
An Investigation of Knee Injury Profiles among Iranian Elite Karatekas: Observations from a Cross-Sectional Study

 ,
,  ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Ethical Issue
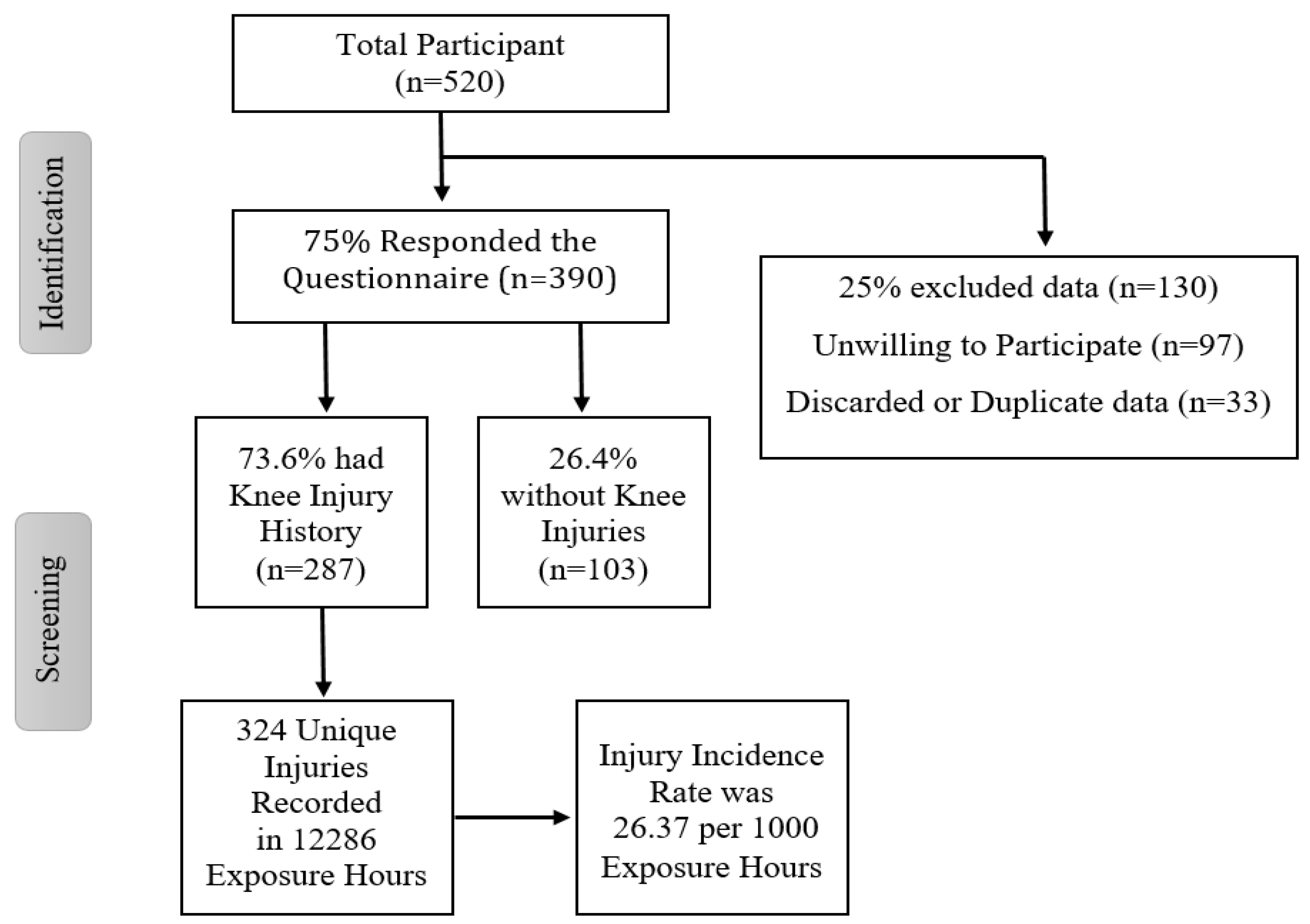
2.2. Participants and Setting
2.3. Questionnaire Development
- (A)
- Questionnaire on Demographic and Sports information: including demographic features, such as height, weight, age, exercise history, the number of training sessions per week, training days and hours, duration of the training, and warm-up methodologies. Questionnaire (A) is enclosed in the paper as Supplementary Materials (NO = 1).
