1. Introduction
From a global perspective, the health risks of the population aging and rising medical expenditure have an important impact on socioeconomic development, which has aroused widespread concerns. Since the beginning of the 21st century, China’s demographic structure has undergone drastic and profound changes alongside the deepening of economic transformation and social transition. The increasing proportion of the aging population is undoubtedly one of the most critical features of China’s demographic transformation. According to the statistics, China’s population of elderly people over 60 increased from 167 to 264 million from 2009 to 2020, an average annual increase of about 8.8 million. In addition, this number will exceed 400 million by 2050, which will account for more than 30% of the total population [
1]. One of the changes with this aging trend is the health status transition. In the past ten years, the average annual growth rate of the elderly population aged 80 and above in China has been 4.7%, which is significantly faster than those who are 60 and above. Because the physical functions of the elderly are gradually weakened as they grow older, the population of disabled and semi-disabled elderly will grow rapidly. At the end of 2019, statistics showed that among the 254 million elderly population in China, about 120 million elderly people suffered from chronic diseases, and the disabled and semi-disabled elderly population exceeded 40 million [
2]. Due to the risks of the health deterioration of the elderly, their demand for medical services is on the rise, along with medical expenditure. In this paper, the relationship between the health status and medical expenditure of the elderly is discussed from both individual and household perspectives. We also predict the population size of the elderly with different health statuses and their medical expenditure for the period 2020–2060. Feasible policy suggestions are provided in order to meet the challenge of rapid population aging.
The aging of populations brings a heavy burden to social old-age security and causes an increase in health care demands and the rapid expansion of medical expenses [
3,
4]. Scrutinizing the related literature, scholars have conducted empirical analysis on the health status of the elderly and discussed how the factors impact their health status. Scholars have also put forward policy implications related to medical care, pensions, and retirement to alleviate the burden of population aging [
5,
6,
7]. Although the factors impacting health have been analyzed, a systematic theoretical framework is still lacking. The framework is the premise to analyze the relationship between elderly health and medical expenditure. Therefore, by referring to the medical behavior theory model of Anderson, this paper constructs a theoretical analysis framework of medical expenses for the elderly through propensity, enablement, and demand factors, which lay a solid foundation for the scientific prediction of the elderly population’s medical expenses.
According to the existing research, the factors impacting elderly health status can be roughly divided into demographic characteristics, socioeconomic status, lifestyle, and other factors. As to the demographic characteristics, the health condition of older men is significantly better than their counterparts [
8,
9]. In addition, the health status of the elderly generally decreases with age [
10]. Even though the abilities of older people decline, they tend to report their health and life positively [
11]. As to socioeconomic factors, the urban elderly are better off than those living in rural areas in terms of physical health, while this conclusion is reversed as to mental health [
12]. Other social and economic factors, such as higher education and income, have a positive impact on elderly health [
13]; however, Zachary Zimmer (2004) [
14] found that the impact of these factors was not significant. In addition, support from family and community can help improve the health levels of the elderly [
15,
16,
17]. As to lifestyle factors, a good lifestyle, such as taking part in physical exercises and entertainment, can help to improve the health levels of the elderly [
18]. In addition, moderate alcohol drinking has little impact, but excessive alcohol drinking increases the morbidity and mortality of the elderly [
19,
20].
Accurate prediction of the health transition of the elderly is of great significance for analyzing their medical expenses. Through the literature review, it is found that scholars mainly make dynamic predictions for elderly health status from macro and micro perspectives. Due to the fact that the factors are multidimensional, the research methods adopted by scholars on this issue are very different. On the one hand, macro forecasting analysis selects key factors and sets key parameters to analyze the different situations of long-term care needs. Different studies referred to different bases when selecting key factors, and the key parameters were also set differently. For example, Comas Herrera (2007) [
21] predicted the health care needs of the elderly in four European countries and set key parameters including lifestyle, nursing cost, health status, and external support. In contrast, Costa Font (2008) [
22] used key parameters such as birth and death rates to simulate the population number and to calculate the population size of the elderly under different health conditions. On the other hand, micro prediction analysis is to build health status transition models and predict the health status of the elderly based on micro survey data. For example, Rickayzen et al. (2002) [
23] first used the Markov method to predict the long-term care needs of the elderly. Peng Rong (2009) [
24] adjusted the health transition probability of the American elderly population using the simple sequential method and predicted the long-term care needs of the Chinese elderly population. Chahed (2013) [
25] and Hu (2015) [
26] constructed logit regression and multiple regression models and made their predictions using the transition probability obtained from regression model simulation. Due to the complexity of the factors impacting health status, the factors are selected differently in different studies, thus the different results.
