
Effects of Short-Term Golden Root Extract (Rhodiola rosea) Supplementation on Resistance Exercise Performance


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
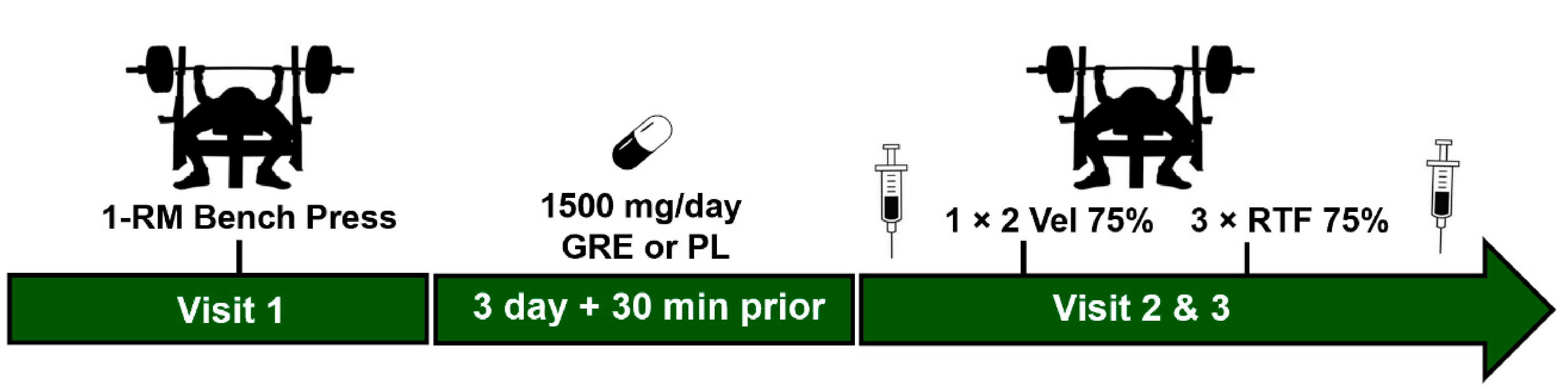
2.2. Study Design
2.3. Supplementation
2.4. Blood Collection and Analysis (Lactate, Epinephrine, Norepinephrine)
2.5. One Repetition Maxium (1-RM) and Familiarization
2.6. Procedures
2.7. Data Analysis
3. Results
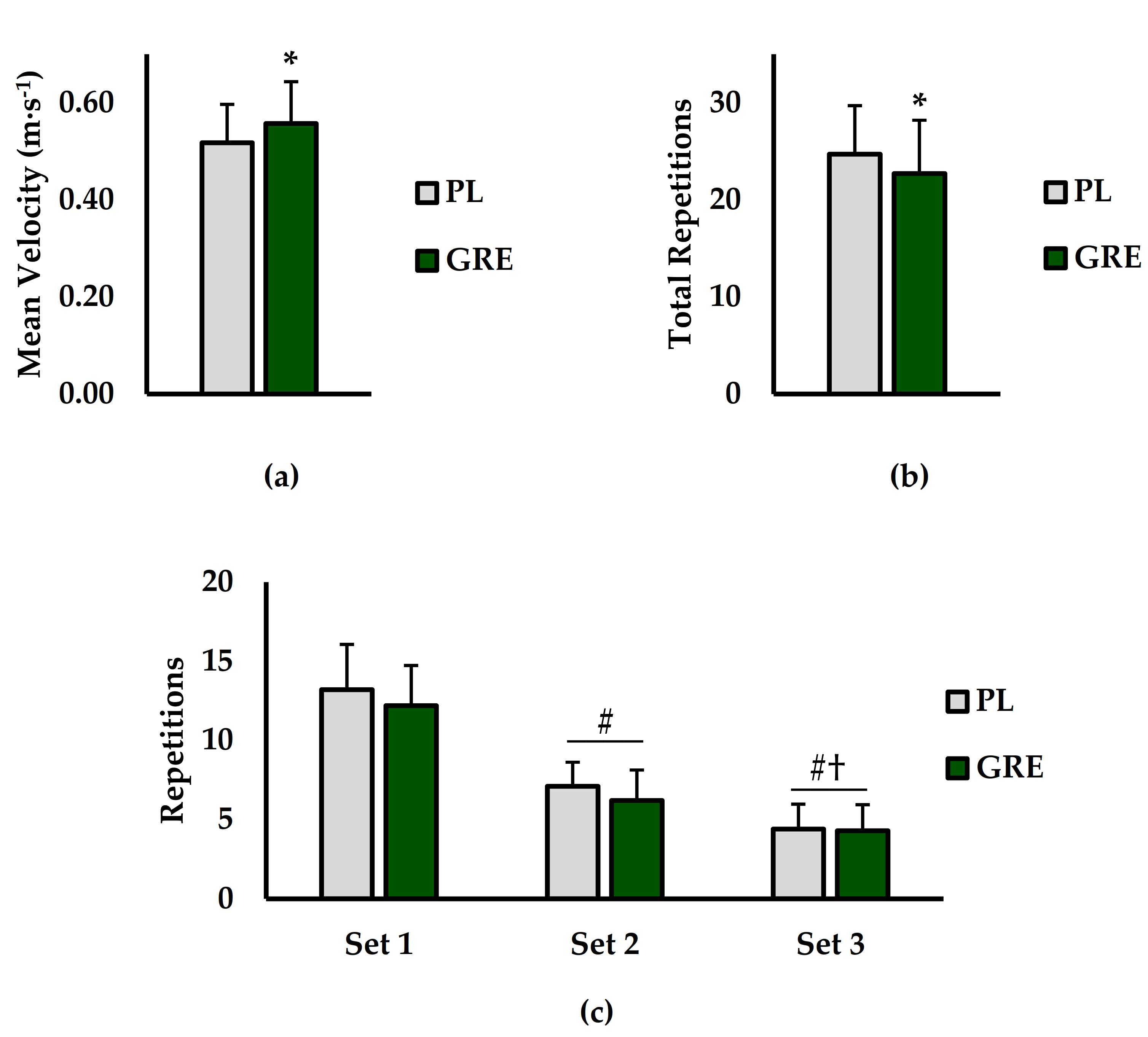
3.1. Mean Velocity and Repetitions to Failure
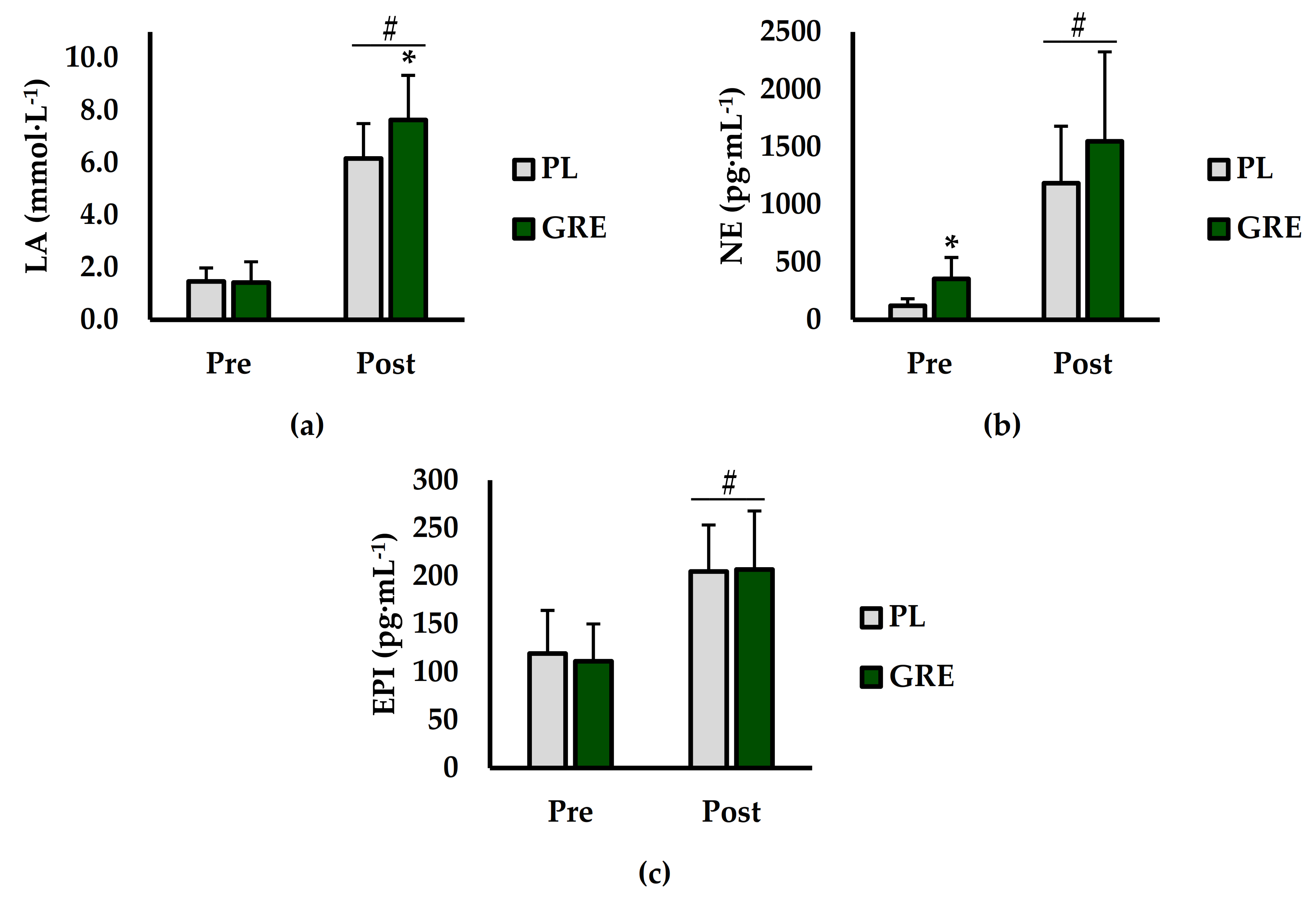
3.2. Blood Lactate, Epinephrine, Norepinephrine
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kelly, G.S. Rhodiola rosea: A possible plant adaptogen. Altern. Med. Rev. 2001, 6, 293–302. [Google Scholar] [PubMed]
- Brown, R.P.; Gerbarg, P.L.; Ramazanov, Z. Rhodiola rosea: A phytomedicinal overview. HerbalGram 2002, 56, 40–52. [Google Scholar]
- Khanum, F.; Bawa, A.S.; Singh, B. Rhodiola rosea: A versatile adaptogen. Compr. Rev. Food Sci. Food Saf. 2005, 4, 55–62. [Google Scholar] [CrossRef] [PubMed]
- Perfumi, M.; Mattioli, L. Adaptogenic and central nervous system effects of single doses of 3% rosavin and 1% salidroside Rhodiola rosea L. extract in mice. Phytother. Res. Int. J. Devoted Pharmacol. Toxicol. Eval. Nat. Prod. Deriv. 2007, 21, 37–43. [Google Scholar]
- Ballmann, C.G.; Maze, S.B.; Wells, A.C.; Marshall, M.M.; Rogers, R.R. Effects of short-term Rhodiola Rosea (Golden Root Extract) supplementation on anaerobic exercise performance. J. Sports Sci. 2018, 37, 998–1003. [Google Scholar] [CrossRef]
- Abidov, M.; Crendal, F.; Grachev, S.; Seifulla, R.; Ziegenfuss, T. Effect of extracts from Rhodiola rosea and Rhodiola crenulata (Crassulaceae) roots on ATP content in mitochondria of skeletal muscles. Bull. Exp. Biol. Med. 2003, 136, 585–587. [Google Scholar] [CrossRef]
