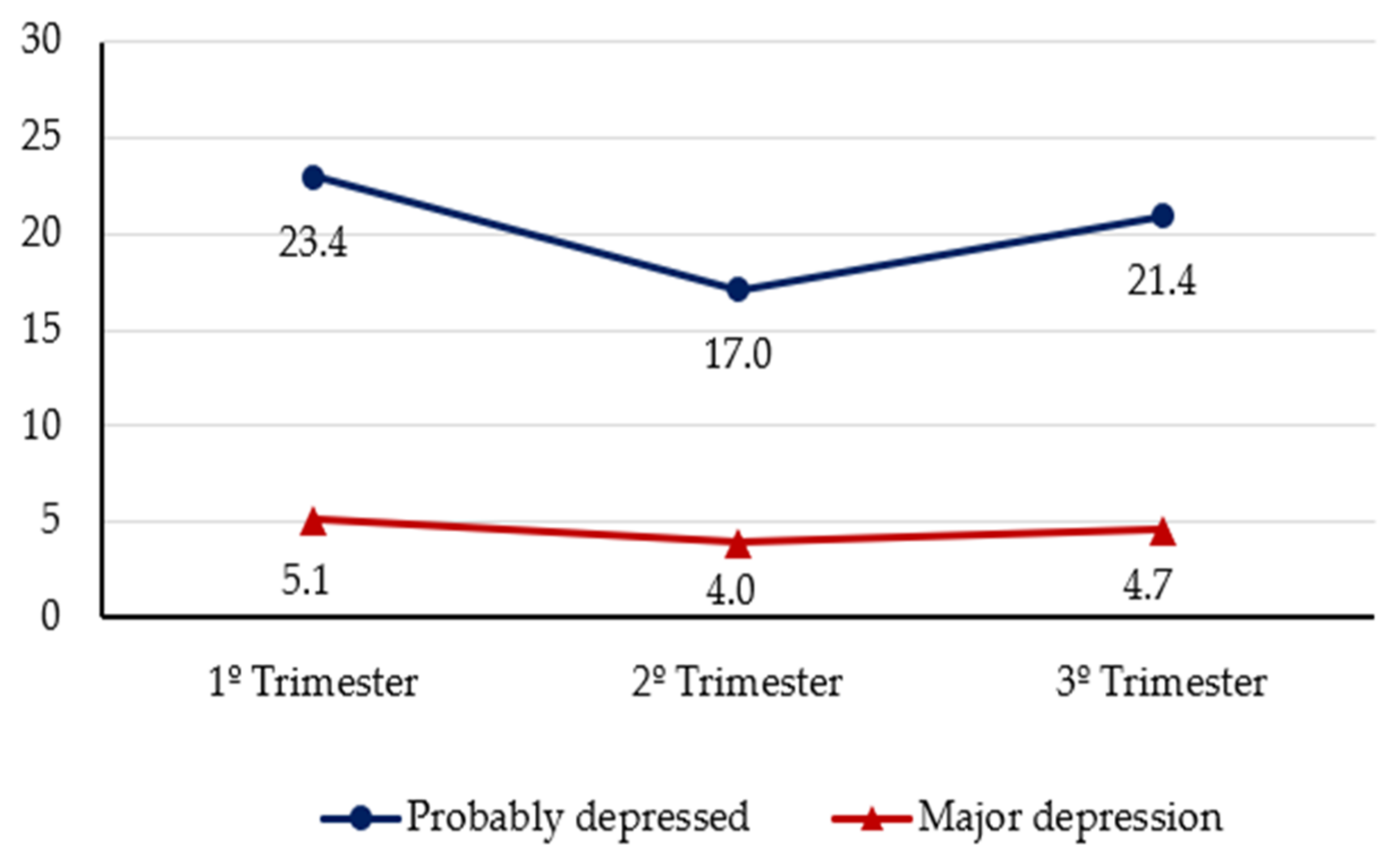
3.2. Trajectory of Depression throughout Pregnancy
3.3. Variables Associated with the Presence of Depression
3.3.1. Sociodemographic Variables
3.3.2. Pregnancy-Related Variables
3.3.3. Psychological Variables
3.4. Predictors of Depression in Each Trimester
4. Discussion
4.1. Trajectory of Depression during Pregnancy
4.2. Variables Associated with Probable Depression and Major Depression in Pregnancy
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Depresión. Datos y cifras [Depression. Data and numbers]. Available online: https://www.who.int/es/news-room/fact-sheets/detail/depression (accessed on 5 April 2019).