- (B)
- Questionnaire on Knee Injury Profile: the history of injury; injured leg (dominant or non-dominant); injury mechanisms; injury time, treatment, and type of aftercare. Injury incidence was determined as Σ injuries/Σ exposure hours × 1000. Questionnaire (B) is enclosed in the paper as Supplementary Materials (NO = 2).
- (C)
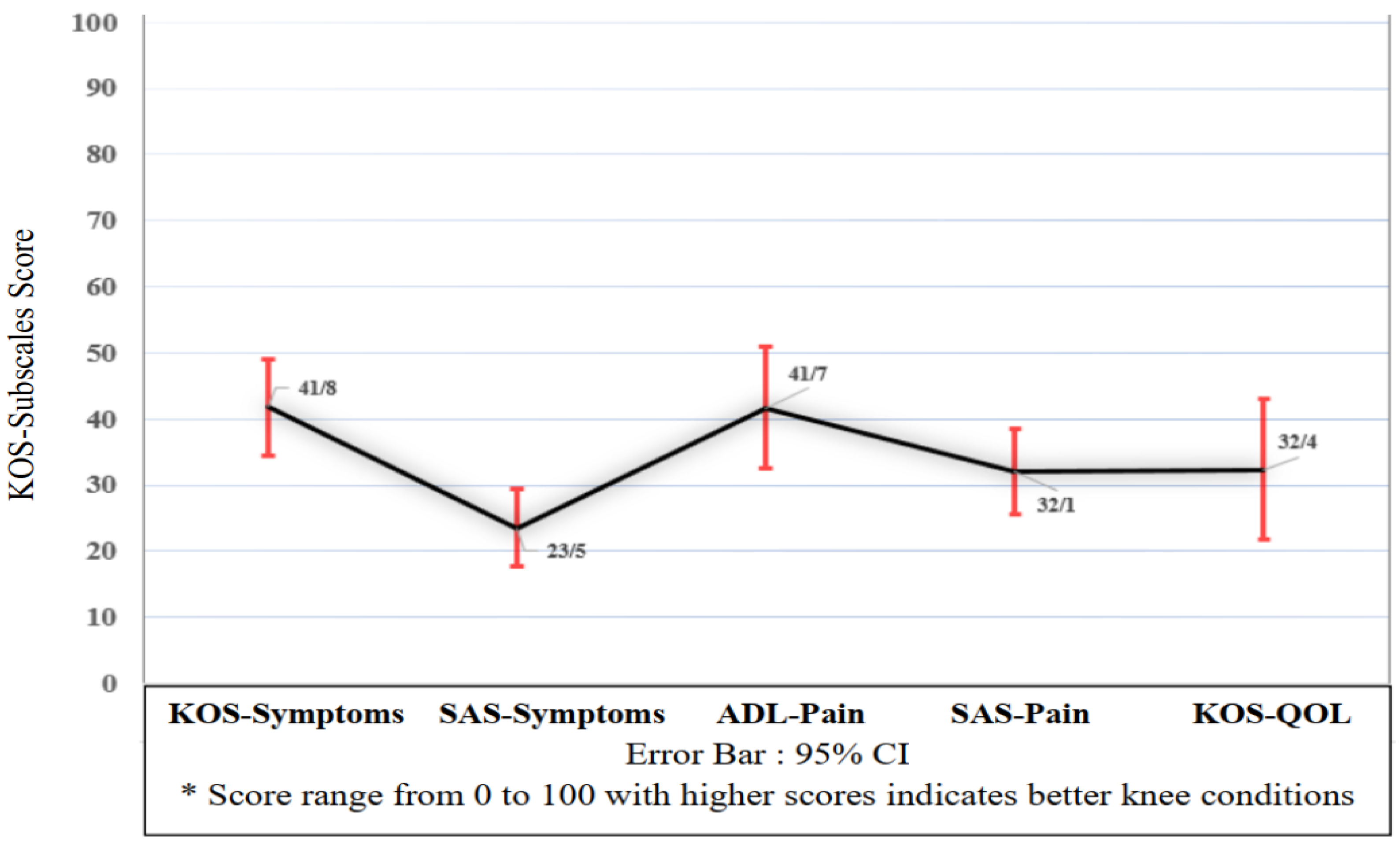
- Knee Outcome Survey (KOS): The KOS is a self-reported questionnaire used to determine the amount of knee joint disability during daily activity and exercise [22,23]. It has been translated into the Persian language [24]. KOS is widely used for the evaluation of various knee injuries, including meniscus damage, ligament, cartilage lesion, patellofemoral pain syndrome, knee dislocation, or osteoarthritis [25,26] in both athletic and elderly populations [27,28].
2.4. Data Collection Procedure
2.5. Data Analyses
3. Results
3.1. Participants’ Characteristics and Sport Backgrounds
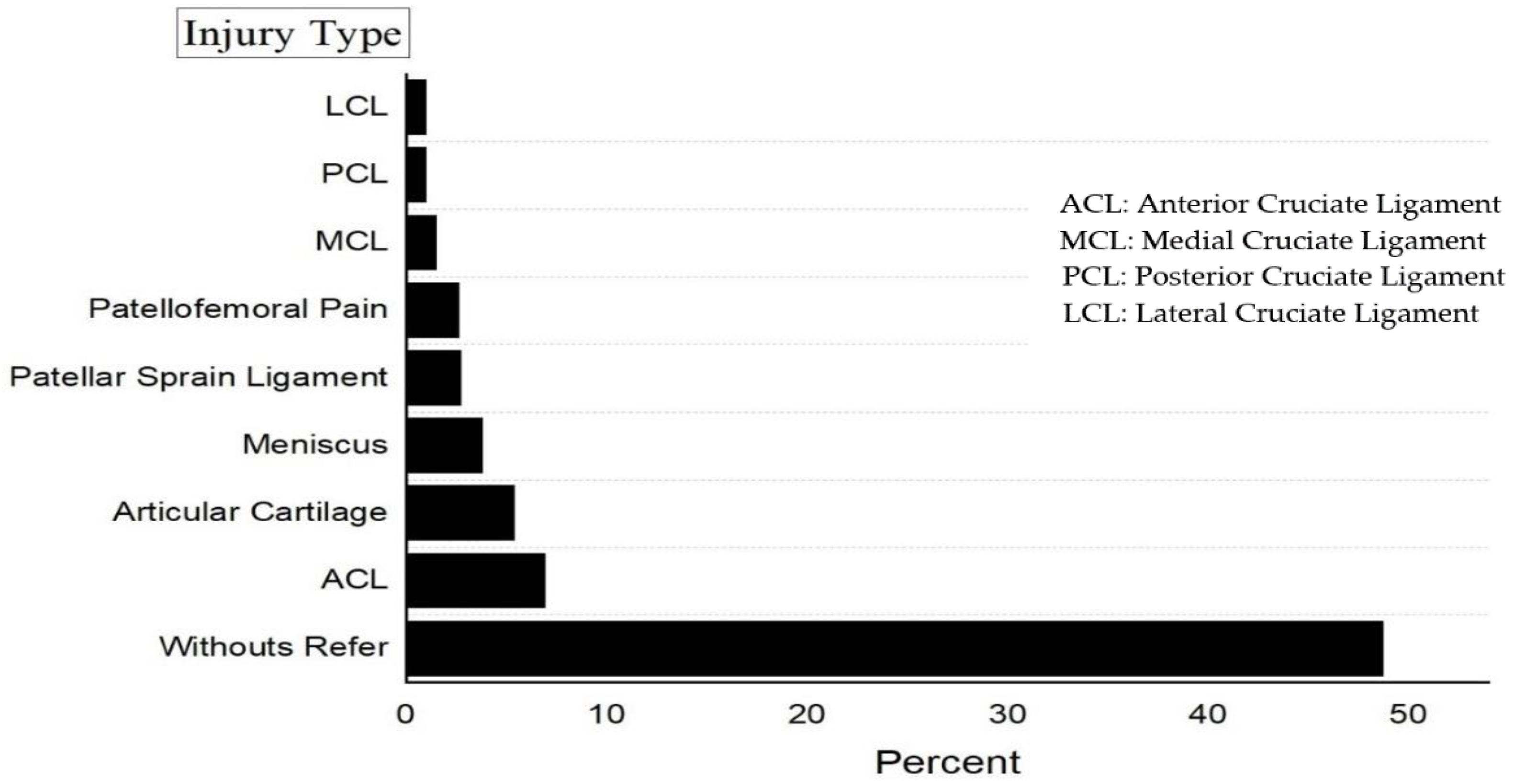
3.2. Participants’ Knee Injury Profiles
3.3. Participants’ KOS Subscales and Self-Reported Score
4. Discussion
Strength and Limitation
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kazemi, M.; Shearer, H.; Choung, Y.S. Pre-competition habits and injuries in Taekwondo athletes. BMC Musculoskelet. Disord. 2005, 6, 26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Viswanath, Y.K.S.; Rogers, I.M. A non-contact complete knee dislocation with popliteal artery disruption, a rare martial arts injury. Postgrad. Med. J. 1999, 75, 552–554. [Google Scholar] [CrossRef] [PubMed]
- Pieter, W. Martial arts injuries. Med. Sport Sci. 2005, 48, 59–73. [Google Scholar] [PubMed] [Green Version]
- Caine, D.; Maffulli, N. Epidemiology of Children’s Individual Sports Injuries: An Important Area of Medicine and Sport Science Research; Karger Medical and Scientific Publishers: Basel, Switzerland, 2005. [Google Scholar]
- Critchley, G.R.; Mannion, S.; Meredith, C. Injury rates in Shotokan karate. Br. J. Sports Med. 1999, 33, 174–177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kazemi, M.; Waalen, J.; Morgan, C.; White, A.R. A profile of Olympic Taekwondo competitors. J. Sport. Sci. Med. 2006, 5, 114–121. [Google Scholar]
