
Facial Self-Touching and the Propagation of COVID-19: The Role of Gloves in the Dental Practice

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design Type
2.2. Data Collection
2.3. Instruments:
2.4. Statistical Analysis
3. Results
3.1. Sociodemographic Variables
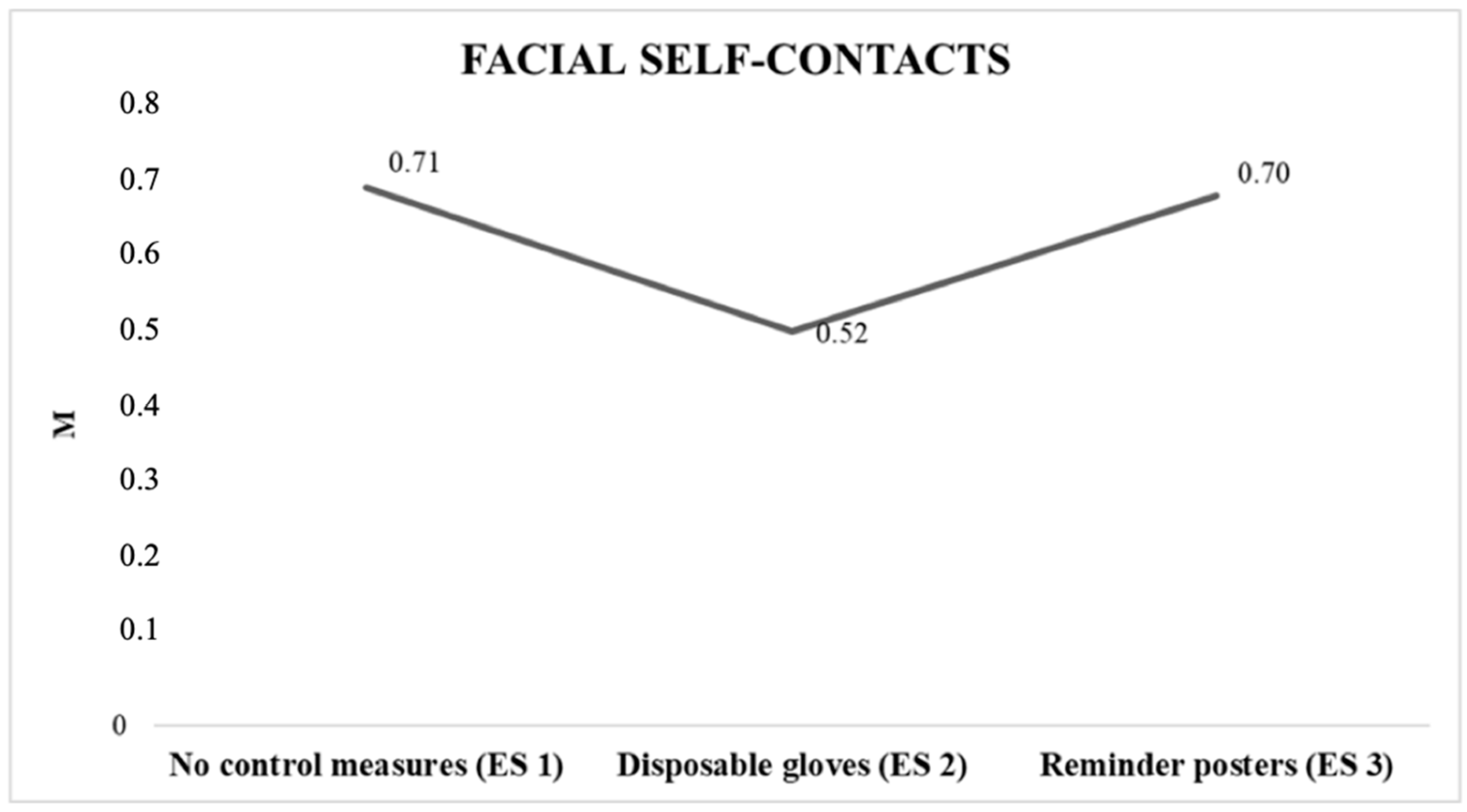
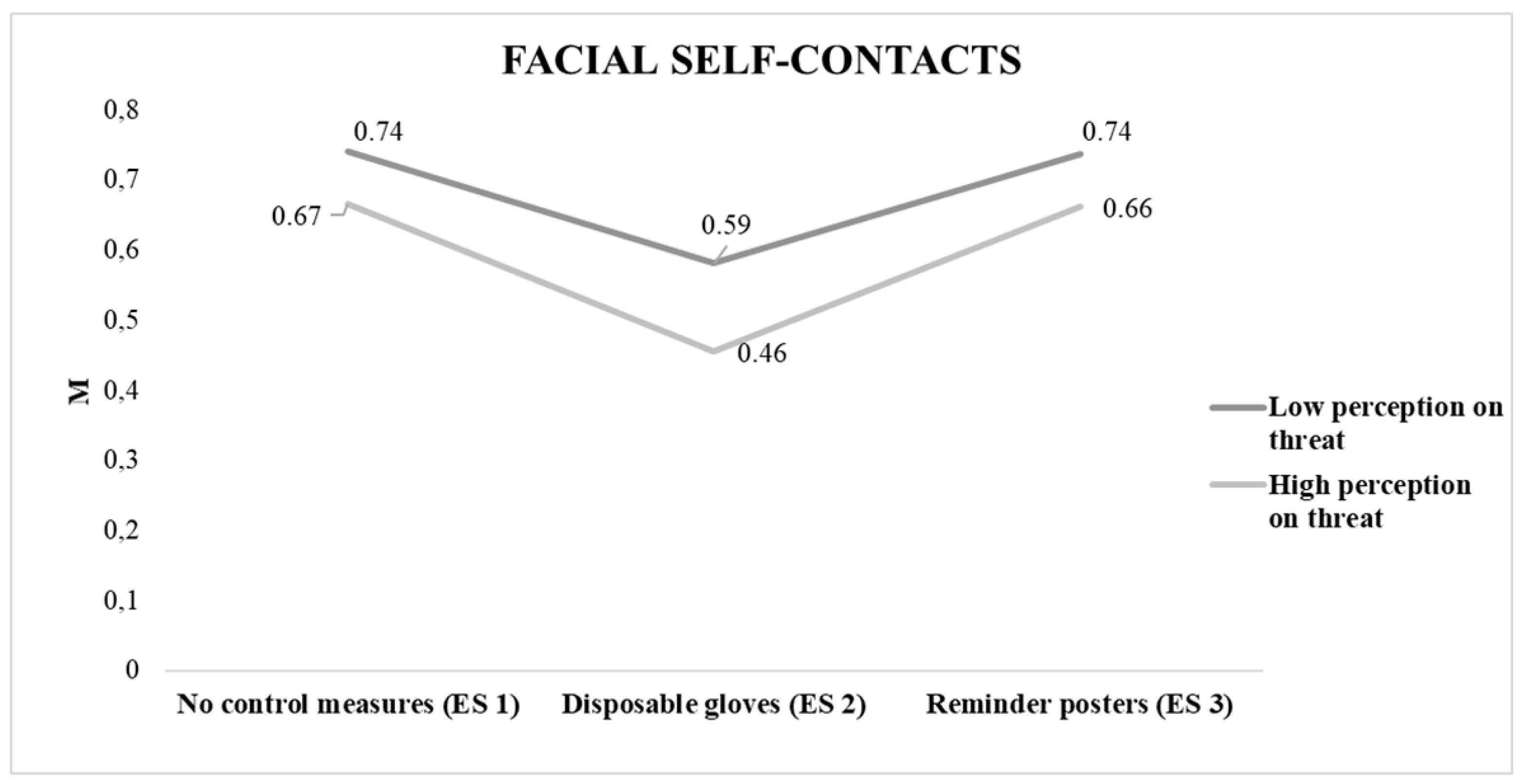
3.2. Facial Self-Touching
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
References
- Country & Technical Guidance-Coronavirus Disease (COVID-19). Retrieved 2 November 2020. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical-guidance (accessed on 5 March 2021).
- WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19—11 March 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 5 March 2021).
- Dhama, K.; Sharun, K.; Tiwari, R.; Dadar, M.; Malik, Y.S.; Singh, K.P.; Chaicumpa, W. COVID-19, an emerging coronavirus infection: Advances and prospects in designing and developing vaccines, immunotherapeutics, and therapeutics. Hum. Vaccines Immunother. 2020, 16, 1232–1238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- COVID-19|European Centre for Disease Prevention and Control. Available online: https://qap.ecdc.europa.eu/public/extensions/COVID-19/COVID-19.html#global-overview-tab (accessed on 5 March 2021).