- Kamysheva, E.; Skouteris, H.; Wertheim, E.H.; Paxton, S.J.; Milgrom, J. A prospective investigation of the relationships among sleep quality, physical symptoms, and depressive symptoms during pregnancy. J. Affect. Disord. 2010, 123, 317–320. [Google Scholar] [CrossRef]
- Bowen, A.; Muhajarine, N. Antenatal depression. Can. Nurse 2006, 102, 26–30. [Google Scholar]
- Lee, A.M.; Lam, S.K.; Sze Mun Lau, S.M.; Chong, C.S.; Chui, H.W.; Fong, D.Y. Prevalence, course, and risk factors for antenatal anxiety and depression. Obstet. Gynecol. 2007, 110, 1102–1112. [Google Scholar] [CrossRef]
- Míguez, M.C.; Fernández, V.; Pereira, B. Depresión postparto y factores asociados en mujeres con embarazos de riesgo [Postpartum depression and associated factors in women with at-risk pregnancies]. Behav. Psychol. 2017, 25, 47–64. [Google Scholar]
- Yonkers, K.A.; Smith, M.V.; Gotman, N.; Belanger, K. Typical somatic symptoms of pregnancy and their impact on a diagnosis of major depressive disorder. Gen. Hosp. Psychiatry 2009, 31, 327–333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saeed, A.; Raana, T.; Saeed, A.M.; Humayun, A. Effect of antenatal depression on maternal dietary intake and neonatal outcome: A prospective cohort. Nutr. J. 2016, 15, 64–93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eastwood, J.; Ogbo, F.A.; Hendry, A.; Noble, J.; Page, A. The impact of antenatal depression on perinatal outcomes in australian women. PLoS ONE 2017, 12, e0169907. [Google Scholar] [CrossRef] [PubMed]
- Goedhart, G.; Snijders, A.C.; Hesselink, A.E.; Van Poppel, N.; Bonsel, G.J.; Vrijkotte, T.G.M. Maternal depressive symptoms in relation to perinatal mortality and morbidity: Results from a large multiethnic cohort study. Psychosom. Med. 2010, 72, 769–776. [Google Scholar] [CrossRef]
- Herrero, T.; Driebe, A.; Fratto, V.; Hamlin, A.; Lacoursiere, D.Y.; Ramos, G.A. Positive antenatal Edinburgh Depression Scale: Examining behavioral and pharmacological therapy on maternal and neonatal outcomes. J. Matern. Fetal Neonatal Med. 2018, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Felice, E.; Saliba, J.; Grech, V.; Cox, J. Validation of the Maltese version of the Edinburgh Postnatal Depression Scale. Arch. Womens Ment. Health 2006, 9, 75–80. [Google Scholar] [CrossRef]
- Matthey, S.; Ross-Hamid, C. Repeat testing on the Edinburgh Depression Scale and the HADS-A in pregnancy: Differentiating between transient and enduring distress. J. Affect. Disord. 2012, 141, 213–221. [Google Scholar] [CrossRef]
- Vázquez, M.B.; Míguez, M.C. Validation of the Edinburgh postnatal depression scale as a screening tool for depression in Spanish pregnant women. J. Affect. Disord. 2019, 246, 515–521. [Google Scholar] [CrossRef]
- Rallis, S.; Skouteris, H.; McCabe, M.; Milgrom, J. A prospective examination of depression, anxiety and stress throughout pregnancy. Women Birth 2014, 27, e36–e42. [Google Scholar] [CrossRef]
- Yanikkerem, E.; Ay, S.; Mutlu, S.; Goker, A. Antenatal depression: Prevalence and risk factors in a hospital based Turkish sample. J. Pak. Med. Assoc. 2013, 63, 472–477. [Google Scholar] [PubMed]
- Yu, Y.; Li, M.; Pu, L.; Wang, S.; Wu, J.; Ruan, L.; Jiang, S.; Wang, Z.; Jiang, W. Sleep was associated with depression and anxiety status during pregnancy: A prospective longitudinal study. Arch. Womens Ment. Health 2017, 20, 695–701. [Google Scholar] [CrossRef] [PubMed]
- Weng, S.C.; Huang, J.P.; Huang, Y.L.; Lee, T.S.; Chen, Y.H. Effects of tobacco exposure on perinatal suicidal ideation, depression, and anxiety. BMC Public Health 2016, 16, 623. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marchesi, C.; Bertoni, S.; Maggini, C. Major and minor depression in pregnancy. Obstet. Gynecol. 2009, 113, 1292–1298. [Google Scholar] [CrossRef]
- Ajinkya, S.; Jadhav, P.R.; Srivastava, N.N. Depression during pregnancy: Prevalence and obstetric risk factors among pregnant women attending a tertiary care hospital in Navi Mumbai. Ind. Psychiatry J. 2013, 22, 37–40. [Google Scholar] [CrossRef]
- Park, J.H.; Karmaus, W.; Zhang, H. Prevalence of and risk factors for depressive symptoms in Korean women throughout pregnancy and in postpartum period. Asian Nurs. Res. 2015, 9, 219–225. [Google Scholar] [CrossRef] [Green Version]
- Míguez, M.C.; Vázquez, M.B. Risk factors for antenatal depression: A review. World J. Psychiatr. 2021, in press. [Google Scholar]
- Bödecs, T.; Szilagyi, E.; Cholnoky, P.; Sándor, J.; Gonda, X.; Rihmer, Z.; Horváth, B. Prevalence and psychosocial background of anxiety and depression emerging during the first trimester of pregnancy: Data from a Hungarian population-based sample. Psychiatr. Danub. 2013, 25, 352–358. [Google Scholar]