- Lystad, R.P.; Augustovičová, D.; Harris, G.; Beskin, K.; Arriaza, R. Epidemiology of injuries in Olympic-style karate competitions: Systematic review and meta-analysis. Br. J. Sports Med. 2020, 54, 976–983. [Google Scholar] [CrossRef]
- Čierna, D.; Lystad, R.P. Epidemiology of competition injuries in youth karate athletes: A prospective cohort study. Br. J. Sports Med. 2017, 51, 1285–1288. [Google Scholar] [CrossRef]
- Beneke, R.; Beyer, T.; Jachner, C.; Erasmus, J.; Hütler, M. Energetics of karate kumite. Eur. J. Appl. Physiol. 2004, 92, 518–523. [Google Scholar] [CrossRef] [PubMed]
- Yalfani, A.; Raeisi, Z. Effects of Lace up Brace on the Ankle Muscles Activity in Different Foot Position during Drop Landing with and without Fatigue. New Approaches Sport Sci. 2019, 1, 9–24. [Google Scholar]
- Burke, D.R. Treating Martial Arts Injuries; Ohara Publications: Burbank, CA, USA, 1981. [Google Scholar]
- Mistry, H.; Connock, M.; Pink, J.; Shyangdan, D.; Clar, C.; Royle, P.; Court, R.; Biant, L.C.; Metcalfe, A.; Waugh, N. Autologous chondrocyte implantation in the knee: Systematic review and economic evaluation. Health Technol. Assess. 2017, 21, 1–294. [Google Scholar] [CrossRef]
- Sahebozamani, M.; Beyranvand, R. A review of injury assessment in Iranian martial artists: Systematic review. Sci. J. Rehabil. Med. 2016, 5, 235–248. [Google Scholar] [CrossRef]
- Mahdavi Mohtasham, H.; Shahrbanian, S. An Investigation of Knee Injury Prevalence and its Mechanism among Premier League Soccer Referees in Iran. J. Sport Biomec. 2017, 2, 29–39. [Google Scholar]
- Naserpour, H.; Mirjani, M. An Investigation of Ankle Injury Prevalence and Its Mechanism Among Iranian Professional Karateka. J. Sport Biomec. 2019, 4, 1–10. [Google Scholar]
- Arriaza, R.; Leyes, M. Injury profile in competitive karate: Prospective analysis of three consecutive World Karate Championships. Knee Surgery Sports Traumatol. Arthrosc. 2005, 13, 603–607. [Google Scholar] [CrossRef] [PubMed]