- De Bock, K.; Eijnde, B.O.; Ramaekers, M.; Hespel, P. Acute Rhodiola rosea intake can improve endurance exercise performance. Int. J. Sport Nutr. Exerc. Metab. 2004, 14, 298–307. [Google Scholar] [CrossRef] [Green Version]
- Noreen, E.E.; Buckley, J.G.; Lewis, S.L.; Brandauer, J.; Stuempfle, K.J. The effects of an acute dose of Rhodiola rosea on endurance exercise performance. J. Strength Cond. Res. 2013, 27, 839–847. [Google Scholar] [CrossRef]
- Jówko, E.; Sadowski, J.; Długołęcka, B.; Gierczuk, D.; Opaszowski, B.; Cieśliński, I. Effects of Rhodiola rosea supplementation on mental performance, physical capacity, and oxidative stress biomarkers in healthy men. J. Sport Health Sci. 2018, 7, 473–480. [Google Scholar] [CrossRef] [Green Version]
- Parisi, A.; Tranchita, E.; Duranti, G.; Ciminelli, E.; Quaranta, F.; Ceci, R.; Cerulli, C.; Borrione, P.; Sabatini, S. Effects of chronic Rhodiola Rosea supplementation on sport performance and antioxidant capacity in trained male: Preliminary results. J. Sports Med. Phys. Fit. 2010, 50, 57. [Google Scholar]
- Ryan, E.D.; Gerstner, G.R.; Mota, J.A.; Trexler, E.T.; Giuliani, H.K.; Blue, M.N.; Hirsch, K.R.; Smith-Ryan, A.E. The Acute Effects of a Multi-Ingredient Herbal Supplement on Performance Fatigability: A Double-Blind, Randomized, and Placebo-Controlled Trial. J. Diet. Suppl. 2020. [Google Scholar] [CrossRef] [PubMed]
- Lowery, R.P.; Joy, J.M.; Dudeck, J.E.; de Souza, E.O.; McCleary, S.A.; Wells, S.; Wildman, R.; Wilson, J.M. Effects of 8 weeks of Xpand® 2X pre workout supplementation on skeletal muscle hypertrophy, lean body mass, and strength in resistance trained males. J. Int. Soc. Sports Nutr. 2013, 10, 44. [Google Scholar] [CrossRef] [Green Version]