- De Vargas, C.; Coll, N.; Da Silveira, M.; Garcia-Bassani, D.; Netsi, E.; César Wehrmeister, F.; … Stein, A. Antenatal depressive symptoms among pregnant women: Evidence from a Southern Brazilian population-based cohort study. J. Affect. Disord. 2017, 209, 140–146. [Google Scholar] [CrossRef] [Green Version]
- Husain, N.; Parveen, A.; Husain, M.; Saeed, Q.; Jafri, F.; Rahman, R.; Tomenson, B.; Chaudhry, I.B. Prevalence and psychosocial correlates of perinatal depression: A cohort study from urban Pakistan. Arch. Womens Ment. Health 2011, 14, 395–403. [Google Scholar] [CrossRef]
- Thompson, O.; Ajayi, I. Prevalence of antenatal depression and associated risk factors among pregnant women attending antenatal clinics in Abeokuta north local government area, Nigeria. Depress. Res. Treat. 2016, 16, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Banti, S.; Mauri, M.; Oppo, A.; Borri, C.; Rambelli, C.; Ramacciotti, D.; Montagnani, M.S.; Camilleri, V.; Cortopassi, S.; Rucci, P.; et al. From the third month of pregnancy to 1 year postpartum. Prevalence, incidence, recurrence, and new onset of depression. Results from the perinatal depression-research & screening unit study. Compr. Psychiatry 2011, 52, 343–351. [Google Scholar] [CrossRef] [PubMed]
- Benute, G.R.G.; Nomura, R.M.Y.; Reis, J.S.; Fraguas-Junior, R.; Lucia, M.C.S.; Zugaib, M. Depression during pregnancy in women with a medical disorder: Risk factors and perinatal outcomes. Clinics 2011, 65, 1127–1131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ogbo, F.A.; Eastwood, J.; Hendry, A.; Jalaludin, B.; Agho, K.E.; Barnett, B.; Page, A. Determinants of antenatal depression and postnatal depression in Australia. BMC Psychiatry 2018, 18, 49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weobong, B.; Asbroek, A.H.A.; Soremekun, S.; Manu, A.A.; Owusu-Agyei, S.; Prince, M.; Kirkwood, B.R. Association of antenatal depression with adverse consequences for the mother and newborn in rural Ghana: Findings from the DON population-based cohort study. PLoS ONE 2014, 9, e116333. [Google Scholar] [CrossRef] [Green Version]
- Giardinelli, L.; Innocenti, A.; Benni, L.; Stefanini, M.C.; Lino, G.; Lunardi, C.; Svelto, V.; Afshar, S.; Bovani, R.; Castellini, G.; et al. Depression and anxiety in perinatal period: Prevalence and risk factors in an Italian sample. Arch. Womens Ment. Health 2012, 15, 21–30. [Google Scholar] [CrossRef]
- Kheirabadi, G.R.; Maracy, M.R. Perinatal depression in a cohort study on Iranian women. J. Res. Med. Sci. 2010, 15, 41–49. [Google Scholar]
- González-Mesa, E.; Kabukcuoglu, K.; Körükcü, O.; Blasco, M.; Ibrahim, N.; Kavas, T. Cultural factors influencing antenatal depression: A cross-sectional study in a cohort of Turkish and Spanish women at the beginning of the pregnancy. J. Affect. Disord. 2018, 238, 256–260. [Google Scholar] [CrossRef]
- Mohammad, K.I.; Gamble, J.; Creedy, D.K. Prevalence and factors associated with the development of antenatal and postnatal depression among Jordanian women. Midwifery 2011, 27, 238–245. [Google Scholar] [CrossRef]
- Waldie, K.E.; Peterson, E.R.; D’Souza, S.; Underwood, L.; Pryor, J.E.; Carr, P.A.; Grant, C.; Morton, S.M.B. Depression symptoms during pregnancy: Evidence from Growing Up in New Zealand. J. Affect. Disord. 2015, 186, 66–73. [Google Scholar] [CrossRef] [PubMed]
- Fadzil, A.; Balakrishnan, K.; Razali, R.; Sidi, H.; Malapan, T.; Japaraj, R.P.; Midin, M.; Jaafar, N.R.N.; Das, S.; Manaf, M.R.A. Risk factors for depression and anxiety among pregnant women in Hospital Tuanku Bainun, Ipoh, Malaysia. Asia Pac. Psychiatry 2013, 5, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Redinger, S.; Norris, S.A.; Pearson, R.M.; Richter, L.; Rochat, T. First trimester antenatal depression and anxiety: Prevalence and associated factors in an urban population in Soweto, South Africa. J. Dev. Orig. Health Dis. 2018, 9, 30–40. [Google Scholar] [CrossRef] [Green Version]
- Rich-Edwards, J.; Kleinman, K.; Abrams, A.; Harlow, B.L.; McLaughlin, T.J.; Joffe, H.; Gillman, M.W. Sociodemographic predictors of antenatal and postpartum depressive symptoms among women in a medical group practice. J. Epidemiol. Community Health 2006, 60, 221–227. [Google Scholar] [CrossRef] [Green Version]
- Cox, J.; Holden, J.M.; Sagovsky, R. Detection of postnatal depression. Development of the 10-item Edinburgh Postnatal Depression Scale. Br. J. Psychiatry 1987, 150, 782–786. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- First, M.B.; Spitzer, R.L.; Gibbon, M.; Williams, J.B.W. Entrevista clínica estructurada para los trastornos del eje I del DSM-IV- versión clínica (SCID-CV) [Structured Clinical Interview for DSM-IV Axis I Disorders, Clinician Version (SCID-CV)]. 1997. Versión Clínica Ed. Masson. Barcelona. Available online: https://libreriaolejnik.cl/fichas/90090.pdf (accessed on 17 November 2015).