- Infección Por el Nuevo Coronavirus COVID-19. Informe Epidemiológico COVID-19; Dirección General de Salud Pública. CONSEJERÍA DE SANIDAD. Available online: https://www.comunidad.madrid/sites/default/files/doc/sanidad/epid/informe_epidemiologico_semanal_covid.pdf (accessed on 5 March 2021).
- Hamedani, S.; Farshidfar, N.; Ziaei, A.; Pakravan, H. The Dilemma of COVID-19 in Dental Practice Concerning the Role of Saliva in Transmission: A Brief Review of Current Evidence. Eur. Oral Res. 2020, 54, 92–100. [Google Scholar] [CrossRef]
- Li, J.-P.O.; Lam, D.S.C.; Chen, Y.; Ting, D.S.W. Novel Coronavirus disease 2019 (COVID-19): The importance of recognising possible early ocular manifestation and using protective eyewear. Br. J. Ophthalmol. 2020, 104, 297–298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wise, J. Covid-19: New coronavirus variant is identified in UK. BMJ 2020, 371, m4857. [Google Scholar] [CrossRef]
- Koyama, T.; Platt, D.; Parida, L. Variant analysis of SARS-CoV-2 genomes. Bull. World Health Organ. 2020, 98, 495–504. [Google Scholar] [CrossRef] [PubMed]
- Pradhan, D.; Biswasroy, P.; Naik, P.K.; Ghosh, G.; Rath, G. A Review of Current Interventions for COVID-19 Prevention. Arch. Med Res. 2020, 51, 363–374. [Google Scholar] [CrossRef] [PubMed]
- Furuya, H. Prediction of Potential Respiratory Tract Infection from SARS-CoV-2 Through Hand-to-face Contact Transmission. Tokai J. Exp. Clin. Med. 2020, 45, 170–175. [Google Scholar]
- Firouzbakht, M.; Omidvar, S.; Firouzbakht, S.; Asadi-Amoli, A. COVID-19 preventive behaviors and influencing factors in the Iranian population; a web-based survey. BMC Public Health 2021, 21, 1–7. [Google Scholar] [CrossRef]
- Roos, A.-L.; Goetz, T.; Voracek, M.; Krannich, M.; Bieg, M.; Jarrell, A.; Pekrun, R. Test Anxiety and Physiological Arousal: A Systematic Review and Meta-Analysis. Educ. Psychol. Rev. 2021, 33, 579–618. [Google Scholar] [CrossRef]
- Kwok, Y.L.A.; Gralton, J.; McLaws, M.-L. Face touching: A frequent habit that has implications for hand hygiene. Am. J. Infect. Control. 2015, 43, 112–114. [Google Scholar] [CrossRef] [PubMed]
- Nicas, M.; Best, D. A Study Quantifying the Hand-to-Face Contact Rate and Its Potential Application to Predicting Respiratory Tract Infection. J. Occup. Environ. Hyg. 2008, 5, 347–352. [Google Scholar] [CrossRef]
- Pérez-Fuentes, M.C.; Molero, M.M.; Martos, Á.; Gázquez, J.J. Threat of COVID-19 and emotional state during quarantine: Positive and negative affect as mediators in a cross-sectional study of the Spanish population. PLoS ONE 2020, 15, e0235305. [Google Scholar] [CrossRef]
- Coem. Protocolo de Prevención Sanitaria Frente al Covid-19. Colegio de Odontólogos de Madrid (COEM). 2020. Available online: https://www.coem.org.es/media/news/pdf/protocoloCovidPacientesCOEM.pdf (accessed on 1 March 2021).