- Livingston, L.A.; Spaulding, S.J. OPTOTRAK measurement of the quadriceps angle using standardized foot positions. J. Athl. Train. 2002, 37, 252–255. [Google Scholar] [PubMed]
- Dadgar, H.; Sahebozamani, M.; Noorai, T.; Sharifian, E. The Relationship between Q—Angle and Non-Contact Injuries of Lower Extremity in Male Karate Players. Sport Med. J. 2011, 1, 83–97. [Google Scholar]
- Destombe, C.; Lejeune, L.; Guillodo, Y.; Roudaut, A.; Jousse, S.; Devauchelle, V.; Saraux, A. Incidence and nature of karate injuries. Jt. Bone Spine 2006, 73, 182–188. [Google Scholar] [CrossRef]
- Rickham, P.P. Human Experimentation Code of Ethics of the World Medical Association. Br. Med. J. 1964, 2, 177. [Google Scholar] [CrossRef] [Green Version]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Lancet 2007, 370, 1453–1457. [Google Scholar] [CrossRef]
- Roos, E.; Roos, H.P.; Lohmander, S.; Ekdahl, C.; Beynnon, B.D. Knee Injury and Osteoarthritis Outcome Score (KOOS)—Development of a self-administered outcome measure. J. Orthop. Sports Phys. Ther. 1998, 28, 88–96. [Google Scholar] [CrossRef]
- Roos, E.M.; Lohmander, L.S. The Knee injury and Osteoarthritis Outcome Score (KOOS): From joint injury to osteoarthritis. Health Qual. Life Outcomes 2003, 1, 64. [Google Scholar] [CrossRef] [Green Version]
- Salavati, M.; Mazaheri, M.; Negahban, H.; Sohani, S.; Ebrahimian, M.; Ebrahimi-Takamjani, I.; Kazemnejad, A. Validation of a Persian-version of Knee injury and Osteoarthritis Outcome Score (KOOS) in Iranians with knee injuries. Osteoarthr. Cartil. 2008, 16, 1178–1182. [Google Scholar] [CrossRef] [Green Version]
- Irrgang, J.J.; Snyder-Mackler, L.; Wainner, R.S.; Fu, F.H.; Harner, C.D. Development of a patient-reported measure of function of the knee. J. Bone Jt. Surgery Ser. A 1998, 80, 1132–1145. [Google Scholar] [CrossRef]
- Piva, S.R.; Gil, A.B.; Moore, C.G.; Fitzgerald, G.K. Responsiveness of the activities of daily living scale of the knee outcome survey and numeric pain rating scale in patients with patellofemoral pain. J. Rehabil. Med. 2009, 41, 129–135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Impellizzeri, F.M.; Mannion, A.F.; Leunig, M.; Bizzini, M.; Naal, F.D. Comparison of the Reliability, Responsiveness, and Construct Validity of 4 Different Questionnaires for Evaluating Outcomes after Total Knee Arthroplasty. J. Arthroplast. 2011, 26, 861–869. [Google Scholar] [CrossRef] [PubMed]