- Remor, E. Psychometric properties of a European Spanish version of the Perceived Stress Scale (PSS). Span. J. Psychol. 2006, 9, 86–93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef]
- Spielberg, C.D.; Gorsuch, R.L.; Lushene, R.E. Manual of State-Trait Anxiety Inventory; Consulting Psichologists Press: Palo Alto, CA, USA, 1970. [Google Scholar]
- Ahmed, A.; Bowen, A.; Feng, C.X.; Muhajarine, N. Trajectories of maternal depressive and anxiety symptoms from pregnancy to five years postpartum and their prenatal predictors. BMC Pregnancy Childbirth 2019, 19, 26. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.; Kim, K.E.; Kim, M.Y.; Park, C.G.; Han, J.Y.; Choi, E.J. Trajectories of depressive symptoms and anxiety during pregnancy and associations with pregnancy stress. Int. J. Environ. Res. Public Health 2021, 18, 2733. [Google Scholar] [CrossRef] [PubMed]
- Segre, L.S.; O’Hara, M.W.; Arndt, S.; Stuart, S. The prevalence of postpartum depression: The relative significance of three social status indices. Soc. Psychiatry Psychiatr. Epidemiol. 2007, 42, 316–321. [Google Scholar] [CrossRef] [PubMed]
- Marcos-Nájera, R.; Rodríguez-Muñoz, M.F.; Lara, M.A.; Navarrete, L.; Le, H.N. A cross-cultural analysis of the prevalence and risk factors for prenatal depression in Spain and Mexico. Cult. Med. Psychiatry 2020, 1–14. [Google Scholar] [CrossRef]
- Koutra, K.; Vassilaki, M.; Georgiou, V.; Koutis, A.; Bitsios, P.; Chatzi, L.; Kogevinas, M. Antenatal maternal mental health as determinant of postpartum depression in a population based mother-child cohort (Rhea Study) in Crete, Greece. Soc. Psychiatry Psychiatr. Epidemiol. 2014, 49, 711–721. [Google Scholar] [CrossRef] [PubMed]
- Sedgh, G.; Bankole, A.; Oye-Adeniran, B.; Adewole, I.F.; Singh, S.; Hussain, R. Unwanted pregnancy and associated factors among Nigerian women. Int. Fam. Plan Perspect. 2006, 32, 175–184. [Google Scholar] [CrossRef]
- Bouchard, G. Adult couples facing a planned or an unplanned pregnancy. J. Fam. Issues 2005, 26, 619–637. [Google Scholar] [CrossRef]
- Bouchard, G.; Boudreau, J.; Hébert, R. Transition to parenthood and conjugal life: Comparisons between planned and unplanned pregnancies. J. Fam. Issues 2006, 27, 1512–1531. [Google Scholar] [CrossRef]
- Vesga-López, O.; Blanco, C.; Keyes, K.; Olfson, M.; Grant, B.F.; Hasin, D.S. Psychiatric disorders in pregnant and postpartum women in the United States. Arch. Gen. Psychiatry 2008, 65, 805. [Google Scholar] [CrossRef] [Green Version]
- Falah-Hassani, K.; Shiri, R.; Dennis, C.L. Prevalence and risk factors for comorbid postpartum depressive symptomatology and anxiety. J. Affect. Disord. 2016, 198, 142–147. [Google Scholar] [CrossRef]
- Ross, L.E.; Gilbert Evans, S.E.; Sellers, E.M.; Romach, M.K. Measurement issues in postpartum depression part 1: Anxiety as a feature of postpartum depression. Arch. Womens Ment. Health 2003, 6, 51–57. [Google Scholar] [CrossRef]
- Van den Bergh, B.R.H.; Mulder, E.J.H.; Mennes, M.; Glover, V. Antenatal maternal anxiety and stress and the neurobehavioural development of the fetus and child: Links and possible mechanisms. A review. Neurosci. Biobehav. Rev. 2005, 29, 237–258. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Probable Depression | Major Depression | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| First Trimester | No (n = 436) | Yes (n = 133) | No (n = 540) | Yes (n = 29) | ||||||||