- Giakoumis, D.; Drosou, A.; Cipresso, P.; Tzovaras, D.; Hassapis, G.; Gaggioli, A.; Riva, G. Real-time monitoring of behavioural parameters related to psychological stress. Stud. Health Technol. Inform. 2012, 181, 287–291. [Google Scholar]
- Edmunds, D.M.; Gothard, L.; Khabra, K.; Kirby, A.; Madhale, P.; McNair, H.; Roberts, D.; Tang, K.K.; Symonds-Tayler, R.; Tahavori, F.; et al. Low-cost Kinect Version 2 imaging system for breath hold monitoring and gating: Proof of concept study for breast cancer VMAT radiotherapy. J. Appl. Clin. Med. Phys. 2018, 19, 71–78. [Google Scholar] [CrossRef]
- Galna, B.; Barry, G.; Jackson, D.; Mhiripiri, D.; Olivier, P.; Rochester, L. Accuracy of the Microsoft Kinect sensor for measuring movement in people with Parkinson’s disease. Gait Posture 2014, 39, 1062–1068. [Google Scholar] [CrossRef] [Green Version]
- Clark, R.A.; Pua, Y.-H.; Fortin, K.; Ritchie, C.; Webster, K.E.; Denehy, L.; Bryant, A.L. Validity of the Microsoft Kinect for assessment of postural control. Gait Posture 2012, 36, 372–377. [Google Scholar] [CrossRef] [PubMed]
- Allahyari, T.; Samani, A.S.; Khalkhali, H.-R. Validity of the Microsoft Kinect for measurement of neck angle: Comparison with electrogoniometry. Int. J. Occup. Saf. Ergon. 2016, 23, 524–532. [Google Scholar] [CrossRef] [PubMed]
- Springer, S.; Seligmann, G.Y. Validity of the Kinect for Gait Assessment: A Focused Review. Sensors 2016, 16, 194. [Google Scholar] [CrossRef]
- Spielberger, C.D.; Gorsuch, R.; Lushene, R.; Vagg, P.R.; Jacobs, G.A. Manual for the State-Trait Anxiety Inventory; Consulting Psychologists Press: Palo Alto, CA, USA, 1983. [Google Scholar]
- Pérez-Fuentes, M.C.; Molero, M.M.; Oropesa, N.F. Questionnaire on Perception of Threat from COVID-19. JCM 2020, 9, 1196. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; 2.a ed., Routledge. 2013. Available online: https://www.taylorfrancis.com/books/9780203771587 (accessed on 3 March 2021).
- Julian, L.J. Measures of anxiety: State-Trait Anxiety Inventory (STAI), Beck Anxiety Inventory (BAI), and Hospital Anxiety and Depression Scale-Anxiety (HADS-A). Arthritis Rheum. 2011, 63, S467–S472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prado-Gascó, V.; Gómez-Domínguez, M.T.; Soto-Rubio, A.; Díaz-Rodríguez, L.; Navarro-Mateu, D. Stay at Home and Teach: A Comparative Study of Psychosocial Risks Between Spain and Mexico During the Pandemic. Front. Psychol. 2020, 11. [Google Scholar] [CrossRef] [PubMed]
- Woods, D.W.; Miltenberger, R.G. Are persons with nervous habits nervous? A preliminary examination of habit function in a nonreferred population. J. Appl. Behav. Anal. 1996, 29, 259–261. [Google Scholar] [CrossRef] [Green Version]
- Ramírez-Ortiz, J.; Castro-Quintero, D.; Lerma-Córdoba, C.; Yela-Ceballos, F.; Escobar-Córdoba, F. Mental health consequences of the COVID-19 pandemic associated with social isolation. Colomb. J. Esthesiol. 2020, 48, 4. [Google Scholar] [CrossRef]
- Duan, L.; Zhu, G. Psychological interventions for people affected by the COVID-19 epidemic. Lancet Psychiatry 2020, 7, 300–302. [Google Scholar] [CrossRef]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate Psychological Responses and Associated Factors during the Initial Stage of the 2019 Coronavirus Disease (COVID-19) Epidemic among the General Population in China. Int. J. Environ. Res. Public Health 2020, 17, 1729. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Questionnaires | Mean | SD |
|---|---|---|
| STAI–S | 18.26 | 13.91 |
| BIPQ–5 | 29.28 | 11.39 |
| Self–touching/minute Experimental situation 1 | 0.70 | 0.11 |
| Self–touching/minute Experimental situation 2 | 0.52 | 0.14 |
| Self–touching/minute Experimental situation 3 | 0.70 | 0.14 |