- Mazaheri, M.; Salavati, M.; Negahban, H.; Sohani, S.; Taghizadeh, F.; Feizi, A.; Karimi, A.; Parnianpour, M. Reliability and validity of the Persian version of Foot and Ankle Ability Measure (FAAM) to measure functional limitations in patients with foot and ankle disorders. Osteoarthr. Cartil. 2010, 18, 755–759. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weigold, A.; Weigold, I.K.; Russell, E.J. Examination of the equivalence of self-report survey-based paper-and-pencil and internet data collection methods. Psychol. Methods 2013, 18, 53–70. [Google Scholar] [CrossRef] [PubMed]
- Rossettini, G.; Palese, A.; Geri, T.; Fiorio, M.; Colloca, L.; Testa, M. Physical therapists’ perspectives on using contextual factors in clinical practice: Findings from an Italian national survey. PLoS ONE 2018, 13, e0208159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piejko, L.; Mosler, D.; Grzebisz, N. Sport Injuries in Karate Kyokushin Athletes. Biomed. J. Sci. Tech. Res. 2019, 15, 11134–11142. [Google Scholar] [CrossRef]
- VencesBrito, A.; Rodrigues-Ferreira, M.; Antonio Castro, M.; Polak, E.; Valente, E.J.; Romero, F.; Figueiredo, A. Sport injuries in Portuguese female and male karateka: A retrospective study. Ido Mov. Cult. J. Martial Arts Anthropol. 2019, 19, 51–57. [Google Scholar]
- Rahnama, N.; Bambaeichi, E.; Bagher Nazarian, A.; Batavani, M.; Sadeghipour, H. Injury profile of Iranian professional male and female karate players. J. Exerc. Sci. Med. 2011, 3, 21–37. [Google Scholar]
- Macan, J.; Bundalo-Vrbanac, D.; Romić, G. Effects of the new karate rules on the incidence and distribution of injuries. Br. J. Sports Med. 2006, 40, 326–330. [Google Scholar] [CrossRef]
- Čierna, D.; Barrientos, M.; Agrasar, C.; Arriaza, R. Epidemiology of injuries in juniors participating in top-level karate competition: A prospective cohort study. Br. J. Sports Med. 2017, 52, 730–734. [Google Scholar] [CrossRef] [PubMed]