Based on the current research on the health and medical expenditure of the elderly, we propose the following summary: first, the health disparity of the elderly is studied as well as the factors impacting elderly health status, such as age, gender, urban or rural areas, and other socioeconomic factors. Second, scholars have suggested that the most important way to improve the health of the elderly is living a healthy lifestyle. Therefore, the popularization of basic medical and health education should be made, and an active and healthy lifestyle should be advocated. Third, scholars have used quantitative methods to analyze the long-term care needs of the elderly and predicted their health care demand and expenditure. Some scholars have predicted the health care needs of the elderly by setting key parameters and simulating the population size. It is generally recognized that the scientific assessment and prediction of the health care needed for the elderly is conducive, which provides the relevant information on the aging population in advance and gives data support for later policy interventions.
Although the current research on elderly health and its prediction has achieved some progress, many shortcomings remain, which are as follows: firstly, scholars have neither established a unified theoretical analysis framework to study the factors that impact elderly health nor incorporated the different health statuses of the elderly in the calculation of medical expenses. However, examining the health status of the elderly and its relation to medical expenditure is a key precondition to make an accurate prediction. Secondly, scholars have studied the health expenditure of the elderly, but an exact classification of health status has rarely been given. In addition, the healthy elderly population has generally not been included in the calculation. Although the per capita medical expenditure of the healthy elderly is lower, the total expenditure is much higher because of the large population, and its growth is fast, in line with the aging population. Thirdly, scholars have adopted the quantitative method in related research. However, the data sources and parameter settings are highly controversial, which may not reflect the actual social situation and may lack practical guiding significance.
This paper makes related improvements to the deficiencies mentioned above. First, we improve the elderly health transition matrix model and establish a theoretical analysis framework for elderly medical expenditure. Second, the health status of the elderly is classified using an authoritative database representing the actual situation of the elderly in China. Based on the scientific model and convincing data, the health transition probability and medical expenditure scale of the elderly in the period 2020–2060 are predicted. Third, according to the changing pattern of the elderly population in China, this paper predicts the changing trend of elderly population size and the medical expenses under different health conditions from 2020 to 2060. This paper also provides feasible policy suggestions on how to respond to the rising medical expenditure and the health care needed.
4. Conclusions and Policy Implications
Under the background of “Healthy China”, advanced age has become a new feature of population aging. With the increasing risk of the elderly’s health status deterioration, providing adequate health care services and effectively controlling the excessive growth of medical expenditure have become a top priority for China in the new era. This paper intends to estimate the size of the elderly population, their health status transition, and the medical expenditure involved. By improving the Markov matrix model and using the TPM, this paper constructs a theoretical analysis framework for the medical expenses of the elderly. This paper evaluates the size of the elderly population with different health states (the healthy, the mildly disabled, the moderate disabled, and the severely disable). It predicts the medical expenses for the period 2020–2060, following the data of CHARLS from 2011 to 2015.
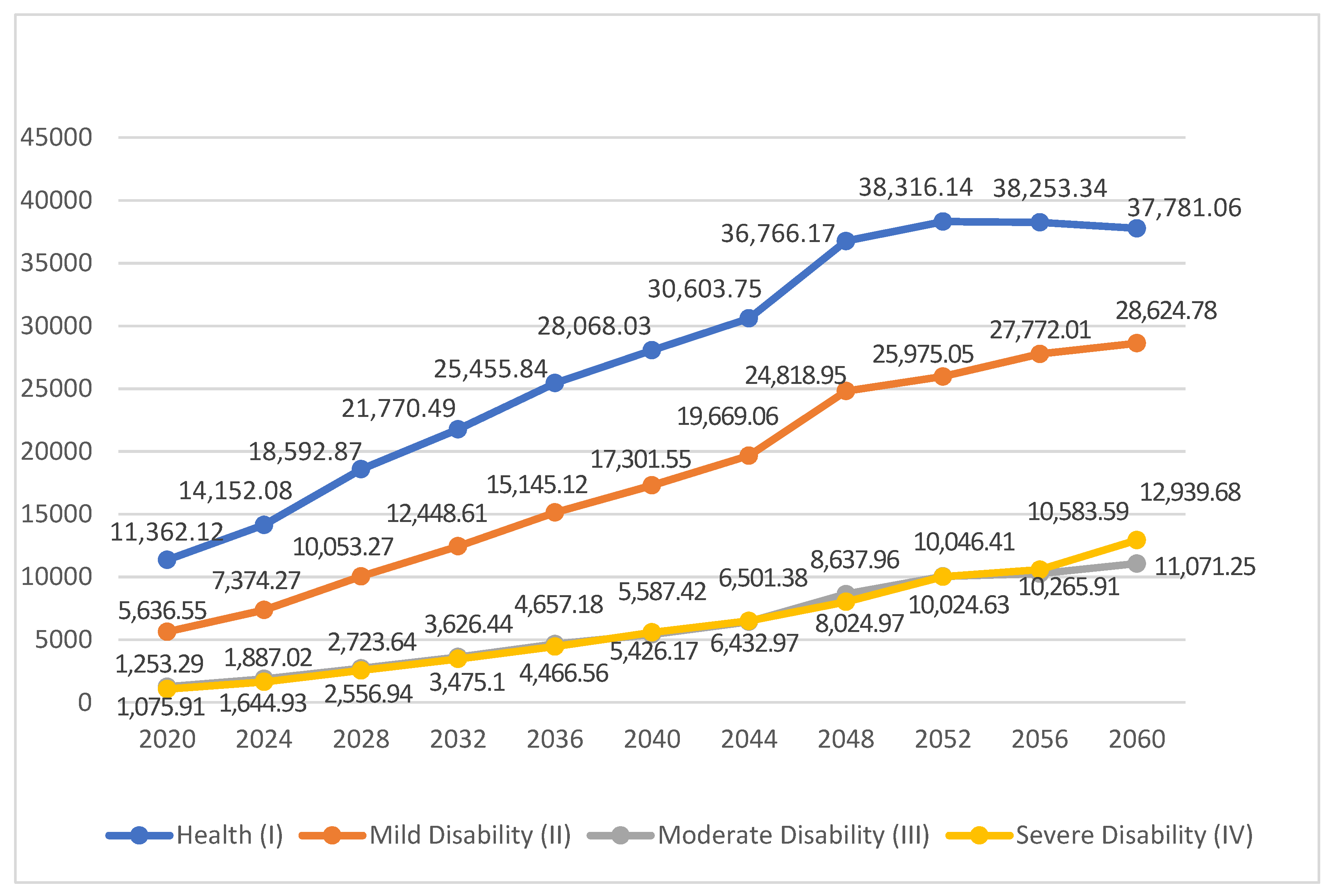