| n | % | n | % | χ2 | V | n | % | n | % | χ2 | V | |
| Age | 8.825 ** | 0.13 | 0.180 | |||||||||
| ≤30 | 121 | 27.8 | 55 | 41.4 | 166 | 30.7 | 10 | 34.5 | ||||
| >30 | 315 | 72.2 | 78 | 58.6 | 374 | 69.3 | 19 | 65.5 | ||||
| Marital Status | 1.001 | 4.778 | ||||||||||
| Unmarried | 20 | 4.6 | 9 | 6.8 | 25 | 4.6 | 4 | 13.8 | ||||
| Married/Cohabiting | 416 | 95.4 | 124 | 93.2 | 515 | 95.4 | 25 | 86.2 | ||||
| Level of Education | 13.809 *** | 0.16 | 4.348 * | 0.09 | ||||||||
| Primary/Secondary | 215 | 49.3 | 90 | 67.7 | 284 | 52.6 | 21 | 72.4 | ||||
| University | 221 | 50.7 | 43 | 32.3 | 256 | 47.4 | 8 | 27.6 | ||||
| Employment Status | 6.419 * | 0.11 | 2.835 | |||||||||
| Working | 339 | 77.8 | 89 | 66.9 | 410 | 75.9 | 18 | 62.1 | ||||
| Not Working | 97 | 22.2 | 44 | 33.1 | 130 | 24.1 | 11 | 37.9 | ||||
| Pregnancy Influenced Employment | 14.979 *** | 0.16 | 8.892 ** | 0.13 | ||||||||
| No | 365 | 83.7 | 91 | 68.4 | 439 | 81.3 | 17 | 58.6 | ||||
| Yes | 71 | 16.3 | 42 | 31.6 | 101 | 18.7 | 12 | 41.4 | ||||
| Monthly Income (Euros) | 9.783 ** | 0.14 | 0.413 | |||||||||
| ≤1000 | 183 | 48.2 | 71 | 65.1 | 240 | 51.6 | 14 | 58.3 | ||||
| >1000 | 197 | 51.8 | 38 | 34.9 | 225 | 48.4 | 10 | 41.7 | ||||
| Second Trimester | No (n = 472) | Yes (n = 97) | No (n = 546) | Yes (n = 23) | ||||||||
| Age | 8.372 ** | 0.12 | 20.727 *** | 0.19 | ||||||||
| ≤30 | 134 | 28.4 | 42 | 43.3 | 159 | 29.1 | 17 | 73.9 | ||||
| >30 | 338 | 71.6 | 55 | 56.7 | 387 | 70.9 | 6 | 26.1 | ||||
| Marital Status | 0.287 | 0.642 | ||||||||||
| Unmarried | 23 | 4.9 | 6 | 6.2 | 27 | 4.9 | 2 | 8.7 | ||||
| Married/Cohabiting | 449 | 95.1 | 91 | 93.8 | 519 | 95.1 | 21 | 91.3 | ||||
| Level of Education | 16.200 *** | 0.17 | 8.108 ** | 0.12 | ||||||||
| Primary/Secondary | 235 | 49.8 | 70 | 72.2 | 286 | 52.4 | 19 | 82.6 | ||||
| University | 237 | 50.2 | 27 | 27.8 | 260 | 47.6 | 4 | 17.4 | ||||
| Employment Status | 1.642 | 12.956 *** | 0.15 | |||||||||
| Working | 360 | 76.3 | 68 | 70.1 | 418 | 76.6 | 10 | 43.5 | ||||
| Not Working | 112 | 23.7 | 29 | 29.9 | 128 | 23.4 | 13 | 56.5 | ||||
| Pregnancy Influenced Employment | 24.166 *** | 0.21 | 11.231 ** | 0.14 | ||||||||
| No | 367 | 77.8 | 52 | 53.6 | 409 | 74.9 | 10 | 43.5 | ||||
| Yes | 105 | 22.2 | 45 | 46.4 | 137 | 25.1 | 13 | 56.5 | ||||
| Monthly Income (euros) | 7.442 ** | 0.12 | 1.872 | |||||||||
| ≤1000 | 199 | 49.1 | 55 | 65.5 | 243 | 51.4 | 11 | 68.8 | ||||
| >1000 | 206 | 50.9 | 29 | 34.5 | 230 | 48.6 | 5 | 31.3 | ||||
| Third trimester | No (n = 447) | Yes (n = 122) | No (n = 542) | Yes (n = 27) | ||||||||
| Age | 3.335 | 20.637 *** | 0.19 | |||||||||
| ≤30 | 130 | 29.1 | 46 | 37.7 | 157 | 29.0 | 19 | 70.4 | ||||
| >30 | 317 | 70.9 | 76 | 62.3 | 385 | 71.0 | 8 | 29.6 | ||||
| Marital Status | 0.132 | 0.313 | ||||||||||
| Unmarried | 22 | 4.9 | 7 | 5.7 | 27 | 5.0 | 2 | 7.4 | ||||
| Married/Cohabiting | 425 | 95.1 | 115 | 94.3 | 515 | 95.0 | 25 | 92.6 | ||||
| Level of Education | 8.948 ** | 0.13 | 6.661 * | 0.11 | ||||||||
| Primary/Secondary | 225 | 50.3 | 80 | 65.6 | 284 | 52.4 | 21 | 77.8 | ||||
| University | 222 | 49.7 | 42 | 34.4 | 258 | 47.6 | 6 | 22.2 | ||||
| Employment Status | 3.378 | 11.145 ** | 0.14 | |||||||||