- Naserpour, H.; Mimar, R.; Khoshjamal Fekri, S. The Effect of Eight-Weeks General Preparation Exercise on Some Selected Biomechanical, Anthropometrical and Physiological Parameters of the Iranian National Females’ Taekwondo Team. J. Sport Biomech. 2017, 3, 7–8. [Google Scholar]
- Sharma, L.; Song, J.; Felson, D.; Cahue, S.; Shamiyeh, E.; Dunlop, D.D. The role of knee alignment in disease progression and functional decline in knee osteoarthritis. JAMA 2001, 286, 188–195. [Google Scholar] [CrossRef] [Green Version]
- Buschbacher, R.M.; Prahlow, N.D.; Dave, S.J. (Eds.) Sports Medicine and Rehabilitation: A Sport-Specific Approach, 2nd ed.; Lippincott Williams & Wilkins: Philadelphia, UK; London, UK, 2009. [Google Scholar]
- Chen, J.; Kim, J.; Shao, W.; Schlecht, S.H.; Baek, S.Y.; Jones, A.K.; Ahn, T.; Ashton-Miller, J.A.; Holl, M.M.B.; Wojtys, E.M. An Anterior Cruciate Ligament Failure Mechanism. Am. J. Sports Med. 2019, 47, 2067–2076. [Google Scholar] [CrossRef] [PubMed]
- Petushek, E.J.; Sugimoto, D.; Stoolmiller, M.; Smith, G.; Myer, G.D. Evidence-Based Best-Practice Guidelines for Preventing Anterior Cruciate Ligament Injuries in Young Female Athletes: A Systematic Review and Meta-analysis. Am. J. Sports Med. 2019, 47, 1744–1753. [Google Scholar] [CrossRef]
- Skinner, H.B.; Barrack, R.L. Joint position sense in the normal and pathologic knee joint. J. Electromyogr. Kinesiol. 1991, 1, 180–190. [Google Scholar] [CrossRef]
- LaBella, C.R.; Huxford, M.R.; Grissom, J.; Kim, K.Y.; Peng, J.; Christoffel, K.K. Effect of neuromuscular warm-up on injuries in female soccer and basketball athletes in urban public high schools: Cluster randomized controlled trial. Arch. Pediatr. Adolesc. Med. 2011, 165, 1033–1040. [Google Scholar] [CrossRef] [Green Version]
- Wu, H.; Hackett, T.; Richmond, J.C. Effects of meniscal and articular surface status on knee stability, function, and symptoms after anterior cruciate ligament reconstruction: A long-term prospective study. Am. J. Sports Med. 2002, 30, 845–850. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Sports Background Variable | Frequency | Sports Background Variable | Frequency |