- Mora-Rodríguez, R.; Pallarés, J.G.; López-Samanes, Á.; Ortega, J.F.; Fernández-Elías, V.E. Caffeine ingestion reverses the circadian rhythm effects on neuromuscular performance in highly resistance-trained men. PLoS ONE 2012, 7, e33807. [Google Scholar] [CrossRef] [Green Version]
- Riebe, D.; Ehrman, J.K.; Liguori, G.; Magal, M.; American College of Sports Medicine. ACSM’s Guidelines for Exercise Testing and Prescription; Wolters Kluwer: Alphen am Rhine, The Netherlands, 2018. [Google Scholar]
- Kim, H.; Bae, S.; Kim, Y.; Cho, C.-H.; Kim, S.J.; Kim, Y.-J.; Lee, S.-P.; Kim, H.-R.; Hwang, Y.-I.; Kang, J.S. Vitamin C prevents stress-induced damage on the heart caused by the death of cardiomyocytes, through down-regulation of the excessive production of catecholamine, TNF-α, and ROS production in Gulo (−/−) Vit C-insufficient mice. Free Radic. Biol. Med. 2013, 65, 573–583. [Google Scholar] [CrossRef]
- Bada, A.; Svendsen, J.; Secher, N.; Saltin, B.; Mortensen, S. Peripheral vasodilatation determines cardiac output in exercising humans: Insight from atrial pacing. J. Physiol. 2012, 590, 2051–2060. [Google Scholar] [CrossRef]
- Ballmann, C.G.; McCullum, M.J.; Rogers, R.R.; Marshall, M.M.; Williams, T.D. Effects of Preferred vs. Nonpreferred Music on Resistance Exercise Performance. J. Strength Cond. Res. 2018. [Google Scholar] [CrossRef]
- Williams, T.D.; Martin, M.P.; Mintz, J.A.; Rogers, R.R.; Ballmann, C.G. Effect of Acute Beetroot Juice Supplementation on Bench Press Power, Velocity, and Repetition Volume. J. Strength Cond. Res. 2020, 34, 924–928. [Google Scholar] [CrossRef]
- Ballmann, C.G.; Cook, G.D.; Hester, Z.T.; Kopec, T.J.; Williams, T.D.; Rogers, R.R. Effects of Preferred and Non-Preferred Warm-Up Music on Resistance Exercise Performance. J. Funct. Morphol. Kinesiol. 2021, 6, 3. [Google Scholar] [CrossRef]