| Working | 344 | 77.0 | 84 | 68.9 | 415 | 76.6 | 13 | 48.1 | ||||
| Not Working | 103 | 23.0 | 38 | 31.1 | 127 | 23.4 | 14 | 51.9 | ||||
| Pregnancy Influenced Employment | 4.066 * | 0.09 | 0.626 | |||||||||
| No | 290 | 64.9 | 67 | 54.9 | 342 | 63.1 | 15 | 55.6 | ||||
| Yes | 157 | 35.1 | 55 | 45.1 | 200 | 36.9 | 12 | 44.4 | ||||
| Monthly Income (euros) | 1.798 | 0.996 | ||||||||||
| ≤1000 | 195 | 50.4 | 59 | 57.8 | 242 | 51.5 | 12 | 63.2 | ||||
| >1000 | 192 | 49.6 | 43 | 42.2 | 228 | 48.5 | 7 | 36.8 | ||||
| Probable Depression | Major Depression | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| First Trimester | No (n = 436) | Yes (n = 133) | No (n = 540) | Yes (n = 29) | ||||||||
| n | % | n | % | χ2 | V | n | % | n | % | χ2 | V | |
| Parity | 4.928 * | 0.09 | 10.197 ** | 0.13 | ||||||||
| Primiparous | 270 | 61.9 | 68 | 51.1 | 329 | 60.9 | 9 | 31.0 | ||||
| Multiparous | 166 | 38.1 | 65 | 48.9 | 211 | 39.1 | 20 | 69.0 | ||||
| Previous Abortions | 11.280 ** | 0.14 | 0.024 | |||||||||
| No | 336 | 77.1 | 83 | 62.4 | 398 | 73.7 | 21 | 72.4 | ||||
| Yes | 100 | 22.9 | 50 | 37.6 | 142 | 26.3 | 8 | 27.6 | ||||
| Pregnancy Planning | 2.282 | 2.569 | ||||||||||
| No | 56 | 12.8 | 24 | 18.0 | 73 | 13.5 | 7 | 24.1 | ||||
| Yes | 380 | 87.2 | 109 | 82.0 | 467 | 83.5 | 22 | 75.9 | ||||
| Pregnancy Reaction | 24.026 *** | 0.21 | 13.684 *** | 0.16 | ||||||||
| Positive | 418 | 95.9 | 111 | 83.5 | 507 | 93.9 | 22 | 75.9 | ||||
| Negative | 18 | 4.1 | 22 | 16.5 | 33 | 6.1 | 7 | 24.1 | ||||
| Pregnancy Complication | 3.637 | 0.058 | ||||||||||
| No | 406 | 93.1 | 117 | 88.0 | 496 | 91.9 | 27 | 93.1 | ||||
| Yes | 30 | 6.9 | 16 | 12.0 | 44 | 8.1 | 2 | 6.9 | ||||
| Second Trimester | No (n = 472) | Yes (n = 97) | No (n = 546) | Yes (n = 23) | ||||||||
| Parity | 6.959 ** | 0.11 | 1.332 | |||||||||
| Primiparous | 292 | 61.9 | 46 | 47.4 | 327 | 59.9 | 11 | 47.8 | ||||
| Multiparous | 180 | 38.1 | 51 | 52.6 | 219 | 40.1 | 12 | 52.2 | ||||
| Previous Abortions | 0.012 | 0.001 | ||||||||||
| No | 348 | 73.7 | 71 | 73.2 | 402 | 73.6 | 17 | 73.9 | ||||
| Yes | 124 | 26.3 | 26 | 26.8 | 144 | 26.4 | 6 | 26.1 | ||||
| Pregnancy Planning | 5.575 * | 0.10 | 8.519 ** | 0.12 | ||||||||
| No | 59 | 12.5 | 21 | 21.6 | 72 | 13.2 | 8 | 34.8 | ||||
| Yes | 413 | 87.5 | 76 | 78.4 | 474 | 86.8 | 15 | 65.2 | ||||
| Pregnancy Reaction | 7.265 ** | 0.11 | 7.935 ** | 0.12 | ||||||||
| Positive | 445 | 94.3 | 84 | 86.6 | 511 | 93.6 | 18 | 78.3 | ||||
| Negative | 27 | 5.7 | 13 | 13.4 | 35 | 6.4 | 5 | 21.7 | ||||
| Pregnancy Complication | 2.407 | 3.480 | ||||||||||
| No | 400 | 84.7 | 76 | 78.4 | 460 | 84.2 | 16 | 69.6 | ||||
| Yes | 72 | 15.3 | 21 | 21.6 | 86 | 15.8 | 7 | 30.4 | ||||
| Third Trimester | No (n = 447) | Yes (n = 122) | No (n = 542) | Yes (n = 27) | ||||||||
| Parity | 1.295 | 0.001 | ||||||||||
| Primiparous | 271 | 60.6 | 67 | 54.9 | 322 | 59.4 | 16 | 59.3 | ||||
| Multiparous | 176 | 39.4 | 55 | 45.1 | 220 | 40.6 | 11 | 40.7 | ||||
| Previous Abortions | 0.251 | 0.003 | ||||||||||
| No | 327 | 73.2 | 92 | 75.4 | 399 | 73.6 | 20 | 74.1 | ||||
| Yes | 120 | 26.8 | 30 | 24.6 | 146 | 26.4 | 7 | 25.9 | ||||
| Pregnancy Planning | 4.048 * | 0.08 | 5.687 * | 0.10 | ||||||||
| No | 56 | 12.5 | 24 | 19.7 | 72 | 13.3 | 8 | 29.6 | ||||
| Yes | 391 | 87.5 | 98 | 80.3 | 470 | 86.7 | 19 | 70.4 | ||||