| Sport Experience | N (%) | Sport Level | N (%) |
| ≤3 years | 5 (1.3%) | National | 98 (25.1%) |
| 3–5 years | 113 (29%) | Club | 292 (74.9%) |
| ≥5 years | 272 (69.7%) | Collegiate | - |
| Sessions Per Week | N (%) | Days per Week | N (%) |
| ≤3 session | 124 (31.8%) | 1–2 days per week | 3 (0.8%) |
| 4–5 sessions | 113 (29%) | 2–3 days per week | 93 (23.8%) |
| 5–6 session | 76 (19.5%) | 3–4 days per week | 161 (41.3%) |
| ≥6 sessions per week | 77 (19.7%) | ≥5 days per week | 133 (34.1%) |
| Warm-up time in each session | N (%) | Sessions in a Day | N (%) |
| ≤15 min | 60 (15.4%) | 1 session | 145 (37.2%) |
| 15–30 min | 300 (76.6%) | 2 sessions | 138 (35.4%) |
| 31–45 min | 28 (7.5%) | 3 sessions | 96 (24.5%) |
| ≥46 min | 2 (0.5%) | ≥3 sessions | 11 (2.7%) |
| Warm-up Method | N (%) | Duration of each session | N (%) |
| Stretching | 28 (7.2%) | ≤1 h | 3 (0.8%) |
| Running | 33 (8.5%) | 1–2 h | 263 (67.4%) |
| Combat exercise | 67 (17.2%) | 2–3 h | 110 (28.2%) |
| Stretching ± running | 65 (16.7%) | ≥3 h | 14 (3.6%) |
| Stretching ± combat exercise | 33 (8.5%) | ||
| Stretching ± Running ± Combat Exercise | 164 (42.1%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Naserpour, H.; Baker, J.S.; Letafatkar, A.; Rossettini, G.; Dutheil, F. An Investigation of Knee Injury Profiles among Iranian Elite Karatekas: Observations from a Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 6888. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18136888
Naserpour H, Baker JS, Letafatkar A, Rossettini G, Dutheil F. An Investigation of Knee Injury Profiles among Iranian Elite Karatekas: Observations from a Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2021; 18(13):6888. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18136888
Chicago/Turabian StyleNaserpour, Hamidreza, Julien S. Baker, Amir Letafatkar, Giacomo Rossettini, and Frédéric Dutheil. 2021. "An Investigation of Knee Injury Profiles among Iranian Elite Karatekas: Observations from a Cross-Sectional Study" International Journal of Environmental Research and Public Health 18, no. 13: 6888. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18136888