- Ballmann, C.G.; Favre, M.L.; Phillips, M.T.; Rogers, R.R.; Pederson, J.A.; Williams, T.D. Effect of Pre-Exercise Music on Bench Press Power, Velocity, and Repetition Volume. Percept. Mot. Ski. 2021, 128, 1183–1196. [Google Scholar] [CrossRef]
- Orange, S.T.; Metcalfe, J.W.; Marshall, P.; Vince, R.V.; Madden, L.A.; Liefeith, A. Test-retest reliability of a commercial linear position transducer (GymAware PowerTool) to measure velocity and power in the back squat and bench press. J. Strength Cond. Res. 2018, 34, 728–737. [Google Scholar] [CrossRef] [Green Version]
- Hori, N.; Andrews, W. Reliability of velocity, force and power obtained from the Gymaware optical encoder during countermovement jump with and without external loads. J. Aust. Strength Cond. 2009, 17, 12–17. [Google Scholar]
- Degrange, T.; Jackson, W.; Williams, T.; Rogers, R.R.; Marshall, M.; Ballmann, C. Acute Caffeine Ingestion Increases Velocity and Power in Upper and Lower Body Free-Weight Resistance Exercises. Int. J. Exerc. Sci. 2019, 12, 1280–1289. [Google Scholar]
- Helms, E.R.; Storey, A.; Cross, M.R.; Brown, S.R.; Lenetsky, S.; Ramsay, H.; Dillen, C.; Zourdos, M.C. RPE and velocity relationships for the back squat, bench press, and deadlift in powerlifters. J. Strength Cond. Res. 2017, 31, 292–297. [Google Scholar] [CrossRef] [PubMed]
- Wei, J.; Carroll, R.J.; Harden, K.K.; Wu, G. Comparisons of treatment means when factors do not interact in two-factorial studies. Amino Acids 2012, 42, 2031–2035. [Google Scholar] [CrossRef] [Green Version]
- Fritz, C.O.; Morris, P.E.; Richler, J.J. Effect size estimates: Current use, calculations, and interpretation. J. Exp. Psychol. Gen. 2012, 141, 2–18. [Google Scholar] [CrossRef] [Green Version]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Erlbaum Associates: Hillsdale, MI, USA, 1988. [Google Scholar]