| Pregnancy Reaction | 11.328 ** | 0.14 | 10.010 ** | 0.13 | ||||||||
| Positive | 424 | 94.9 | 105 | 86.1 | 508 | 93.7 | 21 | 77.8 | ||||
| Negative | 23 | 5.1 | 17 | 13.9 | 34 | 6.3 | 6 | 22.2 | ||||
| Pregnancy Complication | 4.380 * | 0.09 | 10.698 ** | 0.14 | ||||||||
| No | 355 | 79.4 | 86 | 70.5 | 427 | 78.8 | 14 | 51.9 | ||||
| Yes | 92 | 20.6 | 36 | 29.5 | 115 | 21.2 | 13 | 48.1 | ||||
| Attendance at Maternal Classes | 10.357 ** | 0.14 | 6.190 * | 0.10 | ||||||||
| No | 149 | 33.3 | 60 | 49.2 | 193 | 35.6 | 16 | 59.3 | ||||
| Yes | 298 | 66.7 | 62 | 50.8 | 349 | 64.4 | 11 | 40.7 | ||||
| Probable Depression | Major Depression | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| First Trimester | No (n = 436) | Yes (n = 133) | No (n = 540) | Yes (n = 29) | ||||||||
| n | % | n | % | χ2 | V | n | % | n | % | χ2 | V | |
| History of Depression | 9.610 ** | 0.13 | 18.247 *** | 0.19 | ||||||||
| No | 412 | 94.5 | 115 | 86.5 | 506 | 93.7 | 21 | 72.4 | ||||
| Yes | 24 | 5.5 | 18 | 13.5 | 34 | 6.3 | 8 | 27.6 | ||||
| Worsening Mood in Previous Pregnancies (n = 234) | 4.908 * | 0.15 | 6.049 * | 0.16 | ||||||||
| No | 147 | 87.5 | 50 | 75.8 | 184 | 86.0 | 13 | 65.0 | ||||
| Yes | 21 | 12.5 | 16 | 24.4 | 30 | 14.0 | 7 | 35.0 | ||||
| Trait Anxiety | 50.455 *** | 0.30 | 10.463 *** | 0.14 | ||||||||
| No | 428 | 98.2 | 109 | 82.0 | 491 | 90.9 | 21 | 72.4 | ||||
| Yes | 8 | 1.8 | 24 | 18.0 | 49 | 9.1 | 8 | 27.6 | ||||
| State Anxiety | 77.467 *** | 0.37 | 7.770 ** | 0.12 | ||||||||
| No | 419 | 96.1 | 93 | 69.9 | 513 | 95.0 | 24 | 82.8 | ||||
| Yes | 17 | 3.9 | 40 | 30.1 | 27 | 5.0 | 5 | 17.2 | ||||
| Second Trimester | No (n = 472) | Yes (n = 97) | No (n = 546) | Yes (n = 23) | ||||||||
| History of Depression | 14.206 *** | 0.16 | 12.267 *** | 0.15 | ||||||||
| No | 446 | 94.5 | 81 | 83.5 | 510 | 93.4 | 17 | 73.9 | ||||
| Yes | 26 | 5.5 | 16 | 16.5 | 36 | 6.6 | 6 | 26.1 | ||||
| Worsening Mood in Previous Pregnancies (n = 234) | 15.040 *** | 0.25 | 11.106 ** | 0.22 | ||||||||
| No | 163 | 89.1 | 34 | 66.7 | 191 | 86.0 | 6 | 50.0 | ||||
| Yes | 20 | 10.9 | 17 | 33.3 | 31 | 14.0 | 6 | 50.0 | ||||
| Trait Anxiety | 42.958 *** | 0.28 | 38.396 *** | 0.26 | ||||||||
| No | 459 | 97.2 | 78 | 80.4 | 522 | 95.6 | 15 | 65.2 | ||||
| Yes | 13 | 2.8 | 19 | 19.6 | 24 | 4.4 | 8 | 34.8 | ||||
| State Anxiety | 70.950 *** | 0.35 | 30.385 *** | 0.23 | ||||||||
| No | 464 | 98.3 | 75 | 77.3 | 523 | 95.8 | 16 | 69.6 | ||||
| Yes | 8 | 1.7 | 22 | 22.7 | 23 | 4.2 | 7 | 30.4 | ||||
| Third Trimester | No (n = 447) | Yes (n = 122) | No (n = 542) | Yes (n = 27) | ||||||||
| History of Depression | 12.348 *** | 0.15 | 14.259 *** | 0.16 | ||||||||
| No | 423 | 94.6 | 104 | 85.2 | 507 | 93.5 | 20 | 74.1 | ||||
| Yes | 24 | 5.4 | 18 | 14.8 | 35 | 6.5 | 7 | 25.9 | ||||
| Worsening Mood in Previous Pregnancies (n = 234) | 5.246 * | 0.16 | 7.619 * | 0.18 | ||||||||
| No | 155 | 87.6 | 42 | 73.7 | 191 | 85.7 | 6 | 54.5 | ||||
| Yes | 22 | 12.4 | 15 | 26.3 | 32 | 14.3 | 5 | 45.5 | ||||
| Trait Anxiety | 39.298 *** | 0.26 | 41.005 *** | 0.27 | ||||||||
| No | 436 | 97.5 | 101 | 82.8 | 519 | 95.8 | 18 | 66.7 | ||||
| Yes | 11 | 2.5 | 21 | 17.2 | 23 | 4.2 | 9 | 33.3 | ||||
| State Anxiety | 84.056 *** | 0.38 | 28.939 *** | 0.23 | ||||||||
| No | 438 | 98.0 | 90 | 73.8 | 510 | 94.1 | 18 | 66.7 | ||||