| Heart rate/minute | 75.26 | 11.36 |
| Systolic blood pressure | 135.15 | 9.45 |
| Diastolic blood pressure | 86.74 | 4.55 |
| Questionnaires | Gender | Previous Psychological Problems | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean (SD) Man n = 62 | Mean (SD) Woman n = 88 | t | p | d | Mean (SD) Yes n = 26 | Mean (SD) No n = 124 | t | p | d | |
| STAI–S | 14.9 (11.88) | 20.6 (14.8) | 2.51 | 0.01 * | 0.42 | 27.5 (19.1) | 16.3 (11.7) | 3.91 | 0.01 ** | 0.71 |
| BIP–Q5 | 28.2 (11.66) | 29.9 (11.2) | 0.89 | 0.37 | 0.14 | 33.9 (10.6) | 28.3 (11.3) | 2.43 | 0.02 * | 0.51 |
| Self–contacts/minute ES 1 | 0.7 (0.1) | 0.7 (0.1) | 0.51 | 0.6 | 0.08 | 0.6 (0.1) | 0.7 (0.1) | 0.99 | 0.32 | 0.23 |
| Self–contacts/minute ES 2 | 0.5 (0.1) | 0.5 (0.1) | 0.19 | 0.68 | 0.07 | 0.4 (0.1) | 0.5 (0.1) | 1.61 | 0.11 | 0.35 |
| Self–contacts/minute ES 3 | 0.6 (0.1) | 0.7 (0.1) | 0.64 | 0.41 | 0.15 | 0.6 (0.1) | 0.7 (0.1) | 0.16 | 0.87 | 0.06 |
| Heart rate/minute | 75.9 (11.5) | 74.8 (11.2) | 0.58 | 0.55 | 0.09 | 79.6 (11.4) | 74.3 (11.1) | 2.18 | 0.02 | 0.47 |
| Systolic blood pressure | 134.5 (9.6) | 135.5 (9.3) | 0.63 | 0.52 | 0.11 | 137.3 (9.9) | 134.7 (9.3) | 1.22 | 0.22 | 0.26 |
| Diastolic blood pressure | 86.4 (4.5) | 96.9 (4.5) | 0.61 | 0.54 | 0.11 | 87.1 (4.8) | 86.6 (4.5) | 0.50 | 0.63 | 0.18 |
| Questionnaires | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 |
|---|---|---|---|---|---|---|---|---|
| STAI–S | 0.188 * | 0.220 ** | 0.045 | 0.191 * | 0.454 ** | 0.328 ** | 0.136 | |
| BIPQ–5 | –0.393 ** | –0.466 ** | –0.290 ** | 0.082 | 0.043 | 0.044 | ||
| Self–contacts ES 1 | 0.738 ** | 0.824 ** | 0.274 ** | 0.188 * | 0.214 ** | |||
| Self–contacts ES 2 | 0.654 ** | 0.167 * | –0.003 | 0.025 | ||||
| Self–contacts ES 3 | 0.218 * | 0.168 * | 0.149 | |||||
| Heart rate | 0.341 ** | 0.308 ** | ||||||
| Systolic blood pressure | 0.594 ** | |||||||
| Diastolic blood pressure |
| Study | Self–Contacts ES 1 | Self–Contacts ES 2 | Self–Contacts ES 3 | 1–2 | 1–3 | 2–3 |
|---|---|---|---|---|---|---|
| Facial Self–Contact | 0.7 (0.1) | 0.5 (0.1) | 0.7 (0.1) | p < 0.01 ** IC [–2.1—1.6] | 1 IC [–0.11–0.21] | p < 0.01 ** IC [–0.7 –1.2] |
| Variable | Frequency of Self–Contacts in ES 2 | |||||
|---|---|---|---|---|---|---|
| Model 1 | Model 2 | Model 3 | ||||
| B | β | B | β | B | β | |
| Constant | 5.49 ** | 7.59 ** | 7.83 ** | |||
| Heart rate | 0.03 * | 0.16 | 0.03 * | 0.20 | 0.03 * | 0.18 |
| BIPQ–5 | –0.09** | –0.48 | –0.09 ** | –0.49 | ||
| STAI–S | 0.01 | 0.05 | ||||
| R2 | 0.028 | 0.259 | 0.261 | |||
| F | 4.223 * | 25.709 ** | 17.229 ** | |||
| ΛR2 | 0.028 | 0.231 | 0.002 | |||
| ΛF | 4.223 * | 45.913 ** | 0.459 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carrillo-Díaz, M.; Lacomba-Trejo, L.; Romero-Maroto, M.; González-Olmo, M.J. Facial Self-Touching and the Propagation of COVID-19: The Role of Gloves in the Dental Practice. Int. J. Environ. Res. Public Health 2021, 18, 6983. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18136983
Carrillo-Díaz M, Lacomba-Trejo L, Romero-Maroto M, González-Olmo MJ. Facial Self-Touching and the Propagation of COVID-19: The Role of Gloves in the Dental Practice. International Journal of Environmental Research and Public Health. 2021; 18(13):6983. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18136983
Chicago/Turabian StyleCarrillo-Díaz, María, Laura Lacomba-Trejo, Martín Romero-Maroto, and María José González-Olmo. 2021. "Facial Self-Touching and the Propagation of COVID-19: The Role of Gloves in the Dental Practice" International Journal of Environmental Research and Public Health 18, no. 13: 6983. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18136983