- Muñiz-Pumares, D.; Lage-Guede, A.; Firth-Clark, A.; Allgrove, J. Effects of acute supplementation with Rhodiola rosea and L-carnitine on exercise performance, cognitive function and cortisol in healthy active volunteers. Br. J. Sports Med. 2011, 45, A1. [Google Scholar] [CrossRef]
- George, A.J. Central nervous system stimulants. In Drugs in Sport; Routledge: London, UK, 2003; pp. 73–111. [Google Scholar]
- Cairns, S.P.; Borrani, F. β-Adrenergic modulation of skeletal muscle contraction: Key role of excitation–contraction coupling. J. Physiol. 2015, 593, 4713–4727. [Google Scholar] [CrossRef] [Green Version]
- French, D.N.; Kraemer, W.J.; Volek, J.S.; Spiering, B.A.; Judelson, D.A.; Hoffman, J.R.; Maresh, C.M. Anticipatory responses of catecholamines on muscle force production. J. Appl. Physiol. 2007, 102, 94–102. [Google Scholar] [CrossRef] [Green Version]
- Cairns, S.P.; Dulhunty, A.F. The effects of β-adrenoceptor activation on contraction in isolated fast-and slow-twitch skeletal muscle fibres of the rat. Br. J. Pharmacol. 1993, 110, 1133–1141. [Google Scholar] [CrossRef]
- Roatta, S.; Arendt-Nielsen, L.; Farina, D. Sympathetic-induced changes in discharge rate and spike-triggered average twitch torque of low-threshold motor units in humans. J. Physiol. 2008, 586, 5561–5574. [Google Scholar] [CrossRef]
- Frye, G.S.; Ferreira, L.F. Norepinephrine Accelerates Diaphragm Fatigue In Vitro; Wiley Online Library: Hoboken, NJ, USA, 2013. [Google Scholar]
- McCarter, F.D.; James, J.H.; Luchette, F.A.; Wang, L.; Friend, L.A.; King, J.-K.; Evans, J.M.; George, M.A.; Fischer, J.E. Adrenergic blockade reduces skeletal muscle glycolysis and Na+, K+-ATPase activity during hemorrhage. J. Surg. Res. 2001, 99, 235–244. [Google Scholar] [CrossRef] [PubMed]