| Yes | 9 | 2.0 | 32 | 26.2 | 32 | 5.9 | 9 | 33.3 | ||||
| Predictors in the First Trimester | B | WALD | p | OR [95% IC] |
| Age ≤ 30 years | 0.94 | 4,04 | 0.045 | 2.55 [1.02–6.37] |
| Previous Miscarriages | 1.19 | 7.13 | 0.008 | 3.28 [1.37–7.85] |
| High State Anxiety | 1.38 | 4.70 | 0.03 | 3.97 [1.14–13,81] |
| High Perceived Stress | 0.22 | 24.70 | <0.001 | 1.24 [1.14–1.35] |
| Constant | −6.49 | 38.88 | <0.001 | 0.002 |
| Cox and Snell R2 | 0.343 | |||
| Nagelkerke’s R2 | 0.501 | |||
| Predictors in the Second Trimester | ||||
| Probable Depression in the 1st Trimester | 2.61 | 21.41 | <0.001 | 13.61 [4.51–41.14] |
| Higher Perceived Stress in 1st Trimester | 0.12 | 6.53 | 0.011 | 1.14 [1.03–1.24] |
| Higher Perceived Stress in 2nd Trimester | 0.30 | 26.46 | <0.001 | 1.35 [1.21–1.52] |
| Constant | −5.90 | 29.98 | <0.001 | 0.003 |
| Cox and Snell R2 | 0.402 | |||
| Nagelkerke’s R2 | 0.611 | |||
| Predictors in the Third Trimester | ||||
| Major Depression in the 1st Trimester | 1.69 | 6.49 | 0.011 | 5.43 [1.48–19.95] |
| Probable Depression in the 2nd Trimester | 1.82 | 16.47 | <0.001 | 6.19 [2.47–14.91] |
| High State Anxiety in 3rd Trimester | 1.59 | 4.49 | 0.034 | 4.88 [1.13–21.13] |
| Higher Perceived Stress in 3rd Trimester | 0.15 | 15.57 | <0.001 | 1.16 [1.08–1.25] |
| Constant | −5.22 | 36.82 | <0.001 | 0.005 |
| Cox and Snell R2 | 0.368 | |||
| Nagelkerke’s R2 | 0.555 | |||
| Predictors in the First Trimester | B | WALD | p | OR [95% IC] |
| Negative influence of Pregnancy on Work Situation | 1.16 | 5.31 | 0.021 | 3.20 [1.19–8.63] |
| High Perceived Stress | 0.12 | 12.21 | <0.001 | 1.13 [1.05–1.21] |
| Constant | −5.45 | 37.28 | <0.001 | 0.004 |
| Cox and Snell R2 | 0.094 | |||
| Nagelkerke’s R2 | 0.210 | |||
| Predictors in the Second Trimester | ||||
| Age ≤ 30 years | 1.71 | 5.33 | <0.001 | 1.26 [1.13–23.42] |
| High Perceived Stress in the 2nd Trimester | 0.24 | 15.66 | <0.001 | 1.27 [1.13–1.42] |
| Constant | −9.13 | 27.10 | <0.001 | 0.000 |
| Cox and Snell R2 | 0.127 | |||
| Nagelkerke’s R2 | 0.398 | |||
| Predictors in the Third Trimester | ||||
| Age ≤ 30 years | 1.98 | 4.98 | 0.026 | 7.23 [1.27–41.08] |
| High Perceived Stress in the 2nd Trimester | 0.15 | 4.22 | 0.04 | 1.16 [1.01–1.34] |
| High Perceived Stress in 3rd Trimester | 0.16 | 4.20 | 0.04 | 1.18 [1.01–1.37] |
| Constant | −11.51 | 20.60 | <0.001 | 0.000 |
| Cox and Snell R2 | 0.147 | |||
| Nagelkerke’s R2 | 0.485 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Míguez, M.C.; Vázquez, M.B. Prevalence of Depression during Pregnancy in Spanish Women: Trajectory and Risk Factors in Each Trimester. Int. J. Environ. Res. Public Health 2021, 18, 6789. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18136789
Míguez MC, Vázquez MB. Prevalence of Depression during Pregnancy in Spanish Women: Trajectory and Risk Factors in Each Trimester. International Journal of Environmental Research and Public Health. 2021; 18(13):6789. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18136789
Chicago/Turabian StyleMíguez, M. Carmen, and M. Belén Vázquez. 2021. "Prevalence of Depression during Pregnancy in Spanish Women: Trajectory and Risk Factors in Each Trimester" International Journal of Environmental Research and Public Health 18, no. 13: 6789. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18136789