The main findings of this research are as follows: (1) Under the aging trend. Although the elderly have a higher probability of maintaining their basic health status, their physical function decline is still inevitable. Especially for the severely disabled elderly, the rapid growth of population size and medical expenses will bring great pressure to the medical service system. (2) The health status of the elderly has a significant impact on their acceptance of medical diagnoses and treatments as well as medical expenditure. The worse the health status of the elderly, the more willing the families and individuals are to participate in diagnoses and treatments. This leads to higher medical expenditure that is increasingly beyond the affordability of individuals and families. (3) China’s elderly population shows an inverted “U” growth trend, reaching its peak around 2048, at about 434 million people. Among the elderly of different health statuses, the number of mildly disabled elderly will be 121 million. The number of moderately and severely disabled elderly will be 37 and 30 million, respectively. (4) In terms of medical expenditure, the total medical expenditure of the healthy elderly is the largest. This is because it is the largest population. As to the disabled elderly, the severely disabled elderly have the fastest increasing rate of medical expenditure.
To conclude, this study has important implications for making healthy aging policies and controlling the rapid growth of medical expenditure. Firstly, it is recommended to implement precise, classified, and targeted medical services for the elderly in their different health states. To the mildly disabled elderly, disease prevention and rehabilitation should come first because they still have higher probabilities of maintaining their health statuses and recovering healthy states. As to the moderately and severely disabled elderly, whose probabilities of health recovery are relatively small, it is necessary to provide daily care, medical care, spiritual consolations, and hospice care to improve the quality of their later lives. Secondly, there are significant disparities in medical participation and medical expenditure among the elderly living in urban or rural areas and those with different income levels. The medical and health care system should be reformed to improve the affordability of the elderly. The obstacles to the rural and low-income elderly population participating in medical care should be eliminated at the same time. Thirdly, the fast-rising medical expenditure should be shared among individuals, the government, and society. The medical insurance system should be reformed and improved; commercial medical insurance and social and medical treatment systems need to be developed. Fourthly, the elderly population size of China is expected to reach its peak in 2048, when it will face a high burden of pension and medical security. Therefore, strengthening the preventive interventions for the elderly and perfecting the medical service system before 2048 will help alleviate the challenges brought by ever-rising medical expenditure.
Last but not least, in order to scientifically deal with the health deterioration risks and medical expenditure expansion caused by the aging population, it is necessary to strengthen the basic population census and establish a dynamic monitoring mechanism for the disabled elderly. There is still a lack of data on the disabled elderly population. Conducting the census and statistics collections of the different populations can help us understand population distributions and trends, which are the premise for related policies. Therefore, subdivision statistics related to the elderly can be collected during the national census and published in the China population statistics yearbook. Subregional statistics or sampling statistics can also be collected. Furthermore, the elderly are encouraged to report their health status regularly, and a dynamic monitoring system for the disabled elderly should be established. In this way, the health status of the disabled elderly population can be estimated, and professional and targeted health care services can be provided.



 and
and 


{kind=link}