- Qvisth, V.; Hagstrom-Toft, E.; Enoksson, S.; Bolinder, J. Catecholamine regulation of local lactate production in vivo in skeletal muscle and adipose tissue: Role of β-adrenoreceptor subtypes. J. Clin. Endocrinol. Metab. 2008, 93, 240–246. [Google Scholar] [CrossRef] [Green Version]
- Zając, A.; Chalimoniuk, M.; Maszczyk, A.; Gołaś, A.; Lngfort, J. Central and peripheral fatigue during resistance exercise—A critical review. J. Hum. Kinet. 2015, 49, 159. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | Mean ± SD |
|---|---|
| Age (years) | 24.8 ± 5.6 |
| Height (cm) | 178.6 ± 7.1 |
| BM (kg) | 83.2 ± 7.6 |
| Training Experience (years) | 8.7 ± 6.3 |
| 1-RM (kg) | 114.2 ± 15.8 |
| Relative BP Strength [1-RM (kg)/BM (kg)] | 1.4 ± 0.2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Williams, T.D.; Langley, H.N.; Roberson, C.C.; Rogers, R.R.; Ballmann, C.G. Effects of Short-Term Golden Root Extract (Rhodiola rosea) Supplementation on Resistance Exercise Performance. Int. J. Environ. Res. Public Health 2021, 18, 6953. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18136953
Williams TD, Langley HN, Roberson CC, Rogers RR, Ballmann CG. Effects of Short-Term Golden Root Extract (Rhodiola rosea) Supplementation on Resistance Exercise Performance. International Journal of Environmental Research and Public Health. 2021; 18(13):6953. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18136953
Chicago/Turabian StyleWilliams, Tyler D., Haley N. Langley, Caleb C. Roberson, Rebecca R. Rogers, and Christopher G. Ballmann. 2021. "Effects of Short-Term Golden Root Extract (Rhodiola rosea) Supplementation on Resistance Exercise Performance" International Journal of Environmental Research and Public Health 18, no. 13: 6953. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18136953